Paeds · paediatric-dermatology
Contact dermatitis
Also known as Irritant contact dermatitis · Allergic contact dermatitis · Contact eczema · Patch test dermatitis
Fellowship guide to contact dermatitis in children: how to tell irritant from allergic disease at the bedside, the common culprits (nickel, fragrances, methylisothiazolinone, neomycin, saliva, wet work), when a recurrent or treatment-resistant eczema is hiding an allergy, the role and reading schedule of patch testing, and how barrier repair, allergen avoidance and potency-matched topical corticosteroids resolve the lesion while preventing the chronic, infected and facially disfiguring complications.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the eight-year-old who returns to clinic with the same angry, weeping band of eczema around her navel that cleared with steroid last month and came back the day she wore her favourite jeans with the metal button. Her atopic eczema elsewhere is well controlled, yet this one patch refuses to settle. That pattern — a same-site, recurrent, anatomically-clued eruption — is the fingerprint of allergic contact dermatitis, and it is the scenario every general paediatrician must learn to spot. [8]
Contact dermatitis is an eczematous skin inflammation arising from direct skin contact with an exogenous agent. It is divided into irritant contact dermatitis, caused by the direct cytotoxic effect of a chemical or physical agent on the skin cells, and allergic contact dermatitis, a cell-mediated delayed type IV hypersensitivity reaction to a specific allergen. A third, overlapping pattern is photocontact dermatitis, in which a topical or systemic agent becomes allergenic or irritant only in the presence of ultraviolet light. In children, irritant disease is far more common than allergic disease, but the latter is increasingly recognised as patch testing becomes more available. [11] [10]
Three ideas anchor the whole topic. First, the morphology of contact dermatitis is eczematous — erythema, vesicles, weeping, scaling and eventually lichenification — so it mimics and often coexists with atopic eczema, which is the commonest source of diagnostic error. Second, the distribution is the key to the cause: a sharply demarcated eruption in the shape of the offending object or at the site of contact points straight to a contactant, whether irritant or allergic. Third, the distinction between irritant and allergic disease matters because management differs — both need removal of the cause and barrier repair, but only allergic disease benefits from patch testing, allergen identification and long-term avoidance counselling. [8] [9]
Classification
The clearest way to organise contact dermatitis at the bedside is by mechanism, because mechanism predicts the history, the morphology, the distribution and the response to testing. [8]
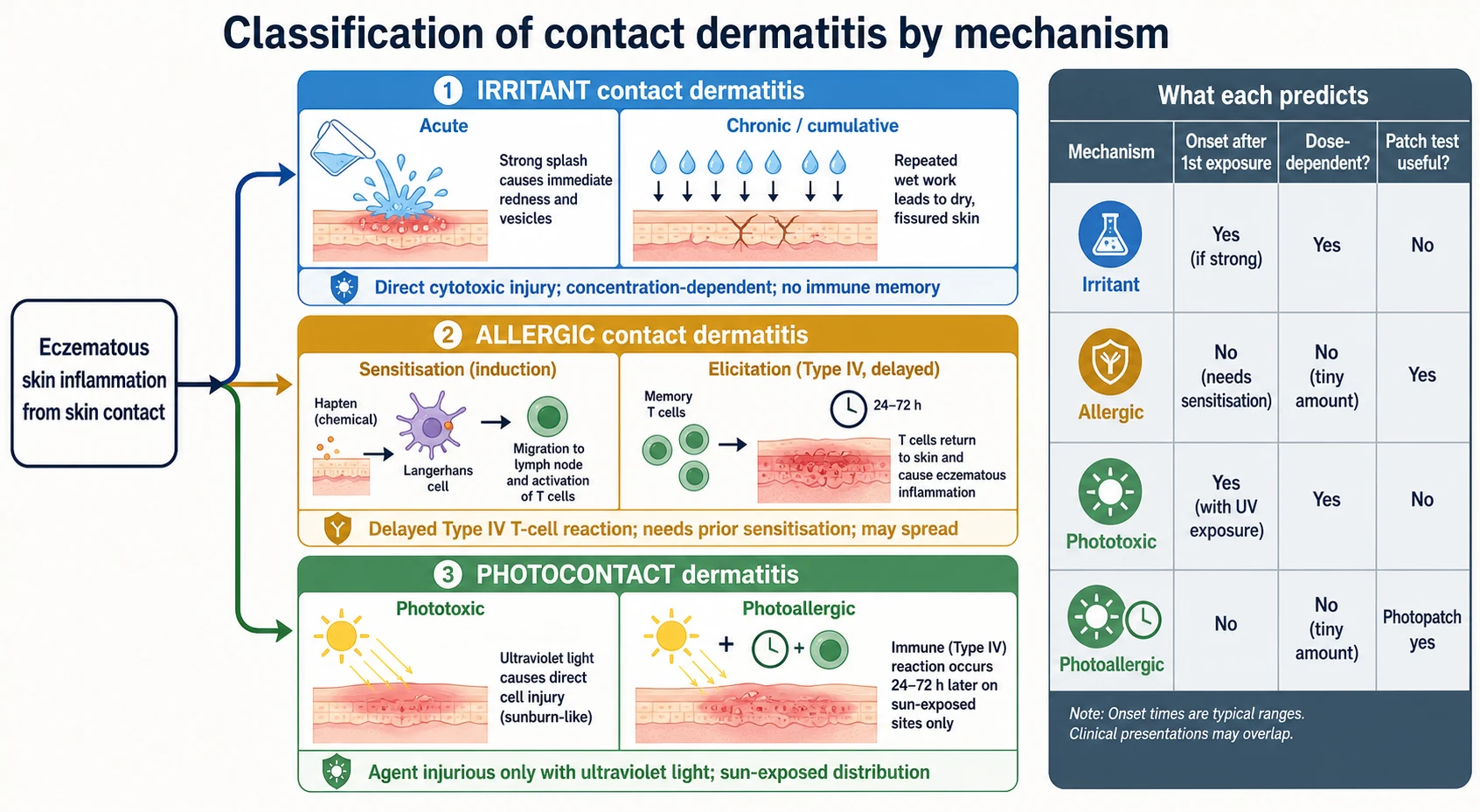
Irritant contact dermatitis is the direct, non-immunological injury of skin cells by a toxic agent. It is concentration- and exposure-dependent: a sufficiently strong irritant damages any child's skin on first contact, while a weak irritant produces dermatitis only after repeated cumulative exposure. The prototype in infants is napkin (diaper) dermatitis from prolonged contact with urine and faeces; in older children it is the chapped, fissured lips of the lip-licker, and the dry, sore hands of a swimmer or a frequent hand-washer. Because no immune memory is involved, the rash is confined to the area of contact and is typically sore or stinging rather than intensely itchy. [8] [11]
Allergic contact dermatitis is a delayed type IV hypersensitivity reaction to a specific allergen in a previously sensitised child. It unfolds in two phases: an induction or sensitisation phase in which the allergen is taken up by skin dendritic cells, processed and presented to naive T-cells in the draining lymph node, generating allergen-specific memory T-cells; and an elicitation phase on re-exposure, when those memory T-cells flood back into the skin and generate the eczematous inflammation. It does not occur on first contact, requires only a small amount of allergen once sensitised, and may spread beyond the contact site. Common childhood allergens include nickel, fragrances, preservatives such as methylisothiazolinone, topical antibiotics such as neomycin, rubber accelerants and chromates. [9] [11]
