Paeds · paediatric-dermatology
Approach to rash in infants and children
Also known as Paediatric rash · Childhood exanthem · Skin eruption in children · Neonatal rash · Approach to exanthem · Rash assessment in children
A morphology-first, distribution-aware and red-flag-driven fellowship approach to any rash from the neonate to the adolescent: classify the lesion, map the pattern, weigh age, fever, itch and mucosa, and separate benign and self-limiting eruptions from the emergencies - meningococcaemia, Stevens-Johnson syndrome/toxic epidermal necrolysis, staphylococcal scalded skin syndrome, necrotising fasciitis, Kawasaki disease and neonatal sepsis or herpes simplex.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A rash is one of the commonest reasons a family brings a child to see you, and it is the presentation that most often makes clinicians feel they are guessing. The mistake is to try to recognise a single disease from its colour or its overall impression. The reliable method is the opposite: describe what you actually see in a structured way, and let the morphology, the distribution and the age of the child narrow the list for you. This page gives you that method, applied from the neonate to the adolescent, and tells you exactly where the danger lies. [1]
Overview & Definition
A rash is any change in the colour, texture or surface of the skin that is widespread or patterned rather than a single isolated lesion. Two terms recur throughout paediatrics. An exanthem is an eruption on the skin surface - the classic childhood "viral rash". An enanthem is the same kind of eruption on a mucosal surface, such as the mouth (for example the Koplik spots of measles or the oral ulcers of hand-foot-and-mouth disease). The distinction matters because an enanthem is a powerful clue to the cause and to several dangerous diagnoses. [5]
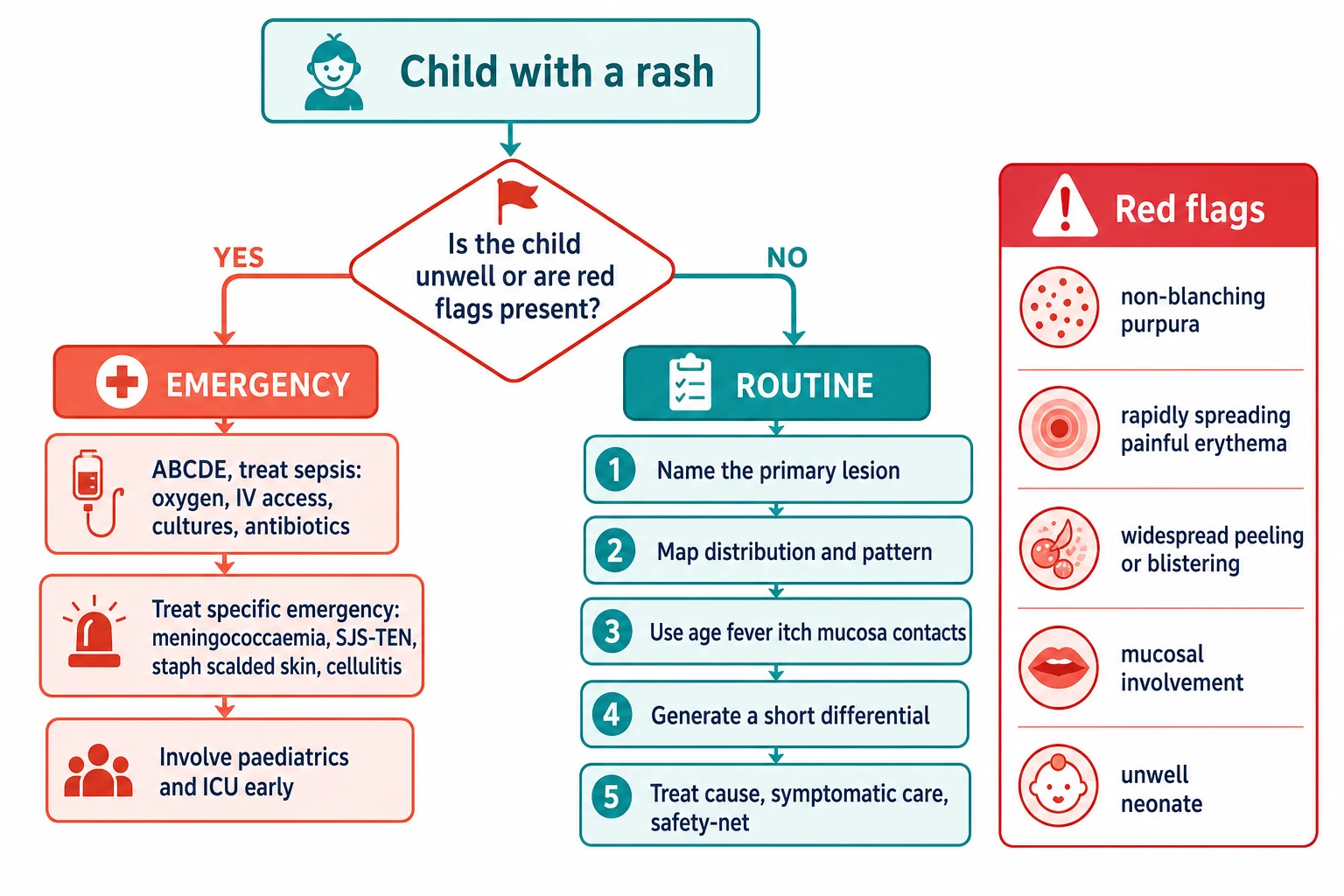
What makes a rash hard is that the same disease can look different on different children and on different skin tones, while very different diseases can look alike. The defence against this is a framework rather than a mental picture: rather than asking "what is this rash?", you ask four questions in order. First, is the child sick or well - because the unwell child with a rash is an emergency regardless of what the rash looks like. Second, what is the morphology - what are the individual lesions? Third, what is the distribution and pattern - where are they and how are they arranged? Fourth, what is the context - the age, the fever, the itch, the mucosa, the contacts and the tempo. Answer those four and the differential collapses to a short list you can reason about. [1]
Classification
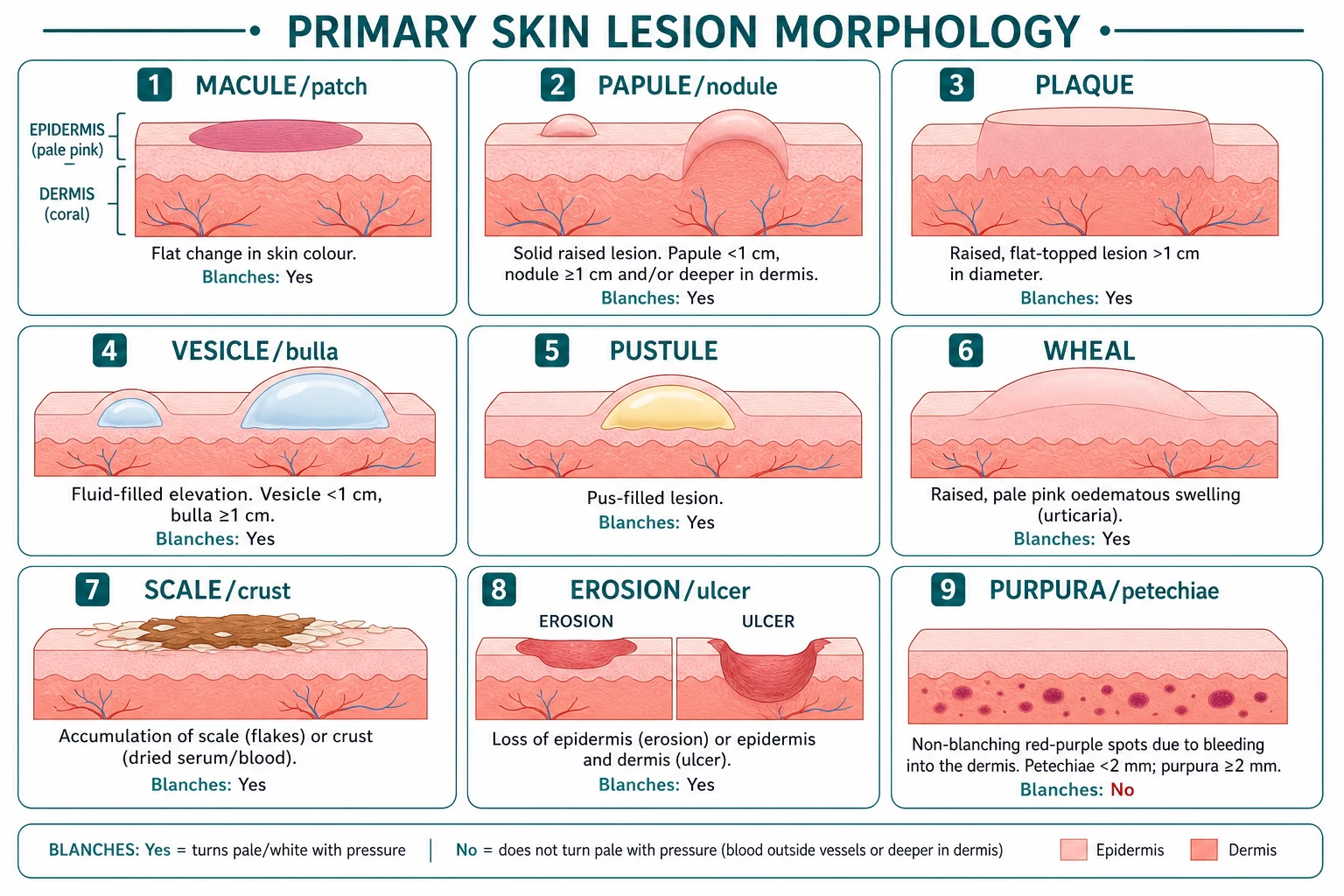
The first classification is by morphology - the shape and feel of the individual lesion, not the overall rash. This is the language dermatology runs on, and using it precisely is what separates a confident assessment from a guess. A macule is a flat colour change you cannot feel, less than about a centimetre; a patch is the same but larger. A papule is a small raised solid bump (under a centimetre); a nodule is larger and deeper. A plaque is a flat-topped raised area, usually more than a centimetre, often formed by papules joining up. A vesicle is a small clear fluid-filled blister; a bulla is a larger one. A pustule is filled with pus (yellow). A wheal is the raised, pale-pink, transient swelling of urticaria. These are your primary lesions. [1]
Layered on top of a primary process you may find secondary changes: scale (flakes of stratum corneum), crust (dried serum or blood, a scab), erosion (loss of epidermis, heals without scarring) and ulcer (loss into the dermis, may scar), plus lichenification (thickened skin from chronic rubbing) and excoriation (scratch marks). These tell you about chronicity and scratching, which is the heart of the eczema story. [1]
