Paeds · paediatric-dermatology
Nappy dermatitis
Also known as diaper dermatitis · diaper rash · nappy rash · ammoniacal dermatitis · irritant napkin dermatitis · candidal napkin dermatitis · Jacquet erosive dermatitis · satellite pustules · zinc oxide barrier · clotrimazole 1 percent · miconazole 2 percent
A fellowship approach to nappy dermatitis in infants, built around the single decision that matters: separating the common irritant contact dermatitis on convex surfaces with spared folds from the candidal dermatitis that involves the folds and carries satellite lesions, so that the barrier cream and the air exposure are used first and the topical antifungal is added when Candida is present. The page covers the pathophysiology of the moisture-and-faecal-enzyme disruption of the stratum corneum, the Candida albicans overgrowth in the warm occluded fold, the bedside pattern recognition of the two main subtypes, the differential of seborrhoeic dermatitis, atopic dermatitis, allergic contact dermatitis, psoriasis, zinc deficiency, and Langerhans cell histiocytosis, the stepwise management from frequent nappy changes and zinc oxide barrier to clotrimazole or miconazole for the candidal rash and short-course hydrocortisone for the inflamed rash, and the red flag of the rash that does not respond in seven days and demands a broader differential.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A nine-month-old boy is brought to the general practitioner by his mother, who has noticed a red, sore rash in the nappy area for five days. The rash began on the buttocks and the lower abdomen and has spread to the groin folds in the last two days, with small red bumps appearing at the edge. He had a course of oral amoxicillin for an ear infection ten days ago. On examination, the buttocks, the genitalia, and the lower abdomen show a confluent bright erythema, and the inguinal folds are now involved with the same beefy redness. Scattered around the edge, on the upper thighs and the lower abdomen, are five small red papules and two tiny pustules. The skin outside the nappy area is clear. This is a candidal nappy dermatitis, almost certainly secondary to the recent antibiotic course, superimposed on an irritant base. The management is the general skin care, the zinc oxide barrier, the clotrimazole 1 percent cream twice daily for fourteen days, and the counsel that the satellite lesions are the hallmark of Candida and the reason the antifungal is indicated. [2] [5]
Folds and satellites — the two questions that separate irritant from candidal
Overview & Definition
Nappy dermatitis, also called diaper dermatitis or nappy rash, is the common inflammatory skin reaction of the skin covered by the nappy in the infant and the young child. It is one of the commonest skin complaints of infancy, affecting up to half of all infants at some point in the first year of life, and it is the archetype of a condition whose recognition is clinical and whose management is preventive. The term is an umbrella that covers several subtypes, but the two that dominate the clinical encounter are the irritant contact dermatitis and the candidal dermatitis, and separating them is the decision that drives the treatment. [1] [9]
The clinical importance of nappy dermatitis lies in its frequency, its distress to the child and the family, and the fact that its management is almost entirely in the hands of the parent and the primary-care clinician. The condition is benign in the great majority, but it is a portal to the broader differential of the persistent rash — the seborrhoeic dermatitis, the atopic dermatitis, the allergic contact dermatitis, the psoriasis, the zinc deficiency of acrodermatitis enteropathica, and the rare but serious Langerhans cell histiocytosis — and the clinician who knows when to look beyond the nappy area avoids the missed diagnosis and the mistreated rash. [4] [12]
The page that follows treats nappy dermatitis as the paediatric generalist encounters it: recognised on the distribution and the morphology, managed with the skin care and the barrier and the antifungal in the right order, and revisited at seven days with the broader differential if it has not resolved. The single skill the fellowship rewards is the bedside separation of the irritant from the candidal subtype, because that separation decides whether the topical antifungal is added or withheld. [2] [3]
Classification
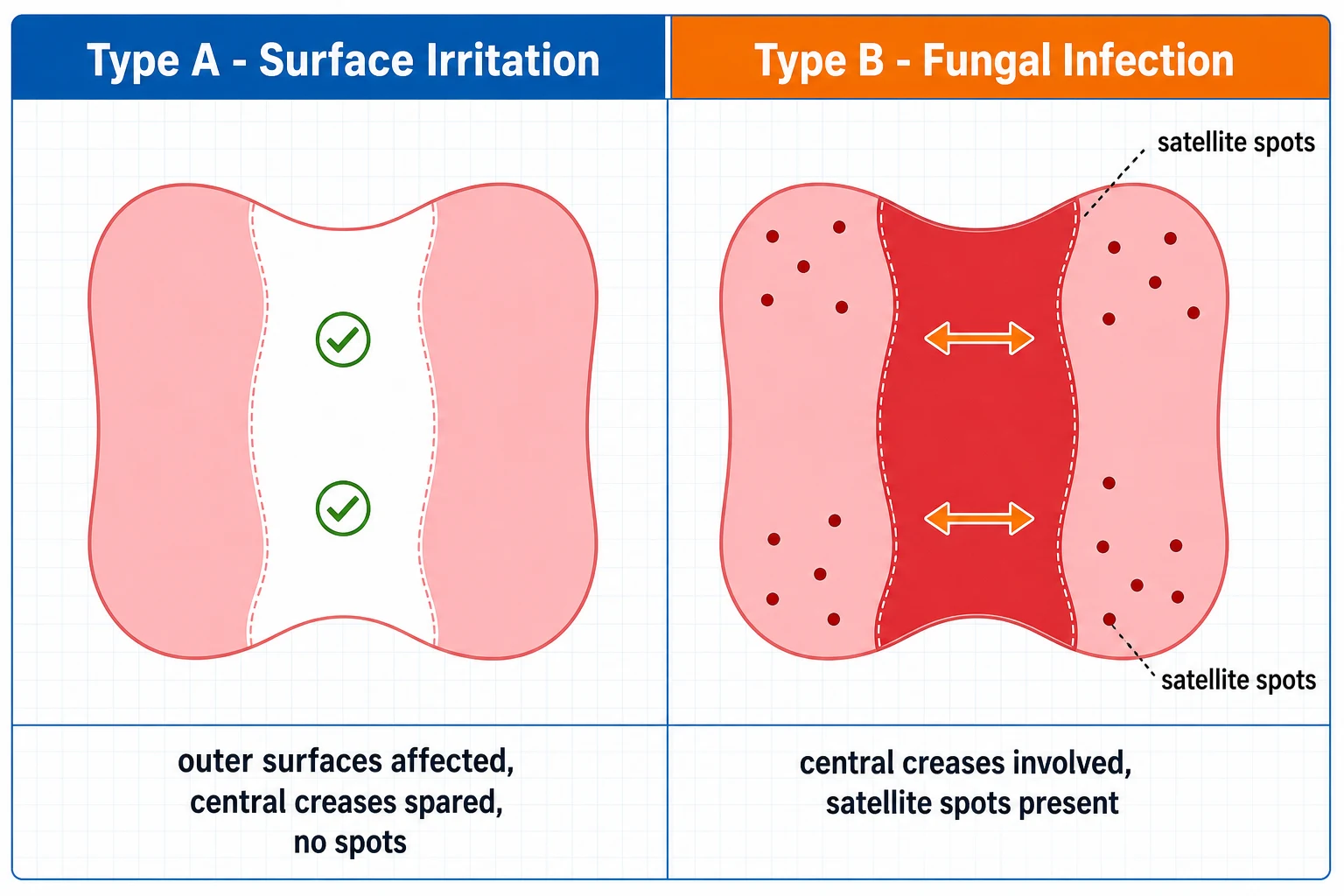
