Paeds · paediatric-dermatology
Nail disorders in children
Also known as Paediatric nail disease · Onychomycosis in children · Trachyonychia · Twenty-nail dystrophy · Ingrown toenail · Paronychia · Longitudinal melanonychia in children
Fellowship topic on nail disorders in children: the nail unit anatomy and the site-based diagnostic principle that matrix lesions change nail shape and surface, nail bed lesions change colour and attachment, and nail fold lesions cause swelling and infection; the classification of paediatric nail disorders into normal and developmental variants, traumatic, infectious (acute and chronic paronychia, onychomycosis), inflammatory and skin-disease associated (psoriasis, alopecia areata, lichen planus, trachyonychia), congenital and genetic (congenital malalignment of the great toenail, nail-patella syndrome, pachyonychia congenita), nail tumours (pyogenic granuloma, subungual exostosis, viral warts, longitudinal melanonychia and the nail matrix naevus) and systemic nail signs (clubbing, koilonychia, Beau lines); the confirm-before-treat principle for onychomycosis with mycology before systemic therapy and weight-based terbinafine or itraconazole; the conservative-first management of the ingrown toenail with wedge excision and phenolisation for recurrent disease; the reassurance and topical steroid approach to idiopathic trachyonychia; the recognition that longitudinal melanonychia in a child is usually benign; the red flags for urgent referral; and the ANZ and international dermatology guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
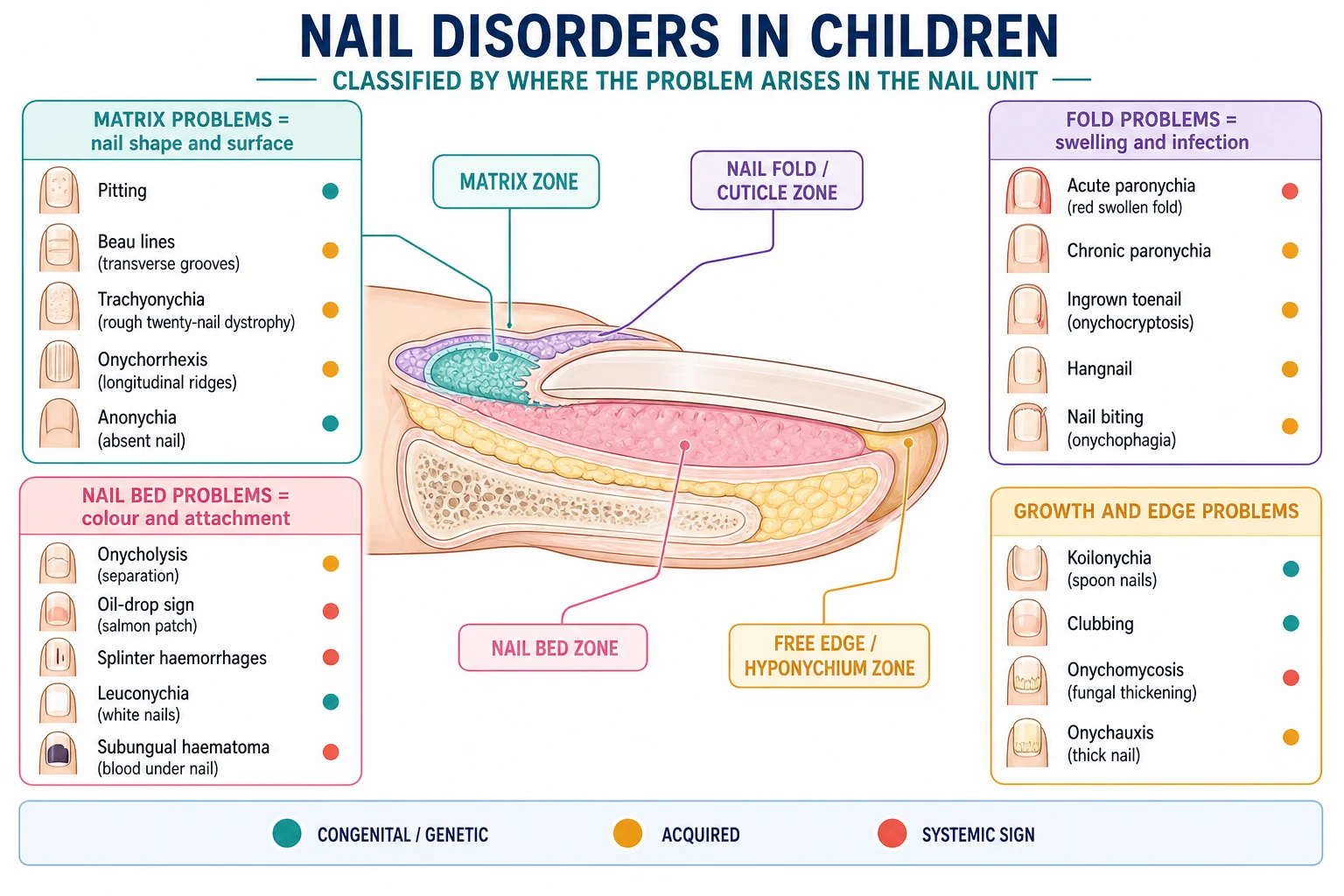
Where the lesion is, that is what you see
Overview & Definition
Picture a ten-year-old brought in because one toenail has turned thick and yellow, or a teenager whose great toe is red and weeping where the nail digs in, or a five-year-old whose twenty nails look rough and sandpaper-like. None of these are dangerous, yet each can disrupt a child's comfort, sport and self-image, and each is solved faster once you know where in the nail unit the problem lives. [1] [2]
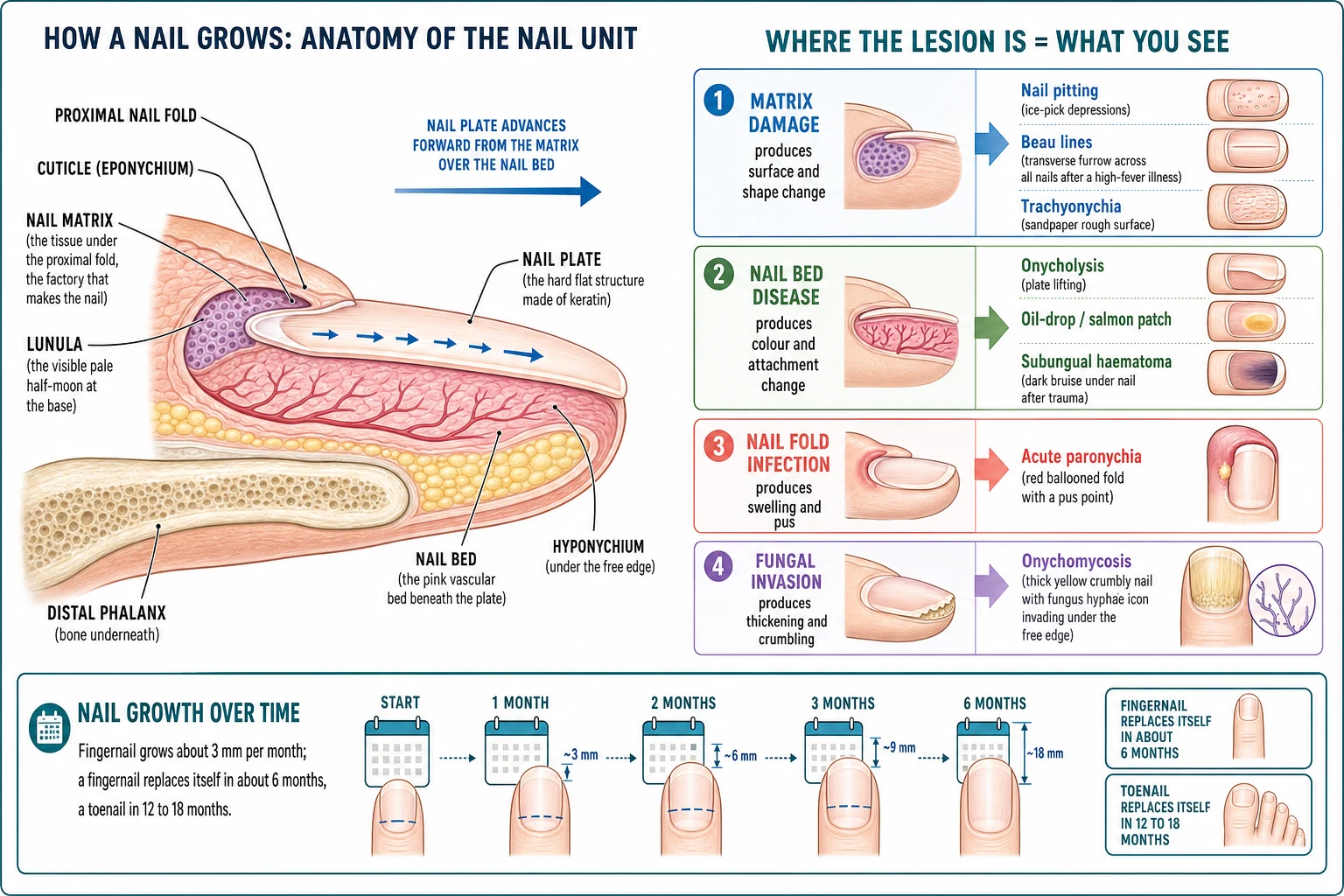
The nail unit is a small but intricate structure. The nail matrix is the germinative epithelium tucked under the proximal nail fold that generates the nail plate; its distal edge shows through the nail as the pale half-moon called the lunula. The nail plate is the hard keratin structure we call the nail, and it rides forward over the tightly adherent nail bed. The proximal and lateral nail folds frame the nail, and a thin layer of keratin called the cuticle (eponychium) seals the gap between the fold and the plate, protecting the matrix. At the tip, the hyponychium marks where the plate finally separates from the bed. Knowing these parts is not anatomy for its own sake — it is the diagnostic method, because the sign you see points back to the part that is diseased. [1] [2]
The clinician's task has three layers. The first is recognition and localisation — deciding whether a thickened nail, a transverse groove, a pigmented band or a swollen fold is fungal, inflammatory, traumatic, congenital or neoplastic. The second is cause-matched, conservative-first management — confirming onychomycosis before treating it, draining a paronychia, and reassuring the family of a child with benign trachyonychia. The third is vigilance for the few red flags — a changing or destructive nail lesion — that demand urgent specialist referral. Nail disorders in children are common and usually benign, but they reward a methodical, anatomy-led approach. [1] [3]
Classification
Think of paediatric nail disorders in cause-based groups, because the group sets the management. The normal and developmental variants come first and need no treatment at all: physiological koilonychia (spoon-shaped nails) is normal in infants and toddlers and resolves with age, and nail biting (onychophagia) is so common in school-age children that it is almost a developmental habit rather than a disease. Recognising these benign patterns spares a child unnecessary investigation and treatment. [1] [2]
The acquired disorders are the bulk of practice. Traumatic nails include the subungual haematoma from a crush injury, nail bed lacerations, and the dystrophy of repetitive trauma from footwear or biting. Infectious nails centre on acute paronychia (a staphylococcal nail fold abscess), chronic paronychia (moisture-driven fold inflammation), and onychomycosis (dermatophyte invasion of the nail bed and plate). The inflammatory and skin-disease-associated nails include nail psoriasis, the geometric pitting of alopecia areata, nail lichen planus, and trachyonychia (twenty-nail dystrophy), which may be idiopathic or secondary to one of these. [2] [3]
