Paeds · paediatric-dermatology
Molluscum contagiosum and viral warts
Also known as molluscum contagiosum · water warts · viral warts · verrucae · verruca vulgaris · common warts · plantar warts · plane warts
Two of the commonest benign, self-limiting viral skin infections of childhood — molluscum contagiosum (a poxvirus causing pearly umbilicated papules) and viral warts (human papillomavirus causing rough keratotic papules) — both managed by default with expectant care and treated actively only when symptomatic, spreading or bothersome.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
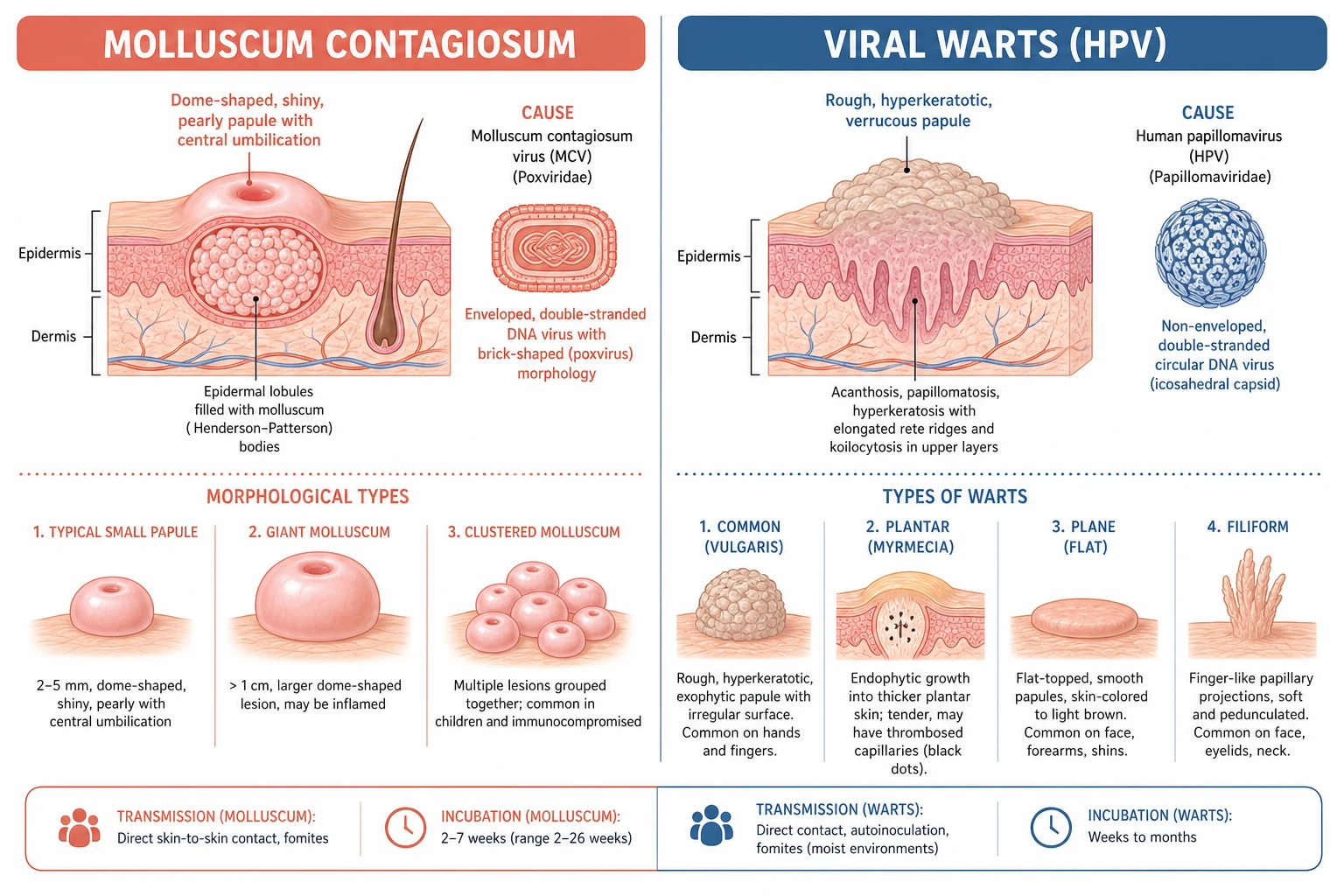
A parent brings a four-year-old to clinic worried about a cluster of small, shiny, pearly bumps in the armpit that have spread over several months, and a rough knob on the side of a thumb that will not go away. Both are everyday primary-care presentations, and both are benign, self-limiting viral infections of the skin. Molluscum contagiosum is a cutaneous infection by a DNA poxvirus that produces smooth, dome-shaped, umbilicated papules, while viral warts are benign epidermal growths driven by human papillomavirus that produce rough, keratotic papules. [2]
The unifying principle is that both conditions are common, contagious but harmless, and resolve spontaneously through cell-mediated immunity in the great majority of children. The central clinical decision is therefore not how aggressively to eradicate them but whether to treat at all: expectant, conservative management is the default, and active treatment is reserved for lesions that are symptomatic, spreading, or genuinely bothersome. A 2015 UK community cohort showed that molluscum has a measurable but modest effect on quality of life, framing reassurance and watchful waiting as a legitimate first choice rather than a default of omission. [3]
Classification
The two conditions are told apart by their morphology and their virus, and each is further sub-classified by site and by the human papillomavirus type that drives it. Molluscum contagiosum is caused by Molluscum contagiosum virus (MCV), a brick-shaped DNA virus of the genus Molluscipoxvirus, and is classified morphologically into typical small papules, clustered lesions that line up along scratches, and the rarer giant molluscum. Viral warts are caused by human papillomavirus (HPV), a circular double-stranded DNA virus, and are classified by clinical site and HPV type, because the type predicts where they grow and how they behave. [2]
The wart subtypes map cleanly onto HPV types and clinical appearance. Common warts (verruca vulgaris), the rough firm papules of the hands and fingers, are caused chiefly by HPV-2, HPV-27 and HPV-57. Plantar warts grow inward on the sole; the deep, painful myrmecia are typically HPV-1, while superficial mosaic warts form confluent plaques. Plane (flat) warts are the smooth, flat-topped, flesh-coloured papules of the face and limbs and are driven by HPV-3, HPV-10 and HPV-28, while filiform warts are finger-like projections on the face. [10]
Epidemiology & Risk Factors
Both conditions rank among the commonest skin complaints of childhood. Molluscum contagiosum peaks between one and ten years of age, with the highest burden in two- to five-year-olds, and a 2014 systematic review documented a rising prevalence in high-income countries that tracks with the broader increase in atopic disease and communal child-care exposure. Viral warts affect up to roughly one in three school-aged children at some point and are most frequent in older children and adolescents, with about two-thirds resolving spontaneously within two years through immune clearance. [1]