The second classification is by distribution and pattern, and it is often more discriminating than morphology alone. Is the rash flexural (the folds of eczema) or extensor (the knees and elbows of psoriasis)? Is it acral, on the hands, feet and face (hand-foot-and-mouth disease, scabies, Kawasaki)? Is it intertriginous or in the napkin area (candidal or irritant nappy rash, seborrhoeic dermatitis)? Is it dermatomal, following a nerve root (zoster)? Is it photodistributed, only on sun-exposed skin? Is there mucosal involvement (the mouth, eyes, genitalia - think SJS/TEN, Kawasaki, HFMD, measles)? And how is it arranged in time - the centrifugal spread of smallpox-classic patterns versus the crops-at-different-stages of chickenpox? Naming the distribution turns "a rash" into "a flexural, scaly, itchy eruption in an atopic toddler" - which is atopic dermatitis. [11]
Epidemiology & Risk Factors
Skin problems sit near the top of every list of why children see a doctor. In primary care, outpatient general paediatrics and the emergency department, rashes and skin complaints are among the most common presentations, and atopic dermatitis is the most prevalent chronic skin disease of childhood. The epidemiology is strongly age-structured, which is why age is one of the four anchor questions in this approach. [1]
The risk factors map onto age and environment. Atopy - a personal or family history of eczema, asthma, allergic rhinitis or food allergy - is the dominant risk factor for atopic dermatitis and shapes the atopic march. Immunocompromise, whether from chemotherapy, transplant, primary immunodeficiency or HIV, raises both the severity and the range of opportunistic skin infections. Crowding and household contacts drive scabies and impetigo, which is why these cluster in families and in institutions. Vaccination status changes the landscape of the classic exanthems: measles and rubola return in under-vaccinated communities. Drug exposure is the key risk factor for drug eruptions and for the severe cutaneous adverse reactions SJS/TEN and DRESS. Travel, animal and insect exposure, and climate add tropical and vector-borne possibilities. In Indigenous, remote and tropical communities, scabies and group A streptococcal impetigo are hyperendemic and drive post-streptococcal glomerulonephritis and acute rheumatic fever - a burden that makes a "simple" skin infection a population-health problem, not just a clinical one. [4]
Pathophysiology
The reason morphology works as a diagnostic tool is that each morphology reflects a mechanism in the skin. If you can read the mechanism from the lesion, you can reason backwards to the cause. This is why the same four mechanisms keep reappearing across completely different diseases. [1]
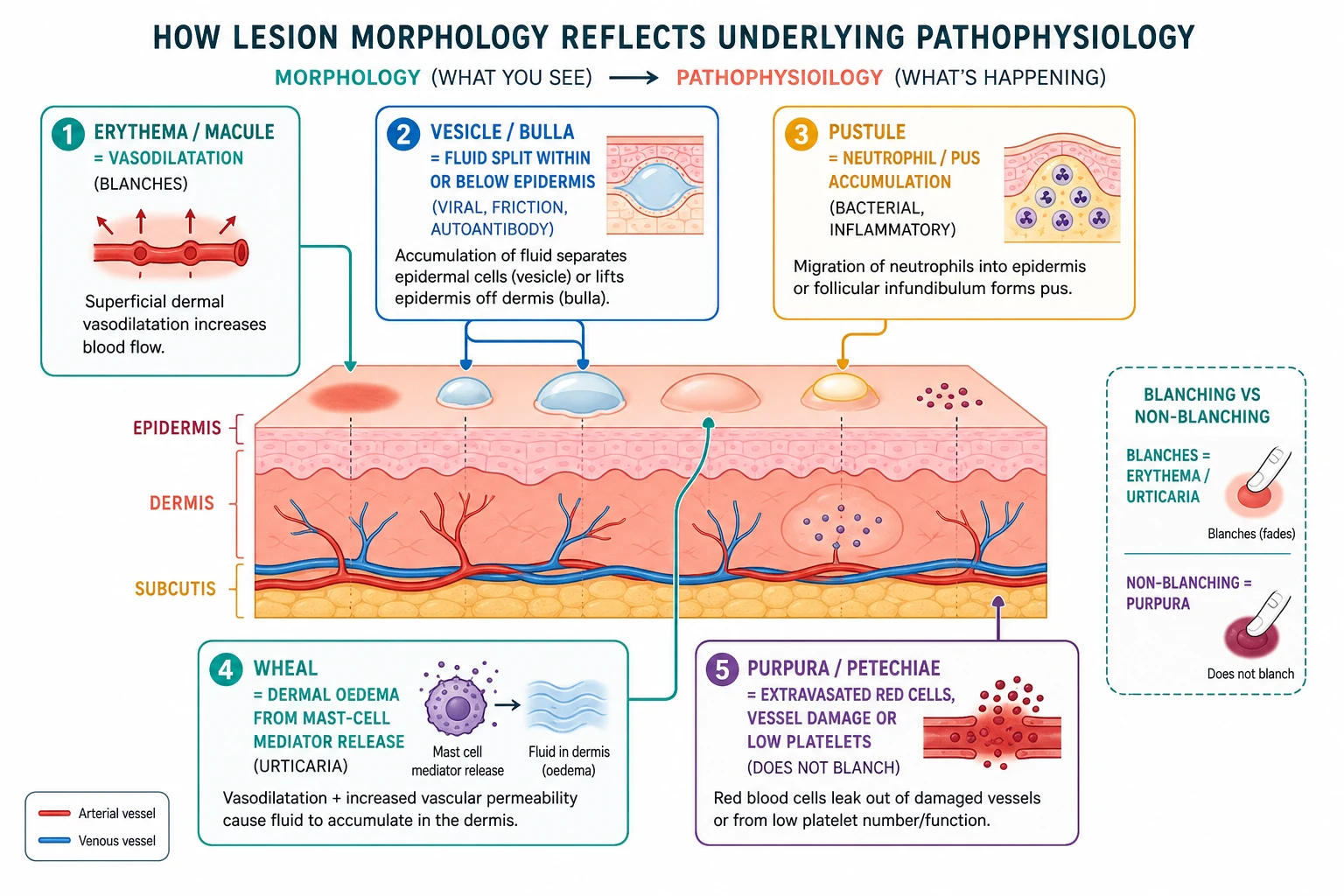
Erythema - redness - is simply vasodilatation, which is why it blanches when you press it: you push the blood out of the dilated vessels. A vesicle or bulla is a collection of fluid within or just below the epidermis, whether from viral destruction of keratinocytes (herpesviruses, enteroviruses), friction, an autoimmune split (in the pemphigus/pemphigoid family) or severe keratinocyte necrosis (SJS/TEN). A pustule is dominated by neutrophils - pus - which points to bacterial infection or intense neutrophilic inflammation, though neonatal pustular eruptions such as erythema toxicum are sterile. A wheal is dermal oedema driven by mast-cell mediator release; the lesion appears, migrates and resolves within 24 hours, which is the hallmark of urticaria. [1]
The mechanism that matters most at the bedside is purpura. Purpura and petechiae are red blood cells that have escaped the vessel into the skin. Because the blood is outside the vessel, pressing on it does nothing - it does not blanch, and this single test separates vascular erythema (which blanches) from bleeding into the skin (which does not). Purpura comes from one of three failures: vessel damage (vasculitis, meningococcal endothelial injury), low or dysfunctional platelets (immune thrombocytopenia, leukaemia), or a coagulation problem. The emergency beneath that mechanism is that meningococcal septicaemia injures the endothelium and can trigger disseminated intravascular coagulation, producing the rapidly evolving petechial-purpuric rash of an unwell child. [7]