The congenital and genetic disorders are individually rare but high-yield. Congenital malalignment of the great toenail deviates the nail plate laterally and can cause dystrophy and ingrowth. Nail-patella syndrome gives hypoplastic or absent thumbnails with absent patellae, iliac horns and nephropathy. Pachyonychia congenita produces gross nail thickening with painful palmoplantar keratoderma. Epidermolysis bullosa and the ectodermal dysplasias cause nail dystrophy or loss. These are the nails that announce a syndrome and need a wider lens. [9] [10]
The remaining groups are the nail tumours and the systemic nail signs. In childhood the common nail tumours are benign — pyogenic granuloma, subungual exostosis, and periungual viral warts — but longitudinal melanonychia and the rare nail melanoma belong in a child's differential too. The systemic signs use the nails as a window to the rest of the body: clubbing, koilonychia, Beau lines, leuconychia and nailfold capillary change can point to cyanotic congenital heart disease, iron deficiency, a recent severe illness or an autoimmune connective tissue disease. [1] [2]
Epidemiology & Risk Factors
Onychomycosis is the fungal nail infection that examiners love to contrast with the adult disease, and the contrast is stark: it affects well under three per cent of children, far below the roughly fourteen per cent of adults, though the prevalence rises through childhood and adolescence. The risk factors are a household contact with tinea pedis or onychomycosis (family transmission is important), communal barefoot activity such as swimming pools, Down syndrome, immunocompromise, and occlusive footwear. This low childhood prevalence is exactly why a child's thickened nail is more often psoriasis or trauma than fungus — and why you confirm before you treat. [4] [2]
Nail biting and the ingrown toenail are the everyday paediatric nail problems whose epidemiology is built around habits and growth. Nail biting affects a large fraction of school-age children and resolves in many, though it can cause dystrophy, paronychia and dental damage when severe. The ingrown toenail concentrates in adolescents and is driven by tight footwear, incorrect (curved) nail trimming, hyperhidrosis and the rapid growth of the adolescent great toe. Recognising these lifestyle drivers is half the management, because the cure is often a pair of shoes and a different way of cutting the nail. [3] [1]
Nail psoriasis is commoner than its low profile suggests. The systematic evaluation of 313 children with psoriasis found nail involvement in a substantial proportion, with pitting the most frequent sign — which is why every child with psoriasis deserves a nail examination, and why nail disease in a child warrants a search for skin and joint disease. The congenital and genetic nail disorders are individually rare; nail-patella syndrome and pachyonychia congenita are autosomal dominant, and a careful family history often unearths affected relatives whose mild nail changes had never been explained. [6] [11]
In Australia and Aotearoa New Zealand, paediatric nail care is delivered through general practice, with specialist paediatric dermatology concentrated in major centres and accessible to rural and remote families mainly through outreach or telehealth. This matters for the conditions that need procedures or systemic therapy — recurrent ingrown toenails needing phenol matrixectomy, confirmed onychomycosis needing oral terbatafine, and the destructive or changing nail lesion needing biopsy — because a child in a remote community may wait months for a dermatologist. Building conservative management into primary care, and clear referral pathways for the red flags, is part of delivering equitable nail care, not an afterthought. [1] [2]
Pathophysiology
The nail grows like a slow production line, and the pathology follows the line. The matrix continuously generates the nail plate, pushing it forward over the nail bed at about 3 mm a month for a fingernail (so a fingernail takes roughly 6 months to regrow, and a toenail 12 to 18 months). Because growth is steady, any brief halt in matrix activity leaves a visible record: a Beau line, a transverse groove that appears across several nails at the same level after a high fever or severe illness and then migrates distally over the following months. Read the position of a Beau line and you can date the illness. [1] [2]