The classification of nappy dermatitis follows the distribution and the cause, and the two main subtypes are separated at the bedside by the fold involvement and the satellite lesions. The irritant contact dermatitis is the commonest subtype, and it presents with the erythema on the convex surfaces — the buttocks, the genitalia, the lower abdomen, and the upper thighs — with the inguinal and the gluteal folds characteristically spared, because the folds are the skin least exposed to the urine and the faeces. The candidal dermatitis, the second commonest subtype, presents with the bright beefy-red erythema that extends into the folds and the satellite papules and pustules scattered beyond the main margin, and it is the subtype that warrants the topical antifungal. [1] [2]
The less common subtypes are named for their morphology or their cause. The Jacquet erosive dermatitis is the severe irritant subtype with the punched-out erosions and the ulcerations at the perianal and the genital skin, and it signals a severe barrier failure or a neglect. The allergic contact dermatitis is the delayed-type hypersensitivity to a component of the nappy or the wipe — the fragrance, the dye, or the preservative — and it presents with the well-demarcated erythema at the sites of contact, sometimes with the pattern of the nappy edge. The seborrhoeic dermatitis of infancy presents with the salmon-coloured, greasy, scaly patches that involve the folds and extend beyond the nappy area to the scalp, the face, and the postauricular skin. [4] [10]
The classification also includes the secondary bacterial infection — the impetiginised nappy dermatitis with the honey-coloured crusts and the weeping erosions from Staphylococcus aureus or Group A streptococcus — and the rare mimics that present as a persistent nappy rash: the psoriasis with the well-defined scaly plaques, the zinc deficiency of acrodermatitis enteropathica with the periorificial and the acral dermatitis, and the Langerhans cell histiocytosis with the purpuric, crusted papules in the folds. The skill at the bedside is to classify the rash first as irritant or candidal, then to reconsider the diagnosis if the rash does not respond to the standard measures within seven days. [4] [12]
Irritant versus candidal nappy dermatitis — the four distinguishing features
Irritant (commonest)
Candidal
Seborrhoeic dermatitis
Allergic contact
Epidemiology & Risk Factors
Nappy dermatitis is one of the commonest skin conditions of infancy. The prevalence peaks between the ages of six and twelve months, coinciding with the introduction of solid foods and the change in the stool composition, and most infants will have at least one episode. The point prevalence, measured in cross-sectional surveys, ranges from about seven to thirty-five percent depending on the population and the definition, and the lifetime prevalence up to the age of two years approaches fifty percent. [1] [3]
The risk factors cluster around the four elements that disrupt the skin barrier: the prolonged contact with urine and faeces, the occlusion and the moisture under the nappy, the friction from the nappy and the wipes, and the change in the skin pH. The infrequent nappy change is the single most modifiable risk factor, because the longer the skin is in contact with the wet and the soiled nappy, the greater the barrier disruption. The introduction of solid foods, the diarrhoeal illness, and the antibiotic therapy all change the stool and increase the faecal enzyme load on the skin. The premature or the low-birth-weight infant has a thinner, more permeable stratum corneum and is more susceptible. [3] [8]
The candidal subtype has its own risk factors, and these are the ones the fellowship candidate names at the bedside. The recent antibiotic therapy, which disrupts the normal flora and allows the Candida overgrowth, is the commonest precipitant. The oral thrush, the concurrent candidal infection elsewhere, the prolonged course of an untreated irritant dermatitis that creates the disrupted barrier, and the immunocompromise all increase the risk. Candida albicans is recovered from the nappy rash in up to forty to seventy-five percent of the cases that last more than three days, which is the practical figure that supports the addition of the antifungal when the rash persists beyond the first few days. [5] [7]
Pathophysiology
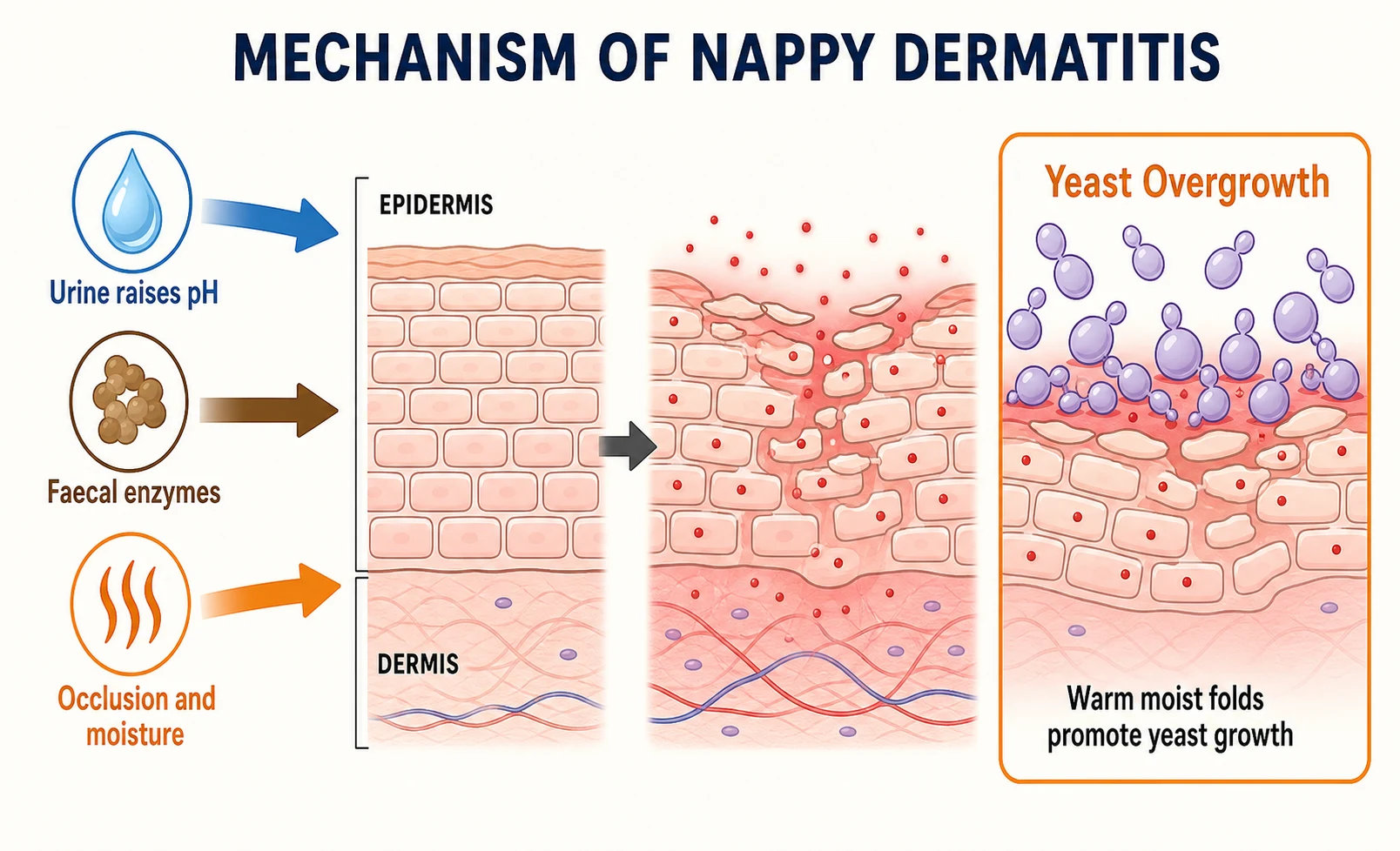
