Paeds · paediatric-dermatology
Drug eruptions including DRESS and AGEP
Also known as Cutaneous adverse drug reaction · Drug rash · DRESS syndrome · Drug-induced hypersensitivity syndrome · AGEP · Acute generalised exanthematous pustulosis · Morbilliform drug eruption
Fellowship guide to drug eruptions in children: how to tell the common benign morbilliform rash from the three severe cutaneous adverse reactions (DRESS, AGEP and SJS-TEN) at the bedside, the drugs and the timing that point to each, the role of eosinophilia, hepatitis and HHV-6 reactivation in DRESS, the sterile pinhead pustules and rapid course of AGEP, and the management of stopping the drug, assessing severity, excluding infection and supporting the child.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the six-year-old started on a cephalosporin for tonsillitis who, ten days in, develops a fever and a widespread pink rash that begins on his trunk and spreads to his limbs. His mother is frightened and wants to know whether the antibiotic is to blame and whether he is safe. That scenario — a child with a rash after a new drug — is one of the most common and most anxiety-provoking presentations in general paediatrics, and the clinician's job is to separate, calmly and quickly, the benign majority from the dangerous few. [1]
A drug eruption is any cutaneous reaction caused by a medication, whether systemic or topical. The vast majority are benign exanthems, of which the morbilliform (measles-like) pattern is by far the commonest, but a small and critically important minority are severe cutaneous adverse reactions that carry significant morbidity and mortality. The two severe reactions covered in this topic are DRESS, the drug reaction with eosinophilia and systemic symptoms, also called drug-induced hypersensitivity syndrome or DIHS, and AGEP, acute generalised exanthematous pustulosis. Stevens-Johnson syndrome and toxic epidermal necrolysis are covered in a dedicated topic because they form a distinct mechanistic and prognostic entity, but they belong to the same severe family and must be excluded at the bedside whenever a drug eruption looks worrying. [2] [3]
Three ideas anchor the whole topic and drive every clinical decision. First, timing is the strongest single clue to the type of reaction, because a morbilliform rash takes days, AGEP takes hours, DRESS takes weeks, and each latency points to a different mechanism. Second, the presence of systemic features — fever, mucosal involvement, lymphadenopathy, eosinophilia, hepatitis or skin pain — is the dividing line between a benign exanthem and a severe cutaneous adverse reaction, and a child who is systemically unwell with a drug rash is never a simple allergy. Third, the first action in any suspected drug eruption, benign or severe, is to stop the culprit drug and to take a precise, chronological medication history, because the drug itself is both the cause and the diagnostic thread. [1] [9]
Classification
The clearest way to organise a drug eruption at the bedside is by the combination of morphology and severity, because together they predict the mechanism, the urgency and the prognosis. [2]
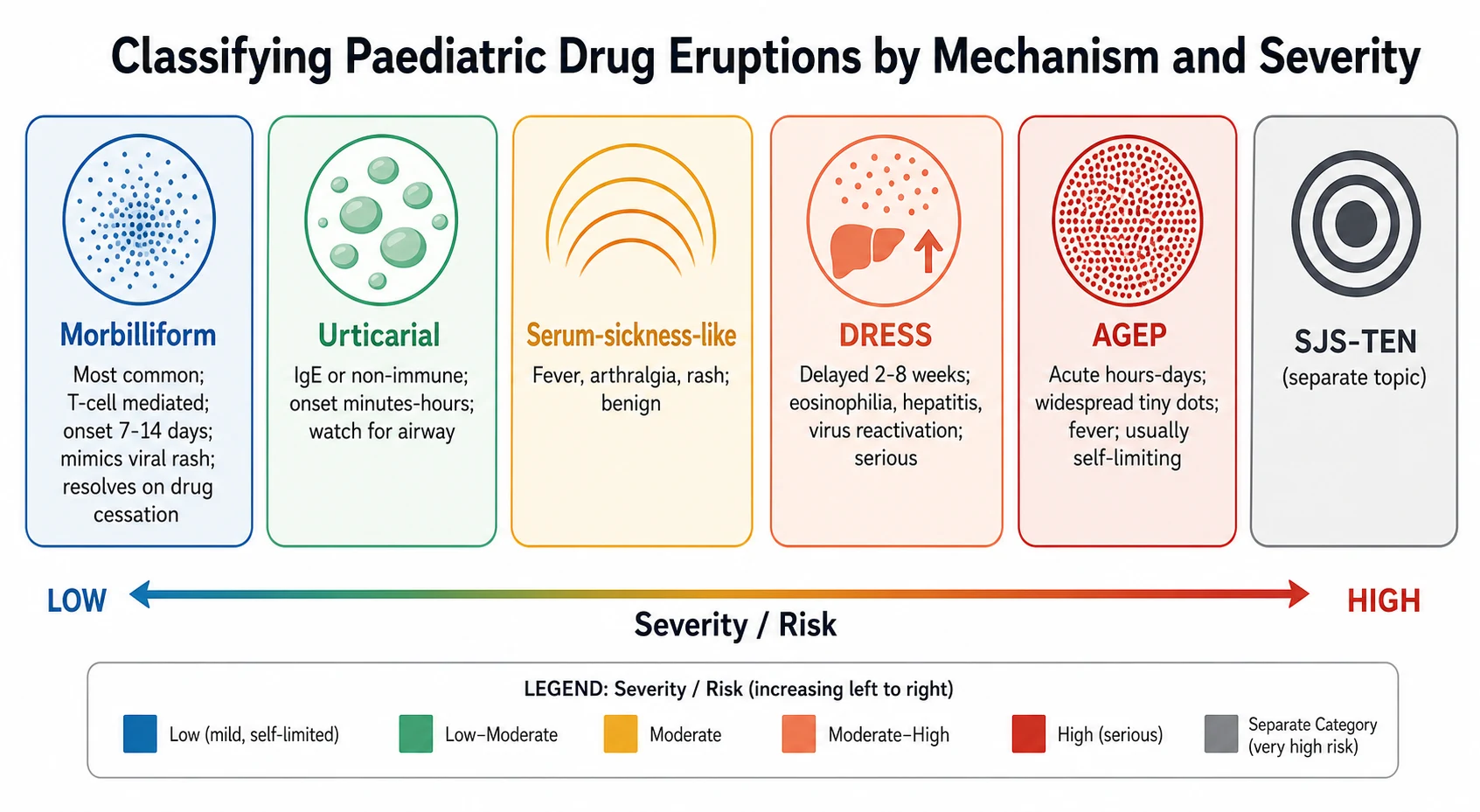
Morbilliform (exanthematous) eruptions are the commonest cutaneous drug reactions, accounting for around nine in every ten. They are T-cell mediated type IV reactions that appear five to fourteen days after a drug is first started, or within one to two days on re-exposure in a previously sensitised child. The rash is a fine, pink, blanching maculopapular eruption that mimics a viral exanthem, begins on the trunk and proximal limbs, and spreads centrifugally, often with mild itch and low-grade fever. Antibiotics — especially penicillins, cephalosporins and sulfonamides — and anticonvulsants are the leading culprits. The eruption resolves over seven to fourteen days once the drug is stopped, and the major diagnostic task is to confirm that it is not evolving into a severe reaction. [1] [2]
Urticarial eruptions present with transient, pruritic wheals, each lasting less than twenty-four hours, that appear minutes to hours after a drug. They may be immunoglobulin-E mediated or non-immunological, and the key concern is not the rash itself but the risk of progression to angio-oedema and anaphylaxis, which is why every urticarial drug reaction demands a careful airway assessment. [2]