The matrix has a useful internal geography. The proximal matrix forms the superficial (dorsal) part of the nail plate, and the distal matrix forms its deeper surface. This is why the depth of a nail abnormality helps to localise the lesion: superficial pitting points to the proximal matrix, and deeper defects point further back. When the whole matrix is irritated — by psoriasis, lichen planus or alopecia areata — it produces a rough, thin, sandpaper plate called trachyonychia, because the matrix is turning out a faulty product across many nails at once. [5] [1]
The nail bed explains the colour-and-attachment signs. Because the bed is tightly bound to the underside of the plate, anything that inflames or lifts it disrupts that adhesion, producing onycholysis (the plate separating from the bed). Psoriasis inflames the bed to produce its oil-drop or salmon-patch discolouration and subungual hyperkeratosis; trauma tears small vessels to produce a subungual haematoma; and dermatophyte fungi invade the bed and the underside of the plate in onychomycosis, thriving in keratin and producing the thickened, crumbly, hyperkeratotic nail. [1] [4]
Onychomycosis deserves its own mechanism paragraph because it drives so much of paediatric nail practice. Dermatophytes — chiefly Trichophyton rubrum and Trichophyton mentagrophytes — invade the nail bed and the underside of the plate from the distal and lateral edges, digesting keratin and provoking subungual hyperkeratosis that lifts the plate. The result is the discoloured, thickened, crumbly nail of distal lateral subungual onychomycosis. Because this appearance overlaps with psoriasis and trauma, the mechanism is invisible to the naked eye, which is the practical reason mycology must precede systemic treatment. [4] [3]
Clinical Presentation
Onychomycosis presents as a thickened, discoloured, crumbly nail, usually a toenail, with subungual hyperkeratosis and onycholysis that begins at the distal or lateral edge and creeps proximally. It is often asymmetric, slow over months to years, and frequently accompanied by tinea pedis in the same child or a household contact. Crucially, the appearance alone cannot distinguish it from psoriasis or trauma, which is why the bedside finding prompts a sample, not a prescription. [4] [1]
Acute paronychia announces itself loudly: a sudden, throbbing, erythematous swelling of a single nail fold, with a visible pointing of pus, usually caused by Staphylococcus aureus entering through a break in the cuticle. Chronic paronychia is its quieter cousin — tender, boggy, reddened folds with nail dystrophy driven by recurrent moisture and inflammation, commoner in children whose hands are often wet, with Candida often present but not the primary driver. The ingrown toenail (onychocryptosis) shows itself at the lateral fold of a great toe: pain, redness and swelling, progressing to granulation tissue and sometimes weeping infection, almost always in an adolescent. [3] [1]
The congenital and pigmented nails bring the high-yield patterns. Congenital malalignment of the great toenail shows a nail plate deviated laterally from birth, risking dystrophy and ingrowth. Pachyonychia congenita presents with gross nail thickening — subungual hyperkeratosis that lifts and distorts the plate — alongside painful palmoplantar keratoderma. Longitudinal melanonychia is a brown-black vertical band of melanin in the nail plate; in a child it is most often a benign nail matrix naevus, present from early life and stable, though a changing or widening band raises the spectre of melanoma. [9] [7]
Differential Diagnosis
For a single thickened or discoloured nail, the differential turns on confirming fungus and finding the mimics. Onychomycosis is mycology-positive with subungual hyperkeratosis and often a household contact, whereas nail psoriasis shows pitting and the oil-drop sign elsewhere and is mycology negative. Trauma (including repetitive shoe trauma and nail biting) fits the history, lichen planus can thin and scar the nail, and a persistent single-nail dystrophy raises the rare possibility of a subungual tumour. The discipline of confirming with mycology resolves the commonest fork. [4] [1]