Transmission occurs by direct skin-to-skin contact, by autoinoculation through scratching, and by fomites; warts are classically linked to swimming pools, communal showers and moist, macerated skin, while molluscum spreads readily between siblings and through shared towels. Both are commoner in children with atopic dermatitis, whose defective epidermal barrier admits virus more easily, and the incubation period is long and variable — roughly two weeks to six months for molluscum and weeks to many months for warts. [2]
Pathophysiology
The two infections share a logic: a DNA virus enters damaged epidermis, hijacks keratinocyte replication, and produces a visible lesion while evading immunity until cell-mediated clearance finally switches on. In molluscum contagiosum, the virus infects the lower epidermal keratinocytes, and infected cells swell with large eosinophilic intracytoplasmic inclusions known as molluscum bodies (or Henderson-Patterson bodies). As these cells migrate upward, the overlying stratum corneum degenerates centrally and the viral core is extruded through the characteristic central umbilication. [2]
A key feature of molluscum is its evasion of host immunity. The virus produces proteins that dampen local inflammation and there is no viraemia, so lesions persist indolently for months with little surrounding redness — until the immune system finally recognises the infection, at which point an inflamed, eczematous halo around the lesions often heralds imminent resolution. This long immune-evasion phase is what makes expectant management rational: most lesions are simply waiting for immunity to catch up. [2]
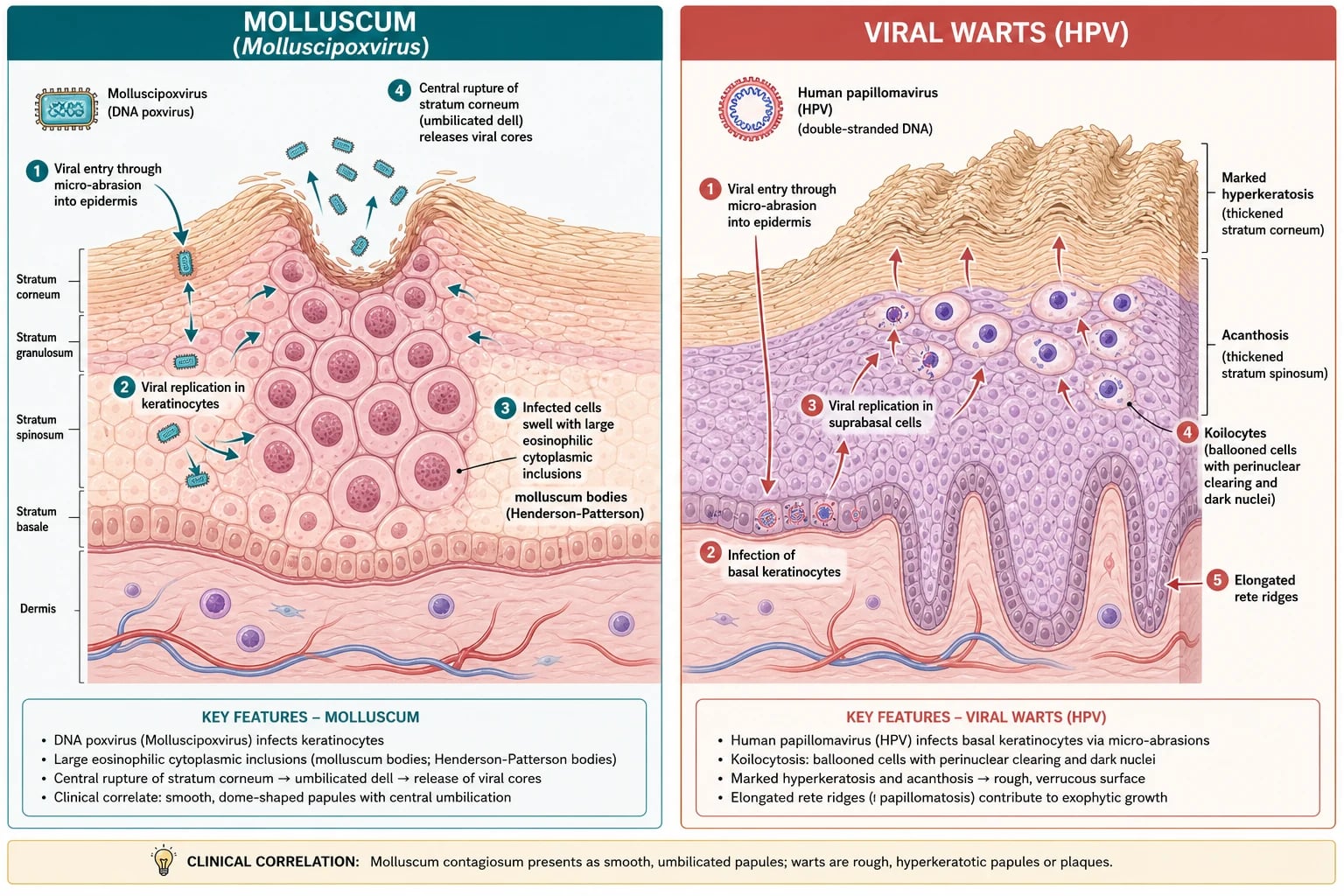
Viral warts follow the same logic with a different virus. Human papillomavirus enters the basal keratinocytes through micro-trauma, and its DNA drives keratinocyte proliferation and abnormal keratinisation. Histologically, the lesion shows koilocytes — ballooned cells with pyknotic, raisin-like nuclei — together with hyperkeratosis, acanthosis, papillomatosis and elongated rete ridges, which together build the rough, exophytic surface. As with molluscum, spontaneous regression depends on a cell-mediated, Th1-type immune response, which explains why warts may persist for years and then vanish abruptly. [10]
VIRAL — why these lesions self-limit
Clinical Presentation
Molluscum contagiosum presents as small, firm, two- to five-millimetre, pearly, flesh-coloured papules, each with a glistening central dell. They are usually painless and may be numerous, clustering in the axillae, on the neck, trunk and flexures, and in the ano-genital area, and they often line up along the line of a scratch through the Koebner phenomenon. Most children are otherwise entirely well, though the lesions may itch or become inflamed as the immune system begins to clear them. [2]
Common warts appear as firm, rough, hyperkeratotic papules, classically on the fingers and the back of the hands, with tiny black dots on the surface that are thrombosed capillary loops. Plantar warts grow inward under pressure: they are tender, yellow-brown papules surrounded by a collar of hyperkeratosis, and the deep myrmecia caused by HPV-1 can be exquisitely painful; when several coalesce into a mosaic plaque they become notoriously resistant. Plane warts are multiple, smooth, flat-topped, flesh-coloured papules on the face and limbs, and filiform warts are finger-like projections, usually on the face and neck. [12]