DRESS (drug reaction with eosinophilia and systemic symptoms), also called drug-induced hypersensitivity syndrome, is a delayed, multi-organ hypersensitivity reaction that develops two to eight weeks after exposure to a culprit drug. Its hallmark is the combination of a widespread, often morbilliform or exfoliative rash, fever, facial oedema, lymphadenopathy, eosinophilia, hepatitis and herpes-virus — usually HHV-6 — reactivation. The classic culprits are the aromatic anticonvulsants (phenytoin, carbamazepine, phenobarbital), sulfonamides, allopurinol, minocycline and dapsone. DRESS carries up to ten per cent mortality and can relapse weeks after the drug is withdrawn, which is why it demands prompt recognition, drug cessation and systemic corticosteroid. [3] [4]
AGEP (acute generalised exanthematous pustulosis) is a rapid, neutrophil-driven reaction in which hundreds of small, sterile, non-follicular pinhead pustules erupt on an erythematous, oedematous skin within hours to a day of a culprit drug, accompanied by fever and neutrophilia. Beta-lactam antibiotics (especially aminopenicillins), macrolides, terbinafine, diltiazem and chloramphenicol are the common triggers. AGEP is usually self-limiting and resolves spontaneously in one to two weeks after drug cessation with superficial desquamation, though it carries a mortality of around two to five per cent. [7] [8]
Epidemiology & Risk Factors
Drug eruptions are among the most common adverse events in paediatric practice, and children on antibiotics and anticonvulsants carry the highest risk. The morbilliform eruption is by far the commonest pattern, and antibiotics — particularly beta-lactams and sulfonamides — are the leading class of culprit, because children receive them frequently for common infections. The severe cutaneous adverse reactions are individually rare, with DRESS estimated at around one to ten per ten thousand exposures to high-risk drugs and AGEP rarer still, but their severity means every clinician must recognise them. [1] [6]
The risk factors divide into drug factors, host factors and genetic factors. The high-risk drugs are few and worth memorising: the aromatic anticonvulsants, sulfonamide antibiotics, allopurinol, nevirapine, minocycline, dapsone and vancomycin for DRESS, and beta-lactams, macrolides and terbinafine for AGEP. Host factors that raise the risk of severe reactions include active infection, immune activation and concurrent autoimmune disease, because a stimulated immune system lowers the threshold for a drug-driven T-cell response. [2] [6]
Who gets a severe drug eruption
The genetic contribution is now well established and examinable. Specific human-leucocyte-antigen alleles confer markedly raised risk of severe reactions to particular drugs: HLA-B15:02 strongly predisposes to carbamazepine-induced SJS-TEN in Han Chinese and South-East Asian populations and is screened before prescribing carbamazepine in some health systems, while HLA-B13:01 is associated with dapsone hypersensitivity. Recent work has also linked severe delayed reactions to interleukin-1 and interleukin-6 biologic inhibitors in children to common HLA-DRB1*15 alleles, showing that the genetic architecture of drug hypersensitivity extends beyond the classical anticonvulsant associations. [12] [10]
Pathophysiology
Every drug eruption covered in this topic is ultimately a T-cell driven, type IV hypersensitivity reaction, and the differences in timing, morphology and severity flow from which T-cell subset dominates, which cytokines it releases, and whether the reaction stays confined to the skin or spills into the systemic circulation. [9]
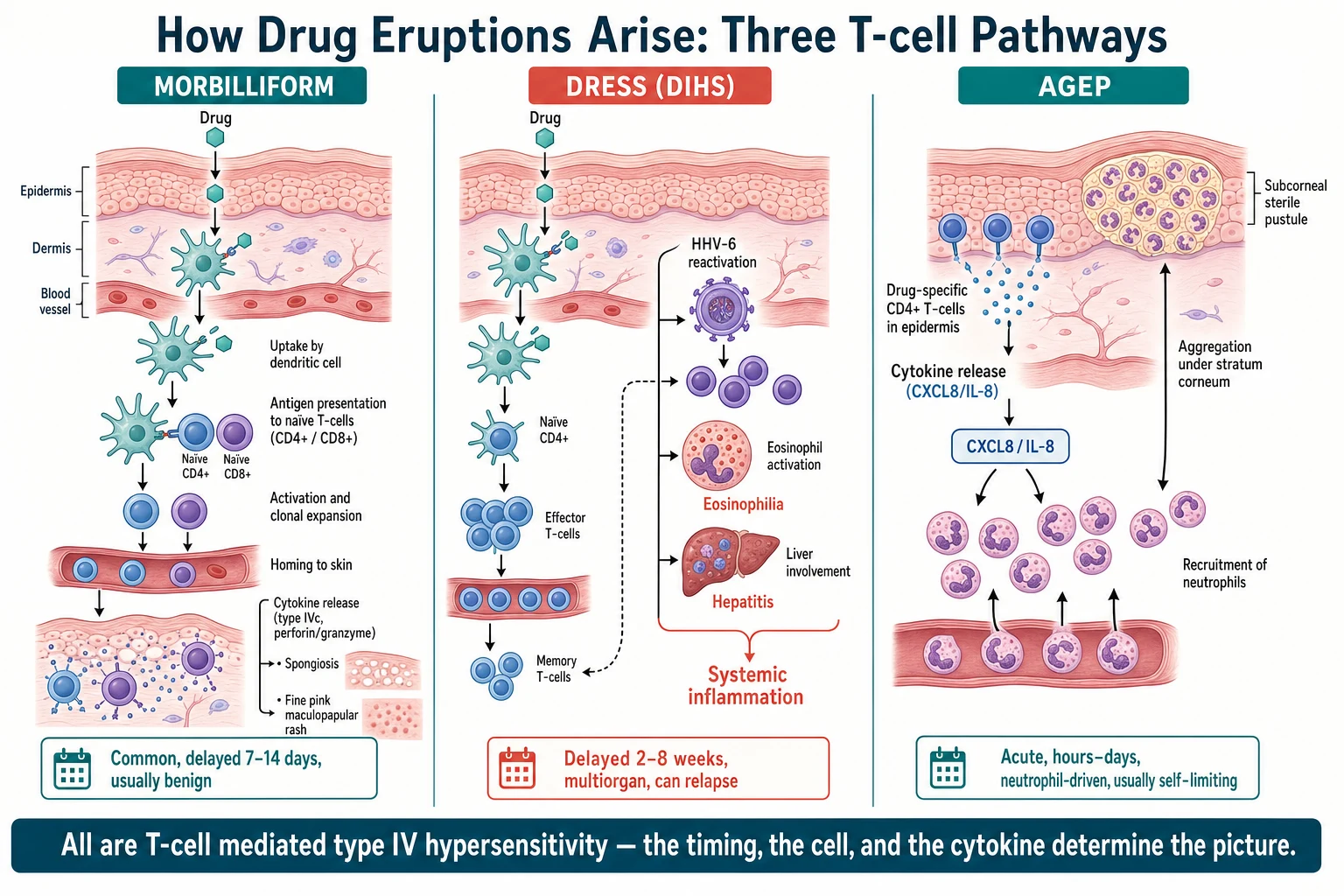
In the morbilliform eruption the drug or its metabolite enters the skin, is taken up by epidermal dendritic cells, and is presented to naive CD4 and CD8 T-cells in the draining lymph node. The activated drug-specific T-cells traffic back to the skin and release cytokines and cytotoxic mediators such as perforin and granzyme, producing spongiosis — intercellular oedema — and the characteristic fine maculopapular rash. The reaction is delayed because it requires T-cell priming and recruitment, which is why it takes five to fourteen days after the first dose and recurs within one to two days on re-exposure, when memory T-cells are already primed. [1] [2]
