Paeds · paediatric-dermatology
Impetigo and bacterial skin infection
Also known as Impetigo · School sores · Non-bullous impetigo · Bullous impetigo · Staphylococcal scalded skin syndrome · Community-acquired MRSA skin and soft tissue infection
Fellowship topic on impetigo and bacterial skin infection in children: the non-bullous and bullous forms of impetigo, ecthyma, and the toxin-mediated staphylococcal scalded skin syndrome; the Staphylococcus aureus and group A streptococcal pathophysiology including desmoglein-cleaving exfoliative toxins; the differential of crusted and blistering paediatric rashes; a clinical diagnosis with swabs reserved for atypical or recurrent disease; stepwise topical and oral antibiotic treatment matched to extent and region, with incision-and-drainage-centred management of abscess and community-acquired MRSA; the post-streptococcal glomerulonephritis complication and the skin-strep-versus-throat-strep distinction from rheumatic fever; and ANZ, UK, US and Canada guidance including remote Indigenous endemic disease.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
What splits the skin — desmoglein-1
Overview & Definition
Picture a four-year-old brought to the clinic with a crusted, weeping sore under the nose that started as a small spot three days ago, has spread across the cheek, and now crops up on the sibling's chin. The child is otherwise well, afebrile and scratching. This is the everyday face of bacterial skin infection in childhood — common, contagious, eminently treatable, and quietly capable, in its complications, of causing real harm. Recognising the form, choosing the treatment by extent, and watching for the post-streptococcal sequelae is the whole skill. [2] [1]
Impetigo is a superficial, highly contagious bacterial infection of the epidermis caused most often by Staphylococcus aureus and group A beta-haemolytic streptococcus (Streptococcus pyogenes). It spreads by direct contact and through broken skin — an insect bite, an abrasion, or the cracked skin of atopic dermatitis giving the organism its entry. It is the most common bacterial skin infection in children worldwide, and its burden falls heavily on young children in warm, humid climates and in disadvantaged and remote communities. [2] [9]
The clinician's task has three layers. The first is recognition — distinguishing impetigo from its mimics, and the benign superficial form from the toxin-mediated and invasive diseases that need the hospital. The second is treatment matched to extent, organism and region, delivered with antibiotic-stewardship discipline so that the common disease does not drive resistance. The third is the public-health and complication layer: school exclusion, household decolonisation, and the vigilance for post-streptococcal glomerulonephritis that turns a skin sore into a renal problem weeks later. [1] [2]
Classification
Sort bacterial skin infection by how deep it goes and which toxin is at work, because depth decides whether a topical cream is enough or a child needs a hospital. The two forms of impetigo sit at the superficial end. Non-bullous impetigo accounts for about seventy percent of cases: a small papule or vesicle ruptures within a day or two to leave the characteristic golden, honey-coloured crust on an erythematous base, classically around the nose and mouth but anywhere a break in the skin has offered entry. It heals without scarring. Either S. aureus or group A streptococcus may cause it. [1] [2]
Bullous impetigo accounts for about thirty percent, occurs at any age but most often in infants and young children, and is caused exclusively by S. aureus strains producing exfoliative toxins A or B. The toxin cleaves desmoglein-1 within the granular layer of the epidermis, separating the superficial epidermis and producing flaccid, translucent bullae up to several centimetres across, with a narrow rim of erythema. The bullae rupture easily and leave a thin, collarette-like rim of scale and a shiny, moist base. Unlike the non-bullous form it can arise on previously intact skin. [8] [1]
Ecthyma is the deeper cousin: group A streptococcal infection that extends through the epidermis into the dermis to produce a punched-out, ulcerated lesion with a thick, dark crust, usually on the legs. It heals with scarring, distinguishing it from the superficial forms, and signals more invasive streptococcal disease that usually warrants oral systemic therapy. [4] [2]
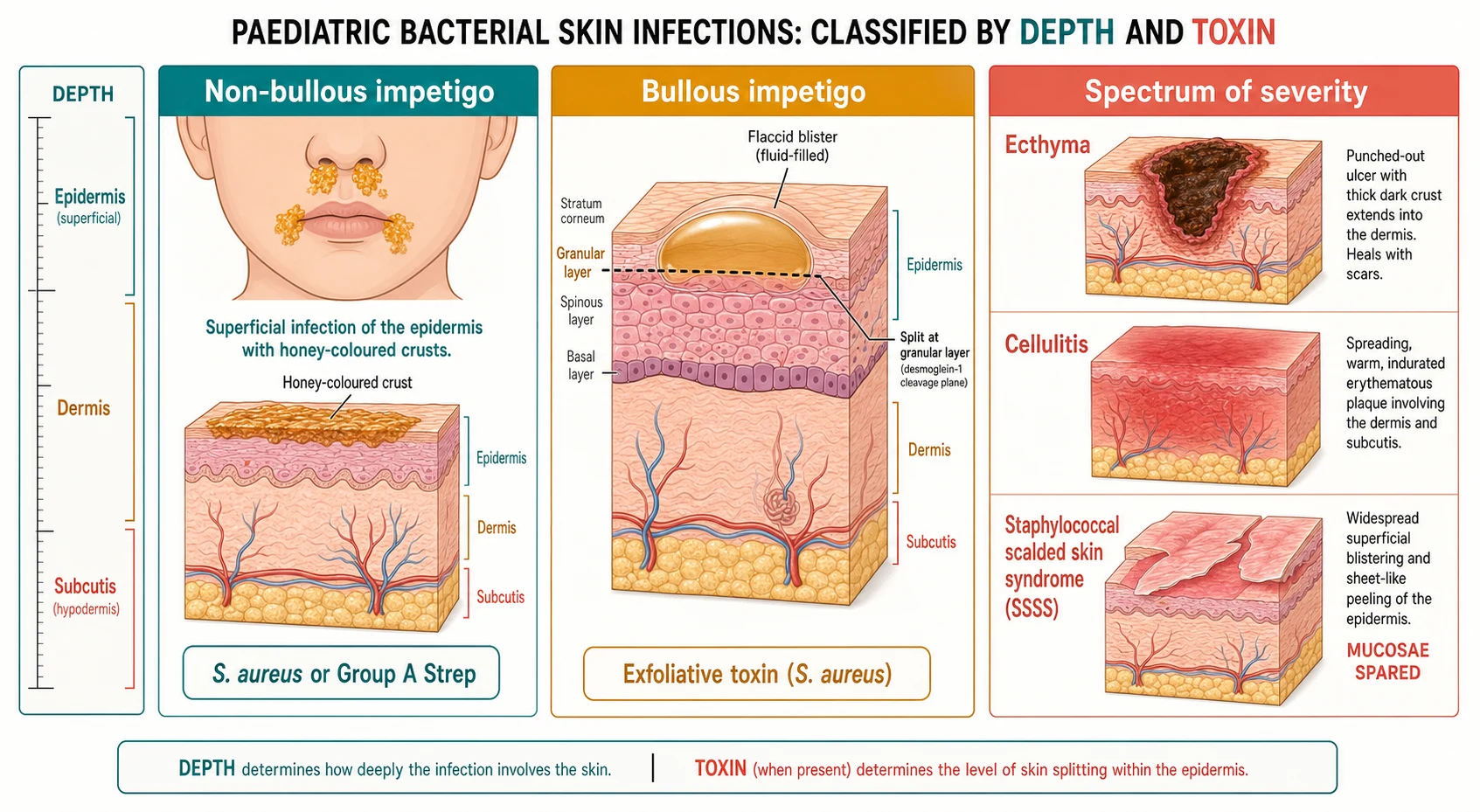
