Paeds · paediatric-dermatology
Congenital melanocytic naevi and pigmentary birthmarks
Also known as congenital melanocytic naevus · congenital melanocytic nevus · giant congenital melanocytic naevus · bathing trunk naevus · cafe-au-lait macule · dermal melanocytosis · Mongolian spot · nevus of Ota · nevus depigmentosus · neurocutaneous melanocytosis · satellite nevi · NRAS mosaicism
A fellowship approach to the congenital pigmentary birthmarks, built around the single decision that matters: separating the common benign lesion — the dermal melanocytosis, the isolated cafe-au-lait macule, and the small congenital melanocytic naevus — from the high-risk lesion that demands the specialist service. The page covers the size-based classification of the congenital melanocytic naevus (CMN) by the projected adult size, the size-risk relationship that concentrates the melanoma risk in the large and the giant CMN, the postzygotic NRAS mosaicism that produces the CMN and the neurocutaneous melanocytosis as a single neural-crest event, the recognition of the child at risk of the neurocutaneous melanocytosis, the differential of the cafe-au-lait macule of the NF1 and the McCune-Albright, the dermal melanocytosis mistaken for the bruise, and the ash-leaf macule of the tuberous sclerosis, and the surveillance and the management from the observation and the baseline photography to the surgery and the laser.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A six-week-old girl is brought to the general practitioner by her mother, who has noticed a large dark-brown patch covering most of the upper back since birth. The patch is well-defined, slightly raised, and covered with fine dark hair, and there are about a dozen smaller dark-brown spots scattered over the rest of the back and the shoulders. The girl was born at term, she is feeding and growing well, and her development is on track. On examination, the patch on the upper back measures fourteen by sixteen centimetres and sits over the thoracic spine, with the surrounding satellite nevi over the back, the shoulders, and the upper arms. The head circumference is on the fiftieth centile, the fontanelle is soft, and the neurological examination is normal. This is a large congenital melanocytic naevus on the posterior axis with multiple satellite nevi — the pattern that raises the concern for the neurocutaneous melanocytosis and warrants the referral to the specialist CMN service and the consideration of the CNS imaging. [2] [6]
Size decides the risk — the CMN classification you can recite
Overview & Definition
The congenital pigmentary birthmarks are the coloured skin lesions present at birth or appearing within the first year of life, and they are among the commonest findings of the newborn and the infant skin examination. The group spans the benign and the commonplace — the dermal melanocytosis of the Mongolian spot that fades by the age of four, the isolated cafe-au-lait macule, and the small congenital melanocytic naevus — to the rare and the serious — the giant congenital melanocytic naevus with the neurocutaneous melanocytosis, and the syndromic pigmentary pattern of the neurofibromatosis type 1. The skill of the paediatric clinician is to recognise the lesion, to stratify the risk, and to identify the small number of children who need the specialist service and the surveillance. [10]
The congenital melanocytic naevus (CMN) is the hamartomatous proliferation of the melanocytes that is present at birth or appears within the first year as the tardive CMN. It is the lesion that carries the melanoma risk, and that risk is the reason the CMN is distinguished from the other pigmentary birthmarks and managed with the surveillance. The CMN is classified by the size — and specifically by the projected adult size, the size the lesion will reach when the child is fully grown — because the size is the single strongest correlate of the melanoma risk and of the risk of the neurocutaneous melanocytosis. [1] [2]
The clinical importance of the pigmentary birthmarks lies in three things. The first is the melanoma risk of the CMN, which is concentrated in the large and the giant lesions and which shapes the surveillance. The second is the neurocutaneous melanocytosis, the rare complication of the large posterior-axis CMN with the satellites, in which the melanocytes populate the leptomeninges and carry the risk of the hydrocephalus and the melanoma of the central nervous system. The third is the syndromic significance of the cafe-au-lait macule and the hypopigmented macule, which point to the neurofibromatosis type 1, the McCune-Albright syndrome, and the tuberous sclerosis when the pattern is recognised. [6] [10]
Classification
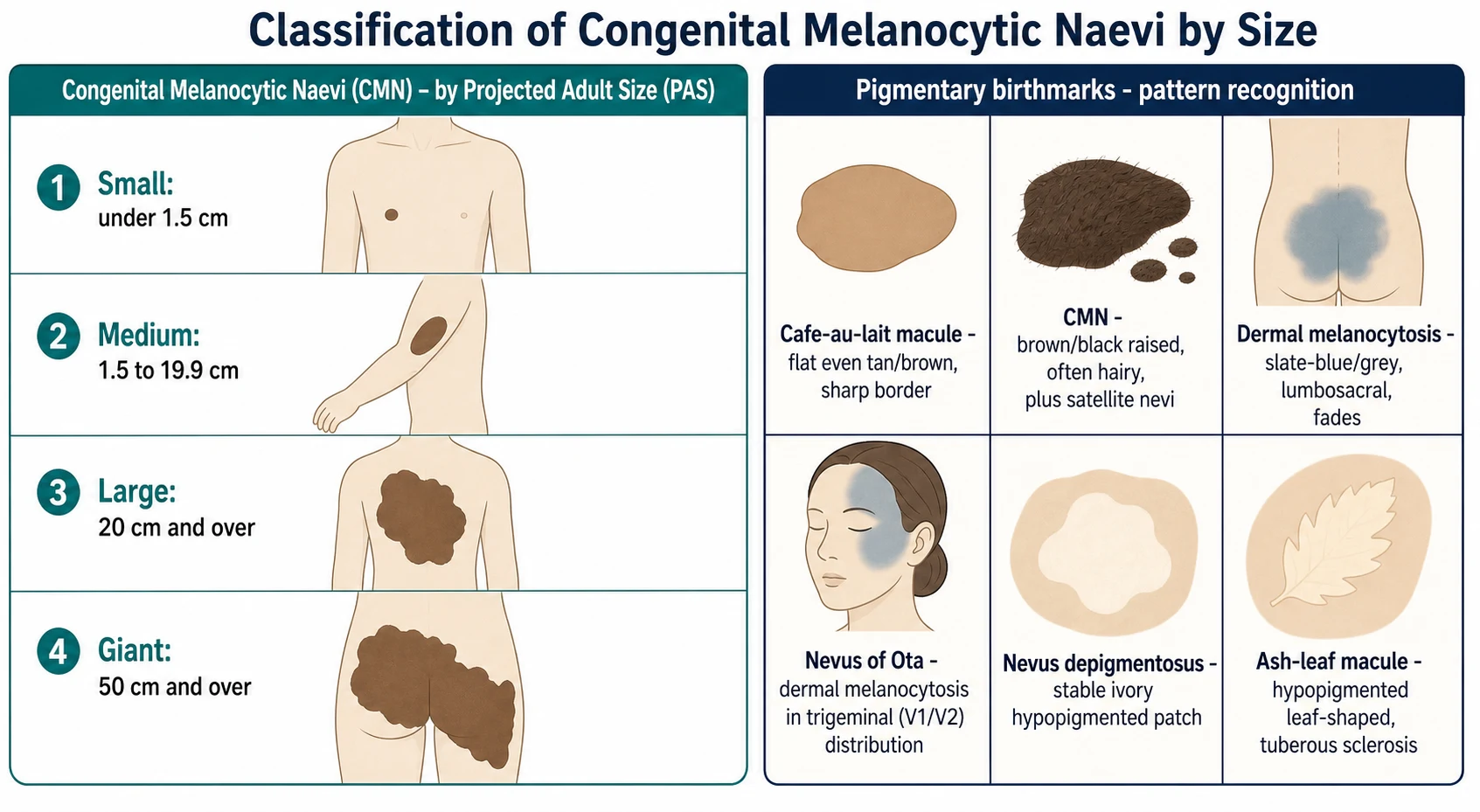