In DRESS the same drug-specific T-cell response is amplified and generalised by herpes-virus reactivation. The prevailing model holds that the culprit drug or its metabolite, often a reactive intermediate generated by an inherited or acquired enzyme defect, triggers a polyclonal T-cell activation and, in parallel, reactivates a latent human herpesvirus — most often HHV-6, but also cytomegalovirus and Epstein-Barr virus. The viral reactivation drives a self-perpetuating inflammatory cascade: eosinophils are recruited and activated, atypical lymphocytes appear in the blood, and the inflammation spills from the skin into the liver, the kidneys, the lungs and occasionally the heart and brain. This combination of drug-specific T-cell injury and virus-driven amplification explains the long latency, the eosinophilia, the multi-organ involvement, the tendency to relapse after the drug is withdrawn, and the high mortality. [3] [4]
In AGEP the drug-specific T-cell response is redirected toward neutrophil recruitment. Drug-specific CD4 T-cells in the skin release very high levels of interleukin-8, a potent neutrophil chemoattractant, which floods the epidermis with neutrophils that aggregate beneath the stratum corneum to form the sterile subcorneal pustules that define the condition. Because the reaction is driven by pre-formed, drug-specific T-cell memory, it erupts rapidly — within hours to a day of exposure — and because it is confined to the epidermis, it is usually self-limiting and resolves once the drug is withdrawn and the pustules desquamate. The speed, the neutrophil dominance and the superficial confinement distinguish AGEP mechanistically from the deep, slow, eosinophilic inflammation of DRESS. [7] [8]
Clinical Presentation
The history does most of the diagnostic work in a drug eruption, because the timing of the rash relative to drug exposure is the single strongest clue to its type. Establish a precise chronological timeline: when each medication was started and stopped, when the rash began, and whether there has been prior exposure. A rash that appears five to fourteen days into a new drug course is consistent with a morbilliform eruption, one that erupts within hours to a day suggests AGEP, and one that appears two to eight weeks after starting an anticonvulsant or sulfonamide, with fever and systemic upset, points to DRESS. Ask about itch, skin pain, mucosal symptoms, fever and malaise, because these features separate a benign exanthem from a severe cutaneous adverse reaction. [1] [9]
The morphology of a morbilliform eruption is a fine, blanching, pink maculopapular rash that begins on the trunk and proximal extremities and spreads outward, mimicking a viral exanthem. There may be mild fever, pruritus and palmar or plantar involvement, but there is no blistering, no mucosal erosion, no skin pain and no significant systemic upset. The key bedside task is to confirm that the rash is not evolving — a morbilliform eruption that develops skin pain, atypical target lesions, blistering or mucosal involvement is crossing into a severe reaction and must be reassessed immediately. [2]
[3] [7]The presentation of DRESS is dominated by its delayed onset and its systemic spread. Two to eight weeks into a culprit drug, the child develops a high fever, a widespread rash that is initially morbilliform but may become infiltrated, purpuric or exfoliative, striking facial oedema, and lymphadenopathy. Blood testing reveals eosinophilia and atypical lymphocytes, and liver involvement — a hepatitis with raised transaminases — is the commonest visceral manifestation, though interstitial nephritis, pneumonitis, myocarditis and encephalitis also occur. The rash and the fever can persist or relapse for weeks after the drug is withdrawn, driven by ongoing herpes-virus reactivation, which is a hallmark that distinguishes DRESS from every other drug eruption. [3] [6]
The presentation of AGEP is dominated by its rapid onset and its characteristic pustules. Within hours to a day of the culprit drug, the child develops a fever and a diffuse, erythematous, oedematous skin onto which hundreds of tiny, sterile, non-follicular pinhead pustules erupt, concentrated in the flexures and the intertriginous areas. Mucosal involvement is mild or absent, which helps separate it from SJS-TEN, and systemic upset is usually modest. The pustules coalesce and then desquamate over one to two weeks as the eruption resolves spontaneously once the drug is stopped. [7] [8]
Differential Diagnosis