The toxin-mediated end of the spectrum is staphylococcal scalded skin syndrome (SSSS). Here the same exfoliative toxin, produced at a localised focus of stainters, circulates systemically and cleaves desmoglein-1 across the skin surface, causing widespread, tender, sandpaper-like erythema followed by large, flaccid bullae and sheet-like peeling around the flexures, mouth and eyes. It affects neonates and young children, the mucous membranes are spared, and the outcome in children is usually good with prompt intravenous anti-staphylococcal therapy and supportive care. [8]
Epidemiology & Risk Factors
Where does impetigo sit, and who does it hurt? It is the most common bacterial skin infection of childhood, with a global systematic review estimating a population prevalence of impetigo in the hundreds of millions, concentrated in tropical and resource-limited settings where warmth, humidity, crowding and skin trauma combine. The burden falls on children between two and six years of age, and in endemic regions the prevalence among school-age children can reach double figures. [2] [9]
The dominant risk factors are breaks in the skin barrier and close contact. Atopic dermatitis with its cracked, excoriated skin is the classic portal of entry, alongside insect bites, abrasions, scabies infestation and chickenpox lesions. Crowded households, poor access to clean water, warm humid climate, and participation in contact sports or childcare all amplify transmission through direct skin-to-skin contact and shared fomites. Understanding who is at risk directs both the individual treatment and the household and community response. [2] [1]
The organism picture has shifted over two decades. Staphylococcus aureus is now the predominant cause across both forms in most settings, with group A streptococcus contributing to non-bullous disease and ecthyma and dominating the impetigo of remote endemic communities. Community-acquired MRSA emerged as a major cause of skin and soft tissue infection in children from the 2000s, carrying the Panton-Valentine leukocidin toxin in many strains and changing empiric antibiotic choice where it is prevalent. [4] [5]
In Australia and Aotearoa New Zealand the burden is starkly uneven. Remote Aboriginal and Torres Strait Islander and Maori and Pasifika communities carry some of the highest documented prevalence of impetigo in the world, driven by household crowding, scabies co-infestation, limited access to water and the warm tropical climate. Group A streptococcus predominates and the downstream burden of post-streptococcal glomerulonephritis and, in some regions, acute rheumatic fever reflects this. The National Healthy Skin Guideline frames impetigo in these settings as a public-health disease requiring combined treatment of skin and scabies, household-based care and improved environmental health. [2] [3]
Pathophysiology
Why does a common skin organism produce a honey crust in one child and a widespread blistering syndrome in another? The answer lies in the toxins and in the integrity of the skin barrier. Staphylococcus aureus and group A streptococcus colonise the skin surface and the nose, and they enter through any break in the stratum corneum — a scratch, an eczematous fissure, an insect bite or a scabies burrow. Once in the superficial epidermis they multiply and provoke an acute inflammatory response, generating the pus that dries into the honey-coloured crust of non-bullous disease. [1] [2]
Bullous impetigo and staphylococcal scalded skin syndrome share a single mechanism. Certain phage-group II strains of S. aureus produce exfoliative toxins A and B, which are serine proteases that specifically cleave the extracellular domain of desmoglein-1. Desmoglein-1 is the desmosomal adhesion molecule that holds keratinocytes together in the superficial, granular layer of the epidermis. When it is cleaved, the superficial epidermis splits, fluid accumulates, and a bulla forms. In bullous impetigo the toxin acts locally at the site of the staphylococcal focus; in staphylococcal scalded skin syndrome the toxin circulates in the bloodstream and cleaves desmoglein-1 across the whole skin surface. [8]
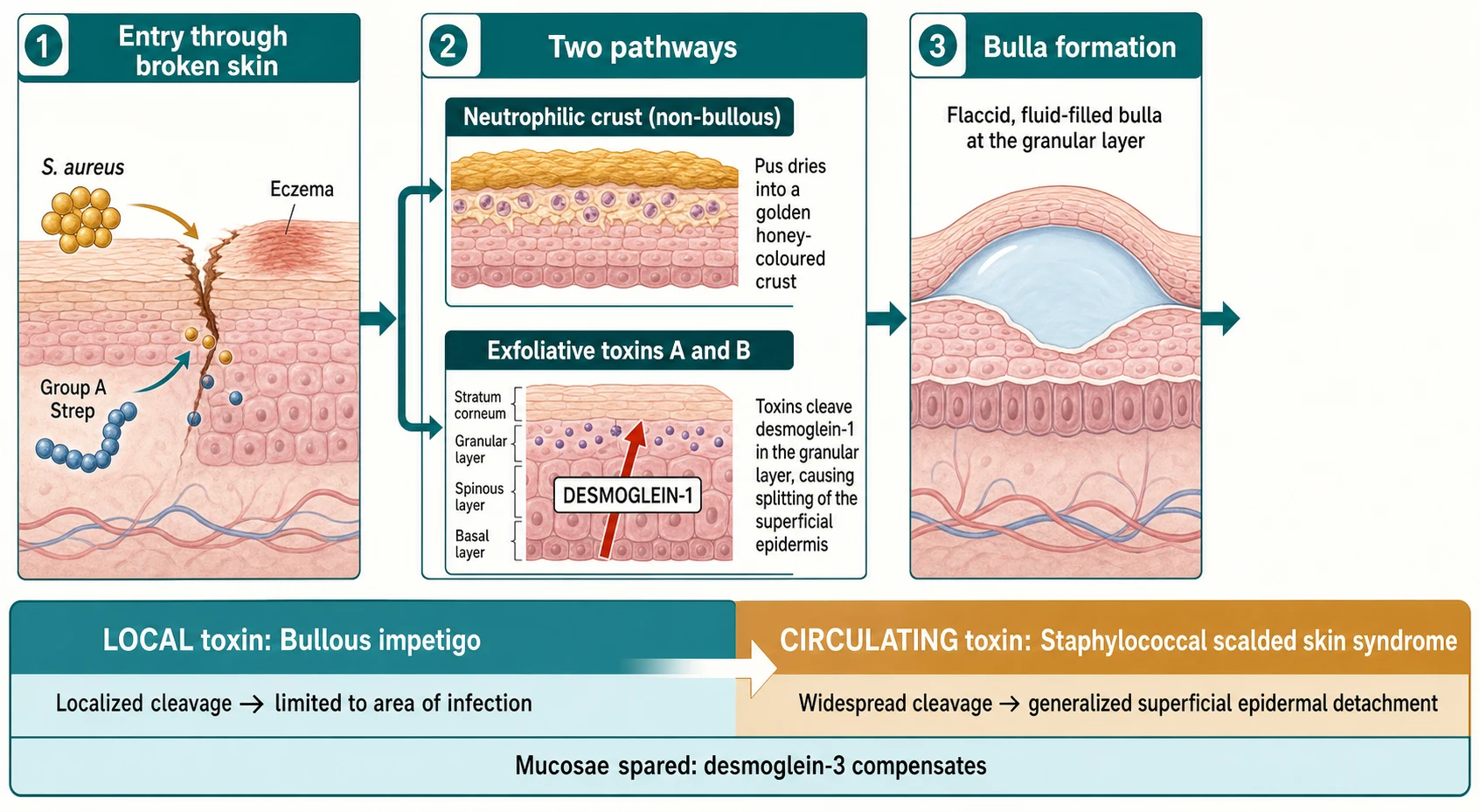
Two consequences follow that examiners test. First, the split occurs in the superficial granular layer, which is why staphylococcal scalded skin syndrome looks like a scald but is far less deep than toxic epidermal necrolysis, and why it heals rapidly once the toxin is cleared — the deeper epidermal stem cells are intact. Second, the mucous membranes are spared, because mucosal epithelium expresses desmoglein-3 as well as desmoglein-1, and the intact desmoglein-3 holds the cells together even when desmoglein-1 is cleaved. This mucosal sparing is the bedside clue that separates staphylococcal scalded skin syndrome from Stevens-Johnson syndrome and toxic epidermal necrolysis. [8]
