Paeds · paediatric-dermatology
Neonatal pustular and vesiculobullous eruptions
Also known as Neonatal pustular dermatosis · Erythema toxicum neonatorum · Transient neonatal pustular melanosis · Neonatal cephalic pustulosis · Neonatal herpes simplex · Staphylococcal scalded skin syndrome of the neonate · Incontinentia pigmenti · Epidermolysis bullosa
Fellowship topic on the neonate presenting with a pustule, vesicle or bulla: the benign transient pustular eruptions (erythema toxicum neonatorum, transient neonatal pustular melanosis, neonatal cephalic pustulosis, infantile acropustulosis, eosinophilic pustular folliculitis) distinguished from the dangerous infections (neonatal herpes simplex, staphylococcal scalded skin syndrome, congenital syphilis, neonatal candidiasis) and the inherited blistering diseases (incontinentia pigmenti, epidermolysis bullosa); the eosinophilic-follicular, exfoliative-toxin desmoglein-1, viral-cytopathic, basement-membrane adhesion-defect and mosaic-X-inactivation pathophysiology; the bedside smear and the decision to reassure the well baby or to escalate the ill or atypical baby with a full sepsis workup, herpes simplex PCR, and empiric intravenous aciclovir and antibiotics; and AAP Red Book, NICE, BNFc and ANZ guidance on the aciclovir dose and the genodermatosis referral pathway.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Smear of a benign pustule is culture-negative
Overview & Definition
Picture a two-day-old term baby on the postnatal ward. The midwife has noticed a scattering of tiny pale-yellow spots on a red base across the chest and back. The baby is feeding well, is pink and warm, and is behaving normally. Nine times out of ten this is erythema toxicum — the commonest of a family of benign neonatal pustular eruptions that come, alarm the parents, and disappear on their own. The skill is not in calling this case benign; it is in never missing the one baby in the same clinic whose pustule or blister is the first sign of disseminated herpes, sepsis or a genodermatosis. [1] [2]
A pustule is a small superficial elevation of the skin filled with purulent (white or yellow) fluid; a vesicle is a clear fluid-filled blister under half a centimetre; and a bulla is a clear fluid-filled blister over half a centimetre. These three primary lesions look different at the bedside, and the difference matters, because a vesicle on a neonate behaves like a far more dangerous object than a follicular pustule on a well baby. The clinical frame is therefore a sorting exercise: take a baby with a pustule, vesicle or bulla and place them on the benign-and-transient side or the dangerous side, fast, and act accordingly. [1] [3]