The features that should prompt a second look rather than routine reassurance are the atypical ones. A lesion that is rapidly growing, bleeding, ulcerated or fixed; a wart that is relentlessly periungual or resists twelve weeks of standard therapy; and extensive, giant or confluent molluscum, particularly in early infancy or an immunosuppressed child, all warrant assessment for a mimic or an underlying immune defect. [2]
Differential Diagnosis
For molluscum, the common mimics are folliculitis, acne, small epidermoid cysts and syringomas, all distinguished by the absence of the central umbilication and the white cheesy core. In an immunocompromised host, disseminated fungal infections such as cryptococcosis or histoplasmosis can mimic molluscum, and a biopsy is warranted when a lesion looks atypical or fails to behave like molluscum should. Ano-genital molluscum in a prepubertal child is usually autoinoculated from elsewhere on the body and does not by itself imply abuse, but the context must be assessed with safeguarding in mind. [2]
For warts, the principal mimic on the sole is the corn or callus, and the two are separated by paring: a wart interrupts the normal skin lines and reveals black thrombosed capillaries and pinpoint bleeding, whereas a corn preserves the dermatoglyphics and shows a clear, hard central core with no bleeding. Plane warts may be confused with lichen planus, which is violaceous, itchy and shows Wickham striae, or with pityriasis versicolor. The most important wart mimic not to miss is a verrucous carcinoma or squamous cell carcinoma masquerading as a treatment-resistant wart, particularly in an immunosuppressed child — any atypical, bleeding or fixed lesion must be biopsied. [12]
Clinical & Bedside Assessment
Both diagnoses are clinical, made on morphology at the bedside, and neither demands investigation in the typical case. The focused assessment documents the number and distribution of lesions, their sites, any secondary inflammation or infection, the presence of itch or pain, and the functional and social impact — whether the child is being kept out of swimming, whether the lesions are visible and distressing, and how the family is coping. A coexisting atopic dermatitis should be sought, because it raises both incidence and the risk of treatment irritation. [2]
A few simple bedside manoeuvres sharpen the diagnosis. Expressing or curetting the central core of a molluscum yields the white, cheesy material of viral bodies, while paring a wart reveals the black capillary dots and pinpoint bleeding that confirm it. Dermoscopy can help in difficult cases: molluscum shows a central white-yellow amorphous umbilication fringed by radial vessels, and warts show thrombosed capillaries and a disrupted pattern. [12]
The assessment must also weigh the immune context. Extensive, giant or refractory lesions, or disease presenting in early infancy, should prompt consideration of an underlying immunodeficiency rather than escalation of topical therapy, and ano-genital lesions require a thoughtful, safeguarding-aware history without any presumption of abuse. The goal of assessment is to confirm the benign diagnosis, exclude the mimics and the immunocompromised host, and decide with the family whether the bother of the lesions justifies the bother of treatment. [2]
Investigations
In the great majority of children no investigations are needed at all, because the diagnosis is clinical and the condition is self-limiting. The role of testing is confined to the atypical, the refractory and the immunocompromised, where the question is no longer "what is this rash?" but "could this be something else, or could this child have an immune defect?". [12]