The two great blistering emergencies illustrate how mechanism decides management even when the clinical picture looks similar. In staphylococcal scalded skin syndrome, a staphylococcal exfoliative toxin cleaves desmoglein-1 in the superficial epidermis, producing a very superficial subcorneal split, widespread tender erythema and superficial peeling with flexural accentuation and no mucosal involvement. In Stevens-Johnson syndrome and toxic epidermal necrolysis, the split is at the basal layer with full-thickness epidermal necrosis, driven by a drug or infection, and mucosal involvement is prominent. They can look alike from the end of the bed, but the cleavage plane and the mucosal pattern point to the right diagnosis and the right disposition. [9] [10]
Clinical Presentation
The history of a rash is often more diagnostic than the look of it, so take it deliberately and in the same order every time. Ask where it started and how it spread: roseola begins on the trunk after the fever falls; measles spreads head-to-toe; IgA vasculitis sits on the lower legs and buttocks. Ask about tempo - the hours-old purpura of meningococcaemia versus the weeks-old scaly eczema. Ask whether the rash is itchy or painful: itch points to eczema, scabies, urticaria and molluscum; pain and tenderness point to cellulitis, erythema nodosum, SJS/TEN and SSSS. Ask about fever and systemic symptoms: a febrile exanthem narrows to infection, drug or Kawasaki; an afebrile, well child narrows to eczema, scabies, molluscum, warts or urticaria. [1]
Then ask the questions that frame the cause. Are there mucosal lesions in the mouth, eyes or genitalia (SJS/TEN, Kawasaki, HFMD, measles)? Are there sick contacts or an outbreak at school or childcare? Is the child immunised, and has there been any drug exposure in the last one to eight weeks (the window for SJS/TEN and drug eruptions)? Is there a personal or family history of atopy? Has the child travelled, or had animal or insect contact? And, especially in an infant, what is in the napkin area, on the scalp and behind the ears? [9]
Atypical presentations are where candidates fail. Early meningococcaemia may be nonspecific for hours, with a flu-like illness and only a few spots before the purpuric cascade. Incomplete Kawasaki is easy to miss because the child does not meet the full criteria yet is still at risk of coronary artery aneurysms. Purpura in deeply pigmented skin is subtler - you must look carefully with good light and palpate. The immunocompromised child may have muted, atypical or disseminated disease. And any unwell neonate with vesicles, pustules or even non-specific erythema must be presumed to have neonatal herpes simplex or sepsis until tested. [3] [8]
Differential Diagnosis
The differential is built by crossing morphology with distribution and context. Rather than listing every disease, group the rash by what you actually see and generate the candidates for that group - this is how you avoid being overwhelmed. The groups below cover almost every rash a child will present with. [1]
Within the eczematous and scaly group, the discriminating features are distribution, itch and tempo. Atopic dermatitis is intensely itchy and, in infants, affects the cheeks and extensor surfaces before settling into the flexural folds of older children; it is virtually always itchy and chronic. Seborrhoeic dermatitis (cradle cap in infants) is greasy, yellow-scaled, sits on the scalp, eyebrows and napkin area, and is not very itchy. Contact dermatitis appears where the culprit touched the skin and has a sharp, geometric border. Tinea is an annular, scaly, slowly enlarging ring with a raised edge and central clearing. [11]
Within the vesiculobullous group, the discriminating features are the lesion content, the distribution and the child's wellness. Chickenpox crops lesions at different stages simultaneously (papules, vesicles, pustules, crusts) and is classically a "dewdrop on a rose petal". Hand-foot-and-mouth disease targets the mouth plus the palms, soles and buttocks. Bullous impetigo has flaccid superficial blisters that rupture easily, leaving a honey-coloured crust. Neonatal herpes can be vesicular, pustular, or present with no skin lesions at all - just sepsis or encephalopathy - which is why any unwell neonate with even one vesicle needs testing and empirical aciclovir. SJS/TEN and SSSS both blister and peel, but SJS/TEN has mucosal involvement and full-thickness necrosis while SSSS spares mucosa and peels superficially. [3] [9] [10]