[4] [6]For a longitudinal pigmented band, the differential is the one that examiners probe most. In a child the commonest cause by far is a benign nail matrix naevus, often with surrounding periungual pigment (a pseudo-Hutchinson sign) and stable from early life. Nail melanoma is rare in children but is the reason a band that is progressively widening, darkening, or in a single nail of a fair-skinned child demands specialist assessment. Dermoscopy helps — a regular brown background with regular longitudinal lines favours a naevus, while an irregular, dark or grey pattern warrants review. A subungual haematoma from trauma gives a dark distal stain that grows out. [7] [8]
For a transverse groove or ridge, think of Beau lines (a transient growth arrest after a systemic illness, present across many nails at the same level, which you can date by its distance from the cuticle), habit-tic deformity (a midline furrow from repeated cuticle pushing, often thumb-sucking or fidgeting), and congenital malalignment. For a swollen nail fold, distinguish acute paronychia (acute, pus, staphylococcal), herpetic whitlow (grouped vesicles and intense pain from herpes simplex, managed with antivirals not antibiotics), chronic paronychia (boggy and moisture-related), and the ingrown toenail (great toe, lateral fold, granulation tissue). [1] [3]
Clinical & Bedside Assessment
Begin with a focused history of the nail problem itself — onset, which nails, tempo, pain, preceding trauma or illness, nail biting, footwear and grooming, and any household skin infection. Then widen the lens: a personal or family history of psoriasis, atopy, alopecia areata or a genodermatosis, immunocompromise, and the impact on the child's school, sport and self-image. The history often names the cause before you look — a household with tinea pedis, a teenager in tight shoes, or a recent high fever that dated a Beau line. [1] [2]
Examine all twenty nails in good light, comparing affected with unaffected nails. Describe which part of the unit is diseased — is it a matrix surface change (pitting, ridges, Beau lines), a bed attachment or colour change (onycholysis, oil-drop, subungual debris), or a fold swelling (paronychia)? Lift the free edge to inspect the hyponychium and subungual debris, examine the nail folds and cuticle, and look at the surrounding skin for tinea pedis, atopic eczema and psoriasis. Palpate for tenderness, warmth and the boggy induration of an abscess. [1] [3]
Apply the systemic screen through the nails. Check for clubbing — loss of the Lovibond angle between nail and fold and a positive Schamroth sign (the diamond window disappears when the index fingers are placed nail-to-nail) — which can signal cyanotic congenital heart disease, inflammatory bowel disease or cystic fibrosis. Look for koilonychia (spoon nails, physiological in infants but a clue to iron deficiency in an older child), Beau lines, leuconychia, and the nailfold capillaries (dilated loops and dropout suggest dermatomyositis or systemic sclerosis). The nails are a window to the child, not just an appendage. [1] [2]
Investigations
Most paediatric nail disorders are diagnosed clinically, and the discipline is to investigate only when it changes management — for the genuinely unclear single nail, the non-responsive nail, and crucially before committing a child to systemic antifungal therapy. Over-investigation of benign variants is itself a failure: physiological koilonychia and stable longitudinal melanonychia of a known naevus need observation, not a battery of tests. [1] [2]
For suspected onychomycosis, confirmation with mycology precedes treatment. Take subungual debris from the most proximal active edge of the diseased nail for potassium hydroxide examination plus fungal culture, or polymerase chain reaction where available, because clinical appearance alone cannot reliably separate fungal infection from psoriasis and trauma. This is the single most important investigation in paediatric nail disease, and the reason is practical: systemic antifungals carry hepatic and drug-interaction risk, so a child should not swallow them on a guess. [4] [3]
For a longitudinal pigmented band, use nail dermoscopy to characterise the pigment. A regular brown background with regular longitudinal lines favours a benign nail matrix naevus; an irregular, widened, dark or grey band warrants specialist review. Document the band with a photograph and a measurement, because change over time is the key discriminator, and serial observation is often the right strategy for a stable band in a child. Nail biopsy is reserved for the genuinely suspicious or changing lesion, and it is a specialist procedure, because the paediatric nail matrix is delicate and biopsy risks permanent dystrophy. [7] [8]