The most important differential for any drug eruption is the viral exanthem, because the two are morphologically indistinguishable and frequently coexist — a child on an antibiotic for a viral illness may have either or both. The timing is the key: a viral exanthem erupts in the expected incubation window of the virus and is not tightly linked to a drug, whereas a morbilliform drug eruption appears five to fourteen days after a specific medication and recurs on re-exposure. When a child on an antibiotic develops a rash during a viral illness, the pragmatic approach is to stop the drug, observe, and document the reaction, rather than labelling a lifelong antibiotic allergy without evidence. [1] [2]
| Condition | Key distinguishing features | Onset / latency |
|---|
Among the severe reactions the critical distinction is between DRESS, AGEP and SJS-TEN. DRESS is delayed, eosinophilic and systemic, with a long latency and herpes-virus reactivation. AGEP is acute, pustular and neutrophilic, with a very short latency and usually mild systemic upset. SJS-TEN presents with target lesions, mucosal erosions and epidermal detachment, and skin pain with a positive Nikolsky sign, and is covered in its own topic because it demands a distinct management pathway. Generalised pustular psoriasis can mimic AGEP histologically and clinically but arises in a child with known psoriasis, evolves over days rather than hours, and is not drug-triggered, and a skin biopsy helps when the diagnosis is uncertain. [7] [11]
Clinical & Bedside Assessment
The bedside assessment of a child with a suspected drug eruption has one goal: to decide, quickly and safely, whether this is a benign exanthem or a severe cutaneous adverse reaction. Begin with a rapid assessment of airway, breathing and circulation, because urticarial reactions can progress to airway compromise and severe reactions can cause fluid loss and sepsis-like physiology across an inflamed or denuded skin. Take the temperature and examine for signs of systemic illness, because fever with a drug rash is a red flag that demands a full reassessment rather than reassurance. [2] [11]
The medication history is the diagnostic centrepiece. List every drug the child has taken in the preceding eight weeks — prescription, over-the-counter, herbal and complementary medicines — and map each onto the timeline of the rash. Pay particular attention to the high-risk drugs: aromatic anticonvulsants, sulfonamides, allopurinol, minocycline, dapsone, vancomycin and nevirapine for DRESS, and beta-lactams, macrolides and terbinafine for AGEP. Ask about prior reactions and about family history of severe drug reactions, because a first-degree relative with a severe cutaneous adverse reaction raises the index of suspicion. [9] [6]
Examine the whole skin, including the mucous membranes, the palms and soles, and the nails. For a morbilliform eruption, confirm the blanching, maculopapular, trunk-to-limb distribution and the absence of blistering, skin pain and mucosal involvement. For a suspected DRESS, look for facial oedema, lymphadenopathy, an infiltrated or exfoliative rash and any signs of hepatic, renal or respiratory involvement. For a suspected AGEP, look for the hundreds of tiny, non-follicular pinhead pustules on an erythematous base, clustered in the flexures, and confirm that the mucosa is spared. Perform the Nikolsky sign — gentle lateral pressure on apparently normal skin — to exclude SJS-TEN whenever the skin looks fragile or blistered. [3] [7]
Investigations
Most morbilliform drug eruptions are diagnosed clinically and need no investigation, but any suspected severe cutaneous adverse reaction demands a structured workup to confirm the pattern, to quantify the organ involvement and to exclude infection. The first-line blood tests are a full blood count, which looks for the eosinophilia and atypical lymphocytes of DRESS or the neutrophilic leucocytosis of AGEP; liver function tests and renal function, which detect the hepatitis and interstitial nephritis of DRESS; and inflammatory markers, which gauge the systemic burden. Blood cultures and viral serology help exclude sepsis and intercurrent viral illness, which are the most dangerous alternative diagnoses in a febrile child with a rash. [3] [9]