The purpuric group is the highest-stakes differential in paediatrics, and the features that distinguish its members decide whether a child is treated for sepsis or sent home. Meningococcaemia is an unwell or febrile child with rapidly evolving non-blanching purpura. Immune thrombocytopenia is a well child with isolated petechiae and bruising but no other blood-count abnormalities. IgA vasculitis (Henoch-Schonlein purpura) is palpable purpura on the lower limbs and buttocks with abdominal pain, arthritis or renal involvement. Leukaemia presents with purpura alongside other cytopenias, pallor, fever and organomegaly. And bruising in a pre-mobile infant, or bruising in unusual places, raises non-accidental injury. [7] [12]
The maculopapular febrile exanthems are the commonest exam scenario, and you distinguish them by their timeline, their prodrome and the pattern of spread. Roseola (human herpesvirus 6) is three to five days of high fever in a well-looking infant, then the rash appears on the trunk as the fever falls. Erythema infectiosum (parvovirus B19, fifth disease) gives the "slapped-cheek" appearance followed by a reticulate trunk rash, and carries a fetal risk in pregnancy. Measles has a prodrome of cough, coryza and conjunctivitis with Koplik spots, then a blotchy rash spreading head-to-toe. Hand-foot-and-mouth disease (coxsackievirus) gives oral ulcers plus palm and sole lesions. Kawasaki is the mimic you must not miss: prolonged fever plus a polymorphous rash, conjunctivitis, strawberry tongue, red cracked lips, and swollen hands and feet. [5] [8]
Clinical & Bedside Assessment
Examine the skin systematically, and do it properly: fully undress the child, use good lighting (natural if possible), and look at the entire skin including the scalp, behind the ears, the napkin area, the palms, the soles, the mucous membranes, the nails and the genitalia. The most common examination error is to look only at the obvious patch and miss the distribution that names the diagnosis. Palpate the lesions for texture and, crucially, for blanching. [1]
Two named bedside manoeuvres carry most of the diagnostic weight. Diascopy - pressing a clear glass slide or lens against the lesion - tests blanching: erythema and urticaria blanch, purpura does not. This is the test that separates the reassuring rash from the emergency, and it costs nothing. The Nikolsky sign is the tangential shearing of apparently normal-appearing epidermis with a finger, leaving a moist glistening surface; it is positive when the epidermis is fragile, in SJS/TEN and in SSSS. A positive Nikolsky sign in an unwell, blistering child is a major red flag. [9] [10]
Assess the whole child before the skin. Use the paediatric assessment triangle - appearance, work of breathing and circulation to skin - and take the vital signs, because an unwell-looking child, tachycardia, prolonged capillary refill, cold peripheries or altered responsiveness changes everything regardless of the rash. Then examine for the associated signs that complete each diagnosis: lymphadenopathy and hepatosplenomegaly; the arthritis and abdominal pain of IgA vasculitis; the conjunctivitis, strawberry tongue, cheilitis and extremity changes of Kawasaki; the ears and throat; and the joints. A focused skin exam is never just the skin. [7] [8]
Investigations
Most paediatric rashes are diagnosed clinically - the history and examination are the investigation, and over-investigating a clearly benign rash is a failure of the method just as much as missing a dangerous one is. Investigations are reserved for the unwell child, the ambiguous purpura, the blistering eruption, the chronic or worsening rash, and the immunocompromised. [1]
For the unwell febrile child with a rash, take a full blood count, C-reactive protein, coagulation studies, a blood culture and a meningococcal PCR; a lumbar puncture is done only if it is clinically safe and indicated, and never at the cost of delaying antibiotics in a shocked child. For a vesicle or blister, swab for PCR to identify herpes simplex and varicella zoster; for a pustule, a Gram stain and bacterial culture directs antibiotic choice. For petechiae or purpura in a well child, a full blood count and film exclude thrombocytopenia and leukaemia, and coagulation studies exclude a bleeding disorder. For a scaly annular lesion suspicious for tinea, a skin scraping for potassium hydroxide microscopy and fungal culture confirms the dermatophyte. [7]