The classification of the congenital pigmentary birthmarks follows the cell of origin and the clinical morphology, and the CMN is further classified by the size, because the size is the correlate of the risk. The CMN is the melanocytic lesion — the brown to the black, the raised, the often hairy plaque — and it is separated from the cafe-au-lait macule (the flat, the evenly pigmented, the sharply bordered patch), the dermal melanocytosis (the slate-blue to the grey, the lumbosacral patch), the nevus of Ota (the dermal melanocytosis in the trigeminal distribution), the nevus depigmentosus (the stable ivory hypopigmented patch), and the ash-leaf macule (the hypopigmented leaf-shaped patch of the tuberous sclerosis). [10] [11]
The size classification of the CMN is the one the fellowship candidate must recite. The Krengel 2013 categorization standardised the assessment of the cutaneous features of the CMN, and the size is measured as the projected adult size — the largest diameter the lesion is predicted to reach in the adult, derived from the body-site-specific growth factors applied to the size at birth or at presentation. The small CMN is under 1.5 cm, the medium CMN is 1.5 to 19.9 cm, the large CMN is 20 cm and over, and the giant CMN is 50 cm and over. The size category decides the level of the surveillance, the need for the specialist referral, and the consideration of the CNS imaging. [2] [4]
The classification also captures the anatomic distribution and the number of the lesions. The single CMN is the common presentation, and the multiple CMN — the large or the giant lesion with the scattered smaller satellite nevi — defines the CMN syndrome, the pattern that carries the elevated risk of the neurocutaneous melanocytosis when the large lesion sits on the posterior axis (the head, the neck, or the spine). The colour heterogeneity, the surface nodularity, and the hairiness are the other features recorded, because they describe the lesion and they flag the nodule that may warrant the biopsy. [2] [9]
The pigmentary birthmarks — the distinguishing features
Congenital melanocytic naevus (CMN)
Cafe-au-lait macule (CALM)
Dermal melanocytosis (Mongolian spot)
Nevus depigmentosus / ash-leaf macule
Epidemiology & Risk Factors
The CMN is one of the commonest birthmarks. The small CMN is found in about one percent of the newborns, and it is the lesion the general paediatrician meets in the routine practice. The medium CMN is less common, and the large and the giant CMN are rare — the large CMN at roughly one in twenty thousand and the giant CMN at roughly one in fifty thousand live births — and they become the specialist referral. The dermal melanocytosis and the isolated cafe-au-lait macule are far commoner still, and the dermal melanocytosis is present in the great majority of the infants of the Asian, the Indigenous, and the darker-skin-type heritage. [5] [10]
The melanoma risk is the central epidemiological fact, and it is strongly correlated with the size of the CMN. The Krengel 2017 review of the melanoma risk in the congenital melanocytic naevi established that the risk is concentrated in the large and the giant CMN, and that the small and the medium CMN carry a melanoma risk close to the population risk. The melanoma in the large and the giant CMN tends to arise in the childhood and the adolescence, which is the reason the surveillance is concentrated in the first two decades, and it may arise in the skin, in the central nervous system in the neurocutaneous melanocytosis, or rarely in the extracutaneous site. [1] [7]
The neurocutaneous melanocytosis is the complication that defines the highest-risk group. The risk is concentrated in the child with the large or the giant CMN on the posterior axis — the head, the neck, or the spine — particularly when there are many satellite nevi, and it is low in the child with the CMN on the limbs or the anterior trunk. The symptomatic neurocutaneous melanocytosis, with the signs of the raised intracranial pressure or the seizures, carries a poor prognosis, and this is the group that warrants the CNS imaging and the neurology. [6] [5]
Pathophysiology
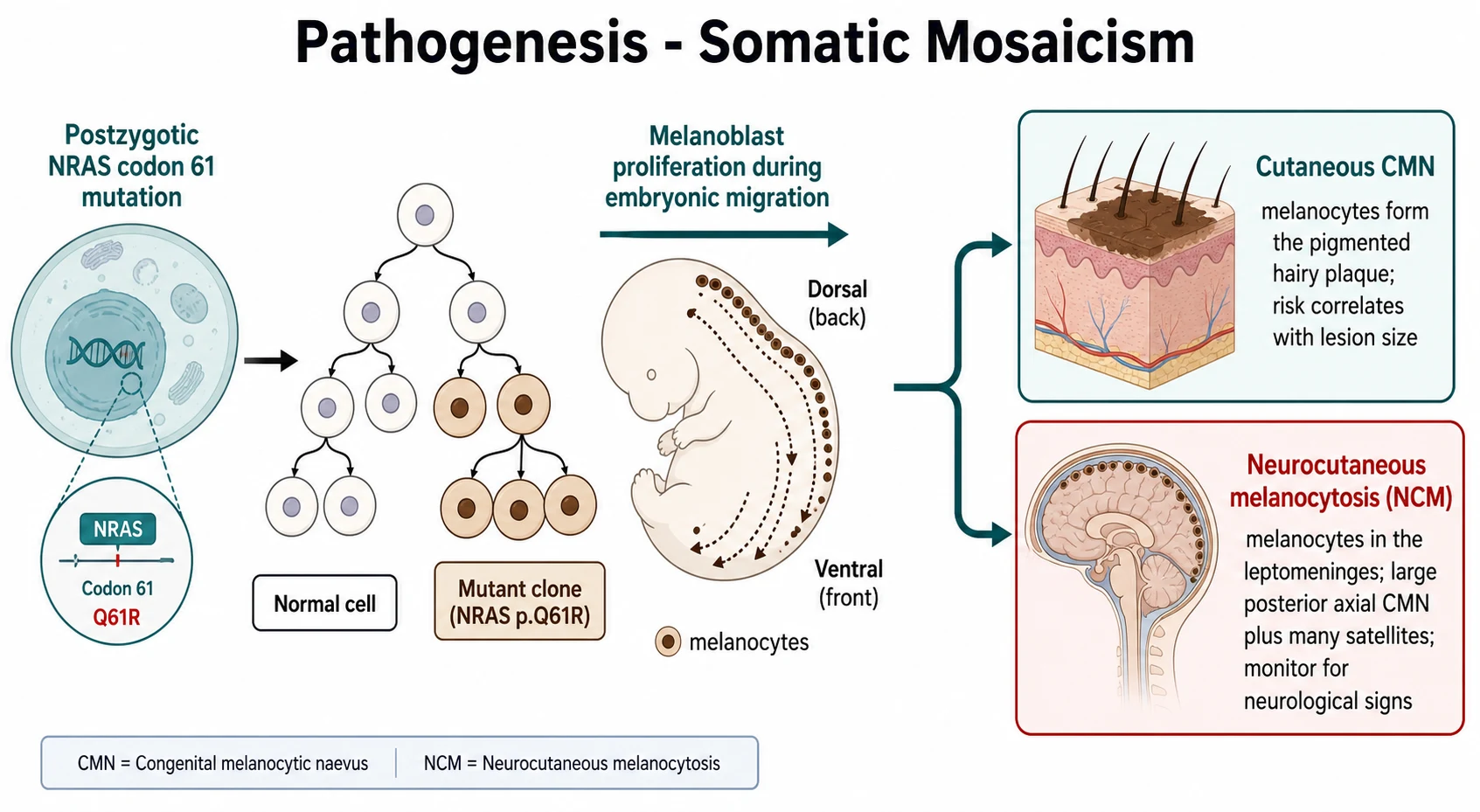
The pathophysiology of the CMN is the somatic (postzygotic) mosaicism in the melanocyte lineage, and it is the single mechanism that explains the cutaneous CMN, the satellite nevi, and the neurocutaneous melanocytosis as one developmental event. Kinsler and colleagues showed in 2013 that the multiple congenital melanocytic nevi and the neurocutaneous melanocytosis are caused by the postzygotic mutations in the codon 61 of the NRAS gene, and the mutation arises in a melanocyte precursor during the embryonic development. The earlier and the more extensive the mutation, the larger the cutaneous lesion, the more numerous the satellites, and the greater the chance of the leptomeningeal involvement — because the neural crest gives rise to both the skin melanocytes and the melanocytes of the central nervous system. [6]
The dermal melanocytosis has a different mechanism at the bedside but the same embryological root. During the development, the melanoblasts migrate from the neural crest along the dorsolateral pathway to their final destination in the epidermis. In the dermal melanocytosis, a subpopulation of the melanocytes fails to complete the migration and comes to rest in the dermis, where the pigment sits deep to the surface. The slate-blue or the grey colour is the optical effect — the Tyndall effect — of the melanin viewed through the overlying skin, in the same way that the deep blood vessels appear blue. The lesion fades as the melanocytes are gradually lost or the pigment is dispersed over the first years of life. [10]