Skin scrapings with potassium hydroxide preparation can confirm either diagnosis when it is in doubt: molluscum shows the large ovoid intracytoplasmic inclusion bodies, and warts show koilocytes. Polymerase chain reaction for HPV typing is not routine but can be useful in persistent, anogenital or atypical warts, or when counselling about human papillomavirus vaccination. A diagnostic biopsy, examined histopathologically, is reserved for atypical, rapidly changing, bleeding or treatment-resistant lesions to exclude a squamous or verrucous carcinoma, and HIV testing should be considered when molluscum is extensive or giant or when warts are unusually refractory. [2]
Management — Resuscitation
Neither condition is a resuscitation emergency in an immunocompetent child, so the acute priority is to exclude the mimics and the immunocompromised host rather than to intervene physically. A child with extensive, giant or refractory molluscum or warts, or disease beginning in the first year of life, should be evaluated for an underlying immunodeficiency — HIV, DOCK8 deficiency or a combined immunodeficiency — before any escalation of topical therapy, because the skin may be the first sign of a systemic immune problem. [2]
The genuinely acute problems are secondary infection and the rare mimic. Scratching or picking at lesions may produce impetiginisation or cellulitis, which requires oral antistaphylococcal and antistreptococcal antibiotics such as flucloxacillin, not topical molluscum or wart therapy. Atopic children carry a higher risk of secondary herpetic infection of broken skin (eczema herpeticum), which is not caused by these viruses but complicates the same disrupted barrier and demands prompt systemic aciclovir. [12]
For ano-genital lesions, the acute task is thoughtful, safeguarding-aware management: most childhood ano-genital molluscum and warts are autoinoculated, so infection-control advice and conservative treatment are appropriate, but local child-protection guidance must be followed whenever the history, examination or distribution raises concern. [2]
Management — Definitive & Stepwise
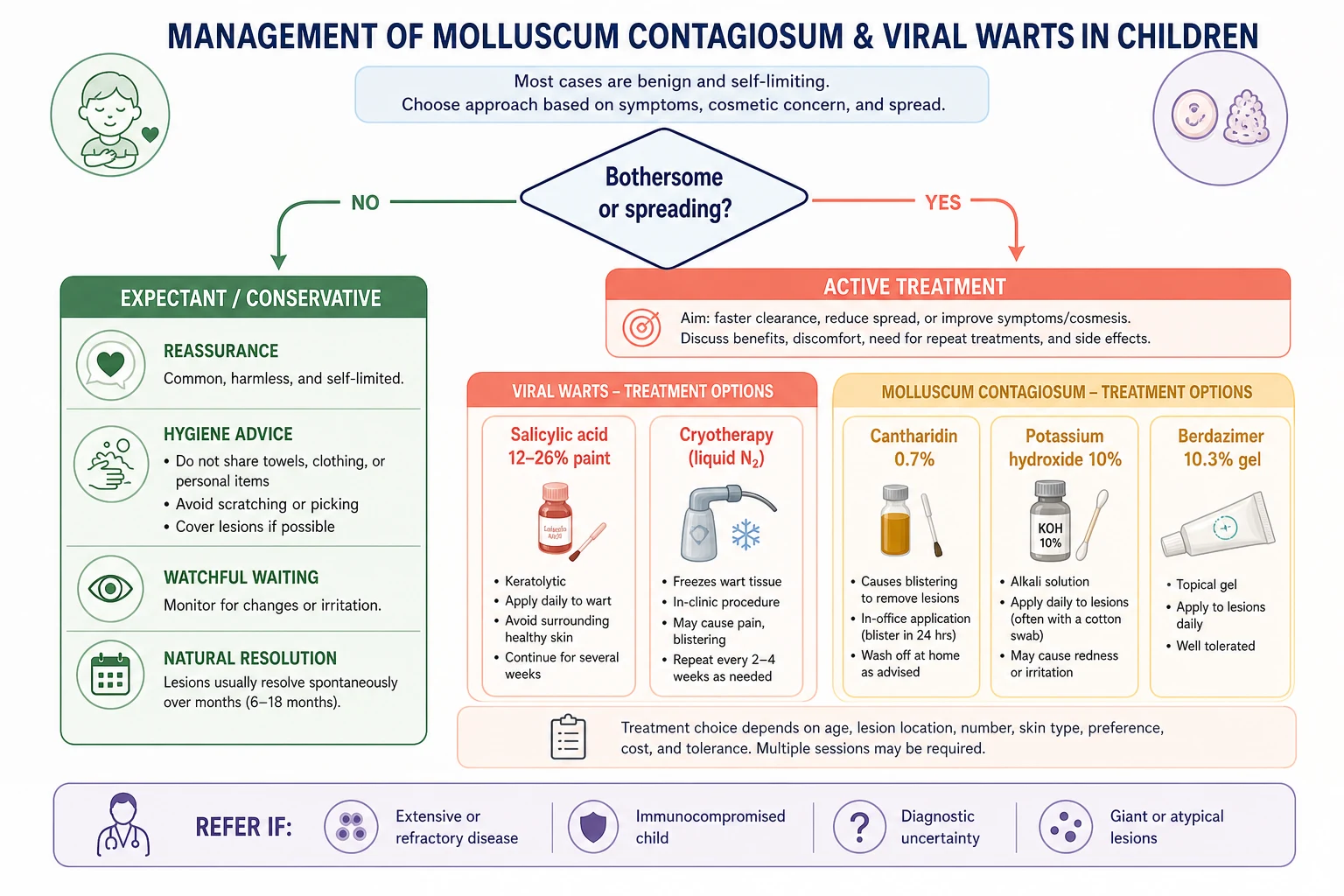
The first and default step for both conditions is expectant, conservative care. Reassure the family that the lesions are benign and self-limiting, give practical hygiene advice — no sharing of towels or flannels, avoid scratching and picking, cover lesions where practical, and encourage hand-washing — and offer review rather than immediate treatment. This is not a default of inaction but an evidence-based choice, because the natural history of both conditions is spontaneous resolution and because every active treatment carries the risk of irritation, scarring or disappointment. [2]
The decision to treat actively is made with the family on the basis of bother: treat when lesions are painful or itchy, when they are spreading despite conservative measures, when they are cosmetically distressing, or when they restrict activities such as swimming or sport. A shared decision that weighs the modest efficacy and the local side-effects of therapy against the natural history is the hallmark of good management, and a clear explanation that most treatments take many weeks is essential to maintain adherence and trust. [7]
Wart treatment ladder
Step 1 expectant: reassurance and hygiene advice; review, especially in young children where two-thirds clear within 2 years
Step 2 first-line active: salicylic acid 12-26% paint or plaster applied daily after soaking and paring the wart