The streptococcal side works differently. Group A streptococcus entering the skin provokes a brisk local pyogenic response and, in a minority of children, sets off an immune-complex glomerulonephritis one to three weeks later when antibody-streptococcal antigen complexes deposit in the glomerulus. Crucially, skin-derived group A streptococcal strains are nephritogenic but not rheumatogenic: impetigo can be followed by post-streptococcal glomerulonephritis but not by acute rheumatic fever, which follows throat infection alone. This single distinction organises the complication screen for every skin sore. [2] [4]
Clinical Presentation
The classic presentation lives on the face of a preschool child. A small papule or vesicle appears at the nose, mouth or an area of broken skin, ruptures within a day or two, and weeps a thin, yellow fluid that dries into the hallmark honey-coloured or golden crust on an erythematous base. The lesions spread centrifugally through auto-inoculation from scratching and through direct contact, and satellite lesions appear nearby. The child is typically afebrile and well, the lesions itch more than they hurt, and regional lymphadenopathy is common. [1] [2]
Bullous impetigo presents differently. Flaccid, translucent bullae up to several centimetres across arise on intact skin, often on the trunk, axillae, neck or diaper area in infants, with a narrow rim of surrounding erythema. The bullae rupture easily, leaving a thin collarette of scale and a moist, shiny base that dries to a varnish-like crust. The split is superficial, so the lesions heal without scarring. Because the disease is toxin-mediated, the lesions can be more widespread than the local staphylococcal focus would suggest. [8] [1]
Staphylococcal scalded skin syndrome is the presentation that must never be missed, and it belongs to the neonate and young infant. It begins with fever, irritability and skin tenderness, then a widespread, scarlatiniform, sandpaper-like erythema that is exquisitely tender to touch. Within a day or two large, flaccid bullae form and the skin wrinkles and shears off in sheets with gentle pressure (Nikolsky sign), particularly around the flexures, neck, perioral and periorbital regions. The child looks unwell, and the superficial loss behaves like a partial-thickness burn, demanding fluid, temperature and wound care alongside intravenous anti-staphylococcal therapy. [8]
The complications are part of the presentation because they often bring the child to care. Cellulitis and erysipelas mark deeper extension of infection; a furuncle or abscess marks a suppurative focus that needs drainage; and post-streptococcal glomerulonephritis arrives one to three weeks later with haematuria, oedema, hypertension and oliguria. A child presenting with puffy eyes, dark urine or a raised blood pressure after a recent skin sore must be assessed for glomerulonephritis regardless of how trivial the skin infection looked. [2] [4]
Differential Diagnosis
For the crusted lesion, the differential turns on morphology and distribution. Atopic dermatitis is itchy, flexural and chronic rather than crusted and weeping, though impetigo commonly complicates it — a sudden weeping, crusted flare in an atopic child is often secondary impetiginisation rather than an eczema exacerbation. Herpes simplex presents as clustered vesicles on an erythematous base, often painful rather than itchy, and recurs in the same site. Chickenpox lesions are in different stages simultaneously and are accompanied by fever. [1] [9]
For the blistering infant, the dangerous differential is the toxin and drug-reaction group. Staphylococcal scalded skin syndrome must be distinguished from Stevens-Johnson syndrome and toxic epidermal necrolysis, from toxic shock syndrome, and from severe Kawasaki disease with desquamation — the mucosal involvement and the drug exposure history are the clues. In a neonate, inherited blistering disorders such as epidermolysis bullosa present with blistering at sites of friction from birth, and bullous impetigo of the neonate can mimic them. A newborn with flaccid bullae needs careful assessment because the threshold to treat and admit is very low. [8] [4]
For the recurrent or abscess-forming child, community-acquired MRSA comes into the differential alongside the recurrent furunculosis of chronic staphylococcal carriage, hidradenitis suppurativa in older adolescents, and an underlying immunodeficiency in the child with unusually severe, persistent or atypical infection. Recurrent skin sepsis in a household should prompt consideration of MRSA colonisation and a decolonisation strategy rather than another round of antibiotics. [5] [7]
Clinical & Bedside Assessment