Photocontact dermatitis is the subset in which a chemical becomes injurious only after absorbing ultraviolet light. Phototoxic reactions are dose-dependent, sunburn-like and non-immunological; photoallergic reactions are eczematous, delayed and immunological, confined to sun-exposed sites. Common culprits include topical non-steroidal anti-inflammatory drugs, some sunscreens and plant-derived psoralens. It is uncommon in children but should be considered when a dermatitis is strictly limited to exposed skin in an outdoor setting. [10]
Epidemiology & Risk Factors
Contact dermatitis is among the most common skin complaints of childhood, but the two mechanisms carry very different epidemiologies. Irritant contact dermatitis is almost universal in infancy because the napkin area, the drooling chin and the lip-licking school-age child are all continually exposed to weak irritants. Allergic contact dermatitis is less common overall, yet studies of patch-tested children report sensitisation rates of around a quarter to a half of those tested, with nickel consistently the leading allergen across continents and age groups. [4] [11]
The risk factors divide into those that increase exposure and those that impair the skin barrier. Atopic eczema is the most important host factor, because a compromised barrier allows easier penetration of irritants and allergens and because children with eczema are exposed to many topical products — emollients, corticosteroids, antiseptics and wet-wrap dressings — each of which can sensitise. The systematic evidence is consistent: children with atopic dermatitis have a higher prevalence of contact allergy than children without, and a recurrent or treatment-resistant eczema in an atopic child warrants patch testing. [5]
Who gets contact dermatitis
Age shapes the likely allergen. Infants and toddlers present with napkin-area irritant dermatitis and lip or facial irritant dermatitis from drooling and pacifier contact. School-age children accumulate exposures — costume jewellery, footwear, topical treatments, school adhesives and wet work — and develop allergic dermatitis to nickel, rubber shoe components and fragrances. Adolescents introduce ear and body piercing (nickel), cosmetics and hair dyes (fragrances and paraphenylenediamine), and increasingly insulin pump and continuous glucose-monitoring adhesives, which have generated a recognisable modern cohort of device-related allergic dermatitis. [12] [10]
Pathophysiology
The barrier is where the story begins. The stratum corneum, held together by ceramide-rich lipids and tight junctions, normally excludes irritants and allergens and retains water. Anything that disrupts it — prolonged wetness, alkaline soaps, friction, the proteases in stool, or the inflammation of atopic eczema — lowers the threshold for both irritant and allergic reactions. This is why atopic children, whose filaggrin-deficient barrier is intrinsically leaky, develop contact dermatitis more readily and more severely than children with intact skin. [5] [8]
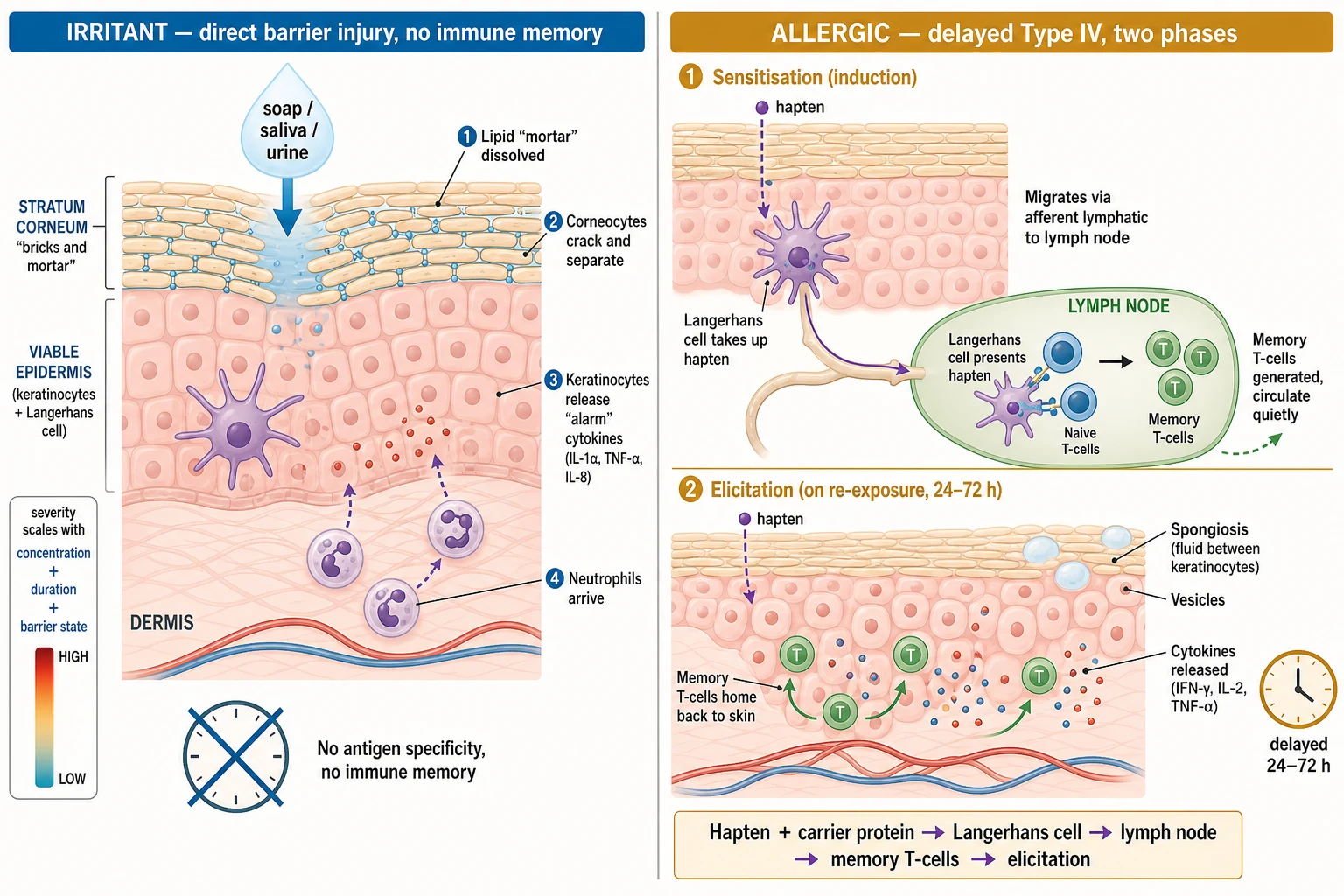
In irritant contact dermatitis the offending chemical acts directly on the keratinocytes and corneocytes. Surfactants dissolve the lipid envelope, alkaline agents raise the skin pH and activate serine proteases, and proteases in faecal matter degrade corneodesmosomes. The damaged keratinocytes release damage-associated cytokines and the skin mounts a non-specific, neutrophil-rich inflammatory response. The severity tracks the concentration of the irritant, the duration of contact and the integrity of the barrier, which is why a napkin left wet all night, or a swimmer who showers with alkaline soap four times a week, predictably develops dermatitis. There is no antigen specificity and no immunological memory. [8] [11]