Step 3 cryotherapy: liquid nitrogen every 2-4 weeks for persistent or bothersome warts
Step 4 second-line: cantharidin, formaldehyde or glutaraldehyde, imiquimod, 5-fluorouracil, bleomycin, laser or photodynamic therapy
Refer: periungual impairment, painful plantar or mosaic warts, immunocompromise, or failure of 12 weeks of standard therapy
Molluscum treatment ladder
Step 1 expectant: reassurance; median time to resolution about 13 months, with most clear by 2 years
Step 2 physical: cantharidin 0.7% topical solution applied in the office and washed off, or cryotherapy, or curettage
Step 3 topical home therapy: potassium hydroxide 10% solution, or berdazimer 10.3% gel applied once daily
Avoid routinely: imiquimod (no benefit over placebo in RCTs) and podophyllotoxin (toxic in children)
Refer: extensive, giant or confluent disease, immunocompromise, diagnostic uncertainty, or refractory lesions
For warts, the stepwise ladder begins with salicylic acid — a 12 to 26 per cent paint or plaster applied daily to the soaked and pared wart — and moves to cryotherapy with liquid nitrogen every two to four weeks for persistent or bothersome lesions. The Cochrane review found salicylic acid modestly superior to placebo but the evidence for cryotherapy being better than salicylic acid was weak, and the randomised EVerT trial found no clear difference between cryotherapy and salicylic acid for plantar warts. Second-line options include cantharidin, formaldehyde and glutaraldehyde, imiquimod, 5-fluorouracil, bleomycin, and laser or photodynamic therapy. [8]
For molluscum, the ladder begins with the expectation of resolution and moves to physical measures — cantharidin 0.7 per cent topical solution (the in-office agent YCANTH, approved in 2023) applied and washed off, cryotherapy, or curettage — and then to home-applied topicals. Potassium hydroxide 10 per cent solution was shown in a placebo-controlled randomised trial to be modestly effective but to cause local irritation, and berdazimer 10.3 per cent gel — the first home prescription topical, approved in 2023 — demonstrated efficacy in an integrated analysis of three randomised trials, including in children with atopic dermatitis. Imiquimod should not be used routinely, because randomised trials showed no benefit over placebo in molluscum, and podophyllotoxin is avoided because of toxicity. [5]
Specific Subtypes & Scenarios
Each wart subtype carries its own practical slant. Common warts on the hands respond well to salicylic acid and, if persistent, to cryotherapy, but watchful waiting is entirely reasonable in a young child. Plantar warts — especially the deep HPV-1 myrmecia and the confluent mosaic plaques — are the hardest to clear and may need paring combined with salicylic acid or cryotherapy, with cantharidin or specialist referral for resistant disease. Plane warts on the face should be managed cautiously and often conservatively, because destructive therapy risks scarring and pigment change; a mild topical retinoid or simple observation is usually wiser than cryotherapy on facial skin. [12]
Filiform warts, the finger-like projections of the face and neck, are best removed by snip excision or light cryotherapy, again with care for scarring on visible skin. Ano-genital molluscum and warts in children are usually autoinoculated and should be managed conservatively, with safeguarding assessed thoughtfully rather than assumed; podophyllotoxin is toxic and avoided, and imiquimod is not used on mucosal surfaces in routine paediatric care. Giant molluscum — lesions greater than ten millimetres — and confluent or extensive disease, particularly in an immunocompromised host, warrant investigation for immunodeficiency and specialist input from dermatology and immunology. [2]