Herpes-virus serology is central to the workup of DRESS. HHV-6 reactivation, with a rising viral load two to three weeks into the illness, supports the diagnosis and helps explain the relapsing course, and concurrent cytomegalovirus and Epstein-Barr virus testing guides the monitoring and the prognosis. In AGEP, the EuroSCAR-derived AGEP validation score combines the acute onset, the typical pustular morphology, the fever and the rapid resolution to confirm the diagnosis and to distinguish it from acute generalised pustular psoriasis. [4] [7]
Skin biopsy is reserved for cases where the diagnosis is genuinely uncertain or where SJS-TEN, pustular psoriasis or an infective pustulosis must be excluded. DRESS shows a dense lymphocytic infiltrate with eosinophils and occasional necrotic keratinocytes, while AGEP shows the diagnostic subcorneal spongiform pustule, and SJS-TEN shows full-thickness epidermal necrosis — three patterns that a good dermatopathologist can distinguish. Patch testing has a limited and late role: it is never performed in the acute phase, but weeks to months after recovery it may help identify the culprit drug and guide future avoidance, and it is more useful in DRESS and AGEP than in SJS-TEN. [9] [5]
Management — Resuscitation
The rare but life-threatening emergencies in a drug eruption are airway compromise from a urticarial reaction progressing to anaphylaxis, fluid and heat loss across a denuded skin in SJS-TEN, and the multi-organ failure of severe DRESS. Begin with airway, breathing and circulation, and treat any sign of anaphylaxis — stridor, wheeze, hypotension, or facial and airway swelling — with intramuscular adrenaline immediately, because an urticarial drug reaction can deteriorate within minutes. For the child with extensive skin loss, follow burn-unit principles of fluid resuscitation, temperature control and aseptic handling, and arrange urgent transfer to a centre with paediatric intensive care and dermatology. [2] [11]
For suspected DRESS, the immediate priority is to stop the culprit drug and to assess and support the failing organs. The child with hepatitis needs close monitoring of liver function and coagulation, the child with interstitial nephritis needs fluid and electrolyte management and renal-function surveillance, and the child with pneumonitis or myocarditis needs respiratory and cardiac support. Systemic corticosteroid is the mainstay of treatment: a regimen such as oral prednisolone at one milligram per kilogram per day is used to suppress the inflammation, tapered slowly over weeks to months because relapse is common and dangerous. [5]
[3] [6]Exclude infection at every stage, because the fever and the rash of a severe drug eruption mimic sepsis, and the immunosuppression used to treat DRESS can mask or worsen an occult infection. Take blood, urine and swab cultures before starting corticosteroid where possible, and treat any confirmed infection promptly. A short course of systemic corticosteroid in a child with a confirmed severe drug eruption is safe and life-saving, but only when infection has been sought and addressed, and the dose must be tapered rather than stopped abruptly to avoid rebound. [5] [4]
Management — Definitive & Stepwise
Definitive management rests on four steps applied in sequence, and the same framework governs the benign and the severe reaction: stop the drug, assess the severity, support the child, and prevent recurrence. The first and most important step in every case is to stop the culprit drug and to review and rationalise all concurrent medications, because continued exposure drives the reaction and the latency. For a benign morbilliform eruption, stopping the drug plus an oral antihistamine for itch and an emollient is all that is needed, and the rash resolves over seven to fourteen days. [1] [2]
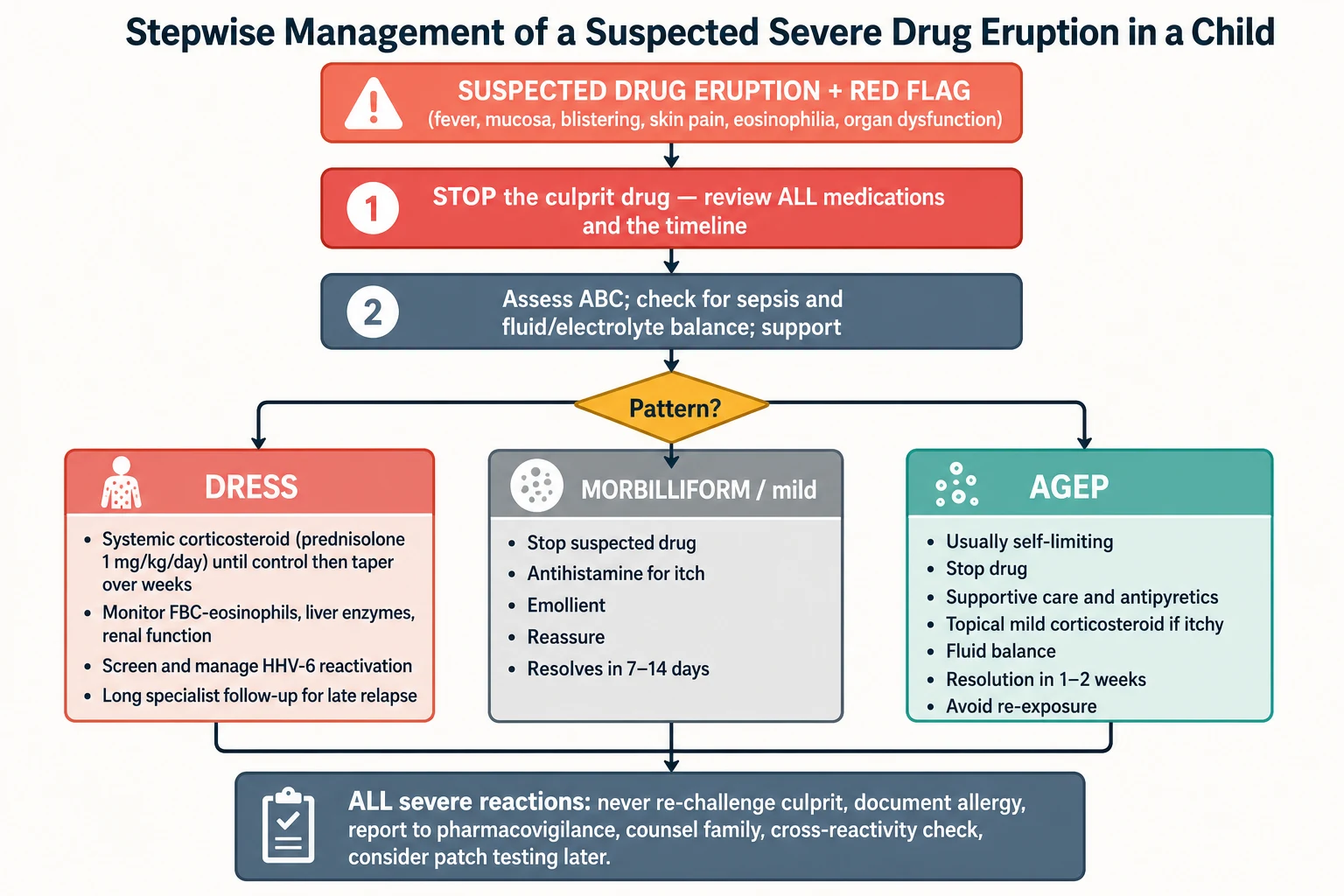
For DRESS, the stepwise approach combines drug cessation with systemic corticosteroid and vigilant organ monitoring. Oral prednisolone at one milligram per kilogram per day suppresses the inflammation and is continued until the fever, the rash and the organ dysfunction settle, then tapered slowly over weeks to months because herpes-virus-driven relapse is common. Liver enzymes, renal function and the eosinophil count are monitored throughout and on tapering, and the family is counselled that the course may relapse and that specialist follow-up is essential. [5] [3]
The four steps of drug-eruption management — STOP, SUPPORT, SCORE, SAVE