A skin biopsy is indicated when the diagnosis remains unclear, when a vasculitis or blistering disorder is suspected, or when malignancy is in the differential. Photography of the lesions - with consent - is invaluable for tracking evolution over time and for the medicolegal record, especially where non-accidental injury is a consideration. And whenever a bruise or purpura appears on a pre-mobile infant or in an unusual distribution, hold the diagnosis of "easy bruising" and consider non-accidental injury, applying the TEN-4-FACESp bruising rule (bruising of the Torso, Ear, or Neck in any child under 4 years, or any bruising in a pre-mobile infant, warrants child-protection assessment). [12]
Management — Resuscitation
The resuscitation phase is governed by a single question: is this child unwell, or is there a red flag? If the answer is yes, the rash is secondary - you resuscitate and treat the threat first, and name the diagnosis afterwards. Start with ABCDE: secure the airway and give oxygen, establish intravenous or intraosseous access, take cultures, and treat sepsis and shock with parenteral antibiotics and fluid boluses per your local paediatric sepsis protocol. [7]
The unwell purpuric child is presumed to have meningococcaemia until proven otherwise. Give oxygen and a parenteral third-generation cephalosporin (for example ceftriaxone or cefotaxime) without waiting for the rash to evolve, take blood cultures and a meningococcal PCR, and manage shock with fluids; retrieve to a paediatric centre early. Antibiotic choice and dosing follow your local paediatric sepsis guideline, and the priority is speed, not diagnostic certainty. [7]
Empirical sepsis antibiotics in the unwell purpuric child
Dose
Parenteral third-generation cephalosporin (e.g. ceftriaxone or cefotaxime) IV, given immediately after cultures - exact agent, dose and frequency per local paediatric sepsis protocol
For Stevens-Johnson syndrome and toxic epidermal necrolysis, stop the suspected culprit drug immediately, provide fluid, electrolyte and temperature support, give aseptic skin and wound care, and involve ophthalmology (to prevent adhesions and corneal damage), dermatology, and the burns or PICU team. For staphylococcal scalded skin syndrome, fluid and temperature support, skin care and an anti-staphylococcal antibiotic are the core of management, with most cases managed supportively. For necrotising fasciitis, the treatment is urgent surgical exploration and debridement alongside broad-spectrum antibiotics - time is tissue. [9] [10]
Management — Definitive & Stepwise
Once the child is well and the red flags are excluded, definitive management is cause-specific and is the subject of the dedicated pages in this domain. The approach page's job is to point you to the right pathway, not to reproduce every treatment in full. The framework is the same each time: treat the cause, relieve the symptoms, prevent complications, and safety-net. [1]
For atopic dermatitis, the backbone is generous, daily emollients plus a stepwise topical corticosteroid ladder matched to severity and site - and explicitly addressing corticosteroid phobia, which is the commonest reason eczema is undertreated. For impetigo, a localised case is managed with a topical antibiotic (mupirocin or fusidic acid per local guidance); widespread or severe disease needs an oral anti-staphylococcal and streptococcal agent. For urticaria, a non-sedating oral antihistamine relieves the itch and wheals. For scabies, a scabicide is applied and all household contacts are treated on the same day. For molluscum contagiosum and viral warts, the default in a well child is watchful waiting, since most resolve spontaneously; active treatment is reserved for symptomatic, persistent or complicated lesions. [4] [6]
Treat the cause: emollients and topical corticosteroid for eczema; topical or oral antibiotic for impetigo; scabicide for scabies; antihistamine for urticaria; watchful waiting for molluscum and warts