The assessment begins with a focused history and a good look at the skin. Ask about onset and evolution, itching or pain, spread pattern, and any break in the skin that preceded it — an insect bite, abrasion, scabies or atopic dermatitis. Ask about household, school and childcare contacts with similar lesions, because impetigo spreads through families and classrooms. And ask about systemic symptoms — fever, malaise, spreading redness, pain out of proportion — that flag the deeper or toxin-mediated disease. [2] [1]
Examine the whole skin, not just the obvious lesion. Describe the primary lesion (papule, vesicle, bulla, crust), its colour (honey-coloured crust is the classic), its base (erythematous), its distribution (face and exposed sites in non-bullous; trunk and intertriginous in bullous), and any regional lymphadenopathy. Look for the portals of entry — scabies burrows, eczematous fissures, chickenpox lesions — and for the signs of deeper extension: a spreading, warm, indurated border of cellulitis, fluctuance of an abscess, or the tender, peeling skin of staphylococcal scalded skin syndrome. [4] [8]
In the sick child, assess the systemic red flags directly. Fever, tachycardia, hypotension, lethargy and reduced perfusion signal invasive disease or toxin-mediated shock. In the neonate or young infant with widespread skin tenderness and peeling, assess hydration, temperature control and the surface area involved, because the superficial skin loss behaves like a burn and demands the same fluid and supportive discipline. A child with post-streptococcal glomerulonephritis presents weeks later, so a new skin sore warrants a blood pressure and, if symptomatic, a urinalysis. [8] [2]
Document the public-health essentials at the bedside. Record the date of onset, the number and distribution of lesions, school or childcare attendance, and the household contact picture. These details drive the advice on exclusion, the household decolonisation decision, and the follow-up plan for recurrent disease. A focused contact and environment history at the first encounter prevents the late realisation that the whole family is trading staphylococci. [1] [7]
Investigations
Impetigo is a clinical diagnosis, and routine swabs are not needed for uncomplicated disease. A swab for microscopy and culture is reserved for the atypical, the recurrent, the non-healing, the severe, and the case that has not responded to first-line treatment — these are the situations where knowing the organism and its sensitivities changes the management. The clinical diagnosis alone is enough to start empiric topical or oral therapy in the common, well child. [1] [9]
When a swab is taken, it should sample the active lesion — the base of a ruptured bulla or the moist surface beneath a crust — rather than dried crust alone. Culture identifies S. aureus and group A streptococcus and the antibiotic sensitivities that guide second-line therapy, including methicillin resistance. In recurrent or household-clustered disease, swabbing the nares and skin folds identifies staphylococcal carriage that a decolonisation strategy must address. [4] [7]
In Australia and New Zealand the National Healthy Skin Guideline and the Therapeutic Guidelines support clinical diagnosis with selective swabbing in endemic and recurrent settings. In remote communities where group A streptococcus predominates and scabies co-exists, assessment includes looking for and treating scabies, screening household contacts, and connecting the family to environmental health support — because the skin sore in these settings is the visible tip of a household and community problem. [2] [3]
Supportive tests are guided by severity. A child who is systemically unwell, has rapidly spreading cellulitis or a suspected toxin-mediated syndrome needs a full blood count, inflammatory markers, renal function and a blood culture before intravenous therapy. In suspected staphylococcal scalded skin syndrome a skin biopsy is not usually required to begin treatment — the clinical picture, the superficial split on frozen section if performed, and the mucosal sparing are enough — but biopsy may help where the differential from Stevens-Johnson syndrome is genuinely unclear. A child with suspected post-streptococcal glomerulonephritis needs urinalysis, serum creatinine, complement C3 and streptococcal serology. [8] [4]
Management — Resuscitation
Resuscitation belongs to the sick child, and in bacterial skin infection that means the toxin-mediated and invasive end of the spectrum. The red flags are a febrile, irritable infant with widespread tender erythema and sheet-like peeling; a rapidly spreading, painful, indurated plaque with systemic upset; fluctuance with sepsis; and the haemodynamic compromise of toxic shock. Any of these warrants urgent assessment, intravenous access and senior review. [8] [4]