For suspected subungual exostosis or a destructive bony lesion, request a radiograph of the distal phalanx to confirm the bony outgrowth. For scarring or atypical nail dystrophy suspected to be lichen planus, a nail biopsy (by a specialist) can confirm and guide treatment to save the matrix. Otherwise, reserve investigations for the diagnostic dilemma, and let clinical pattern and observation carry the rest. [9] [1]
Management — Resuscitation
Resuscitation in paediatric nail disease is about recognising the few problems that cannot wait while reassuring yourself that the great majority are benign. The red flags are a progressive, widening or darkening longitudinal melanonychia in a single nail of a fair-skinned child (possible nail melanoma), a persistent subungual lesion causing nail destruction or bone involvement (possible subungual exostosis or malignancy), and scarring nail lichen planus with a forward-growing pterygium that threatens permanent matrix loss. Each needs prompt specialist referral rather than a topical cream. [1] [7]
The acute traumatic nail is the one true bedside emergency. A tense, painful subungual haematoma from a recent crush injury needs trephination (a small hole through the nail to release the blood) for immediate pain relief, ideally within hours while the clot is still liquid. A nail bed laceration with significant haemorrhage needs repair with fine absorbable sutures to restore alignment and prevent permanent dystrophy, with the nail plate replaced as a splint and the finger protected. These are time-sensitive interventions that protect the matrix. [12] [1]
Keep resuscitation in proportion. Most children with a nail complaint are well, with a fungal nail, an ingrown toenail or trachyonychia that will be managed conservatively or with a topical agent over months. The danger lives in the changing or destructive lesion, the abscess needing drainage, and the scarring matrix inflammation — each a reason to act now, but each a small minority of the nail problems you will see. [1] [3]
Management — Definitive & Stepwise
Definitive management runs as a cause-matched ladder that begins with benign and conservative measures and reserves systemic drugs and surgery for confirmed, symptomatic or refractory disease. The paediatric nail is forgiving and grows back, so the art is to match the intensity to the problem, protect the matrix, and avoid the harms of unnecessary systemic therapy. [1] [2]
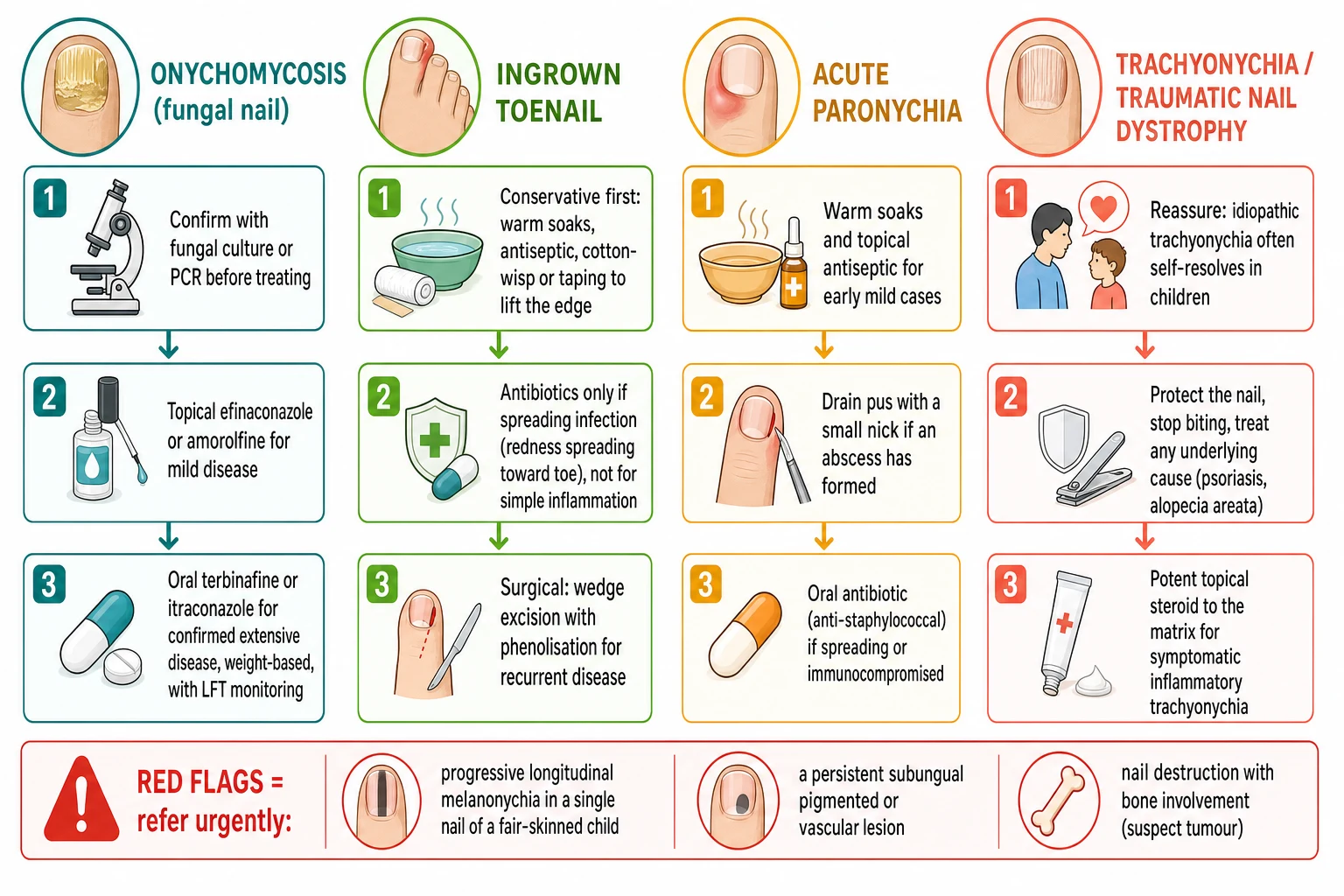
For onychomycosis, confirm first then treat. Topical amorolfine or efinaconazole (or ciclopirox) suits limited distal disease, applied over many months. For confirmed extensive disease, weight-based oral terbinafine is first-line for dermatophyte infection, with itraconazole an alternative. The recognised terbinafine weight bands are under 20 kg at 62.5 mg once daily, 20 to 40 kg at 125 mg once daily, and over 40 kg at 250 mg once daily, given for about 6 weeks for fingernails and 12 weeks for toenails, with liver function monitoring for systemic therapy. Because toenails take 12 to 18 months to regrow, set the family's expectation that a normal-looking nail is many months away. [4] [3]
Paediatric nail disorder therapy ladder (confirm local formularies such as BNF for Children)
For the ingrown toenail, start conservative and stay there for most children: warm antiseptic soaks, proper square (not curved) nail trimming, a cotton-wisp or taping technique to lift the offending edge off the inflamed fold, footwear change, and advice to avoid digging. Reserve an oral antibiotic for genuinely spreading infection (redness tracking toward the toe or systemic upset), not for simple inflammation, because the problem is usually mechanical. Wedge excision of the lateral nail edge with phenol matrixectomy is reserved for recurrent or severe disease that has failed conservative care, and it gives a low recurrence rate. [3] [1]
For acute paronychia, use warm soaks and a topical antiseptic for early mild cases, drain a pointing abscess with a small nick (the single most effective step), and add an oral anti-staphylococcal beta-lactam such as flucloxacillin or cephalexin at weight-based paediatric dosing when infection is spreading or the child is immunocompromised. For chronic paronychia, keep the hands dry and use a topical corticosteroid with or without an antifungal, because the driver is inflammation and moisture rather than a single pathogen. [3] [1]
The stepwise paediatric nail pathway
Localise the lesion to the part of the nail unit (matrix, bed or fold) and take a focused history of onset, trauma, biting, footwear, household infection and skin disease.