Relieve symptoms: itch, pain, fever - and protect the skin barrier
Prevent complications: treat secondary infection; address corticosteroid phobia; ensure vaccine catch-up where relevant
Safety-net: give written advice on red flags that mandate return
Arrange follow-up: primary care for chronic rashes; paediatric or dermatology referral for uncertain, severe or persistent disease; ED or PICU for any deterioration
For Kawasaki disease, early treatment prevents coronary artery aneurysms: intravenous immunoglobulin 2 g/kg and aspirin are given within ten days of fever onset, with cardiology follow-up and echocardiography. This is the one dermatological-appearing emergency where the rash is the cue but the heart is the target, which is why recognising it is so high-yield. [8]
Specific Subtypes & Scenarios
Neonatal rash (0 to 28 days)
The neonate is the highest-stakes age band because benign, self-limiting eruptions sit side by side with life-threatening infection, and a small lesion can be the only clue. The benign eruptions are common and reassuring when recognised: erythema toxicum neonatorum (fleeting erythematous macules with central pale papules or pustules, present in many term babies), transient neonatal pustular melanosis (present at birth, leaves a fine scale and hyperpigmentation), milia (tiny white epidermal cysts on the nose), sebaceous gland hyperplasia, miliaria (heat rash), mongolian or congenital dermal melanocytosis (blue-grey patches over the sacrum), and seborrhoeic dermatitis (cradle cap). [2]
The danger in a neonate is infection. Any unwell neonate with vesicles, pustules, or non-specific erythema must be presumed to have neonatal herpes simplex (which can present with skin lesions, sepsis, or encephalopathy, sometimes with no skin lesions at all), staphylococcal infection including scalded skin syndrome, group B streptococcal or listeria sepsis, scabies, or congenital syphilis. The threshold to investigate and treat empirically is deliberately low: a septic screen including HSV PCR and empirical aciclovir is appropriate in the unwell neonate with an unexplained eruption. [3]
Acute febrile exanthem
The febrile child with a blanching maculopapular rash is the classic exam stem, and you distinguish the viral exanthems by their timeline, prodrome and spread: roseola (fever then rash as fever falls), erythema infectiosum (slapped cheek then reticulate rash), measles (prodrome and Koplik spots, head-to-toe spread), rubella, chickenpox (crops at different stages), hand-foot-and-mouth disease (oral and acral), and infectious mononucleosis (ampicillin-related rash if exposed). Always weigh a drug eruption and, above all, Kawasaki disease, which is defined by prolonged fever plus mucocutaneous features and is the one you cannot afford to miss. [5] [8]
Purpura in a well child
When the child is well, purpura and petechiae are less often sepsis and more often immune thrombocytopenia (isolated low platelets in an otherwise well child), IgA vasculitis (palpable purpura on the lower limbs and buttocks with abdominal pain, arthritis or renal involvement), or trauma and non-accidental injury. A full blood count, film and coagulation profile sort most of these out; the key is that "well" is a clinical judgement, and any deterioration reopens the sepsis question. [12]
Atopic dermatitis and adolescence
Atopic dermatitis is the archetype of the eczematous, itchy, flexural eruption and is covered in depth in its own page; in adolescence the emphasis shifts to acne vulgaris, seborrhoeic and contact dermatitis, psoriasis, and drug eruptions, with attention to psychosocial impact, adherence and confidentiality. [11]
Complications & Pitfalls
When a rash goes wrong, it usually does so in one of three ways: the broken skin gets infected, a streptococcal sore triggers a delayed immune attack on the kidneys or heart, or a severe blistering eruption leaves scars and adhesions. Secondary infection is the commonest: eczema and scabies become impetiginised, and any broken skin can be seeded by staphylococci or streptococci. Post-streptococcal sequelae follow group A streptococcal skin infection, driving post-streptococcal glomerulonephritis and, in high-risk communities, acute rheumatic fever - which is why a skin infection is never "just a skin infection" in remote ANZ. Scarring, pigment change and adhesions follow the severe blistering disorders, especially the ocular complications of SJS. [4] [9]