Complications & Pitfalls
A child who scratches molluscum until it spreads to a sibling, a child whose cryotherapy leaves a pale scar on dark skin, and a child whose extensive, bleeding "wart" turns out to be a carcinoma — these are the three ways molluscum and warts go wrong. The disease itself spreads by autoinoculation and between siblings through scratching and shared towels, and the Koebner phenomenon lines molluscum and warts up along the line of trauma; secondary bacterial infection from scratching produces impetigo or cellulitis. The inflammatory halo that appears around molluscum as immunity engages is benign and often a sign of imminent clearance, not a complication. [2]
The treatment complications are largely iatrogenic and avoidable. Scarring and pigment change — especially post-inflammatory hyper- or hypopigmentation — follow over-aggressive destructive therapy, particularly cryotherapy on darker skin, runoff of cantharidin onto surrounding skin, and curettage. Matching the intensity of treatment to the lesion and the site, protecting surrounding skin, and stepping back once the lesions are clear are the safeguards against trading a self-limiting bump for a permanent scar. [12]
Complications and how to avoid them
The two great pitfalls are mirror images of each other. The first is over-treating self-limiting disease more aggressively than the disease itself, generating scars, pigment change and parental anxiety for lesions that would have vanished on their own. The second is under-investigating the child whose disease is genuinely atypical: extensive or giant molluscum, or a wart that bleeds, ulcerates or resists twelve weeks of therapy, may be the first sign of immunodeficiency or of a verrucous or squamous cell carcinoma, and must be biopsied or investigated rather than treated harder. [2]
Prognosis & Disposition
The prognosis is excellent for both conditions in the immunocompetent child. Molluscum contagiosum is self-limiting, with a median time to resolution of about thirteen months — roughly half of children clear within one year and the great majority within two — and although the effect on quality of life is measurable, it is modest. Childhood warts resolve spontaneously in about two-thirds of cases within two years through cell-mediated immunity, though plantar and mosaic warts are more persistent and may linger for years in a minority. [3]
Disposition is overwhelmingly primary care. Most children are managed with reassurance and review in general practice or the community, with referral to paediatric dermatology reserved for refractory, extensive, painful or atypical lesions, for periungual or plantar disease that impairs function, and for the immunocompromised host. A clear safety-net is essential: advise families to return for any lesion that is rapidly enlarging, bleeding, ulcerated or painful, or for any sign of spreading secondary infection. [12]
Recurrence is possible, because human papillomavirus can remain latent and re-exposure is common, but the long-term outlook in an immunocompetent child is complete resolution without sequelae — provided the treatment has been kinder than the disease. [2]
Special Populations
Children with atopic dermatitis develop both molluscum and warts more often than their peers, because the barrier defect that defines eczema gives viruses easier entry, and their eczematous skin tolerates topical therapy less well. Managing the underlying eczema is part of managing these infections, and treatment choices must respect the fragility of atopic skin. [6]