Confirm before treating: sample subungual debris for potassium hydroxide and culture or polymerase chain reaction before any systemic antifungal; dermoscopy and serial photography for a pigmented band.
Benign and conservative first: reassure around physiological koilonychia and idiopathic trachyonychia; stop biting; change footwear; trim nails square; warm soaks.
Onychomycosis: topical amorolfine or efinaconazole for limited disease; weight-based oral terbinafine for confirmed extensive disease with liver-function monitoring.
Ingrown toenail: conservative soaks, cotton-wisp or taping, square trimming; antibiotics only for spreading infection; wedge excision with phenolisation for recurrent disease.
Acute paronychia: warm soaks; drain a pointing abscess; oral anti-staphylococcal beta-lactam if spreading or immunocompromised.
Traumatic nail: trephinate a tense subungual haematoma within hours; repair nail bed lacerations with absorbable sutures and replace the plate as a splint.
Red flags — refer urgently: a changing or widening longitudinal melanonychia in a single nail of a fair-skinned child, a destructive subungual lesion with bone involvement, or scarring nail lichen planus.
Specific Subtypes & Scenarios
A child with a single thickened, discoloured toenail. Confirm onychomycosis with mycology before treating. For limited disease use a topical agent, and for confirmed extensive disease use weight-based oral terbinafine for 12 weeks with liver-function monitoring. Check the household for tinea pedis and treat contacts, because family transmission sustains childhood onychomycosis. Set the expectation that a normal toenail is 12 to 18 months away. If mycology is negative, reconsider psoriasis and trauma. [4] [1]
An adolescent with a recurrent ingrown great toenail. Begin with conservative care — warm soaks, square trimming, a cotton-wisp or tape to lift the edge, footwear change — and reserve antibiotics for spreading infection. For recurrent or severe disease, offer wedge excision of the lateral nail edge with phenol matrixectomy, which gives a low recurrence rate, and reinforce square trimming and wide-toe footwear for prevention. Address the lifestyle drivers or the problem returns. [3] [1]
A school-age child with rough, thin, sandpaper-like nails (trachyonychia). Reassure the family that idiopathic trachyonychia often improves or resolves over months to years, protect the nails, and stop biting and picking. Screen the skin, scalp and hair for psoriasis, alopecia areata and lichen planus, because trachyonychia may be the first clue to one of these. Use a potent topical corticosteroid to the proximal nail fold and matrix for symptomatic inflammatory disease, and watch for the scarring pterygium of lichen planus that needs urgent treatment. [5] [1]
A child with a longitudinal brown nail band. Characterise it with dermoscopy, document and photograph it, and recognise that a nail matrix naevus is the commonest cause in children and is usually stable. Refer for biopsy only if the band is progressively widening, darkening or atypical, or arises as a single nail in a fair-skinned child — the red flags for nail melanoma, which is rare but cannot be dismissed. Serial observation is the right strategy for a stable benign-looking band. [7] [8]
A child with nail psoriasis. Look for pitting, onycholysis, the oil-drop sign and subungual hyperkeratosis, and apply a potent topical corticosteroid to the nail bed and matrix, with or without calcipotriol. Examine the skin, scalp and joints, because nail psoriasis accompanies skin disease and predicts juvenile psoriatic arthritis — any joint complaint needs a musculoskeletal examination and early rheumatology referral. Treat the underlying skin disease, because the nails follow the skin. [6] [1]
A young child with gross nail thickening from birth (pachyonychia congenita) or absent thumbnails with a family history (nail-patella syndrome). Recognise the genodermatosis: pachyonychia congenita gives gross nail thickening with painful palmoplantar keratoderma and oral leukoplakia from keratin mutations, and nail-patella syndrome gives hypoplastic or absent thumbnails with absent patellae, iliac horns and nephropathy. Refer to dermatology and clinical genetics, screen for the associated features, and involve the family in a multidisciplinary plan. [11] [9]
Complications & Pitfalls
The first pitfall is treating onychomycosis without confirmation. The thickened, discoloured nail of fungus overlaps with psoriasis and trauma, and systemic antifungals carry hepatic and drug-interaction risk, so a child should never swallow them on appearance alone. Mycology first is the rule, and it protects the child from unnecessary systemic therapy while revealing the mimics. [4] [1]
The second pitfall is overusing antibiotics for the ingrown toenail. Most inflammation is mechanical — the nail edge digging into the fold — and it settles with conservative nail care, soaks and footwear change, not antibiotics. Reserve an oral antibiotic for genuinely spreading infection, because reflexive prescribing drives resistance and treats the wrong problem. The cure is often a different way of cutting the nail and a wider shoe. [3] [1]
The third pitfall is missing scarring nail lichen planus. A child with progressive nail thinning, dystrophy and a forward-growing pterygium (scar) has matrix destruction underway, and delay risks permanent nail loss. This is one of the few paediatric nail emergencies: a prompt potent topical or intralesional corticosteroid to the matrix can save the nail, so the key is to recognise lichen planus before the scar is fixed. [5] [1]
The fourth pitfall is dismissing a changing longitudinal melanonychia. Although nail melanoma is rare in children, a single progressively widening or darkening band, especially in a fair-skinned child, is the red flag that demands specialist assessment and possible biopsy. The safety lies in dermoscopy, documentation and serial observation — measuring the band so that change is detected early. [7] [8]