The pitfalls are where exams are won and lost, and most are cognitive errors rather than knowledge gaps. The first is diagnosis by colour - trusting a red impression instead of describing morphology and distribution. The second is missing purpura in deeply pigmented skin, where you must look carefully and palpate. The third is over-diagnosing drug allergy from a coincidental viral exanthem, which creates a lifelong inaccurate label. The fourth is confusing SSSS with TEN: both blister and have a positive Nikolsky sign, but SSSS is superficial and spares mucosa while TEN is full-thickness and involves mucosa. The fifth is missing incomplete Kawasaki in a child who does not meet the full criteria. The sixth is attributing bruising to trauma and missing non-accidental injury in a pre-mobile infant. The seventh is missing scabies because the burrows are subtle. And the eighth is corticosteroid phobia, which is the commonest reason eczema is undertreated. [11]
Prognosis & Disposition
Most paediatric rashes are benign and self-limiting, and a confident, safety-netted disposition back to primary care is the right answer far more often than admission. Disposition is decided by the sick-or-well assessment and the red flags, not by the name of the rash: a well child with a clearly benign eruption goes home with written advice; an unwell child, a neonate, or any child with purpura, widespread blistering or Kawasaki features is managed in hospital with the appropriate specialty input. [1]
The emergency eruptions need the right environment: meningococcaemia and sepsis need PICU and retrieval; SJS/TEN and extensive SSSS need burns, dermatology and ophthalmology involvement; necrotising fasciitis needs the surgeon now; and Kawasaki needs cardiology and IVIG within ten days. Chronic rashes - eczema, psoriasis, acne - need longitudinal care in primary care and specialist clinics, with education, adherence support and a clear plan for flares. Whatever the disposition, every child leaves with a safety-net: written red-flag advice and a clear pathway back. [9] [11]
Special Populations
The neonate carries the highest stakes, because benign mimics and life-threatening infection overlap; keep the threshold for a septic screen, HSV PCR and empirical aciclovir low in any unwell neonate with an eruption. The immunocompromised child may have atypical, muted or disseminated disease and needs a lower threshold for investigation and specialist input - a "minor" rash can be a major problem. In deeply pigmented skin, erythema and purpura are subtler, so use good lighting and palpation and do not be falsely reassured. [3]
In Indigenous, remote and tropical communities, scabies and group A streptococcal impetigo are hyperendemic and drive post-streptococcal glomerulonephritis and acute rheumatic fever, so a skin infection carries public-health weight - screening and treating household contacts, and linking to regional skin-health programs, is part of the management. The adolescent brings acne with its psychosocial burden, plus confidentiality and self-management considerations. And children who are atopic, complex-chronic or technology-dependent often have severe eczema, recurrent infection and disrupted skin flora that need a coordinated, longitudinal plan. [4] [11]
Evidence, Guidelines & Regional Differences
The approach is consistent across regions, but the operational details differ by jurisdiction. In the United Kingdom, NICE guideline NG143 governs the assessment of fever in under-fives and CG57 governs atopic eczema in children; the UK Health Security Agency publishes rash-and-fever guidance for outbreak settings. In Australia and Aotearoa New Zealand, the Royal Children's Hospital Melbourne clinical practice guidelines cover exanthems and eczema, and ASCIA governs the management of anaphylaxis and allergic rashes, including the autoinjector weight bands. In the United States, the American Academy of Dermatology publishes atopic dermatitis guidelines and the American Academy of Pediatrics Red Book governs exanthem and vaccine-preventable disease management. The World Health Organization Integrated Management of Childhood Illness algorithm includes a rash branch used in resource-limited settings worldwide. [1]