For suspected staphylococcal scalded skin syndrome, admit and treat as a burn. Start intravenous anti-staphylococcal therapy — flucloxacillin (or vancomycin or clindamycin where MRSA is likely or the child is critically ill) — provide meticulous fluid, electrolyte and temperature management, apply non-adherent wound care and adequate analgesia, and monitor for secondary infection and heat and fluid loss. The superficial loss behaves like a partial-thickness burn even though the split is high in the epidermis, because the compromised barrier weeps and loses heat and water. [8]
For invasive cellulitis, necrotising infection or sepsis, give intravenous broad-spectrum therapy early, source-control any collection by drainage, and escalate to intensive care for the shocked child. Antibiotics for severe, rapidly spreading cellulitis in a child should cover streptococcus and staphylococcus, with MRSA cover added where locally prevalent or where the child has risk factors. Do not wait for culture in the child who is deteriorating. [4] [5]
Start the definitive therapy for uncomplicated impetigo promptly so that the contagious period is shortened and the household spread is contained, but keep resuscitation separate in your mind: the well child with crusted impetigo needs a cream or a short oral course, while the sick child with toxin-mediated or invasive disease needs the hospital, the intravenous line and the supportive bundle. [1] [8]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway matched to extent, organism and region, with stewardship discipline at every step. A few localised lesions take a short topical course; widespread, bullous or severe disease takes an oral antibiotic; an abscess takes drainage first; and recurrent or household disease adds a decolonisation layer. The art is choosing the least antibiotic that will work and no less. [1] [4]
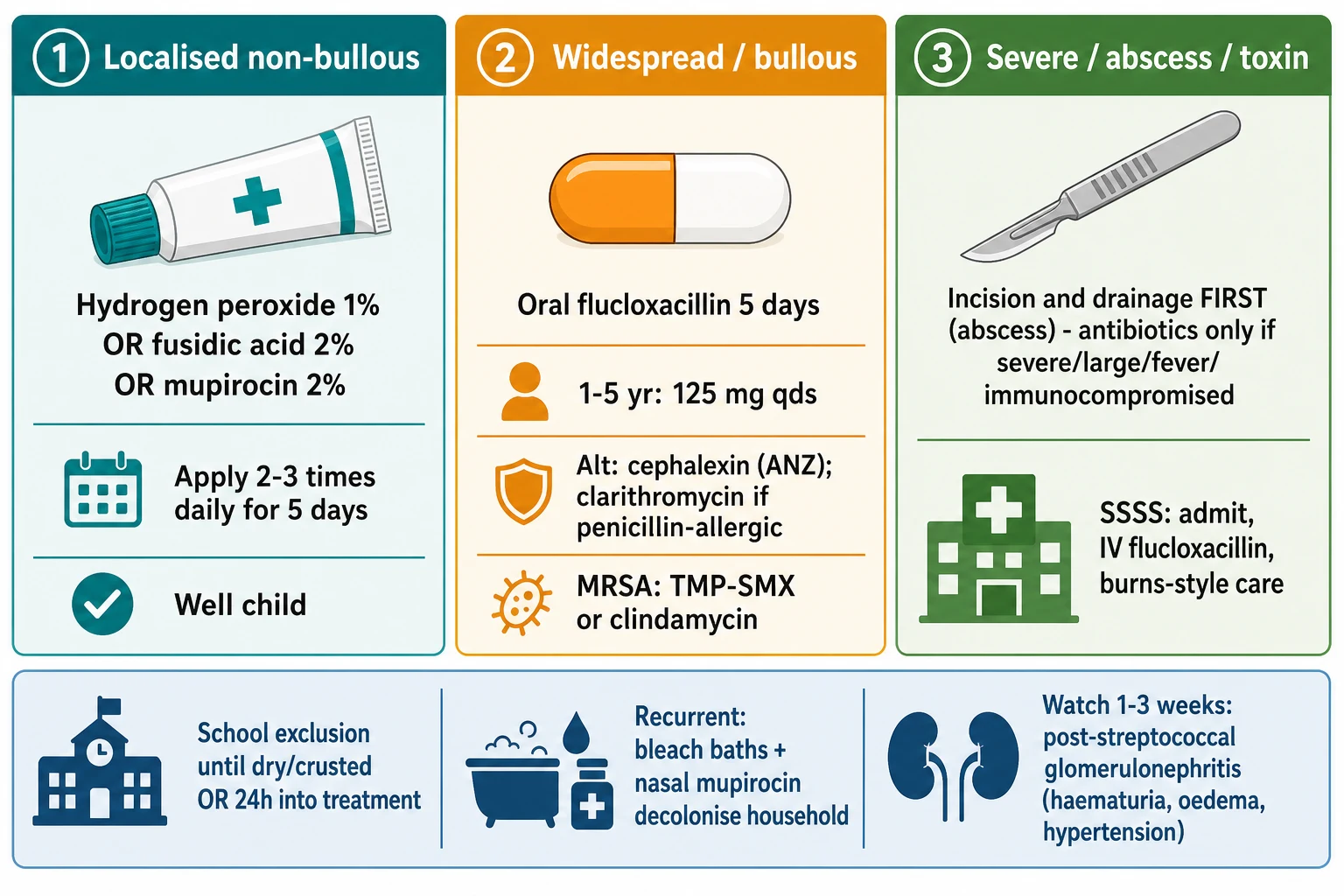
For localised non-bullous impetigo — a few discrete lesions and a well child — a short topical course is first-line. Current UK guidance (NICE) recommends topical hydrogen peroxide 1% cream applied two to three times daily for up to five days as first-line, with a topical antibiotic such as fusidic acid 2% applied three times daily for five days as the alternative where hydrogen peroxide is unsuitable. Where mupirocin is used (for example in Australasian practice or where MRSA is a consideration), it is applied three times daily for five days. Topical therapy limits systemic exposure and resistance, and it is enough for genuinely localised disease. [1] [9]
For widespread, bullous, severe or non-responsive impetigo, an oral anti-staphylococcal antibiotic is first-line. Oral flucloxacillin for five days is the standard first choice where staphylococcus and streptococcus are both possible: in the UK, child 1 month to 1 year 62.5 mg four times daily, 1 to 5 years 125 mg four times daily, 5 to 12 years 250 mg four times daily, and 12 to 17 years 500 mg four times daily. In Australasian practice cephalexin (25 mg/kg up to 500 mg twice daily for five days) or dicloxacillin or flucloxacillin is used. For the penicillin-allergic child, clarithromycin or erythromycin for five days is the alternative. [1] [3]
Impetigo antibiotic ladder (BNFc / NICE / eTG — confirm locally)
In remote endemic Australian and New Zealand communities, where group A streptococcal impetigo is prevalent and injection and clinic access shape care, the non-inferiority trial evidence supports a short three-day oral course of co-trimoxazole (trimethoprim 8 mg/kg/day plus sulfamethoxazole 40 mg/kg/day in two divided doses) as an alternative to intramuscular benzathine benzylpenicillin, with treatment of co-existing scabies and attention to environmental health. This regional pathway reflects both the organism and the logistics of remote care, and it is the basis of the National Healthy Skin Guideline approach. [3] [2]
For a skin abscess or furuncle, drainage is the treatment, not the antibiotic. Incision and drainage is first-line, and antibiotics are added only for the severity flags — large size, multiple lesions, extensive surrounding cellulitis, fever, immunocompromise, very young age, or failure of drainage — because placebo-controlled trials showed that antibiotics add only modest benefit to adequate drainage of small uncomplicated abscesses. Where an antibiotic is needed and community-acquired MRSA is plausible, trimethoprim-sulfamethoxazole or clindamycin is preferred over a beta-lactam, with clindamycin reserved where local inducible resistance has been excluded. [6] [12]
The stepwise impetigo and skin-infection pathway
Assess severity: a well child with localised lesions can be treated in the community; a febrile, toxic or rapidly spreading child goes to hospital.
Localised non-bullous impetigo: a five-day topical course (hydrogen peroxide 1% or fusidic acid 2%, or mupirocin 2% where used).