Allergic contact dermatitis is a classical delayed type IV hypersensitivity reaction, and the hapten concept is central. Most contact allergens are small, lipid-soluble molecules — haptens — too small to be immunogenic on their own. In the sensitisation phase the hapten penetrates the epidermis, binds self-carrier proteins, and is taken up by Langerhans cells, the resident dendritic cells of the skin. The Langerhans cell matures, migrates to the regional lymph node and presents the hapten–peptide complex on major histocompatibility complex molecules to naive CD4 and CD8 T-cells, generating a clonal population of allergen-specific memory T-cells that quietly circulate for years. [9]
In the elicitation phase, a re-exposure to the same hapten recruits those memory T-cells back into the skin within 24 to 72 hours. They release cytokines that drive the eczematous inflammation — spongiosis, vesiculation and a lymphocytic infiltrate — and the child develops the intensely itchy, well-demarcated eruption that defines allergic contact dermatitis. Because the reaction is T-cell mediated, it is delayed by hours to days and is wholly different from the immediate urticarial or anaphylactic reactions of type I allergy, a distinction the exam rewards and the bedside demands. [1] [9]
Clinical Presentation
The history is the single most powerful diagnostic tool in contact dermatitis, because the eruption is tied to a contact that the child or parent can usually name once prompted. Ask about new skin products, cosmetics, jewellery, footwear, topical treatments, occupational or hobby exposures, school craft adhesives, and any change in the week before onset. Establish the timing: an irritant reaction can follow a single strong exposure or accumulate over weeks, whereas an allergic reaction requires prior sensitisation and appears 24 to 72 hours after re-exposure. Probe the symptom quality, because irritant dermatitis tends to sting or burn while allergic dermatitis itches intensely. [8] [6]
The morphology of an acute contact dermatitis is eczematous. Erythema is followed by papules and vesicles that may weep and crust, and in chronic disease the skin becomes dry, fissured, scaly and lichenified. The distribution is the diagnostic centrepiece. A sharply geometric or linear eruption in the shape of a watch strap, a shoe, a belt buckle or an adhesive dressing points directly to a contactant. Irritant dermatitis stays within the contact boundary and favours the most exposed, barrier-compromised sites — the napkin area, the hands, the perioral skin and the lip. Allergic dermatitis is usually more intensely inflamed and pruritic and may spread beyond the contact site, occasionally as a generalised autoeczematisation or id reaction. [9] [11]
[8] [9]Recognisable distribution patterns do much of the diagnostic work. A periumbilical or earlobe dermatitis in a pierced or belt-wearing child implicates nickel. A dermatitis on the dorsum of the foot sparing the interdigital spaces implicates a rubber shoe component or leather chromate. A facial or neck dermatitis in a child who has just changed shampoo, perfume or moisturiser implicates a fragrance or preservative, with methylisothiazolinone a modern and common culprit in leave-on products. A leg or stoma dermatitis arising under a topical antibiotic implicates neomycin or bacitracin. And in the child with type one diabetes, an itchy, well-demarcated eruption under an insulin pump site or glucose sensor implicates the adhesive or, less often, the insulin itself. [12] [4]
Differential Diagnosis
Atopic eczema is the great mimicker and the most common alternative diagnosis, and the two conditions frequently coexist. Atopic eczema favours the flexures in an older child and the face and extensor surfaces in an infant, has a strong atopic family history, and is chronically relapsing rather than linked to a discrete contact. The key diagnostic error is to label a same-site, contact-shaped eruption as a flare of atopic eczema, apply more steroid, and miss the contactant — which is why a treatment-resistant or anatomically-clued eczema drives the decision to patch test. [5] [6]
| Condition | Key distinguishing features | Patch test |
|---|
The infected or secondarily inflamed eczema must also be distinguished, because a contact dermatitis that is weeping, crusted and spreading with regional lymphadenopathy may be impetiginised or, rarely, complicated by eczema herpeticum. A rapid onset of painful, monomorphic punched-out vesicles or pustules on an eczematous base raises herpes simplex virus infection and demands urgent assessment and systemic antiviral therapy rather than topical steroid escalation. [8]