The cafe-au-lait macule is the lesion of the increased melanogenesis without the increase in the melanocyte number. The basal keratinocytes produce more melanin, and the macule is flat, evenly pigmented, and sharply bordered because the increased pigment is uniform across the patch. The RAS-MAPK pathway links the cafe-au-lait macule to the syndromes: the neurofibromatosis type 1 is caused by the loss of the NF1 gene (the neurofibromin, a RAS-GAP), and the McCune-Albright syndrome is caused by the postzygotic GNAS mutation that constitutively activates the Gs-alpha and the cAMP pathway downstream. [10] [11]
The melanoma arises in the CMN through the acquisition of the additional genetic hits on the background of the NRAS-mutant clone, and it may arise in the cutaneous naevus, in the central nervous system in the neurocutaneous melanocytosis, or rarely in the extracutaneous site such as the retroperitoneum. This distribution is the biological reason that the prophylactic excision of the cutaneous CMN cannot eliminate the melanoma risk — the melanoma may arise in the residual naevus cells, in the satellites, or in the central nervous system — and it is the principle that places the surveillance, rather than the routine excision, at the centre of the management. [1] [3]
Clinical Presentation
The typical CMN presents as the brown to the black, the well-defined, the often hairy plaque present at birth. The colour varies from the light brown to the near-black, and it may be heterogeneous within the single lesion. The surface may be smooth, pebbly, or nodular, and the larger lesions tend to be more nodular and more hairy. The hairiness is a characteristic feature — the lesion is often covered with the darker, the coarser, the terminal hair that distinguishes it from the non-melanocytic macule. The small CMN is the common, the stable, the solitary lesion; the large and the giant CMN is the garment-like lesion over the trunk (the bathing-trunk naevus) or the limb, with the surrounding satellite nevi, and it carries the cosmetic and the psychosocial burden that the clinician must address. [2] [9]
The cafe-au-lait macule presents as the flat, the evenly tan to the light-brown patch with the smooth and the sharp border, present from the birth or the early childhood. It is the homogenous colour and the regular border that distinguish the typical NF1 macule from the irregular, the jagged coast-of-Maine border of the McCune-Albright macule. The number and the size are recorded at every visit, because the six or more macules over the five millimetres before the puberty (over the fifteen millimetres after the puberty) is the NIH criterion for the neurofibromatosis type 1. [10]
The dermal melanocytosis, the Mongolian spot, presents as the slate-blue to the grey patch over the lumbosacral area, the buttocks, or the shoulders, present at birth and fading by the age of the two to the four years. It is common in the infants of the Asian, the Indigenous, the African, and the darker-skin-type heritage, and it is the lesion that must be documented in the medical record at the newborn examination, because the slate-blue patch can be mistaken for the bruise and the misdiagnosis of the non-accidental injury is the harm the clinician prevents. The nevus of Ota is the dermal melanocytosis in the distribution of the trigeminal nerve (the V1 and the V2), the unilateral slate-brown to the blue-grey discolouration of the periorbital skin, and it persists and carries the lifelong risk of the glaucoma and the melanoma. [10]
Differential Diagnosis
The differential of the congenital pigmentary birthmark is the first place the clinician looks when the lesion does not fit the simple pattern. The CMN is separated from the acquired melanocytic naevus by the presence at the birth or in the first year, the larger size, and the hairiness. The cafe-au-lait macule is separated from the CMN by the flatness and the even pigment — the CMN is raised and often hairy, and the cafe-au-lait is a flat macule. The dermal melanocytosis is separated by the slate-blue to the grey colour and the lumbosacral location, and the nevus of Ota by the trigeminal distribution. [10] [11]
The cafe-au-lait macule itself has the differential the fellowship candidate must hold. The isolated macule is the benign finding, and it requires no investigation. The six or more macules over the five millimetres before the puberty (over the fifteen millimetres after the puberty) meet the NIH criterion for the neurofibromatosis type 1, and the assessment proceeds to the search for the axillary and the inguinal freckling, the Lisch nodules on the slit-lamp, the neurofibromas, and the family history. The McCune-Albright macule is larger, fewer, and has the irregular coast-of-Maine border, and it accompanies the fibrous dysplasia and the endocrine overactivity (the precocious puberty) of the McCune-Albright syndrome. [10]