The pathophysiology of the irritant nappy dermatitis is the disruption of the stratum corneum by the combined assault of the moisture, the faecal enzymes, and the elevated pH under the occluded nappy. The healthy stratum corneum is a barrier of corneocytes embedded in the lipid matrix, and it protects the underlying living epidermis from the irritants and the microbes. Under the nappy, the occlusion and the moisture hydrate the stratum corneum and increase its permeability, so the irritants penetrate more readily. The urine raises the skin pH by the action of the urease-producing organisms that convert the urea to ammonia, and the elevated pH activates the faecal proteases and lipases that digest the corneocyte proteins and the lipids, further disrupting the barrier. The result is the inflammation, the erythema, and the characteristic shiny, glazed appearance of the irritated skin. [8] [11]
The candidal nappy dermatitis is the opportunistic overgrowth of Candida albicans on the disrupted skin. The warm, moist, occluded environment under the nappy, particularly in the skin folds, is the ideal growth condition for the yeast, and the disrupted stratum corneum of the irritant dermatitis provides the portal of entry. The Candida multiplies on the surface, invades the parakeratotic stratum corneum, and triggers the intense inflammatory response that produces the bright beefy-red erythema, the scaly border, and the satellite lesions. The satellite papules and pustules are the colonies of Candida that have spread beyond the main margin, and they are the clinical hallmark of the candidal subtype. [5] [7]
The maturation of the skin, the introduction of the super-absorbent disposable nappies, and the frequent nappy change all contribute to the resolution. The older child's thicker stratum corneum and the drier environment of the toilet-trained child make the condition rare after the age of two. The modern super-absorbent nappy, which wicks the moisture away from the skin and keeps the pH lower, has reduced the incidence and the severity of the irritant dermatitis compared with the cloth nappy, and this is the evidence that supports the recommendation for the disposable super-absorbent nappy as the preventive measure. [3] [6]
Clinical Presentation
The child with the irritant nappy dermatitis presents with the red, sore rash confined to the nappy area. The rash is on the convex surfaces — the buttocks, the genitalia, the lower abdomen, and the upper thighs — and it spares the inguinal and the gluteal folds. The affected skin is erythematous, shiny, and glazed, with a relatively sharp margin that often corresponds to the edge of the nappy. There may be maceration, scaling, and small fissures, and in the more severe cases there are erosions. The child is usually well and afebrile, but may be irritable, especially during the nappy change and the cleansing, because the inflamed skin is tender. The onset is gradual over days, and the rash follows the periods of prolonged wetness — the night, the long car journey, or the episode of diarrhoea. [1] [9]
The candidal nappy dermatitis presents with the brighter, more intense erythema that extends into the folds. The inguinal, the gluteal, and the perianal folds are now involved, and the erythema is beefy red with a sharply demarcated, scaly border. The pathognomonic feature is the satellite lesions — the small red papules and the tiny pustules scattered beyond the main margin of the rash, on the upper thighs, the lower abdomen, and the suprapubic skin. The onset may be more acute than the irritant subtype, and there is often a history of a recent antibiotic course, an oral thrush, or a pre-existing irritant dermatitis that has been present for several days. The child may be more distressed by the candidal rash because the inflammation is more intense. [5] [7]
The severe irritant subtype, the Jacquet erosive dermatitis, presents with the punched-out erosions and the shallow ulcerations at the perianal and the genital skin, sometimes with the nodular or the granulomatous surface. It is the severe end of the irritant spectrum, and it signals a profound barrier failure, a neglect, or an underlying problem such as the excessive faecal enzyme production. The allergic contact dermatitis presents with the well-demarcated erythema and the vesiculation at the sites of the allergen contact, and it may follow a change of the nappy brand, the wipe, or the barrier cream. [4] [10]
Differential Diagnosis
The differential of the nappy-area rash is the first place the clinician looks when the rash does not fit the simple irritant or candidal pattern. The seborrhoeic dermatitis of infancy presents with the salmon-coloured, greasy, scaly patches in the folds — the inguinal, the axillary, and the postauricular — and on the scalp as the cradle cap. Unlike the candidal dermatitis, it extends well beyond the nappy area and is less intensely red. The atopic dermatitis involves the nappy area less often than the extensor surfaces in infancy, but the pruritic, flexural distribution and the family history distinguish it. The key: the nappy area is often SPARED in atopic dermatitis because the moisture under the nappy prevents the xerosis that drives the eczema elsewhere. [4] [12]