Clinical & Bedside Assessment
The assessment of a child with suspected contact dermatitis rests on a focused history and a careful whole-skin examination, because the morphology and the distribution together carry the diagnosis. Take the history first, before the child undresses, so the exposure narrative is fresh. Ask when the rash began, where it began, what makes it better or worse, what topical and systemic treatments have been used, and crucially what new exposures preceded it — products, jewellery, footwear, hobbies, school activities and medical devices. Establish whether the child is atopic, because an atopic background raises both the likelihood of coexisting eczema and the threshold to test for superimposed allergy. [8] [6]
Examine the whole skin, not only the obvious eruption. Map the distribution precisely, because a geometric or object-shaped boundary is the strongest single clue to a contactant. Note the morphology — erythema, vesicles, weeping, crusting, fissuring or lichenification — and whether there are signs of secondary infection such as pustules, golden crusts, regional lymphadenopathy or systemic upset. Look for clues in the nails, the scalp and the napkin area, and inspect any medical device sites. Assess the impact on sleep, school and function, and the psychological burden of a visible or chronic eruption, which is often substantial in school-age children. [9] [8]
Decide at the bedside whether this is likely irritant or allergic. An irritant pattern is sore rather than itchy, sharply confined to the contact site, and linked to a known exposure such as wet work, saliva or a napkin. An allergic pattern is intensely itchy, may spread beyond the site, and follows re-exposure to a specific allergen after a delay. In practice many children show a mixed picture, and the decision to patch test is driven less by certainty at first contact than by recurrence, same-site predilection, failure of standard eczema therapy, or a strong distribution clue. [2] [6]
Investigations
Most contact dermatitis is diagnosed clinically and needs no laboratory test, and the temptation to swab, scrape or biopsy a straightforward case should be resisted. Investigations are reserved for confirming allergic disease, excluding mimics, and detecting secondary infection or complication. The centrepiece of allergic contact dermatitis investigation is the epicutaneous patch test, a diagnostic rather than a screening test that must be targeted to a realistic clinical suspicion. [1] [3]
Patch testing is the gold-standard investigation for allergic contact dermatitis. Allergens are applied to the upper back in standardised chambers held under occlusive tape, left in place for 48 hours, and then removed and read. The decisive reading is at 72 to 96 hours (day three or four), because delayed type IV reactions take time to declare, and a second reading around day seven catches late reactors, particularly to metals and antibiotics. A positive reaction is a localised eczematous response at the allergen site, graded from doubtful erythema through papular, vesicular and confluent reactions. Relevance must then be assessed — whether the allergen explains the child's dermatitis now or in the past — because a positive patch test without relevance does not by itself make the diagnosis. [1] [7]
[1] [7]Children are not simply small adults in patch testing. The European Academy of Allergy and Clinical Immunology and the Pediatric Contact Dermatitis Workgroup recommend a tailored paediatric baseline series, with additional series chosen by history — a shoe series for foot dermatitis, a fragrance series for facial dermatitis, and a child's own products when relevant. The concentration of some allergens is reduced for children to avoid false-positive irritant reactions, and the smaller back may limit the number of chambers that can be applied at once, sometimes requiring staged testing. The family must be counselled that a positive reaction reproduces a small patch of dermatitis at the test site, and that the whole exercise is diagnostic, not curative. [3] [7]