In remote and Indigenous ANZ communities, scabies and group A streptococcal impetigo are hyperendemic. A single painful skin sore is a population-health issue: alongside individual treatment, screen and treat household contacts, consider intramuscular benzathine benzylpenicillin for streptococcal skin infection where indicated, and link to regional skin-health and acute rheumatic fever prevention programs. ASCIA autoinjector weight bands are used for community-held adrenaline: 150 micrograms for 7.5 to 20 kg, 300 micrograms for 20 to 30 kg, and 500 micrograms for over 30 kg. [4]
Drug choices for impetigo vary: topical mupirocin or fusidic acid for localised disease, oral flucloxacillin, dicloxacillin or cephalexin for widespread disease, and intramuscular benzathine benzylpenicillin in remote ANZ settings for streptococcal skin infection and acute rheumatic fever prevention. Antibiotic stewardship and rising resistance shape these choices, which is why naming your local guideline matters. Controversies include whether routine topical antibiotic or antiseptic is preferred for impetigo, how long to treat, when to biopsy an uncertain rash, and how to manage uncomplicated molluscum, where evidence supports expectant management in most children. [4] [6]
Exam Pearls
A small set of facts separates a pass from a distinction on this topic. Blanching separates erythema and urticaria from purpura - it is the single highest-yield bedside test, and the glass slide costs nothing. The Nikolsky sign is positive in both SSSS and SJS/TEN, but the cleavage plane differs: SSSS splits superficially (subcorneal, flaccid clear fluid, flexural accentuation, no mucosal involvement) while SJS/TEN shows full-thickness epidermal necrosis with prominent mucosal involvement. [9] [10]
Remember the one-liners. Kawasaki: fever for five days or more plus mucocutaneous features, treat with IVIG 2 g/kg and aspirin within ten days. Chickenpox: crops of lesions at different stages simultaneously. Roseola: high fever for three to five days, then the rash appears as the fever falls. Erythema infectiosum: "slapped cheek" then reticulate rash, parvovirus B19, fetal risk in pregnancy. Meningococcaemia: any unwell child with a non-blanching rash is presumed to have it - treat first, investigate after. Henoch-Schonlein purpura: palpable purpura on the lower limbs and buttocks with abdominal pain, arthritis and renal involvement. And the trap that catches the unprepared: neonatal herpes can present without any skin lesion at all, so a low threshold to test and treat is part of safe neonatal care. [3] [8] [12]
References
- [1]Jalalabadi F Common Pediatric Skin Lesions: A Comprehensive Review of the Current Literature. Seminars in plastic surgery, 2016.PMID 27478417
- [2]Chadha A Common Neonatal Rashes. Pediatric annals, 2019.PMID 30653638
- [3]Wilson JL Neonatal Dermatology. Primary care, 2025.PMID 40835282
- [4]Hartman-Adams H Impetigo: diagnosis and treatment. American family physician, 2014.PMID 25250996
- [5]Saguil A Hand-Foot-and-Mouth Disease: Rapid Evidence Review. American family physician, 2019.PMID 31573162
- [6]Meza-Romero R Molluscum contagiosum: an update and review of new perspectives in etiology, diagnosis, and treatment. Clinical, cosmetic and investigational dermatology, 2019.PMID 31239742
- [7]Thompson MJ Clinical recognition of meningococcal disease in children and adolescents. Lancet (London, England), 2006.PMID 16458763
- [8]Rife E Kawasaki Disease: an Update. Current rheumatology reports, 2020.PMID 32924089
- [9]Ramien ML Stevens-Johnson syndrome in children. Current opinion in pediatrics, 2022.PMID 35836393
- [10]Brazel M Staphylococcal Scalded Skin Syndrome and Bullous Impetigo. Medicina (Kaunas, Lithuania), 2021.PMID 34833375
- [11]Guttman-Yassky E Atopic dermatitis. Lancet (London, England), 2025.PMID 39955121
- [12]Leung AKC Henoch-Schonlein Purpura in Children: An Updated Review. Current pediatric reviews, 2020.PMID 32384035