The allergic contact dermatitis is the delayed hypersensitivity to a component of the nappy, the wipe, or the topical preparation. The dye in the coloured nappy, the fragrance or the preservative (methylisothiazolinone) in the wipe, and the component of the cream are the common allergens. The rash is well-demarcated and tracks the pattern of the allergen contact, and it does not respond to the standard barrier measures until the allergen is removed. The patch testing is indicated for the persistent case. [10]
The rare mimics are the ones the fellowship candidate names to demonstrate the breadth of the differential. The psoriasis presents with the well-defined, silvery, scaly plaques, sometimes in the nappy area as the napkin psoriasis, and it may be the first presentation of the chronic plaque psoriasis. The zinc deficiency, the acrodermatitis enteropathica, presents with the periorificial and the acral dermatitis — around the mouth, the anus, and the hands and the feet — and it is associated with the chronic diarrhoea and the alopecia. The Langerhans cell histiocytosis presents with the purpuric, crusted papules in the folds, the seborrhoeic distribution, and the scalp, and it is the serious diagnosis not to miss. The child-protection awareness is the scald or the burn with the sharp demarcation that does not fit the nappy dermatitis pattern. [4] [12]
Clinical & Bedside Assessment
The assessment of the nappy dermatitis begins with the history, and the two questions that matter are the nappy-change frequency and the stool pattern. The parent is asked how often the nappy is changed, whether the child sleeps through the night in a wet nappy, and whether the child has had a diarrhoeal illness or a recent antibiotic course. The introduction of solid foods, the change of the nappy brand or the wipe, and the application of any new cream or lotion are the other elements of the history that may reveal the precipitant. The history of the oral thrush, the concurrent skin condition, and the family history of atopy are the background that frames the differential. [2] [8]
The examination is the distribution and the morphology. The nappy is removed and the child is examined in the prone and the supine position, and the clinician looks for the two features that separate the irritant from the candidal subtype: the fold involvement and the satellite lesions. The irritant dermatitis shows the erythema on the convex surfaces with the folds spared; the candidal dermatitis shows the erythema extending into the folds and the satellite papules beyond the margin. The severity is assessed by the extent of the erythema, the presence of the erosions or the ulcerations, and the degree of the discomfort. [1] [2]
The examination also looks beyond the nappy area. The scalp is examined for the cradle cap of seborrhoeic dermatitis, the face and the flexures for the atopic dermatitis, and the skin outside the nappy for the generalised rash that may signal a systemic condition. The growth, the development, and the general appearance of the child are assessed, because the chronic diarrhoea and the failure to thrive with the periorificial rash point to the zinc deficiency. The lymphadenopathy, the hepatosplenomegaly, and the generalised purpuric papules point to the Langerhans cell histiocytosis. The skill at the bedside is the full skin examination, not just the nappy area. [4] [12]
Investigations
The diagnosis of the nappy dermatitis is clinical, and no investigations are required in the typical case. The distribution and the morphology, the history of the nappy-change frequency and the stool pattern, and the presence or the absence of the fold involvement and the satellite lesions are sufficient to make the diagnosis and to choose the treatment. The swab, the skin scraping, and the culture are reserved for the atypical or the persistent case. [2] [8]
The skin scraping for the potassium hydroxide preparation and the fungal culture is the investigation that confirms the candidal dermatitis when the diagnosis is uncertain. The scraping of the scaly border or the satellite pustule reveals the budding yeast cells and the pseudohyphae under the microscope, and the culture grows the Candida albicans. In practice, the clinical picture is sufficiently characteristic that the scraping is unnecessary in the typical candidal rash, and the empirical trial of the topical antifungal serves as both the diagnostic and the therapeutic test. [5] [7]