The clinician's task has three layers. The first is recognition — naming the benign eruption from its morphology and timing, and spotting the dangerous patterns that should never be reassured. The second is the decision to investigate: the well baby with a classic benign lesion needs nothing but reassurance and a safety-net, whereas the ill or atypical baby needs a full sepsis evaluation, herpes simplex PCR and empiric aciclovir. The third is the pathway for the genodermatoses, where the general paediatric role is to recognise, protect the skin, and refer for biopsy-confirmed diagnosis. [1] [6]
Classification
Sort neonatal blistering and pustular eruptions by the primary lesion, because the morphology points you to the mechanism and the danger. A pustule raises a different set of possibilities from a clear vesicle or a large bulla, and within each morphology the same split recurs — benign-transient on one side, infectious or inherited on the other. [1]
For the pustule, the benign-transient group holds most of the common disease. Erythema toxicum neonatorum is the follicular, erythema-based pustule of the first days of life. Transient neonatal pustular melanosis is present at birth, has no erythematous base, involves the palms and soles, and leaves hyperpigmentation. Neonatal cephalic pustulosis (often called neonatal acne) is a papulopustular eruption of the cheeks and chin in the first weeks. Infantile acropustulosis and eosinophilic pustular folliculitis are less common itchy, recurrent pustular eruptions of infancy that complete the benign side. The infectious-and-dangerous pustules are staphylococcal impetigo, congenital syphilis, neonatal candidiasis and, occasionally, disseminated herpes. [2] [3] [4]
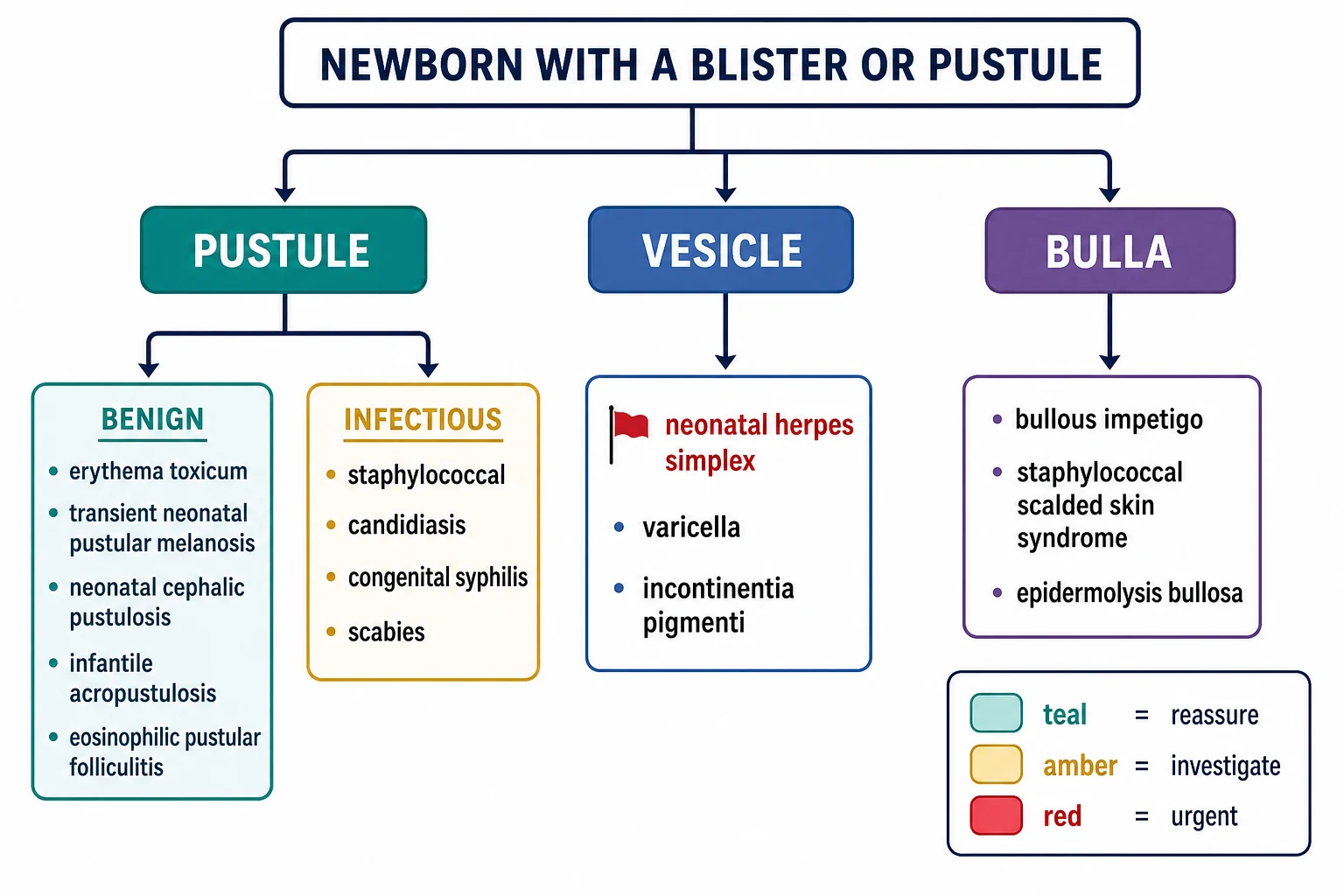
For the vesicle and bulla, the dangerous group dominates the differential. A clustered vesicle on an erythematous base in an ill neonate is neonatal herpes simplex until proven otherwise. Widespread tender erythema with flaccid bullae and sheet-like desquamation is staphylococcal scalded skin syndrome. A linear, blaschkoid vesicular eruption in a female neonate is incontinentia pigmenti. Blistering and skin loss from birth at sites of friction is epidermolysis bullosa. The mucosae hold one of the most useful clues: staphylococcal scalded skin syndrome spares them, whereas Stevens-Johnson syndrome and toxic epidermal necrolysis involve them — a distinction that holds even in the youngest babies. [10] [8] [9]
Epidemiology & Risk Factors