For AGEP, management is predominantly supportive, because the reaction is usually self-limiting. Stop the drug, control the fever with antipyretics, maintain fluid and electrolyte balance, apply a mild topical corticosteroid or an emollient for comfort, and monitor for the rare complication of secondary skin infection. The pustules resolve with superficial desquamation over one to two weeks, and systemic corticosteroid is reserved for the unusually severe or extensive case. The child is discharged with clear documentation of the culprit and advice to avoid it lifelong, because re-exposure can trigger a faster and more severe recurrence. [7] [8]
The final step — preventing recurrence — applies to every reaction, benign or severe, and is where most preventable harm occurs. Document the allergy clearly in the medical record and on an allergy card for the family, check for cross-reactivity among related drugs (especially the aromatic anticonvulsants and the sulfonamides, which share metabolites and can cross-react), report the reaction to the national pharmacovigilance programme, and never re-challenge a confirmed severe cutaneous adverse reaction, because re-exposure can be fatal. Refer to allergy and dermatology for structured follow-up and, where appropriate, delayed patch testing to confirm the culprit. [9] [2]
Specific Subtypes & Scenarios
Anticonvulsant DRESS (the classic DIHS presentation) is the archetype. A child started on phenytoin, carbamazepine, phenobarbital or lamotrigine develops, two to eight weeks into treatment, a fever, a morbilliform rash, facial oedema, lymphadenopathy, eosinophilia and hepatitis. The aromatic anticonvulsants are oxidised to a reactive arene-oxide metabolite that is detoxified by the enzyme epoxide hydrolase, and an inherited or acquired defect in this pathway allows the toxic metabolite to accumulate and trigger the syndrome. The practical implication is cross-reactivity: a child who has reacted to one aromatic anticonvulsant may react to the others, so sodium valproate, levetiracetam or topiramate — non-aromatic alternatives — are preferred for future seizure control. [3] [6]
Sulfonamide and antibiotic DRESS is increasingly recognised and broadens the culprit list beyond the anticonvulsants. Sulfamethoxazole, dapsone, minocycline and vancomycin are the leading antibiotic causes, and sulfonamides share the same reactive-metabolite problem as the anticonvulsants, generating a hydroxylamine that is toxic to cells. Dapsone carries an additional HLA-B*13:01 association, and minocycline is notable for producing DRESS with a long latency and a sometimes severe hepatitis, which is why the drug is used sparingly and with monitoring in children. [6] [12]
Allopurinol DRESS is the adult-orientated but paediatric-relevant pattern that arises in children treated for hyperuricaemia, leukaemia or tumour-lysis prophylaxis. Allopurinol and its active metabolite oxypurinol accumulate in renal impairment, which is why dose adjustment for renal function is essential, and the HLA-B*58:01 allele strongly predisposes to allopurinol-induced severe cutaneous adverse reactions. A child on allopurinol who develops a rash two to eight weeks in, with fever and eosinophilia, has DRESS until proven otherwise. [4] [3]
AGEP after a beta-lactam is the commonest scenario. A child started on an aminopenicillin such as amoxicillin develops, within a day, a fever and hundreds of pinhead pustules over an erythematous, oedematous skin, and the pustules are sterile and non-follicular, which distinguishes them from a bacterial folliculitis. The rapid onset, the characteristic morphology and the spontaneous resolution on drug cessation make the diagnosis, and the main task is to distinguish it from DRESS and from SJS-TEN, which it can superficially resemble before the pustules declare. [7] [8]
Biologic-inhibitor reactions are a growing and modern cohort. Severe delayed hypersensitivity reactions to interleukin-1 inhibitors such as anakinra and canakinumab, and to interleukin-6 inhibitors such as tocilizumab, used in children with systemic juvenile idiopathic arthritis and autoinflammatory disease, have been linked to common HLA-DRB1*15 alleles. This expands the genetic landscape of drug hypersensitivity beyond the classical anticonvulsant and sulfonamide associations and reminds the clinician that any new biologic, in a genetically susceptible child, can trigger a severe delayed reaction. [12]
Complications & Pitfalls