The bacterial swab is indicated when the rash is weeping, crusted, or spreading, and the secondary bacterial infection is suspected. The Staphylococcus aureus and the Group A streptococcus are the common organisms, and the honey-coloured crusts, the bullae, and the painful erosions are the clinical clues. The biopsy is reserved for the rare persistent case that does not respond to the standard measures and where the serious diagnosis — the Langerhans cell histiocytosis, the zinc deficiency, or the psoriasis — is suspected, and it is the dermatology referral that guides the biopsy. The blood tests for the zinc level are indicated when the acrodermatitis enteropathica is suspected on the periorificial rash and the chronic diarrhoea. [4] [12]
Management — Resuscitation
The management of the nappy dermatitis does not, in the typical case, demand a resuscitation. The child is well, and the condition is a skin inflammation, not a systemic illness. The resuscitative principle is the prompt recognition of the secondary bacterial infection and the severe erosive subtype, because these are the scenarios that demand the urgent treatment. The febrile, unwell child with the weeping, spreading rash has the secondary bacterial infection, and the swab and the oral antibiotic — the flucloxacacin at twenty-five to fifty milligrams per kilogram per day in divided doses for the staphylococcal infection, or the phenoxymethylpenicillin for the streptococcal — are started. [1] [8]
The severe erosive subtype, the Jacquet erosive dermatitis, is the resuscitative scenario of the irritant spectrum. The punched-out erosions and the ulcerations demand the aggressive barrier, the air exposure, and the review, and the underlying cause — the neglect, the excessive faecal enzyme load, or the underlying condition — is sought. The pain is managed with the oral paracetamol at fifteen milligrams per kilogram per dose, and the soft, non-adherent dressing is applied to the erosions. [4]
The analgesia is the humane element of the management. The inflamed nappy dermatitis is tender, and the nappy change is painful. The gentle cleansing with the warm water and the soft cloth, the patting dry rather than the rubbing, and the application of the barrier before the skin is fully exposed all reduce the discomfort. The oral paracetamol is given before the particularly painful nappy change in the severe case. [2] [8]
Management — Definitive & Stepwise
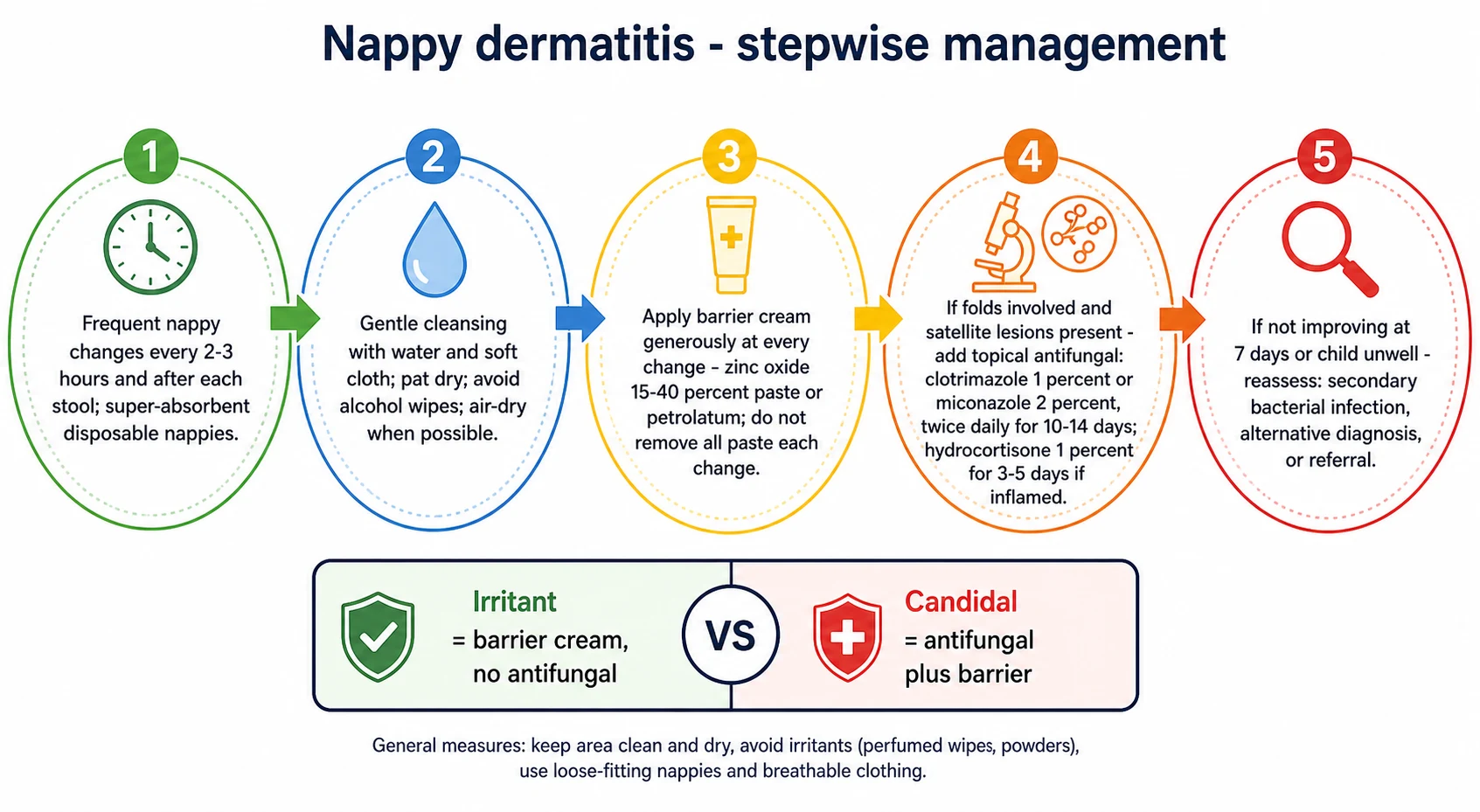
The definitive management of the nappy dermatitis is built from three elements, applied in the sequence that matches the subtype: the general skin care, the barrier preparation, and the antifungal when Candida is present. The general skin care is the foundation, and it is the element that prevents the recurrence. The nappy is changed frequently — every two to three hours during the day and after every stool, and at least once during the night for the young infant. The super-absorbent disposable nappy is preferred because it wicks the moisture away from the skin and keeps the pH lower than the cloth nappy. The skin is cleansed gently with the warm water and the soft cloth or the cotton wool, and the alcohol-based and the fragranced wipes are avoided because they irritate the inflamed skin. The skin is patted dry or left to air-dry, and the air exposure — the nappy-free time — is encouraged whenever practical. [3] [6]
The barrier preparation is the second element, and it is applied to every nappy change in both the irritant and the candidal subtypes. The zinc oxide paste at fifteen to forty percent, the petrolatum, and the dimethicone-based creams are the common barriers, and they work by forming the physical layer between the skin and the irritant. The barrier is applied generously — thick enough to be visible — and it is not scrubbed off at every change. The old layer is gently wiped and the new layer applied on top, so the skin is not traumatised by the repeated cleansing. The barrier is the mainstay of both the prevention and the treatment of the irritant subtype. [3] [8]
The management of the nappy dermatitis — the steps
General skin care: change the nappy every two to three hours and after every stool; use the super-absorbent disposable nappy; cleanse with warm water and a soft cloth, not the alcohol wipe; pat dry and air-dry when possible.