Adjunctive tests have defined and limited roles. A skin swab for bacterial culture and sensitivity confirms suspected secondary infection and guides antibiotic choice. A viral swab or polymerase chain reaction test for herpes simplex virus confirms eczema herpeticum. A skin scraping for mycology excludes tinea in an annular plaque. Skin biopsy is rarely needed and shows non-specific spongiosis in both irritant and allergic disease, so it does not reliably distinguish them; it is reserved for excluding psoriasis, lymphoma or another specific dermatosis when the diagnosis is genuinely uncertain. Repeat open application testing and the use-strip method help confirm reactivity to a child's own cosmetic product. [6] [8]
Management — Resuscitation
Contact dermatitis is rarely a resuscitation problem, and true emergencies are limited to two scenarios. The first is the rare child with severe, extensive acute allergic contact dermatitis — for example, a florid eruption after hair dye application — who is systemically unwell, in severe pain, unable to sleep, or at risk of secondary skin infection and fluid loss across a large inflamed surface. The second is the suspicion of eczema herpeticum or a rapidly spreading cellulitis, where sepsis and dissemination are the threats. In both, the immediate priority is to assess and stabilise the child, treat infection or systemic inflammation, and arrange urgent specialist input, not to refine the dermatological diagnosis. [8] [9]
For the child with extensive weeping dermatitis, apply cool compresses to settle the acute inflammation and remove all likely contactants and topical products from the skin. Identify and treat secondary bacterial infection with an oral antistaphylococcal antibiotic such as flucloxacillin, dosed by weight, and escalate to intravenous therapy if the child is febrile, systemically unwell, or immunocompromised. If eczema herpeticum is suspected, start systemic aciclovir promptly and arrange dermatological review; topical steroids are withheld until infection is controlled. A short course of systemic corticosteroid is occasionally used for a severe, extensive allergic reaction, under specialist guidance and with attention to the child's growth, infection risk and the need for a taper. [8]
The most important resuscitative principle is the paradox that topical steroids, the mainstay of treatment, can also be the cause: a topical antibiotic, a preservative, or even the vehicle of a corticosteroid can sensitise and worsen the very dermatitis it is meant to treat. When a dermatitis worsens or fails to respond to a topical agent, that agent becomes a suspect and should be withdrawn, not intensified. [9] [5]
Management — Definitive & Stepwise
Definitive management rests on three pillars applied in sequence: identify and remove the cause, repair the skin barrier, and suppress the inflammation with a potency-matched topical corticosteroid. The cause is removed by taking a precise exposure history and eliminating the irritant or allergen from the child's environment, which alone resolves many cases and prevents recurrence. Barrier repair uses generous and frequent application of a bland, fragrance-free emollient and, in napkin dermatitis, a barrier cream such as zinc oxide or petrolatum with frequent nappy changes and air exposure. Inflammation control uses a topical corticosteroid matched to the site — a mild preparation for the face, flexures and napkin area, and a moderate or potent preparation for the trunk and limbs — applied once or twice daily until the dermatitis settles, then stepped down. [8] [9]
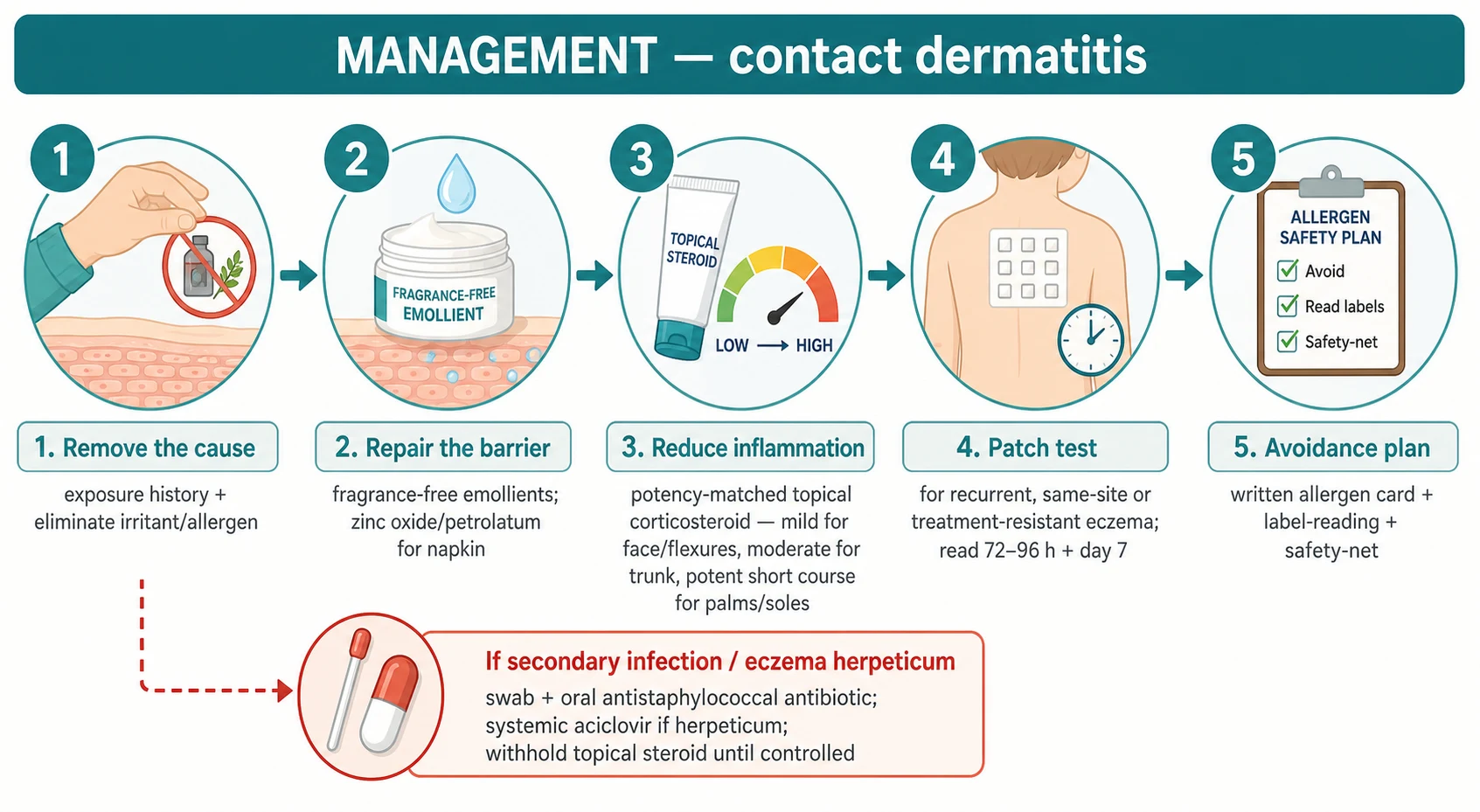
The choice of topical corticosteroid potency follows the site and the severity rather than the mechanism. A mild preparation, such as hydrocortisone, is used for the delicate skin of the face, eyelids, flexures and napkin area. A moderate preparation, such as triamcinolone or betamethasone valerate, suits the trunk and limbs of most children. A potent preparation is reserved for a short, supervised course on thick lichenified skin of the palms or soles, and very potent preparations are avoided in children except under specialist supervision. Emollients continue throughout and after the steroid course to consolidate the barrier, and the fingertip-unit measure guides the quantity applied. Review the child to confirm resolution and to reinforce avoidance. [8] [6]