The fifth pitfall is labelling physiological koilonychia as iron deficiency. Spoon-shaped nails are normal in infants and toddlers, particularly the great toenails, and resolve with age; iron studies are reasonable only in an older child with other features of deficiency. The same calm applies to nail biting and idiopathic trachyonychia — recognising the benign paediatric variant spares the child unnecessary investigation. [1] [2]
The sixth pitfall is ignoring the psychosocial burden. Visible nail dystrophy, bitten nails and recurrent ingrown toenails affect a school-age child's confidence, sport and friendships, and nail biting in particular can signal anxiety. Addressing the psychosocial dimension — and involving psychology when the biting is driven by distress — is part of the management, not a footnote. [1] [3]
Prognosis & Disposition
The disposition for most paediatric nail disorders is outpatient and primary-care led, with reassurance and benign measures sufficient for the majority. Idiopathic trachyonychia often improves or resolves over months to years, physiological koilonychia resolves with age, and stable longitudinal melanonychia of a known naevus needs only serial observation. Set the family's expectations around the slow nail growth rate — a normal-looking toenail after treatment is a year or more away. [5] [1]
Treated onychomycosis clears in a good proportion of children, but recurrence is possible and complete regrowth takes months because of the slow growth rate. Ingrown toenails managed with proper conservative care, and with phenol matrixectomy where needed, have a low recurrence rate, and nail trauma repaired promptly has a good cosmetic outcome. The congenital and genetic nail disorders run a chronic course shaped by the underlying syndrome, and need coordinated dermatology and genetics care. [4] [9]
The disposition hardens around the red flags. A changing or destructive subungual lesion and scarring nail lichen planus need urgent dermatology referral to exclude malignancy and to prevent permanent matrix loss; a recurrent ingrown toenail needing surgery and extensive onychomycosis needing systemic therapy need a dermatology or surgical pathway. At each review, re-examine the nails, re-document any pigmented band, and reinforce the conservative measures and safety-netting. [1] [7]
Special Populations
Infants and toddlers most often show the benign developmental variants — physiological koilonychia is normal at this age — and congenital nail disorders present at birth. Use only gentle topical measures, and involve a specialist for congenital malalignment of the great toenail that is causing dystrophy, because early surgery can prevent permanent deformity. The threshold to refer a neonate with an absent or grossly abnormal nail is low, to catch the genodermatoses. [1] [9]
Adolescents carry the ingrown toenail and nail biting at their peak, driven by footwear, grooming and stress, and they bear the greatest psychosocial burden of visible dystrophy. Address the lifestyle drivers, involve the adolescent in the management plan, and screen mood and anxiety when nail biting is severe, because the habit can be a window onto distress. Contraception and pregnancy avoidance are not usually an issue in nail therapy, but terbinafine and itraconazole still need careful prescribing in this age group. [3] [1]
Immunocompromised children — those on chemotherapy, post-transplant, or with primary immunodeficiency — have commoner and more severe fungal nail disease and atypical paronychia, and systemic therapy may interact with their complex medication regimens. Coordinate with the treating oncology, transplant or immunology team before starting systemic antifungals, and lower the threshold for mycological confirmation and specialist input. [4] [1]
Children with Down syndrome have a higher prevalence of onychomycosis and other nail changes, so lower the threshold for mycological confirmation when a nail looks fungal. Children with epidermolysis bullosa and the ectodermal dysplasias have nail dystrophy or loss as part of their syndrome, and need gentle, multidisciplinary care with a dermatologist to protect what nail unit remains. [9] [2]
Children in rural, remote and disadvantaged communities face real inequity of access to specialist dermatology and to the procedures that some nail disorders need. Deliver as much as possible through primary care — confirmation, conservative management and clear referral pathways — and use outreach and telehealth so that distance is not the reason a child with a destructive nail lesion waits months for a diagnosis. [1] [2]
Evidence, Guidelines & Regional Differences
The evidence base for paediatric nail disorders rests on a set of comprehensive reviews that frame the anatomy-led approach and the spectrum of disease. The Bellet review of paediatric nail disorders and the Smith and Rubin review lay out the classification, the common acquired and congenital disorders, and the diagnostic method, while the Axler, Bellet and Lipner review of inflammatory and infectious nail disease in children focuses the practical management of paronychia, onychomycosis and the inflammatory nails. These are the framing references for the topic. [1] [2] [3]
Nail psoriasis in 313 children with psoriasis
Population: A systematic evaluation of 313 children with psoriasis, examining the prevalence and patterns of nail involvement.
Key finding
Nail psoriasis was common in this large paediatric cohort, with pitting the most frequent sign, quantifying a burden that is easily overlooked in children and reinforcing the need to examine the nails of every child with psoriasis.
Practice change
The study establishes nail psoriasis as a frequent and clinically meaningful paediatric finding, justifying routine nail examination and joint screening in children with psoriasis.