Widespread, bullous or non-responsive disease: five days of oral flucloxacillin (or cephalexin in ANZ practice; clarithromycin or erythromycin if penicillin-allergic).
Abscess or furuncle: incision and drainage first; add antibiotics only for severe, large, multiple, very-young or immunocompromised cases.
Where MRSA is suspected or proven: trimethoprim-sulfamethoxazole or clindamycin in place of a beta-lactam.
Recurrent or household disease: add a decolonisation strategy — antiseptic washes or bleach baths, nasal decolonisation, and treat household carriers.
Suspected SSSS: admit, give intravenous anti-staphylococcal therapy, and deliver burns-style fluid, wound and analgesia care.
Follow up: review healing, advise school exclusion, screen household contacts, and watch for post-streptococcal glomerulonephritis for one to three weeks.
For recurrent or household-clustered disease, a decolonisation strategy targets the staphylococcal carrier state rather than the single lesion. Chlorhexidine or dilute bleach baths (approximately five millilitres per litre of a five-percent household bleach in a full bath, soaking five to ten minutes, twice weekly for about a month) reduce recurrent infection, and intranasal mupirocin twice daily for five to seven days treats nasal carriage, applied to all colonised household members together to prevent re-seeding. The randomised trial evidence for bleach baths supports their place alongside routine hygiene in recurrent disease. [7]
Specific Subtypes & Scenarios
A preschool child with localised crusted impetigo. This is the bread-and-butter case. Confirm the clinical diagnosis, give a five-day topical course, advise gentle cleansing and hand hygiene, exclude from school or childcare until lesions are dry, crusted or healed (or until 24 hours after starting effective treatment, per local policy), and screen for the underlying portal of entry such as atopic dermatitis or scabies. Review healing at the end of the course. [1] [2]
An infant with bullous impetigo. Bullous disease reflects toxin-mediated staphylococcal infection and is usually treated with an oral anti-staphylococcal antibiotic rather than a topical alone. Confirm the lesions are superficial and the child is well; if the child is febrile, irritable, or has widespread tender erythema beyond the bullae, escalate to assessment for staphylococcal scalded skin syndrome. The threshold to treat bullous disease systemically, and to admit the unwell infant, is deliberately low. [8] [1]
A neonate or young infant with staphylococcal scalded skin syndrome. This is the presentation that goes to hospital. Admit for intravenous anti-staphylococcal therapy, burns-style fluid and temperature management, non-adherent wound care and analgesia, and monitor closely for secondary infection, electrolyte disturbance and heat loss. Identify and treat the primary staphylococcal focus — often a conjunctival, umbilical or skin focus. The outlook in children is good with prompt treatment, in contrast to the high mortality seen in adults with the same disease. [8]
A child with a skin abscess. Drainage is the treatment; antibiotics are adjunctive for the severity flags. Perform incision and drainage, send pus for culture where possible, and add an MRSA-active antibiotic (trimethoprim-sulfamethoxazole or clindamycin) for large, multiple, extensive, febrile, very-young or immunocompromised children. The placebo-controlled trial evidence shows antibiotics add only modest benefit to adequate drainage for small uncomplicated abscesses, so reserve them. [6] [12]
A child with community-acquired MRSA skin infection. Where MRSA is locally prevalent or the child has risk factors, choose an oral agent active against MRSA — trimethoprim-sulfamethoxazole (trimethoprim 8 to 12 mg/kg/day in two divided doses) or clindamycin (10 to 20 mg/kg/day, maximum 1.8 g/day, in three divided doses, where inducible resistance is excluded). The clindamycin-versus-trimethoprim-sulfamethoxazole trial in uncomplicated skin infection informed this choice, and the paediatric MRSA treatment literature supports both agents. [5] [10]
A child with recurrent furunculosis or a household cluster. Move from treating the lesion to treating the carrier and the environment. Combine antiseptic washes or bleach baths with intranasal mupirocin decolonisation of the child and all colonised household members, treat scabies if present, reinforce hygiene and wound care, and address any underlying skin disease such as atopic dermatitis. The bleach-bath trial evidence supports this combination approach. [7]
A child in a remote endemic community. Treat the skin sore within the household and environmental context: a short oral course of co-trimoxazole or intramuscular benzathine penicillin for streptococcal impetigo, treatment of scabies, screening and treatment of household contacts, and connection to environmental health support. The skin sore here is a public-health marker as much as an individual complaint, and the National Healthy Skin Guideline frames the integrated response. [2] [3]
Complications & Pitfalls
The most important complication is post-streptococcal glomerulonephritis, which follows skin infection with nephritogenic group A streptococcal strains one to three weeks after the sore. It presents with haematuria (often tea- or cola-coloured urine), oedema, hypertension and oliguria, and resolves spontaneously in most children, though a small proportion develop chronic kidney disease. A child presenting with these features after a recent skin sore needs urinalysis, blood pressure, renal function, complement C3 and streptococcal serology. [2] [4]
The cardinal pitfall is the false reassurance that impetigo is trivial. The same organism family produces staphylococcal scalded skin syndrome, toxin-mediated shock, cellulitis, necrotising infection and, weeks later, glomerulonephritis. A clinician who treats the crust and forgets to ask about systemic features, to look for tender peeling skin, or to warn the family about dark urine and puffy eyes has missed the part of the disease that harms. The crust is the visible problem; the toxin, the invasion and the immune complex are the hidden ones. [8] [2]
A second pitfall is overusing topical antibiotics. Fusidic-acid resistance in staphylococci rose in parallel with widespread topical use, which is why current guidance reserves topical antibiotics and, in the UK, prefers topical hydrogen peroxide first-line for localised disease. Repeated topical courses for recurrent disease drive resistance without addressing the carrier state, and they signal the need for a decolonisation strategy instead. [1] [9]
A third pitfall is treating an abscess with antibiotics alone. The cure for a suppurative collection is drainage, and a trial of a beta-lactam in a child with a fluctuant abscess — particularly where community-acquired MRSA is possible — delays the only intervention that reliably works. Antibiotics are adjunctive for the severity flags, never a substitute for incision and drainage. [6] [12]