Apply the barrier preparation generously at every nappy change: the zinc oxide paste at fifteen to forty percent, the petrolatum, or the dimethicone cream. Do not scrub the old layer off — wipe gently and apply the new layer on top.
If the folds are involved and the satellite papules are present, add the topical antifungal: the clotrimazole 1 percent cream or the miconazole 2 percent cream, twice daily for ten to fourteen days, applied to the affected skin before the barrier layer.
If the rash is intensely inflamed, add the hydrocortisone 1 percent cream once or twice daily for three to five days, applied sparingly to the inflamed skin. Do not exceed seven days, and avoid the potent steroids in the nappy area because the occlusion increases the absorption and the risk of the skin atrophy.
If the rash is weeping, crusted, or spreading, and the secondary bacterial infection is suspected, take the swab and start the oral antibiotic: the flucloxacillin for the staphylococcal or the phenoxymethylpenicillin for the streptococcal infection.
If the rash has not improved at seven days of the standard measures, reconsider the diagnosis: the seborrhoeic dermatitis, the atopic dermatitis, the allergic contact dermatitis, the psoriasis, the zinc deficiency, and the Langerhans cell histiocytosis. Refer to the dermatology if the diagnosis is uncertain.
The topical antifungal is the third element, and it is added when the candidal subtype is confirmed by the fold involvement and the satellite lesions. The clotrimazole 1 percent cream, the miconazole 2 percent cream, and the nystatin ointment are the common choices, applied twice daily for ten to fourteen days to the affected skin. The antifungal is applied first, and the barrier is applied on top, so the antifungal reaches the skin and the barrier protects it. The short course of the hydrocortisone 1 percent cream, once or twice daily for three to five days, is added when the inflammation is intense, and it is applied sparingly to the inflamed skin. The potent and the fluorinated steroids are avoided in the nappy area because the occlusion increases the absorption and the risk of the skin atrophy, and the combination steroid-antifungal-antibiotic creams are avoided as the routine first-line because they increase the sensitisation and the steroid exposure. [5] [7]
Specific Subtypes & Scenarios
The irritant nappy dermatitis of the six-to-twelve-month-old is the commonest scenario, and it responds to the general skin care and the barrier in the great majority. The zinc oxide paste applied at every change, the frequent nappy changes, and the gentle cleansing clear the rash within three to seven days in the typical case. The family is counselled on the nappy-change frequency, the avoidance of the alcohol wipes, and the air exposure, and the recurrence is prevented by the maintenance of the same measures. The follow-up is unnecessary if the rash resolves as expected. [3] [6]
The candidal nappy dermatitis after the antibiotic course is the scenario that tests the recognition of the folds and the satellite lesions. The recent antibiotic therapy disrupts the normal flora and allows the Candida overgrowth, and the rash presents acutely with the fold involvement and the satellite papules. The management is the addition of the clotrimazole 1 percent or the miconazole 2 percent cream, twice daily for fourteen days, alongside the barrier and the general skin care. The response is usually rapid, with the improvement visible within three to five days, and the family is reassured that the Candida is the consequence of the antibiotic and not a sign of a serious underlying condition. [5] [7]
In Australia and Aotearoa New Zealand, the nappy dermatitis is managed in the general practice and the primary care setting, with the over-the-counter availability of the zinc oxide and the petrolatum barriers and the topical antifungals. The Aboriginal and the Torres Strait Islander and the Maori children in the remote communities may have the limited access to the disposable nappies and the clean water, and the telehealth and the outreach support the management. The dermatology referral is available through the public and the private systems for the persistent or the atypical rash, and the wait times in the regional centres are managed by the telehealth dermatology. [3] [6]
The persistent nappy dermatitis is the scenario that demands the broader differential, and it is the single most important red flag. The rash that does not respond to the good barrier measures and the topical antifungal within seven days is not a treatment failure — it is a diagnostic reconsideration. The seborrhoeic dermatitis, the atopic dermatitis, the allergic contact dermatitis, the psoriasis, the zinc deficiency, and the Langerhans cell histiocytosis are the conditions that hide among the persistent rashes, and the dermatology referral and the targeted investigations — the skin scraping, the bacterial swab, the biopsy, the zinc level — are the next steps. The clinician who holds this red flag in mind avoids the months of the mistreated, persistent rash. [4] [12]
The erosive subtype, the Jacquet erosive dermatitis, is the severe scenario that demands the aggressive management and the review. The punched-out erosions and the ulcerations at the perianal and the genital skin signal the profound barrier failure, and the management is the thick barrier paste, the air exposure, and the review at forty-eight hours. The underlying cause — the neglect, the frequent liquid stools, or the underlying condition — is sought, and the child-protection awareness is maintained when the erosions do not fit the offered history. [4] [8]
Complications & Pitfalls
The complications of the nappy dermatitis are few in the great majority, but the secondary bacterial infection is the one that demands the vigilance. The disrupted skin barrier is the portal of entry for the Staphylococcus aureus and the Group A streptococcus, and the impetiginised rash — with the honey-coloured crusts, the weeping erosions, and the spreading erythema — is the clinical picture. The bacterial swab and the oral antibiotic are the management, and the child who is febrile or unwell is assessed for the more severe soft-tissue infection. [1] [8]