The onychomycosis evidence is anchored by the Solis-Arias and Garcia-Romero review, which establishes the low childhood prevalence, the household-transmission risk factors, and the confirm-before-treat principle with topical and systemic therapy options. The trachyonychia evidence comes from the Jacobsen and Tosti comprehensive review, which sets out the clinical variants, the association with lichen planus, psoriasis and alopecia areata, and the generally favourable prognosis that underpins a conservative, reassuring approach in children. [4] [5]
The pigmented nail band is grounded in the nail expert group's clinical review of longitudinal melanonychia (Ricardo et al) and the paediatric dermoscopy study (Ansari et al), which together establish the diagnostic framework and the benign predominance of the nail matrix naevus in children while naming the red flags for melanoma. The congenital and genetic domain draws on the congenital and hereditary nail disease review (Bernal Masferrer et al), the genetics of isolated hereditary nail disorders (Khan et al), and the pachyonychia congenita keratin mutation study (Forrest et al). The traumatic domain is served by the fingernail injury in children review (Braga Silva). [7] [8] [9] [10] [11] [12]
The regional policy structure is consistent in principle and varies in access. Weight-based paediatric terbinafine dosing for onychomycosis is standard across the BNF for Children, North American and Australasian dermatology guidance, though the threshold for routine liver-function monitoring for short courses varies. The conservative-first management of the ingrown toenail and idiopathic trachyonychia is universal, and the threshold for biopsy of paediatric longitudinal melanonychia remains a specialist judgement that balances the rarity of childhood nail melanoma against the risk of permanent matrix damage from biopsy. [1] [4]
The controversies are real: the role of routine liver-function monitoring for short-course terbinafine in an otherwise well child; the relative place of topical versus systemic antifungals for paediatric onychomycosis; the threshold and timing for biopsy of a paediatric pigmented band; and the timing of surgery for congenital malalignment of the great toenail. The defence against each is the same — a methodical, anatomy-led assessment, confirmation before systemic therapy, conservative measures first, and a low threshold for specialist referral when a red flag appears. [1] [2]
Exam Pearls
- The single most useful principle: localise the lesion to the part of the nail unit — matrix lesions change shape and surface (pitting, Beau lines, trachyonychia), bed lesions change colour and attachment (onycholysis, oil-drop, subungual haematoma), fold lesions cause swelling and pus (paronychia). [1]
- Fingernails grow about 3 mm per month and take 6 months to regrow; toenails take 12 to 18 months — which is why a Beau line from a systemic illness migrates distally over months and why treated nails take so long to look normal. [1]
- Confirm onychomycosis with mycology (potassium hydroxide plus culture or polymerase chain reaction) before systemic therapy; never treat a child's thickened nail with oral antifungals on appearance alone. [4]
- Terbinafine weight bands: under 20 kg 62.5 mg once daily, 20 to 40 kg 125 mg once daily, over 40 kg 250 mg once daily, for about 6 weeks (fingernails) or 12 weeks (toenails). [4]
- In a child, a longitudinal brown nail band is most often a benign nail matrix naevus; nail melanoma is rare — but a single progressively widening, darkening band in a fair-skinned child is the red flag for specialist assessment. [7]
- Acute paronychia is staphylococcal: drain the pus, and add an anti-staphylococcal beta-lactam if spreading; herpetic whitlow gives grouped vesicles and needs antivirals, not antibiotics. [3]
- Idiopathic trachyonychia (twenty-nail dystrophy) in a child often self-resolves — reassure, protect the nail, and reserve a potent topical steroid for symptomatic inflammation; watch for scarring nail lichen planus. [5]
- Physiological koilonychia (spoon nails) is normal in infants and toddlers; in an older child, consider iron deficiency. [1]
- The ingrown toenail is managed conservatively first (soaks, square trimming, cotton-wisp or taping); antibiotics are for spreading infection; wedge excision with phenolisation is for recurrent disease. [3]
- Recognise the genodermatoses: pachyonychia congenita (gross nail thickening, KRT6A or KRT16 mutations, painful palmoplantar keratoderma), nail-patella syndrome (hypoplastic thumbnails, absent patellae, iliac horns, nephropathy, LMX1B), and scarring nail lichen planus that threatens permanent matrix loss. [11] [9]
References
- [1]Bellet JS Pediatric Nail Disorders. Dermatol Clin, 2021.PMID 33745636
- [2]Smith RJ; Rubin AI Pediatric nail disorders: a review. Curr Opin Pediatr, 2020.PMID 32692049
- [3]Axler EN; Bellet JS; Lipner SR Tackling Inflammatory and Infectious Nail Disorders in Children. Cutis, 2024.PMID 39159345
- [4]Solis-Arias MP; Garcia-Romero MT Onychomycosis in children. A review. Int J Dermatol, 2017.PMID 27612431
- [5]Jacobsen AA; Tosti A Trachyonychia and Twenty-Nail Dystrophy: A Comprehensive Review and Discussion of Diagnostic Accuracy. Skin Appendage Disord, 2016.PMID 27843915
- [6]Pourchot D; Bodemer C; Phan A; Bursztejn AC; et al Nail Psoriasis: A Systematic Evaluation in 313 Children with Psoriasis. Pediatr Dermatol, 2017.PMID 27873356
- [7]Ricardo JW; Bellet JS; Jellinek N; Lee D; et al Evaluation and diagnosis of longitudinal melanonychia: A clinical review by a nail expert group. J Am Acad Dermatol, 2025.PMID 40023404
- [8]Ansari MS; Mahmoudi H; Sadeghinia A; Azizzadeh-Roodpishi S; et al Dermoscopic Evaluation of Longitudinal Melanonychia in Children: A Prospective Study. Indian J Dermatol, 2021.PMID 34759421
- [9]Bernal Masferrer L; Matei MC; Gilaberte Calzada Y; Navarro Campoamor L [Translated article] Congenital and Hereditary Nail Disease. Actas Dermosifiliogr, 2024.PMID 38972583
- [10]Khan S; Basit S; Habib R; Kamal A; et al Genetics of human isolated hereditary nail disorders. Br J Dermatol, 2015.PMID 26149975
- [11]Forrest CE; Casey G; Mordaunt DA; Thompson EM; et al Pachyonychia Congenita: A Spectrum of KRT6a Mutations in Australian Patients. Pediatr Dermatol, 2016.PMID 27041546
- [12]Braga Silva J Fingernail injury in children. Hand Surg Rehabil, 2024.PMID 36682538