Most neonatal pustular eruptions are common, and most are benign. Erythema toxicum neonatorum affects up to half of term newborns and is rare in the very preterm baby under 1000 grams; it peaks at 24 to 48 hours of life and fades within days. Transient neonatal pustular melanosis occurs in roughly four to five percent of Black newborns and far less often in white infants, and it is present at birth. Neonatal cephalic pustulosis appears in the first two to four weeks. Together these benign eruptions account for the overwhelming majority of pustules a clinician will see on a postnatal ward or in a primary-care clinic. [2] [3] [4]
The dangerous infections are individually uncommon but collectively the reason this topic carries its weight. Neonatal herpes simplex affects roughly one in 3000 to one in 20000 live births depending on region and reporting, and most cases are acquired during passage through an infected birth canal. The risk to the baby is highest when the mother has a primary first-episode genital herpes lesion near delivery, because primary infection carries high-level viral shedding and the maternal antibody has not yet developed; recurrent maternal HSV sheds far less virus and the risk of transmission is much lower. [6] [7]
The risk factors that raise suspicion of a dangerous cause group around the baby and the mother. On the baby's side, prematurity and low birth weight, an ill appearance, fever, and lesions that do not fit a benign pattern lower the threshold to investigate. On the maternal and peripartum side, prolonged rupture of membranes, a scalp electrode in the presence of genital HSV, a maternal genital HSV lesion or fever at delivery, and inadequate antenatal syphilis screening or treatment all point toward the dangerous end of the differential. Recognising these upstream factors is part of the bedside risk-stratification. [7] [11]
In Australia and Aotearoa New Zealand, the late-presentation and inadequately treated maternal syphilis has driven a resurgence of congenital syphilis, so a pustular or vesicular eruption with hepatosplenomegaly, snuffles, or palmar and plantar involvement in an unwell neonate from a mother with incomplete screening must be treated as congenital syphilis until excluded. Remote and Aboriginal and Torres Strait Islander communities also carry higher rates of staphylococcal and streptococcal skin disease, so staphylococcal scalded skin syndrome and bullous impetigo remain real neonatal presentations that need early anti-staphylococcal therapy. [11] [10]
Pathophysiology
Why does a follicle erupt into a harmless eosinophilic pustule in one baby, while a clear vesicle in another turns out to be a disseminating herpes infection? Each major entity has its own mechanism, and the mechanism explains the morphology. [1]