The pitfall of the over-treatment is the one the fellowship candidate names to demonstrate the restraint. The potent topical steroid, applied in the occluded nappy area, causes the skin atrophy and the striae within weeks, and the combination steroid-antifungal-antibiotic creams — the Trimovate-type preparations — increase the sensitisation, the steroid exposure, and the cost without the additional benefit over the individual agents. The hydrocortisone 1 percent for three to five days is the maximum steroid the nappy area needs in the typical case, and the specialist referral is the safeguard before the potent steroid is used. [7] [8]
The pitfall of the missed underlying condition is the one that harms the child. The zinc deficiency, the acrodermatitis enteropathica, presents with the periorificial dermatitis, the chronic diarrhoea, and the alopecia, and it is missed when the nappy-area rash is treated as the simple irritant dermatitis. The Langerhans cell histiocytosis presents with the purpuric, crusted papules in the seborrhoeic distribution, and it is missed when the persistent rash is treated with the escalating steroids rather than the biopsy. The child-protection awareness is the safeguard when the rash does not fit the offered mechanism or the pattern. [4] [12]
Prognosis & Disposition
The prognosis of the nappy dermatitis is excellent. The irritant subtype responds to the general skin care and the barrier within three to seven days in the great majority, and the candidal subtype responds to the addition of the antifungal within three to five days. The recurrence is common in the first year of life, driven by the wetness, the stool change, and the intercurrent illness, but the condition resolves permanently as the child matures, the skin thickens, and the toilet training removes the nappy. There is no long-term scarring, no pigmentation change, and no residual deformity in the typical case. [3] [9]
The disposition is primary care. The general practitioner and the child-health nurse own the recognition, the management, and the counselling of the typical nappy dermatitis. The dermatology referral is reserved for the persistent or the atypical rash, the suspected underlying condition, and the severe erosive subtype that does not respond to the standard measures. The emergency department is the destination for the febrile, unwell child with the suspected secondary bacterial infection. The long-term follow-up is unnecessary in the typical case, and the family is the safeguard against the recurrence through the maintenance of the general skin care. [2] [8]
Special Populations
The child with the recurrent nappy dermatitis is managed with the sustained general skin care and the anticipatory guidance. The family is counselled that the recurrence is driven by the wetness, the stool change, and the intercurrent illness, and the sustained barrier application and the frequent nappy changes are the prevention. The recurrent candidal subtype is managed with the prompt addition of the antifungal at the first sign of the fold involvement, and the underlying predisposition — the frequent antibiotic courses or the immunocompromise — is explored. [5] [7]
The child with the complex chronic condition or the technology dependence is at the higher risk of the nappy dermatitis because of the prolonged immobilisation, the frequent liquid stools, and the compromised skin integrity. The child with the spina bifida or the anorectal malformation has the reduced perineal sensation and the altered continence, and the aggressive barrier regimen and the skin surveillance are the management. The child with the immunocompromise is at the higher risk of the candidal and the bacterial superinfection, and the threshold for the swab and the systemic treatment is lower. [8]
The child with the disability or the neurodiversity may have the sensory aversion to the nappy change and the cleansing, and the behavioural support and the adapted routine are the management. The Indigenous and the socioeconomically disadvantaged child in the remote community may have the limited access to the disposable nappies and the clean water, and the practical support, the culturally safe education, and the non-judgemental approach are the management. The migrant and the refugee family may have the different nappy practices and the language barrier, and the interpreter and the culturally appropriate education are the management. [3] [6]
Evidence, Guidelines & Regional Differences
The evidence for the prevention and the treatment of the nappy dermatitis is anchored in the reviews and the clinical trials of the skin-care measures, the barrier preparations, and the topical antifungals. The Chiriac and Wollina 2024 narrative review in the Wiener Medizinische Wochenschrift provides the contemporary overview of the clinical presentation, the subtypes, and the treatment, and it frames the irritant-versus-candidal distinction as the decision that drives the treatment. [1]
The Octarica 2025 systematic review in the Acta Dermatovenerologica Alpina appraised the preventive and the curative approaches to the diaper dermatitis in children, and it confirmed the effectiveness of the frequent nappy changes, the super-absorbent disposable nappies, and the barrier preparations as the preventive measures, and the zinc oxide and the petrolatum as the first-line barriers. The Blume-Peytavi and Kanti 2018 review in the Pediatric Dermatology, "Prevention and treatment of diaper dermatitis," framed the stepwise approach from the general skin care to the barrier to the antifungal, and it is the structure the fellowship candidate follows at the bedside. [3] [6]
Octarica 2025 — preventive and curative approaches to diaper dermatitis in children
Systematic review of the interventions for the prevention and the treatment of the diaper dermatitis in children, appraising the skin-care measures, the barrier preparations, the topical antifungals, and the topical corticosteroids.
Key finding
The frequent nappy changes, the super-absorbent disposable nappies, and the barrier preparations (zinc oxide, petrolatum) are the effective preventive measures. The topical antifungals (clotrimazole, miconazole) are effective for the candidal subtype. The combined measures are more effective than the single intervention.