A practical rule: the three R's of contact dermatitis
The acutely weeping dermatitis is soothed and dried before a steroid is applied. Cool saline or an astringent compress applied for 15 minutes several times a day dries the weeping surface, and a sedating antihistamine at night helps the itchy child sleep. Once the surface is dry, the topical corticosteroid and emollient are introduced. For irritant napkin dermatitis, the specific management combines frequent nappy changes, gentle cleansing with water, a barrier cream and, where candidal superinfection is present, a topical antifungal; it is one of the commonest irritant dermatitides of infancy and responds rapidly to these measures. [8]
Patch testing is indicated when allergic contact dermatitis is genuinely suspected: a recurrent same-site eczema, an eczema that fails appropriate atopic therapy, or a strong distribution clue. The results are interpreted with relevance in mind, and the confirmed allergen is added to a written avoidance plan and patient card, because the long-term cure of allergic contact dermatitis is avoidance, not medication. Refer to dermatology when patch testing is needed, when the dermatitis is severe or extensive, when there is diagnostic uncertainty, or when the child has a chronic dermatitis that is affecting growth, sleep, school or psychological wellbeing. [2] [1]
Specific Subtypes & Scenarios
Nickel allergic contact dermatitis is the archetype and the single most frequent childhood allergy, driven by costume jewellery, earrings, belt buckles, jean buttons and piercings. The classic presentation is an itchy, well-demarcated periumbilical or earlobe dermatitis in a school-age or adolescent child, and avoidance of nickel-releasing items resolves the lesion. Regulatory limits on nickel release in Europe have reduced sensitisation rates, but nickel remains dominant worldwide, and a careful history of metal contact is one of the highest-yield questions in paediatric dermatology. [4] [11]
Napkin (diaper) dermatitis is the commonest irritant dermatitis of infancy. Prolonged contact with urine and faeces — the proteases and lipases of which damage the stratum corneum — produces the well-demarcated, glazed erythema of the convex surfaces that spares the folds, where skin-on-skin contact protects. Secondary candidal infection extends into the folds and produces satellite pustules. Management combines frequent nappy changes, gentle cleansing with water, air exposure and a barrier cream, with a topical antifungal for candidal superinfection; the diagnosis is clinical and corticosteroids are usually unnecessary. [8]
Fragrance and preservative allergy has risen with the proliferation of cosmetic and leave-on products, and methylisothiazolinone has been a defining modern epidemic, producing facial and hand dermatitis in children exposed through wet wipes, shampoos, moisturisers and sunscreens. The distribution follows the product — a facial rash from a face cream, a perianal rash from a wet wipe — and avoidance is the mainstay, supported by fragrance-free and preservative-free substitutions. A child whose dermatitis began with a new product should stop that product while patch testing is arranged. [10]
Device-related allergic dermatitis in children with type one diabetes is a growing and clinically important cohort. Insulin pump and continuous glucose-monitoring adhesives, and less often insulin or isophane itself, generate itchy, well-demarcated eruptions at the site of the device that can threaten device adherence and glycaemic control. Management combines adhesive rotation, barrier films under the device, patch testing to identify the culprit, and substitution of the device or adhesive, often in partnership with the diabetes team. [12]
The treatment-resistant atopic child deserves particular attention, because superimposed contact allergy is easy to miss. An atopic child whose eczema localises to one site, recurs after steroid withdrawal, or fails to respond to an appropriate regimen should be patch tested, and the systematic evidence confirms a higher prevalence of contact allergy in this group. The lesson is that atopic eczema and contact dermatitis coexist, and the failure of standard therapy is a signal to look for a contactant, not to escalate the steroid indefinitely. [5] [6]