Immunocompromised children — those with HIV, a primary immunodeficiency, or iatrogenic immunosuppression — present with extensive, giant, refractory or atypical lesions, and the approach shifts from conservative dermatology to investigating and supporting the immune system with specialist input. Extensive molluscum in particular is a recognised cutaneous sign of HIV and of DOCK8 deficiency, and warrants HIV testing and immunology referral. Epidermodysplasia verruciformis, a rare genetic susceptibility to human papillomavirus caused by mutations in EVER1, EVER2, TMC6 or TMC8, produces widespread plane-wart-like lesions with a lifelong risk of malignant transformation and demands dermatology and oncology surveillance. [2]
Indigenous and remote-area children often carry a heavy burden of coexisting bacterial skin sepsis and scabies, so the viral lesions are best managed within a community, culturally safe Healthy Skin programme that treats the whole skin rather than the single diagnosis. Refugee, migrant and asylum-seeking children may have had limited access to care and present with more advanced disease, and the consultation must accommodate language and health-literacy barriers with practical, sustainable advice. Adolescents with genital lesions raise the question of sexual transmission and the opportunity to offer human papillomavirus vaccination according to the national schedule. [12]
Evidence, Guidelines & Regional Differences
The evidence base for molluscum is limited but improving. A 2023 systematic review and network meta-analysis found that several active agents were superior to placebo but that no single treatment clearly dominated, reinforcing expectant management as a legitimate first choice. The modern therapeutic story is the 2023 regulatory approval of two agents: cantharidin 0.7 per cent topical solution (YCANTH) for in-office use, and berdazimer 10.3 per cent gel (Zelsuvmi) as the first home prescription topical, supported by a 2024 integrated analysis of three randomised trials and a dedicated analysis in children with atopic dermatitis. Earlier randomised work established potassium hydroxide 10 per cent as modestly effective but irritant, and — importantly — showed that imiquimod was no better than placebo. [7]
For warts, the Cochrane review of topical treatments found salicylic acid modestly superior to placebo but judged the evidence for cryotherapy, and for cryotherapy over salicylic acid, to be weak. The randomised EVerT trial and its economic evaluation found no clear clinical or cost-effectiveness advantage of cryotherapy over salicylic acid for plantar warts, and a randomised paediatric study compared cryotherapy with imiquimod combined with a keratolytic. The popular duct-tape occlusion method has weak and inconsistent trial evidence and is best regarded as a low-harm home measure rather than a proven standard. [8]
Regional practice is broadly convergent on conservative-first care. The United Kingdom NICE Clinical Knowledge Summaries and the Australian Therapeutic Guidelines both recommend reassurance and hygiene as the default, with active treatment guided by bother rather than by lesion count, and the American and British Academies of Dermatology emphasise matching treatment intensity to the site and avoiding scarring. The shared message across regions is that these are benign, self-limiting infections and that the harm of over-treatment is real. [2]
Exam Pearls