A fourth pitfall is the wrong empiric agent where MRSA is prevalent. A beta-lactam does not cover community-acquired MRSA, so a child with risk factors or a non-resolving abscess in a high-prevalence region should receive trimethoprim-sulfamethoxazole or clindamycin rather than another flucloxacacin course. Knowing the local MRSA epidemiology is part of the prescription. [5] [10]
The final pitfall is conflating skin and throat streptococcal complications. Skin-derived group A streptococcal infection causes glomerulonephritis but not rheumatic fever; throat-derived infection causes both. A child with impetigo does not need rheumatic-fever prophylaxis, and a clinician who reaches for it has misapplied throat logic to the skin. [2] [4]
Prognosis & Disposition
Most impetigo heals completely within one to two weeks of effective treatment, and it heals without scarring because the split is superficial. The morbidity lies less in danger than in discomfort, contagiousness, spread through households and schools, and, in endemic communities, the cumulative burden of recurrent disease and its complications. For the well child the disposition is community management with topical or oral therapy and clear safety-netting. [1] [2]
Disposition follows severity. Admit the neonate or young infant with staphylococcal scalded skin syndrome, the child with invasive or rapidly spreading cellulitis, the child with sepsis or toxin-mediated shock, and the immunocompromised child with extensive disease. Manage at home the well child with localised or moderate impetigo, with oral therapy where needed and review at the end of the course. The threshold for admitting the very young and the immunocompromised is deliberately low. [8] [4]
At discharge, complete the antibiotic course, confirm healing, clear the school-exclusion advice, complete any household decolonisation, and give the family a clear safety-net for return — spreading redness, increasing pain, fever, lethargy, and, in the weeks that follow, dark urine, puffy eyes or a swollen face. Reinforce the underlying skin care, because controlling atopic dermatitis or scabies is what prevents the next impetigo. [1] [7]
Recurrence is common, particularly in the atopic child, in household carriers, and in endemic communities, because neither treatment nor natural infection confers durable immunity to staphylococcal or streptococcal colonisation. A decolonisation strategy, treatment of the underlying skin disease, and attention to household and environmental factors are what break the cycle of recurrence — not another antibiotic. [7] [2]
Special Populations
Neonates and young infants carry the highest risk of toxin-mediated disease. Staphylococcal scalded skin syndrome, bullous impetigo and invasive staphylococcal infection cluster here, and the threshold to assess, swab and admit is very low. A neonate with blistering or widespread tender erythema is a hospital patient until proven otherwise. [8]
Children with atopic dermatitis are the classic portal-of-entry group — the cracked, excoriated skin of poorly controlled eczema is repeatedly colonised and infected. The key is to treat the impetigo and to intensify eczema control at the same time, because secondary impetiginisation will recur as long as the barrier is broken. A weeping flare in an atopic child is often infection, not exacerbation. [1] [9]
Immunocompromised children are at risk of severe, persistent and atypical infection, and they warrant a lower threshold for systemic therapy, swabbing and admission. The organism may be unusual and the disease more invasive, so early culture and broad empiric therapy are appropriate when these children present with skin sepsis. [4] [5]
Aboriginal and Torres Strait Islander, Maori and Pasifika children, and refugee, asylum-seeking and migrant families carry disproportionate burden, particularly in remote communities where impetigo, scabies and post-streptococcal disease concentrate. Ensure culturally safe, equitable care delivered with the family and community, treat skin and scabies together, use trained interpreters, and address the environmental determinants — crowding, water access and housing — that sustain endemic disease. Disadvantage should never be the reason a skin sore becomes a renal or cardiac problem. [2] [3]
Children in remote and rural settings need pathways that work where they live. The choice between an oral short course and an intramuscular injection, the role of outreach and telehealth, and the connection to environmental health services all shape a plan that is deliverable in the community rather than one that depends on a distant clinic. Retrieval is mobilised early when a remote child deteriorates. [2] [3]
Evidence, Guidelines & Regional Differences
The treatment evidence for impetigo is anchored by the Cochrane review of interventions for impetigo, which found that topical and oral antibiotics both improve cure over placebo, that there is little to choose between topical agents, and that in many settings a short course of a single agent is effective. The systematic review of emerging treatment strategies across endemic and non-endemic settings frames the same question at the global level, confirming the effectiveness of short topical and oral courses while highlighting the place of newer agents such as ozenoxacin. [1] [9]
Co-trimoxazole versus benzathine penicillin for endemic impetigo (the DRUID/SRRT trial)
Population: Indigenous children in a remote Australian region with impetigo in a highly endemic setting, randomised to short-course oral co-trimoxazole versus intramuscular benzathine benzylpenicillin in a non-inferiority design.
Key finding
A three-day oral course of co-trimoxazole was non-inferior to a single intramuscular injection of benzathine benzylpenicillin for streptococcal impetigo, offering a practical oral alternative in remote endemic settings.
Practice change
Where streptococcal impetigo is endemic, a short oral co-trimoxazole course is a pragmatic, acceptable alternative to injection, and it underpins the National Healthy Skin Guideline regional pathway.
The abscess and MRSA evidence reshaped practice over a decade. The placebo-controlled trials of trimethoprim-sulfamethoxazole for uncomplicated skin abscess showed a modest benefit of antibiotics over placebo added to drainage, confirming drainage as the primary treatment and antibiotics as adjunctive for selected patients. The clindamycin-versus-trimethoprim-sulfamethoxazole trial in uncomplicated skin infection, the cephalexin-plus-trimethoprim-sulfamethoxazole-versus-cephalexin trial in cellulitis, and the paediatric MRSA treatment literature together support trimethoprim-sulfamethoxazole or clindamycin as oral therapy where MRSA is a concern. [5] [6]
TMP-SMX versus placebo for uncomplicated skin abscess
Population: Adults and children with small, uncomplicated skin abscesses undergoing incision and drainage, randomised to trimethoprim-sulfamethoxazole versus placebo for seven days.
Key finding
Trimethoprim-sulfamethoxazole improved clinical cure at seven to ten days compared with placebo, including in the subset with MRSA, though the absolute benefit over drainage alone was modest.
Practice change
Drainage remains the primary treatment of an abscess; add an MRSA-active antibiotic for the severity flags rather than routinely for every small abscess.