The complications of a severe drug eruption flow from unrecognised organ involvement, from untreated infection, and from the consequences of the treatment itself. DRESS causes hepatitis that can progress to acute liver failure, interstitial nephritis that can cause acute kidney injury, pneumonitis, myocarditis and encephalitis, and it can relapse weeks after the drug is withdrawn, driven by persistent herpes-virus reactivation. AGEP is usually self-limiting but can cause secondary skin infection and, rarely, fluid and electrolyte disturbance across an inflamed skin, and the rare overlap with SJS-TEN carries the worst prognosis of all. [3] [4]
The pitfalls are largely diagnostic and avoidable. The first is dismissing a long-latency rash as a trivial drug allergy — a rash two to eight weeks after an anticonvulsant or sulfonamide, with fever and eosinophilia, is DRESS until proven otherwise, and the delay in diagnosis directly worsens the outcome. The second is misreading AGEP as a bacterial folliculitis and treating it with another antibiotic that may itself be a culprit, rather than stopping the drug and supporting the child. The third is failing to exclude infection before starting systemic corticosteroid, which can mask and worsen an occult sepsis. [6] [7]
The avoidable errors
The treatment-related pitfalls complete the picture. Stopping systemic corticosteroid abruptly in DRESS invites a relapse that can be more severe than the original presentation, so the taper must be slow and supervised. Over-labelling a child with a lifelong antibiotic allergy on the basis of a non-specific rash during a viral illness restricts future treatment options unnecessarily, and the remedy is a careful history and, where appropriate, delayed allergy assessment to confirm or refute the label. Failing to document and report the reaction leaves the family and future clinicians blind to the risk, and is a recurring source of preventable re-exposure. [1] [9]
Prognosis & Disposition
The prognosis of a morbilliform drug eruption is excellent: it resolves within seven to fourteen days of stopping the drug, leaves no sequelae, and the main task is to confirm that it was not the herald of a severe reaction. The prognosis of AGEP is also good in the great majority of cases, because it is self-limiting and resolves in one to two weeks after drug cessation, though the small mortality and the occasional severe case demand vigilance and supportive care. [1] [7]
The prognosis of DRESS is guarded and unpredictable. It carries up to ten per cent mortality, driven by liver failure, overwhelming infection and the rare cardiac and neurological complications, and it can relapse weeks to months after the drug is withdrawn. Long-term follow-up is essential because the hepatitis, the renal injury and the endocrine consequences of a prolonged steroid course may declare themselves late, and because the reactivation of HHV-6 and other herpes viruses can drive a relapsing, polycyclic course that is unique to this syndrome. [3] [4]
Disposition depends on the severity and the pattern. A benign morbilliform eruption is managed in the community with drug cessation and follow-up. DRESS is admitted for investigation, organ support and systemic corticosteroid, and is managed jointly by general paediatrics, dermatology, allergy and, where organ failure is present, intensive care. AGEP is usually managed on the ward with supportive care, with intensive care reserved for the extensive or complicated case. Every child with a confirmed severe cutaneous adverse reaction is discharged with documented allergy advice, a written avoidance plan, and structured allergy and dermatology follow-up, including consideration of delayed patch testing to confirm the culprit. [2] [5]
Special Populations
Children on chronic anticonvulsants are the population at highest risk of DRESS, because the aromatic anticonvulsants remain among the commonest culprits and are widely used in paediatric epilepsy. A child who develops a fever and a rash two to eight weeks after starting or escalating an anticonvulsant has DRESS until proven otherwise, and the future seizure management must use a non-cross-reactive alternative such as sodium valproate, levetiracetam or topiramate, with careful counselling of the family and the neurology team. [3] [6]
Immunocompromised children carry a higher burden of drug exposure and a stimulated immune system, both of which raise the risk and the severity of drug eruptions. Children on chemotherapy, post-transplant immunosuppression or biologic therapy receive many high-risk drugs and have frequent infections that complicate the differential, so the threshold to investigate a new rash thoroughly is lower and the partnership with oncology, transplant and rheumatology teams is essential. [12] [4]