Erythema toxicum is an idiopathic, benign reaction centred on the hair follicle. The pustule sits on a follicle, and its contents are rich in eosinophils, which is why a Wright or Giemsa-stained smear shows eosinophils and why affected babies often have a peripheral eosinophilia. The reaction is self-limiting and leaves no trace, consistent with an exaggerated but harmless response to colonisation of the newborn skin. [2]
Staphylococcal scalded skin syndrome shares a single mechanism with the bullous impetigo of older infants. Certain phage-group II strains of Staphylococcus aureus produce exfoliative toxins A and B, which are serine proteases that specifically cleave desmoglein-1 — the adhesion molecule that holds keratinocytes together in the superficial, granular layer of the epidermis. When desmoglein-1 is cleaved, the superficial epidermis splits, fluid accumulates, and a bulla forms; if the toxin circulates from a distant focus, the splitting becomes widespread and the skin shears off in sheets. The mucous membranes are spared because mucosal epithelium co-expresses desmoglein-3, which holds the cells together even when desmoglein-1 is cleaved. [10]
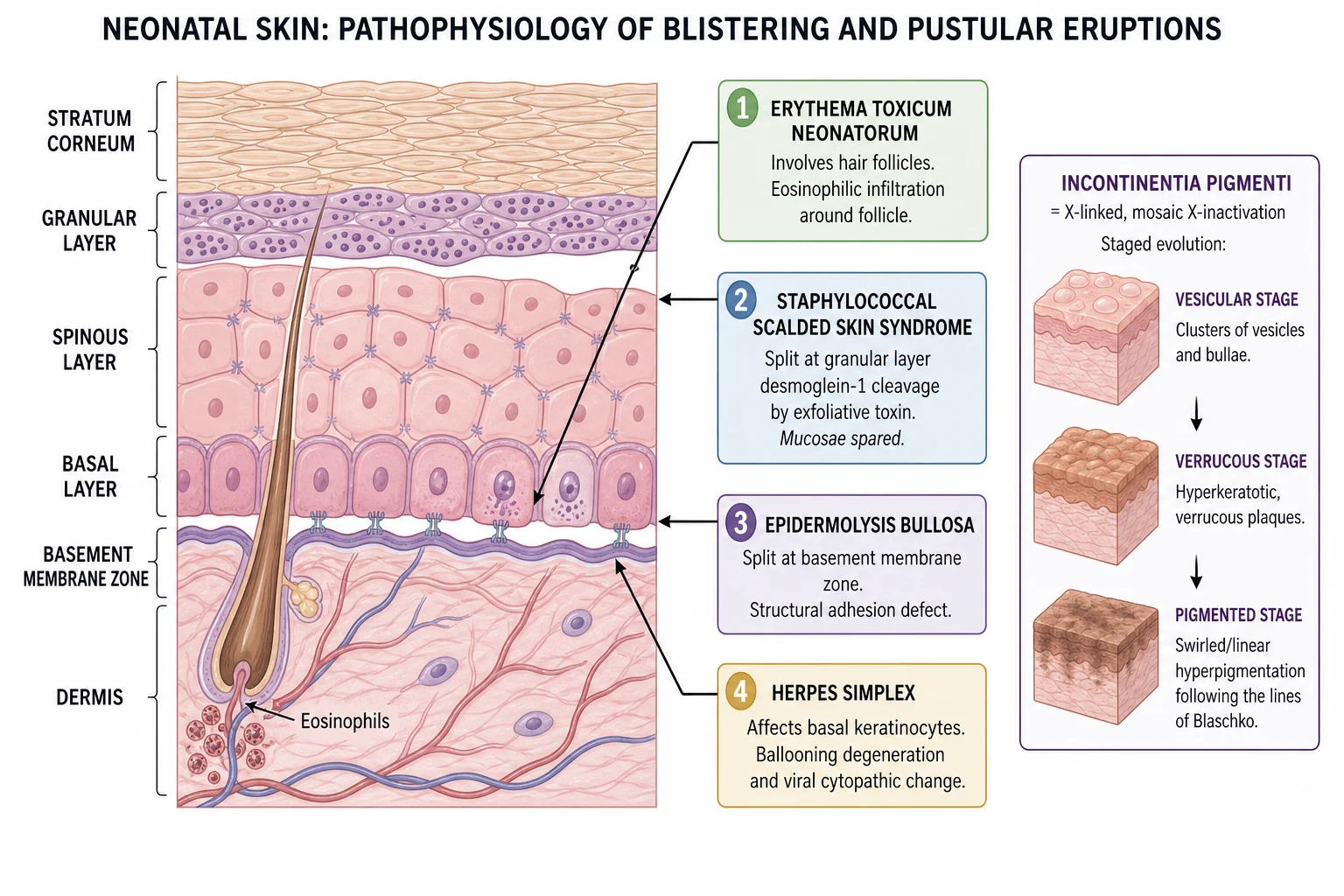
Neonatal herpes simplex destroys infected keratinocytes directly. The virus produces ballooning degeneration and a viral cytopathic effect in the basal and parabasal cells, and a Tzanck smear of an unroofed vesicle may show multinucleated giant cells. The clinical danger comes from where the virus goes next: it may stay as skin-eye-mouth disease, or it may disseminate to the liver, lungs and adrenal glands, or reach the central nervous system as meningoencephalitis. The disseminated and central-nervous-system forms carry the highest mortality and the worst long-term neurodevelopmental outcome, and the risk climbs the longer treatment is delayed. [6] [7]
Epidermolysis bullosa is a group of inherited defects of the structures that glue the epidermis to the dermis. Depending on the mutated gene and the resulting protein, the split sits at a different level — within the basal layer in simplex disease, at the basement membrane zone in junctional disease, and in the upper dermis in dystrophic disease. In every subtype the shared mechanism is the same: minor friction or trauma shears the skin at a mechanically weak level, which is why the blisters appear at the points of handling — hands, feet, oral cavity and nappy area — and why gentle handling is both diagnosis and treatment. [9]