For written and viva exams, the high-yield facts cluster around the virus, the morphology and the principle of conservative-first care. Be ready to name Molluscum contagiosum virus as a DNA poxvirus of the genus Molluscipoxvirus, to describe the pearly umbilicated papule, and to name the molluscum (Henderson-Patterson) bodies seen on cytology; and to name human papillomavirus as the cause of warts, to give the type associations — common HPV-2, 27 and 57, plantar or myrmecia HPV-1, plane HPV-3, 10 and 28 — and to describe koilocytes on histology. [2]
The management answer examiners reward is the stepwise, bother-driven ladder. For warts, salicylic acid 12 to 26 per cent is first-line, cryotherapy with liquid nitrogen every two to four weeks is second, and the EVerT trial showed no clear benefit of cryotherapy over salicylic acid for plantar warts. For molluscum, the ladder is expectant care, then cantharidin 0.7 per cent or cryotherapy, then potassium hydroxide 10 per cent or berdazimer 10.3 per cent gel, with imiquimod explicitly not recommended because randomised trials were negative. The black dots on a wart are thrombosed capillaries, and paring distinguishes a wart (interrupted skin lines, pinpoint bleeding) from a corn (preserved lines, clear core). [8]
Finally, name the red flags. Extensive, giant or refractory molluscum, or a wart that bleeds, ulcerates or resists twelve weeks of therapy, demands investigation for immunodeficiency and for a squamous or verrucous carcinoma mimic. The single principle that ties the topic together is that these are benign, self-limiting, transmissible childhood infections, and the goal of treatment is to be kinder than the disease. [2]
References
- [1]Olsen JR, Gallacher J, Piguet V, et al Epidemiology of molluscum contagiosum in children: a systematic review Fam Pract, 2014.PMID 24297468
- [2]Schaffer JV, Berger EM Molluscum Contagiosum JAMA Dermatol, 2016.PMID 27627044
- [3]Olsen JR, Gallacher J, Finlay AY, et al Time to resolution and effect on quality of life of molluscum contagiosum in children in the UK: a prospective community cohort study Lancet Infect Dis, 2015.PMID 25541478
- [4]Giner-Soriano M, Teixidó C, Marsal JR, et al Randomized placebo-controlled clinical trial on efficacy and safety of topical 10% Potassium hydroxide for molluscum contagiosum treatment in children J Dermatolog Treat, 2019.PMID 30668179
- [5]Sugarman JL, Hebert A, Browning JC, et al Berdazimer gel for molluscum contagiosum: An integrated analysis of 3 randomized controlled trials J Am Acad Dermatol, 2024.PMID 37804936
- [6]Paller AS, Green LJ, Silverberg N, et al Berdazimer gel for molluscum contagiosum in patients with atopic dermatitis Pediatr Dermatol, 2024.PMID 38413239
- [7]Chao YC, Ko MJ, Tsai WC, et al Comparative efficacy of treatments for molluscum contagiosum: A systematic review and network meta-analysis J Dtsch Dermatol Ges, 2023.PMID 37199262
- [8]Kwok CS, Gibbs S, Bennett C, et al Topical treatments for cutaneous warts Cochrane Database Syst Rev, 2012.PMID 22972052
- [9]Stefanaki C, Lagogiani I, Kouris A, et al Cryotherapy versus imiquimod 5% cream combined with a keratolytic lotion in cutaneous warts in children: A randomized study J Dermatolog Treat, 2016.PMID 25886088
- [10]Egawa N, Doorbar J The low-risk papillomaviruses Virus Res, 2017.PMID 28040475
- [11]Stamuli E, Cockayne S, Hewitt C, et al Cost-effectiveness of cryotherapy versus salicylic acid for the treatment of plantar warts: economic evaluation alongside a randomised controlled trial (EVerT trial) J Foot Ankle Res, 2012.PMID 22369511
- [12]Loo SK, Tang WY Warts (non-genital) BMJ Clin Evid, 2014.PMID 24921240