The child-protection distinction is the one the fellowship candidate must hold for the dermal melanocytosis. The slate-blue patch of the Mongolian spot over the lumbosacral area can be mistaken for the bruise, and the mistake is the harm of the false allegation of the non-accidental injury. The dermal melanocytosis is present at the birth, it is macular and non-tender, it sits over the lumbosacral area, and it fades over the first years. The documentation of the lesion in the medical record at the newborn examination, and the recognition of the pattern in the darker-skin-type infant, are the safeguards against the misdiagnosis. The bruise of the non-accidental injury, by contrast, is the tender, the evolving, the patterned lesion that does not fit the dermal melanocytosis distribution. [10]
The hypopigmented birthmark has its own differential. The nevus depigmentosus is the stable, the hypopigmented (but not depigmented) patch from the birth, and it is the isolated and the benign lesion. The ash-leaf macule is the hypopigmented, the leaf-shaped or the confetti macule that is the earliest cutaneous sign of the tuberous sclerosis, and the finding warrants the Wood's lamp examination (the macules are enhanced), the assessment for the other features of the tuberous sclerosis (the angiofibromas, the shagreen patch, the seizures, the developmental delay), and the consideration of the genetics referral. The segmental vitiligo is the acquired, the progressive, the depigmented (not hypopigmented) lesion, and it is distinguished by the history of the progression. [11]
Clinical & Bedside Assessment
The assessment of the congenital pigmentary birthmark begins with the recognition — the distribution, the colour, the border, the surface, and the presence at the birth. The lesion is examined in the good light, and the clinician looks for the four features that classify the melanocytic lesion: the colour (the brown to the black), the border (the well-defined and the regular), the surface (the raised and the often hairy), and the presence at the birth or in the first year. The size is measured — the largest diameter at the present, and the projected adult size derived from the body-site-specific growth factor — and the location, the colour, the surface features, the hairiness, and the number and the location of the satellite nevi are recorded. [2] [4]
The examination of the child with the large or the giant CMN extends beyond the skin. The head circumference is measured and plotted, because the hydrocephalus of the neurocutaneous melanocytosis may present with the macrocephaly. The developmental assessment is performed, and the neurological examination checks for the signs of the raised intracranial pressure, the seizures, the focal deficit, and the developmental regression. The location of the large lesion is noted — the posterior axis (the head, the neck, the spine) is the high-risk distribution, and the anterior trunk and the limbs are the lower-risk distribution — and the number of the satellite nevi is counted, because the multiple satellites with the large posterior-axis lesion define the highest-risk pattern for the neurocutaneous melanocytosis. [6] [5]
The examination of the child with the cafe-au-lait macules is the full skin examination with the count. The macules are counted and measured — the number and the largest diameter of each — and the examination extends to the search for the axillary and the ingueral freckling, the cutaneous neurofibromas, and the Lisch nodules (the iris hamartomas seen on the slit-lamp examination). The growth, the development, the blood pressure, and the spine are examined, because the neurofibromatosis type 1 affects the growth, the learning, the vasculature, and the spine. The family history of the NF1, the McCune-Albright, or the tuberous sclerosis is taken when the syndromic pattern is suspected. [10]
Investigations
The diagnosis of most congenital pigmentary birthmarks is clinical, and no investigations are required in the typical small CMN, the isolated cafe-au-lait macule, or the dermal melanocytosis. The distribution, the colour, the border, the surface, and the presence at the birth are sufficient to make the diagnosis and to choose the management. The baseline photography and the dermoscopy are the investigations that establish the baseline for the lifelong surveillance of the CMN, and they are the tools that document the lesion and the change over the time. [3] [4]
The magnetic resonance imaging (MRI) of the brain and the spine is the investigation that screens for the neurocutaneous melanocytosis, and it is reserved for the high-risk pattern. The large or the giant CMN on the posterior axis (the head, the neck, or the spine) with the multiple satellite nevi, and any CMN with the neurological signs (the macrocephaly, the seizures, the developmental delay, the signs of the raised intracranial pressure), are the indications for the MRI. The shift in the contemporary practice is toward the selective imaging — the imaging of the high-risk pattern and the symptomatic child — rather than the routine imaging of every large CMN, because the detection of the clinically silent leptomeningeal melanocytosis does not always change the management and the imaging carries the sedation and the anaesthesia burden in the infant. The decision is made with the specialist CMN service and the neurology. [6] [3]