The recurrent-disease evidence supports a decolonisation strategy. The randomised trial of bleach baths plus routine hygiene versus hygiene alone in children with recurrent infection showed a reduction in recurrent skin infections, anchoring the place of dilute bleach baths alongside nasal decolonisation and household measures in the child who keeps coming back. [7]
The toxin-mediated disease evidence is summarised in the recent systematic review of paediatric staphylococcal scalded skin syndrome, which consolidates the clinical features, the work-up and the management — intravenous anti-staphylococcal therapy, supportive burn-style care and a generally favourable paediatric outcome — and confirms the diagnosis as clinical with biopsy reserved for the genuinely ambiguous case. [8]
The regional policy structure is consistent in principle and varies in detail. In the UK, NICE antimicrobial-prescribing guidance and the Clinical Knowledge Summary set the topical-first approach for localised impetigo and oral flucloxacillin for widespread disease. In Australia and New Zealand, the Therapeutic Guidelines and the National Healthy Skin Guideline set the local pathway, with a particular focus on the oral and intramuscular options and the integrated household approach for remote endemic disease. In the US, the IDSA skin and soft tissue infection guideline and AAP guidance set drainage-first management for abscess and the MRSA-active oral agents where indicated. In Canada, the Canadian Paediatric Society guidance mirrors this drainage-first, MRSA-aware approach. In every region the principle is the same: match the antibiotic to the extent and the organism, drain the pus, reserve topical therapy for localised disease, and watch for the post-streptococcal complication. [4] [1]
The controversies are real and active: the rising resistance that drives the preference for hydrogen peroxide and the restriction of topical fusidic acid; the optimal role of newer topical agents such as ozenoxacin; the balance between drainage and antibiotics for the small abscess; whether to decolonise and how aggressively; and the inequities in burden and access that leave remote and disadvantaged children carrying the disease. The defence against each is the same: stewardship-conscious empiric therapy, drainage where there is pus, a decolonisation layer for recurrence, and a public-health lens for the communities where impetigo is endemic. [9] [2]
Exam Pearls
- Impetigo is a superficial, contagious infection with two forms: non-bullous (honey-coloured crust, around seventy percent) caused by S. aureus or group A streptococcus, and bullous (flaccid bullae, around thirty percent) caused by exfoliative-toxin-producing S. aureus. [1]
- The mechanism uniting bullous impetigo and staphylococcal scalded skin syndrome is exfoliative toxins A and B cleaving desmoglein-1 in the granular layer; the difference is local toxin versus circulating toxin. [8]
- The diagnosis is clinical; swabs are for atypical, recurrent, severe or non-healing disease. [9]
- Localised non-bullous impetigo takes a five-day topical course (UK NICE: hydrogen peroxide 1% first-line; fusidic acid 2% or mupirocin 2% as alternatives). [1]
- Widespread, bullous or severe disease takes five days of oral flucloxacillin (or cephalexin in ANZ; clarithromycin or erythromycin if penicillin-allergic). [3]
- An abscess is treated by incision and drainage first; antibiotics are adjunctive for the severity flags — large, multiple, extensive cellulitis, fever, very young, immunocompromised. [6]
- Where community-acquired MRSA is suspected, use trimethoprim-sulfamethoxazole or clindamycin rather than a beta-lactam. [5]
- Staphylococcal scalded skin syndrome: a febrile, irritable neonate or young infant with widespread tender erythema, flaccid bullae, Nikolsky sign and spared mucosae — admit, give intravenous anti-staphylococcal therapy and burns-style care. [8]
- The key complication is post-streptococcal glomerulonephritis one to three weeks after skin infection (haematuria, oedema, hypertension) — and skin strep does not cause rheumatic fever, only throat strep does. [2]
- Recurrent or household disease needs a decolonisation strategy (bleach baths, intranasal mupirocin, household treatment), not repeated antibiotics. [7]
References
- [1]Koning S; van der Sande R; Verhagen AP; van Suijlekom-Smit LW; et al Interventions for impetigo. Cochrane Database Syst Rev, 2012.PMID 22258953
- [2]Bowen AC; Mahe A; Hay RJ; Andrews RM; et al The Global Epidemiology of Impetigo: A Systematic Review of the Population Prevalence of Impetigo and Pyoderma. PLoS One, 2015.PMID 26317533
- [3]Bowen AC; Tong SY; Andrews RM; O'Meara IM; et al Short-course oral co-trimoxazole versus intramuscular benzathine benzylpenicillin for impetigo in a highly endemic region: an open-label, randomised, controlled, non-inferiority trial. Lancet, 2014.PMID 25172376
- [4]Stevens DL; Bisno AL; Chambers HF; Dellinger EP; et al Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis, 2014.PMID 24973422
- [5]Miller LG; Daum RS; Creech CB; Young D; et al Clindamycin versus trimethoprim-sulfamethoxazole for uncomplicated skin infections. N Engl J Med, 2015.PMID 25785967
- [6]Talan DA; Mower WR; Krishnadasan A; Abrahamian FM; et al Trimethoprim-Sulfamethoxazole versus Placebo for Uncomplicated Skin Abscess. N Engl J Med, 2016.PMID 26962903
- [7]Kaplan SL; Forbes A; Hammerman WA; Lamberth L; et al Randomized trial of bleach baths plus routine hygienic measures vs. routine hygienic measures alone for prevention of recurrent infections. Clin Infect Dis, 2014.PMID 24265356
- [8]Gray L; Hansen AM; Cipriano SD Pediatric Staphylococcal Scalded Skin Syndrome: A Systematic Review of the Literature to Inform Work-Up and Management. Pediatr Dermatol, 2025.PMID 40650480
- [9]Gahlawat G; Tesfaye W; Bushell M; Abrha S; et al Emerging Treatment Strategies for Impetigo in Endemic and Nonendemic Settings: A Systematic Review. Clin Ther, 2021.PMID 34053699
- [10]Hyun DY; Mason EO; Forbes A; Kaplan SL Trimethoprim-sulfamethoxazole or clindamycin for treatment of community-acquired methicillin-resistant Staphylococcus aureus skin and soft tissue infections. Pediatr Infect Dis J, 2009.PMID 19057459
- [11]Moran GJ; Krishnadasan A; Mower WR; Abrahamian FM; et al Effect of Cephalexin Plus Trimethoprim-Sulfamethoxazole vs Cephalexin Alone on Clinical Cure of Uncomplicated Cellulitis: A Randomized Clinical Trial. JAMA, 2017.PMID 28535235
- [12]Daum RS; Miller LG; Immergluck L; Fritz S; et al A Placebo-Controlled Trial of Antibiotics for Smaller Skin Abscesses. N Engl J Med, 2017.PMID 28657870