Complications & Pitfalls
The complications of contact dermatitis are driven by unrecognised cause, undertreatment, overtreatment and secondary infection. The most common is chronicity — a dermatitis that recurs because the contactant is never identified, evolving into a dry, fissured, lichenified skin that impairs sleep, school and self-esteem. Secondary bacterial infection with Staphylococcus aureus or streptococcus produces weeping, crusting, regional lymphadenopathy and occasionally cellulitis, and eczema herpeticum is the rare but serious viral complication that demands urgent systemic aciclovir. The skin of a long-standing contact dermatitis may also become secondarily sensitised to the very treatments used, particularly topical antibiotics and preservatives. [8] [9]
The pitfalls are largely diagnostic and avoidable. The first is mistaking a contact-shaped eruption for a flare of atopic eczema and escalating the steroid rather than looking for a contactant. The second is reading a patch test too early or on inflamed skin and being falsely reassured by a negative result. The third is the excited skin or angry back syndrome, in which a strongly positive reaction inflames adjacent sites and produces a crop of false positives, demanding repeat testing of individual allergens once the skin has settled. The fourth is treating a positive patch test as the diagnosis without assessing relevance, leading to unnecessary and burdensome avoidance. [1] [6]
The avoidable errors
The treatment-related pitfalls complete the picture. Overuse of a potent topical corticosteroid on delicate skin causes atrophy, telangiectasia and striae, and systemic absorption from large-area or occluded use can suppress the hypothalamic–pituitary–adrenal axis in a small child. Conversely, the fear of steroids leads to under-treatment and chronicity. The antidote is potency-matched, time-limited, supervised use with clear instructions to the family, combined with emollients and avoidance. [8]
Prognosis & Disposition
The prognosis of contact dermatitis is excellent when the cause is identified and removed. Irritant dermatitis settles within days to weeks once the irritant is withdrawn, the barrier is repaired, and a short course of potency-matched steroid is applied, and recurrence is preventable with ongoing barrier care. Allergic dermatitis settles in the same timeframe once the allergen is avoided, and the long-term outlook depends entirely on whether avoidance is sustained: a child who avoids the confirmed allergen does well, while continued exposure drives chronicity and complications. [8] [9]
The prognosis is poorer when the contactant is never identified, particularly in the atopic child with superimposed allergy, and in the device-dependent child whose medical device cannot easily be changed. In these groups the dermatitis tends to recur and to accumulate sensitisation to new products, which is why patch testing and a written avoidance plan are part of good disposition rather than an optional add-on. [5] [12]
Disposition is usually to the general paediatrician or primary clinician with dermatology referral for patch testing when allergic disease is suspected. The child with secondary infection or eczema herpeticum needs acute care and follow-up. The child with a confirmed allergen is discharged with a written avoidance card, education on reading product labels, and clear safety-netting advice about the warning signs of infection. Most children are managed in the community, with rural and remote clinicians supported by telehealth and by outreach patch-testing services where these exist. [2] [8]
Special Populations
Infants and toddlers present predominantly with irritant disease — napkin dermatitis, drooling facial dermatitis and pacifier-related cheilitis — because their barrier is thin and their exposures are wet and frictional. Allergic disease is less common but possible, particularly to topical products and rubber. Management emphasises barrier care, frequent nappy changes and gentle cleansing, and topical steroids are used sparingly and at the lowest effective potency because of the high surface-area-to-mass ratio and the risk of systemic absorption. [8]