The biopsy is indicated for the changing or the nodular area within a CMN. The new nodule, the colour change, the bleeding, or the rapid growth within the CMN raises the concern for the melanoma, and the biopsy — or the excision — is the investigation that distinguishes the melanoma from the benign proliferative nodule (the common, the benign, the organising nodule within the large CMN). The benign proliferative nodule is the frequent finding in the large CMN in the first months of life, and the clinician who recognises it avoids the unnecessary alarm, but the changing lesion in the older child demands the assessment. The neurofibromatosis type 1 is confirmed by the clinical NIH criteria and the slit-lamp examination, with the genetic testing when the diagnosis is uncertain. [7] [8]
Management — Resuscitation
The management of most congenital pigmentary birthmarks does not demand a resuscitation. The child is well, and the condition is a skin lesion, not a systemic illness, in the great majority. The resuscitative principle is the prompt recognition of the time-critical presentations — the melanoma within the CMN, and the symptomatic neurocutaneous melanocytosis — because these are the scenarios that demand the urgent referral. [1] [7]
The melanoma within the CMN is the time-critical cutaneous presentation. The rapidly enlarging nodule, the colour change, the bleeding, or the ulceration within a CMN demands the urgent referral to the specialist CMN service or the paediatric oncology, and the biopsy or the excision. The melanoma risk is concentrated in the childhood in the large and the giant CMN, and the index of the suspicion is the higher in the first two decades. [7] [8]
The symptomatic neurocutaneous melanocytosis is the neurological emergency. The child with the large posterior-axis CMN who develops the headache, the vomiting, the seizure, the developmental regression, the hydrocephalus, or the focal deficit has the raised intracranial pressure or the leptomeningeal involvement, and the urgent neurology, the urgent neuroimaging, and the management of the intracranial pressure are the priorities. The symptomatic neurocutaneous melanocytosis carries the poor prognosis, and the palliative and the supportive care may be the role when the prognosis is established. The itch and the discomfort of the larger CMN are managed with the emollients and the topical measures, and the oral analgesia with the paracetamol at fifteen milligrams per kilogram per dose is added when the discomfort is significant. [6] [9]
Management — Definitive & Stepwise
The definitive management of the CMN is built from four elements, applied in the sequence that matches the size and the risk: the observation and the surveillance, the surgery, the laser, and the psychosocial support. The small and the medium CMN are managed with the observation, the baseline photography, the dermoscopy, the education on the self-examination and the change, and the lifelong skin checks — and the observation is the mainstay, because the melanoma risk is close to the population risk and the prophylactic excision does not eliminate it. The family is counselled on the sun protection, the change that must prompt the review, and the realistic expectation of the lesion over the time. [3] [4]
The surgery is the option for the selected CMN, and the decision is individualised rather than routine. The indications are the cosmetic and the psychosocial burden of the visible lesion, the functional impairment, and the difficult-to-monitor site — and the surgery is the choice of the family and the specialist service, not the default. The surgical options are the serial excision (the staged removal over the several procedures), the tissue expansion (the insertion of the expander to grow the extra skin for the closure), the skin grafting, and the neonatal curettage (the removal of the superficial naevus cells in the first two weeks of life, when the naevus cells are the more superficial and the skin is the more adherent). The surgery reduces the bulk and the colour of the lesion and it may ease the surveillance, but it cannot eliminate the melanoma risk, because the melanoma may arise in the residual cells, the satellites, or the central nervous system — and this is the principle the fellowship candidate must state. [3] [5]
The management of the congenital melanocytic naevus — the steps
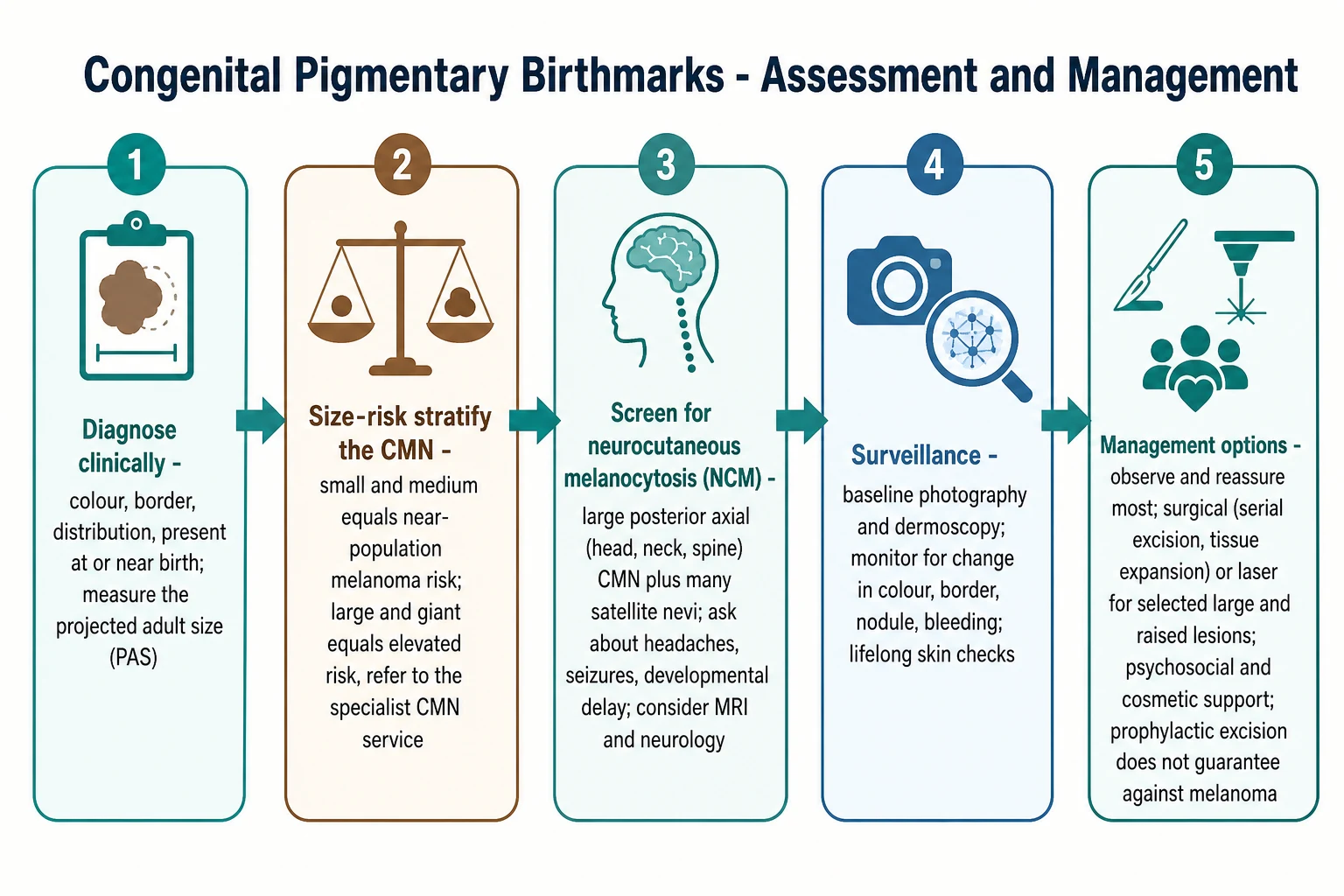
Recognise and classify the lesion: the colour, the border, the distribution, and the presence at the birth; measure the largest diameter and the projected adult size, and assign the size category (small under 1.5 cm, medium 1.5 to 19.9 cm, large 20 cm and over, giant 50 cm and over).