Children of Asian and South-East Asian heritage are relevant to the HLA associations that drive severe reactions, particularly HLA-B*15:02 and carbamazepine-induced SJS-TEN, and the increasing use of pre-prescription pharmacogenetic screening in some health systems reflects this. A culturally competent history that explores ethnicity and family history of severe drug reactions is part of safe prescribing, and the results guide the choice of drug and the counselling of the family. [10] [9]
Indigenous, migrant and socioeconomically disadvantaged children may face barriers to specialist follow-up, to documented allergy records and to pharmacovigilance reporting, and language and health-literacy barriers can compound the risk of inadvertent re-exposure. A written, plain-language allergy card, clear safety-netting advice, and low-threshold referral to allergy and dermatology services, supported by telehealth where access is limited, are part of equitable care for this vulnerable group. [1]
Evidence, Guidelines & Regional Differences
| Region | Key guidance | Pharmacogenetic screening | Notable culprits |
|---|
Two controversies a candidate should be able to discuss are the role of pharmacogenetic screening and the optimal duration of corticosteroid in DRESS. Pre-prescription HLA screening before carbamazepine has reduced SJS-TEN in screened populations and is now embedded in several national guidelines, but its extension to other drug-HLA pairs and to other populations remains an active area of research. The optimal corticosteroid regimen in DRESS — the dose, the route and the duration of taper — is not settled by randomised trials, and practice varies, though the consensus favours a moderate-dose systemic corticosteroid tapered slowly over weeks to months, with close monitoring for relapse. [4] [5]
Exam Pearls
References
- [1]Nguyen E, Gabel CK, Yu J, Hata T, Shih I, et al. Pediatric drug eruptions. Clin Dermatol, 2020.PMID 33341197
- [2]Del Pozo-Magaña BR, Liy-Wong C, Yan AC, Pope E Drugs and the skin: A concise review of cutaneous adverse drug reactions. Br J Clin Pharmacol, 2024.PMID 35974692
- [3]Wei BM, Fox LP, Kaffenberger BH, Hughey LC, Shinkai K, et al. Drug-induced hypersensitivity syndrome/drug reaction with eosinophilia and systemic symptoms. Part II diagnosis and management. J Am Acad Dermatol, 2024.PMID 37516356
- [4]Awad A, Goh MS, Trubiano JA, Phillips EJ Drug Reaction With Eosinophilia and Systemic Symptoms: A Systematic Review. J Allergy Clin Immunol Pract, 2023.PMID 36893848
- [5]Calle AM, Aguirre N, Ardila JC, Garcia B, Ortega-Lopez M, et al. DRESS syndrome: A literature review and treatment algorithm. World Allergy Organiz J, 2023.PMID 37082745
- [6]Sharifzadeh S, Mohammadpour AH, Tavanaee A, Vahdati-Nasab O, Hashemzaei M, et al. Antibacterial antibiotic-induced drug reaction with eosinophilia and systemic symptoms (DRESS) syndrome: a literature review. Eur J Clin Pharmacol, 2021.PMID 33025080
- [7]Halevy S Acute generalized exanthematous pustulosis. Curr Opin Allergy Clin Immunol, 2009.PMID 19458527
- [8]Bhat YJ, Akhtar S, Ahmad M, Latif I, Mir AI, et al. Etiopathological and Clinical Study of Acute Generalized Exanthematous Pustulosis: Experience from a Tertiary Care Hospital in North India. Indian Dermatol Online J, 2020.PMID 32695700
- [9]Brockow K, Wurpts G, Trautmann A, Ring J, Kapp A, et al. Guideline for allergological diagnosis of drug hypersensitivity reactions: S2k Guideline of the German Society for Allergology and Clinical Immunology (DGAKI) in cooperation with the German Dermatological Society (DDG). Allergologie Select, 2023.PMID 37705676
- [10]Levi N, Bastuji-Garin S, Mockenhaupt M, Dunant A, Liss Y, et al. Medications as risk factors of Stevens-Johnson syndrome and toxic epidermal necrolysis in children: a pooled analysis. Pediatrics, 2009.PMID 19153164
- [11]Ramien ML, Kohorst MA, Son MBH, Lalonde AT, Schaffer JV, et al. Stevens-Johnson syndrome in children. Curr Opin Pediatr, 2022.PMID 35836393
- [12]Saper VE, Ombrello MJ, Tremoulet AH, Zaffer MC, Oshima K, et al. Severe delayed hypersensitivity reactions to IL-1 and IL-6 inhibitors link to common HLA-DRB1*15 alleles. Ann Rheum Dis, 2022.PMID 34789453