The atopic child is the population in whom contact allergy is most often missed, because the default diagnosis of an eczematous eruption is atopic eczema. The barrier defect of atopy increases both irritant and allergic susceptibility, and the systematic evidence supports a higher prevalence of contact allergy in atopic children. The threshold to patch test is lower, and a recurrent, same-site or treatment-resistant eczema in an atopic child is the clearest indication. [5] [6]
Children with chronic medical devices and complex needs form a growing and vulnerable cohort. Type one diabetes devices, stomas, hearing aids and orthopaedic braces all generate adhesive- or material-related dermatitis that can threaten device adherence and quality of life. Management combines device rotation, barrier films, patch testing and substitution, and it requires close partnership with the treating specialty team. [12]
Indigenous, migrant and socioeconomically disadvantaged children may face barriers to specialist patch testing, specialist products and follow-up, and outdoor and occupational exposures (including plant-derived Compositae allergy) may shape the differential. Culturally safe assessment, attention to language and health literacy, and a low threshold to refer for patch testing when access allows are part of equitable care, and telehealth-supported patch testing is extending reach into rural and remote communities. [2]
Evidence, Guidelines & Regional Differences
| Region | Key guidance | Patch-test access | Notable allergens |
|---|
The two controversies a candidate should be able to discuss are the relationship between atopic eczema and contact allergy, and the threshold for patch testing in children. The older view that atopy protected against contact allergy has been overturned by systematic reviews showing a higher prevalence of sensitisation in atopic children, which has lowered the threshold to test. The methylisothiazolinone epidemic, driven by its broad use in leave-on cosmetics, illustrates how regulatory exposure shapes sensitisation rates and how product reformulation can curb an epidemic. And the rise of device-related dermatitis in diabetes care is generating new evidence on adhesive and insulin allergens that is still maturing. [5] [10]
Exam Pearls
References
- [1]Johansen JD, Aalto-Korte K, Agner T, Andersen KE, Bircher A, et al. European Society of Contact Dermatitis guideline for diagnostic patch testing - recommendations on best practice. Contact Dermatitis, 2015.PMID 26179009
- [2]Tam I, Yu J Allergic Contact Dermatitis in Children: Recommendations for Patch Testing. Curr Allergy Asthma Rep, 2020.PMID 32548648
- [3]de Waard-van der Spek FB, Darsow U, Mortz CG, Orton D, Aschoff R, et al. EAACI position paper for practical patch testing in allergic contact dermatitis in children. Pediatr Allergy Immunol, 2015.PMID 26287570
- [4]DeKoven JG, Silverberg JI, Warshaw EM, Maibach HI, Belisto DV, et al. North American Contact Dermatitis Group Patch Test Results: 2017-2018. Dermatitis, 2021.PMID 33970567
- [5]Simonsen AB, Johansen JD, Deleuran M, Mortz CG, Sommerlund M, et al. Contact allergy in children with atopic dermatitis: a systematic review. Br J Dermatol, 2017.PMID 28470762
- [6]Neale H, Garza-Mayers AC, Tam I, St Louis J, Yu J Pediatric allergic contact dermatitis. Part 2: Patch testing series, procedure, and unique scenarios. J Am Acad Dermatol, 2021.PMID 33217511
- [7]Yu J, Atwater AR, Brod B, Chen JK, Chiu V, et al. Pediatric Baseline Patch Test Series: Pediatric Contact Dermatitis Workgroup. Dermatitis, 2018.PMID 29933256
- [8]Seth D, Poowuttikul P, Kamat D, Pansare M, Nassef M Contact Dermatitis in Children. Pediatr Ann, 2021.PMID 34044703
- [9]Brown C, Yu J Pediatric Allergic Contact Dermatitis. Immunol Allergy Clin North Am, 2021.PMID 34225896
- [10]Tam I, Yu J Pediatric contact dermatitis: what's new. Curr Opin Pediatr, 2020.PMID 32618793
- [11]Simonsen AB, Deleuran M, Johansen JD, Sommerlund M Contact allergy and allergic contact dermatitis in children - a review of current data. Contact Dermatitis, 2011.PMID 21851361
- [12]Alves da Silva C, Bregnhøj A, Mowitz M, Zachariae C Contact dermatitis in children caused by diabetes devices. Contact Dermatitis, 2022.PMID 35634681