Stratify the risk: the small and the medium CMN carry the near-population melanoma risk and are managed in the primary care with the observation and the surveillance; the large and the giant CMN carry the elevated risk and are referred to the specialist CMN service.
Screen for the neurocutaneous melanocytosis in the high-risk pattern: the large or the giant CMN on the posterior axis (the head, the neck, or the spine) with the multiple satellite nevi, and any CMN with the neurological signs; consider the MRI and the neurology referral.
Establish the surveillance: the baseline photography and the dermoscopy at the presentation, the education on the self-examination and the change that must prompt the review, the sun protection, and the lifelong skin checks.
Consider the surgery or the laser for the selected case: the serial excision, the tissue expansion, the skin grafting, or the neonatal curettage for the cosmetic, the psychosocial, the functional, or the difficult-to-monitor indication; the pigment-specific laser for the lightening. Individualise the decision with the specialist service; never the routine prophylactic excision as the melanoma guarantee.
Provide the psychosocial support: the counselling of the family on the risk, the realistic expectation, and the cosmetic burden; the peer and the support-group linkage for the child with the visible CMN; and the transition to the adult care in the adolescence.
The laser is the option for the lightening of the CMN and the cafe-au-lait macule, and it is the pigment-specific Q-switched and the picosecond lasers that target the melanin. The laser lightens the lesion rather than removing it, and the recurrence is common, so it is the cosmetic adjunct rather than the definitive treatment. The cafe-au-lait macule is managed with the reassurance for the isolated lesion, the NF1 assessment for the six or more, and the laser for the cosmetically significant lesions, with the realistic expectation of the partial response and the recurrence. The psychosocial support is the element the fellowship candidate names to demonstrate the whole-child care: the cosmetic burden of the visible CMN, the anxiety of the family about the melanoma, and the peer and the support-group linkage are the issues that shape the quality of the life of the child and the family. [9] [10]
Specific Subtypes & Scenarios
The small CMN in the primary care is the commonest scenario, and it is managed with the reassurance, the baseline photography, the education on the change, and the discharge to the routine skin checks. The melanoma risk is close to the population risk, the lesion is stable, and the family is counselled on the sun protection and the change that must prompt the review. The follow-up is unnecessary if the lesion remains stable, and the specialist referral is reserved for the changing or the atypical lesion. [1] [3]
The large and the giant CMN in the specialist CMN service is the scenario that demands the multidisciplinary approach. The assessment includes the baseline photography, the dermoscopy, the consideration of the MRI for the neurocutaneous-melanocytosis screening in the high-risk pattern, the surveillance for the melanoma and the hydrocephalus, and the surgery or the laser for the selected case. The psychosocial support — the counselling, the cosmetic burden, the peer linkage — is the integral element, because the visible CMN shapes the quality of the life and the self-image of the child and the family. The German CMN registry documented the clinical course, the treatment modalities, and the quality of the life in the patients with the CMN, and it is the contemporary evidence on the burden and the outcome. [9] [5]
In the Australia and the Aotearoa New Zealand, the large and the giant CMN are managed through the specialist paediatric dermatology services in the major paediatric centres, with the multidisciplinary input from the plastic surgery, the neurology, the psychology, and the genetics. The telehealth dermatology supports the assessment and the surveillance of the child in the rural and the remote setting, and the local photography and the coordinated retrieval bridge the distance. The Aboriginal and the Torres Strait Islander and the Maori children have the higher baseline prevalence of the dermal melanocytosis and the cafe-au-lait macule, and the culturally safe counselling and the documentation of the benign birthmark prevent the misdiagnosis. The public-system access funds the surgery and the laser where they are indicated. [10] [3]
The CMN syndrome with the neurocutaneous melanocytosis is the highest-risk scenario. The MRI screens for the leptomeningeal melanocytosis, the neurology monitors for the hydrocephalus and the seizures, and the surveillance extends to the melanoma of the skin and the central nervous system. The symptomatic neurocutaneous melanocytosis has the poor prognosis, and the palliative and the supportive care may be the role. The asymptomatic neurocutaneous melanocytosis detected on the MRI has the variable but the guarded course, and the shared decision with the family and the specialist service frames the surveillance. [6] [5]
The multiple cafe-au-lait macule presentation is the scenario that demands the NF1 assessment. The six or more macules over the five millimetres before the puberty (over the fifteen millimetres after the puberty) meet the NIH criterion, and the assessment proceeds to the slit-lamp examination for the Lisch nodules, the search for the axillary and the inguinal freckling and the neurofibromas, the developmental and the learning assessment, and the genetic counselling. The dermal melanocytosis is managed with the reassurance, the documentation in the medical record, and the review for the persistence beyond the age of the four or the aberrant location. The nevus of Ota is managed with the lifelong ophthalmology surveillance for the glaucoma and the melanoma risk, and the laser for the cosmesis. [10] [11]
Complications & Pitfalls
The complications of the CMN are the melanoma and the neurocutaneous melanocytosis. The melanoma presents as the changing nodule, the colour change, the bleeding, or the ulceration within the CMN, and it may arise in the cutaneous naevus, in the central nervous system in the neurocutaneous melanocytosis, or rarely in the extracutaneous site. The index of the suspicion is the higher in the large and the giant CMN and in the first two decades, and the biopsy or the excision of the changing lesion is the safeguard. [7] [8]