The Taudorf 2019 evidence-based review of the cutaneous candidiasis treatments in the Journal of the European Academy of Dermatology and Venereology confirmed the effectiveness of the topical azoles — the clotrimazole and the miconazole — for the localised candidal infection, and it is the evidence that supports the first-line topical antifungal for the candidal nappy dermatitis. The Dutta 2015 review of the candidal diaper dermatitis in the Indian Pediatrics framed the clinical recognition of the fold involvement and the satellite lesions and the empirical antifungal trial. [5] [7]
The Fölster-Holst 2018 review of the differential diagnoses of the diaper dermatitis in the Pediatric Dermatology is the definitive reference for the broader differential — the seborrhoeic, the atopic, the allergic, the psoriatic, and the rare mimics — and it is the reference the fellowship candidate cites when the rash does not respond in seven days. The Alberta 2005 report of the diaper dye dermatitis in the Pediatrics is the evidence for the allergic contact dermatitis to the nappy dye, and it is the reminder that the change of the nappy brand may be the cause and the cure. [4] [10]
The regional differences are modest. The Australian Therapeutic Guidelines and the Royal Children's Hospital Melbourne guidelines frame the nappy dermatitis with the same stepwise approach — the general skin care, the barrier, and the antifungal — and the over-the-counter availability of the zinc oxide and the clotrimazole makes the management accessible in the primary care. The NICE Clinical Knowledge Summaries in the United Kingdom and the American Academy of Pediatrics guidelines converge on the same approach. The practice in some regions still defaults to the combination steroid-antifungal creams as the first-line, but the contemporary evidence and the guideline updates favour the individual agents in the stepwise approach. [2] [3]
Exam Pearls
The fellowship answer turns on five facts. The first is the bedside distinction: the irritant subtype on the convex surfaces with the folds spared, and the candidal subtype with the fold involvement and the satellite lesions. The second is the pathophysiology: the moisture, the faecal enzymes, and the elevated pH disrupt the stratum corneum, and the Candida overgrows on the disrupted skin in the warm, moist fold. The third is the management sequence: the general skin care, the zinc oxide barrier, and the clotrimazole or miconazole antifungal added when Candida is present. The fourth is the hydrocortisone 1 percent for three to five days as the maximum steroid in the nappy area, with the potent steroids avoided because the occlusion increases the absorption. The fifth is the red flag: the rash that does not respond in seven days demands the broader differential, not the escalating treatment. [1] [4]
The three examiner traps are the following. The first is the antifungal prescribed for the convex-surface-only rash with the folds spared — the irritant subtype that needs the barrier alone, not the antifungal. The second is the potent topical steroid or the combination cream used in the nappy area — the occlusion increases the absorption and the atrophy risk, and the hydrocortisone 1 percent is the maximum for the short course. The third is the persistent rash treated with the escalating steroids rather than the diagnostic reconsideration — the missed seborrhoeic dermatitis, the zinc deficiency, or the Langerhans cell histiocytosis. [4] [7]
The examiner rewards the candidate who frames the nappy dermatitis around the pattern recognition, the stepwise treatment, and the red-flag reconsideration. The irritant subtype is the barrier and the skin care; the candidal subtype adds the antifungal; and the persistent rash demands the differential. This three-part framing — recognise the subtype, match the treatment, and reconsider at seven days — is the fellowship answer in miniature. [2] [3]
How do you tell the irritant from the candidal nappy dermatitis at the bedside?
By the fold involvement and the satellite lesions. The irritant dermatitis presents on the convex surfaces — the buttocks, the genitalia, the lower abdomen, and the upper thighs — with the inguinal and the gluteal folds spared, because the folds are the skin least exposed to the urine and the faeces. The candidal dermatitis extends into the folds and carries the satellite papules and pustules scattered beyond the main margin, and it often follows the antibiotic course or the oral thrush. The fold involvement and the satellites are the two features that decide whether the antifungal is added. [1] [5]
References
- [1]Chiriac A, Wollina U. Diaper dermatitis - a narrative review of clinical presentation, subtypes, and treatment. Wiener Medizinische Wochenschrift, 2024.PMID 37861874
- [2]Helms LE, Burrows HL. Diaper Dermatitis. Pediatrics in Review, 2021.PMID 33386307
- [3]Blume-Peytavi U, Kanti V. Prevention and treatment of diaper dermatitis. Pediatric Dermatology, 2018.PMID 29596731
- [4]Folster-Holst R. Differential diagnoses of diaper dermatitis. Pediatric Dermatology, 2018.PMID 29596730
- [5]Dutta A, Dutta M, Nag SS. Candidal Diaper Dermatitis. Indian Pediatrics, 2015.PMID 26713999
- [6]Octarica SG, Ellistasari EY, Dewi AK, et al. Preventive and curative approaches to diaper dermatitis in children: a systematic review. Acta Dermatovenerologica Alpina Pannonica et Adriatica, 2025.PMID 41014074
- [7]Taudorf EH, Jemec GBE, Hay RJ, et al. Cutaneous candidiasis - an evidence-based review of topical and systemic treatments to inform clinical practice. Journal of the European Academy of Dermatology and Venereology, 2019.PMID 31287594
- [8]Kazaks EL, Lane AT. Diaper dermatitis. Pediatric Clinics of North America, 2000.PMID 10943265
- [9]Singalavanija S, Frieden IJ. Diaper dermatitis. Pediatrics in Review, 1995.PMID 7731909
- [10]Alberta L, Sweeney SM, Wiss K. Diaper dye dermatitis. Pediatrics, 2005.PMID 16140691
- [11]Wolf R, Wolf D, Tuzun B, Tuzun Y. Diaper dermatitis. Clinics in Dermatology, 2000.PMID 11173200
- [12]Prasad HR, Srivastava P, Verma KK. Diaper dermatitis - an overview. Indian Journal of Pediatrics, 2003.PMID 14510084