The pitfall of the over-treatment is the one the fellowship candidate names to demonstrate the restraint. The routine prophylactic excision of the small CMN does not eliminate the melanoma risk, because the melanoma may arise in the residual cells, the satellites, or the central nervous system, and it exposes the child to the surgical and the anaesthetic risk and the scarring. The observation and the surveillance, rather than the routine excision, are the mainstay for the small and the medium CMN, and the surgery is the individualised decision for the cosmetic, the functional, or the difficult-to-monitor indication. [3] [5]
The pitfall of the missed syndrome is the one that harms the child. The six or more cafe-au-lait macules missed as the isolated lesions delay the diagnosis of the neurofibromatosis type 1 and the developmental and the learning support. The hypopigmented ash-leaf macule missed as the isolated lesion delays the diagnosis of the tuberous sclerosis and the management of the seizures. The slate-blue dermal melanocytosis mistaken for the bruise is the harm of the false allegation of the non-accidental injury, and the documentation and the recognition prevent the misdiagnosis. [10] [11]
Prognosis & Disposition
The prognosis of the small and the medium CMN is benign. The melanoma risk is close to the population risk, the lesion is stable over the life, and the routine skin checks are the surveillance. The prognosis of the large and the giant CMN is the variable — the elevated melanoma risk concentrated in the childhood, the need for the specialist surveillance, and the variable cosmetic and the psychosocial outcome. The surgery and the laser may improve the appearance and the ease of the surveillance, and the psychosocial support shapes the quality of the life. [1] [9]
The prognosis of the symptomatic neurocutaneous melanocytosis is poor, with the high mortality from the hydrocephalus, the seizures, and the leptomeningeal melanoma, once the symptoms develop. The asymptomatic neurocutaneous melanocytosis detected on the MRI has the variable but the guarded course, and the shared decision with the family and the specialist service frames the surveillance. The dermal melanocytosis has the excellent prognosis — the fading by the age of the two to the four years for the great majority, and the persistence in the minority. [6] [10]
The disposition is the primary care for the small CMN, the isolated cafe-au-lait macule, and the dermal melanocytosis; the specialist CMN service for the large and the giant CMN and the suspected neurocutaneous melanocytosis; and the multidisciplinary care for the CMN syndrome and the syndromic pigmentary birthmarks. The long-term follow-up is the lifelong skin checks for the CMN, the ophthalmology for the nevus of Ota, and the developmental and the genetic surveillance for the neurofibromatosis type 1 and the tuberous sclerosis. [3] [11]
Special Populations
The infant with the giant CMN and the early neurocutaneous-melanocytosis risk is managed in the neonatal period with the multidisciplinary referral, the MRI, the neurology, and the family support. The early assessment and the establishment of the surveillance and the psychosocial support shape the outcome and the quality of the life. [5] [6]
The child with the neurofibromatosis type 1 and the multiple cafe-au-lait macules is managed with the developmental surveillance, the learning-support assessment, the ophthalmology, the blood-pressure monitoring, and the genetic counselling. The recognition of the NF1 from the cafe-au-lait macule count is the entry to the longitudinal care that addresses the growth, the learning, the vasculopathy, and the orthopaedic complications. [10]
The Indigenous and the darker-skin-type child with the dermal melanocytosis and the cafe-au-lait macule is managed with the recognition of the higher baseline prevalence, the documentation in the medical record, and the culturally safe counselling. The dermal melanocytosis is the expected finding in the great majority of the infants of the Asian, the Indigenous, the African, and the Polynesian heritage, and the over-investigation and the misdiagnosis as the bruise are the harms the recognition prevents. The adolescent with the visible CMN or the cafe-au-lait macule is managed with the psychosocial support, the cosmetic and the laser options, and the transition to the adult care. [10] [11]
The child in the rural and the remote setting with the large CMN is managed with the telehealth specialist consultation, the local photography and the dermoscopy, and the coordinated retrieval for the specialist assessment and the surgery. The family with the financial and the access barriers is supported through the public-system referral, the funded surgery and the laser where indicated, and the peer and the support-group linkage. [3] [9]
Evidence, Guidelines & Regional Differences
The evidence for the melanoma risk in the CMN is anchored in the Krengel 2017 review in the British Journal of Dermatology, "Melanoma risk in congenital melanocytic naevi." The review established that the melanoma risk is concentrated in the large and the giant CMN, that the small and the medium CMN carry a risk close to the population risk, and that the estimates carry the uncertainty of the historical and the selection bias. This is the evidence the fellowship candidate cites for the size-risk relationship that drives the surveillance. [1]
Krengel 2017 — melanoma risk in congenital melanocytic naevi
A comprehensive review of the melanoma risk in the congenital melanocytic naevi, appraising the historical and the contemporary data on the risk by the size category, the site, and the age, and the influence of the selection bias on the estimates.
Key finding
The melanoma risk is concentrated in the large and the giant CMN, with the risk elevated and the majority of the melanomas arising in the childhood and the adolescence. The small and the medium CMN carry a melanoma risk close to the population risk. The historical high estimates reflect the selection and the reporting bias, and the contemporary population data suggest a lower but the clearly elevated risk for the large and the giant lesions.
The Krengel 2013 categorization in the Journal of the American Academy of Dermatology standardised the assessment of the cutaneous features of the CMN — the size by the projected adult size, the number, the colour heterogeneity, the surface, and the anatomic distribution — and it is the framework the fellowship candidate follows at the bedside. The Price 2015 paper in the Pediatric Dermatology, "Practical application of the new classification scheme for congenital melanocytic nevi," translated the categorization into the clinical practice, and it is the reference for the measurement and the recording. [2] [4]
The Kinsler 2013 paper in the Journal of Investigative Dermatology established that the multiple CMN and the neurocutaneous melanocytosis are caused by the postzygotic mutations in the codon 61 of the NRAS, and it is the biological explanation for the size, the satellites, and the leptomeningeal involvement as the single mosaic event. The Caccavale 2021 study in the Dermatology and the Zalaudek 2020 study in the JAAD characterised the melanoma arising in the CMN and the dermoscopic features, and they are the references for the recognition of the melanoma within the CMN. [6] [7] [8]
The Wramp 2017 German CMN registry and the Oei 2021 international core-domain-set paper are the contemporary evidence on the clinical course, the treatment modalities, the quality of the life, and the standardisation of the outcome measurement in the CMN. The Arneja and Gosain 2007 review of the giant CMN in the Plastic and Reconstructive Surgery is the surgical reference. The Dohil 2000 and the Tey 2010 papers are the references for the pigmentary and the hypopigmented birthmarks. [9] [12] [5] [10] [11]
The regional differences are modest. The specialist CMN service model in the United Kingdom and the Europe concentrates the multidisciplinary care in the few centres, and the Australia and the Aotearoa New Zealand deliver the care through the major paediatric centres with the telehealth support for the rural and the remote. The access to the surgery and the laser varies, and the practice on the routine MRI for the asymptomatic large CMN has shifted toward the selective imaging of the high-risk pattern. The patient registries and the support organisations (the Naevus International and the national CMN support groups) shape the contemporary evidence and the family support. [12] [9]
Exam Pearls
The fellowship answer turns on five facts. The first is the size classification: the small under 1.5 cm, the medium 1.5 to 19.9 cm, the large 20 cm and over, the giant 50 cm and over — all by the projected adult size. The second is the size-risk relationship: the melanoma risk is concentrated in the large and the giant CMN, and the small and the medium carry the near-population risk. The third is the neurocutaneous melanocytosis: the large posterior-axis CMN (the head, the neck, the spine) with the multiple satellites is the high-risk pattern, and the symptomatic NCM carries the poor prognosis. The fourth is the management: the observation and the surveillance are the mainstay, and the prophylactic excision does not guarantee against the melanoma. The fifth is the syndromic recognition: the six or more cafe-au-lait macules of the NF1, the coast-of-Maine macule of the McCune-Albright, and the ash-leaf macule of the tuberous sclerosis. [1] [2] [10]
The three examiner traps are the following. The first is the routine prophylactic excision of the small CMN — it does not eliminate the melanoma risk, and the observation and the surveillance are the mainstay. The second is the over-reassurance of the changing lesion within a CMN — the melanoma risk is concentrated in the childhood, and the changing lesion demands the assessment. The third is the dermal melanocytosis mistaken for the bruise — the documentation and the recognition prevent the misdiagnosis of the non-accidental injury. [3] [7] [10]
The examiner rewards the candidate who frames the congenital pigmentary birthmark around the recognition, the size-risk stratification, the neurocutaneous-melanocytosis screening, and the surveillance. The size decides the risk; the posterior-axis location with the satellites raises the NCM concern; and the observation with the baseline photography and the lifelong skin checks is the mainstay, with the surgery and the laser for the selected case. This four-part framing — recognise, stratify, screen, surveil — is the fellowship answer in miniature. [1] [3]
Why does the prophylactic excision of the CMN not eliminate the melanoma risk?
Because the melanoma in the CMN may arise in the residual naevus cells left after the excision, in the satellite nevi, in the central nervous system in the neurocutaneous melanocytosis, or rarely in the extracutaneous site. The postzygotic NRAS mosaicism affects the melanocyte lineage broadly — the skin and the leptomeninges share the neural-crest origin — so the excision of the one visible lesion cannot remove every mutant cell. This is the biological reason the observation and the surveillance, rather than the routine prophylactic excision, are the mainstay of the management of the CMN. [6] [3]
References
- [1]Krengel S, Reyes-Múgica M. Melanoma risk in congenital melanocytic naevi. British Journal of Dermatology, 2017.PMID 28504374
- [2]Krengel S, Scope A, Dusza SW, et al. New recommendations for the categorization of cutaneous features of congenital melanocytic nevi. Journal of the American Academy of Dermatology, 2013.PMID 22982004
- [3]Krengel S, Marghoob AA. Current management approaches for congenital melanocytic nevi. Dermatologic Clinics, 2012.PMID 22800546
- [4]Price HN, O'Haver J, Marghoob A, et al. Practical application of the new classification scheme for congenital melanocytic nevi. Pediatric Dermatology, 2015.PMID 25346440
- [5]Arneja JS, Gosain AK. Giant congenital melanocytic nevi. Plastic and Reconstructive Surgery, 2007.PMID 17632335
- [6]Kinsler VA, Thomas AC, Ishida M, et al. Multiple congenital melanocytic nevi and neurocutaneous melanosis are caused by postzygotic mutations in codon 61 of NRAS. Journal of Investigative Dermatology, 2013.PMID 23392294
- [7]Caccavale S, Calabrese G, Mattiello E, et al. Cutaneous Melanoma Arising in Congenital Melanocytic Nevus: A Retrospective Observational Study. Dermatology, 2021.PMID 33053549
- [8]Zalaudek I, Conforti C, Guarneri F, et al. Clinical and dermoscopic characteristics of congenital and noncongenital nevus-associated melanomas. Journal of the American Academy of Dermatology, 2020.PMID 32360715
- [9]Elisabeth Wramp M, Langenbruch A, Augustin M, et al. Clinical course, treatment modalities, and quality of life in patients with congenital melanocytic nevi - data from the German CMN registry. Journal der Deutschen Dermatologischen Gesellschaft, 2017.PMID 28214318
- [10]Dohil MA, Baugh WP, Eichenfield LF. Vascular and pigmented birthmarks. Pediatric Clinics of North America, 2000.PMID 10943257
- [11]Tey HL. A practical classification of childhood hypopigmentation disorders. Acta Dermato-Venereologica, 2010.PMID 20107718
- [12]Oei W, Fledderus AC, Spuls PI, et al. Development of an international core domain set for medium, large and giant congenital melanocytic naevi as a first step towards a core outcome set for clinical practice and research. British Journal of Dermatology, 2021.PMID 33237568