Incontinentia pigmenti works by a different logic again. It is an X-linked dominant disorder caused by mutation of the IKBKG (NEMO) gene, lethal in most males, so affected babies are nearly always female. The cutaneous pattern is mosaic: because of random X-inactivation, the abnormal cells survive in streaks that follow the lines of Blaschko, producing the characteristic linear, swirling distribution. The eruption then evolves through stages — vesicular, then verrucous, then linear hyperpigmented, then atrophic — and the same gene defect can affect the eyes, teeth and central nervous system, which is why recognition triggers those screens. [8]
Clinical Presentation
The benign eruptions share a pattern: a well, feeding, afebrile neonate with a lesion that fits a recognised morphology. Erythema toxicum appears in the first one to two days as blotchy erythematous macules, each topped by a central pale-yellow papule or pustule, scattered over the trunk, face and proximal limbs and sparing the palms and soles. The baby is completely well. The lesions migrate and resolve within days without treatment or scarring. [2]
Transient neonatal pustular melanosis is striking because it is present at birth and lacks the erythematous base of erythema toxicum. The pustules are flaccid and non-erythematous, and they rupture quickly to leave a fine collarette of scale, which then evolves into a hyperpigmented macule over weeks to months. The distribution includes the palms and soles — the inverse of erythema toxicum — and it is more common in Black and darker-skinned newborns. [3]
Neonatal cephalic pustulosis presents in the first weeks of life as small papules and pustules on the cheeks, forehead and chin of an otherwise well baby. It lacks the comedones of true adolescent acne, which is why many now prefer the term cephalic pustulosis over neonatal acne. It resolves over weeks. Infantile acropustulosis and eosinophilic pustular folliculitis are less common, itchy, recurrent eruptions — acropustulosis on the palms, soles and extensor surfaces in episodes, and eosinophilic pustular folliculitis on the scalp and extremities — that complete the benign side. [4] [5]
The dangerous presentations are the ones you cannot reassure. A clustered or scattered vesicular eruption on an ill, febrile neonate is neonatal herpes simplex; the vesicles may be on the scalp (especially at a scalp-electrode site), the trunk, or the eye, and a vesicle anywhere on a sick neonate demands the herpes workup. Widespread tender erythema with flaccid bullae and sheet-like desquamation, a positive Nikolsky sign and spared mucosae is staphylococcal scalded skin syndrome. Pustules with hepatosplenomegaly, snuffles, respiratory distress or palmar-plantar involvement raise congenital syphilis; a widespread congenital candidal pustulosis produces a diffuse erythematous pustular eruption from birth. A linear, blaschkoid vesicular eruption in a female neonate is incontinentia pigmenti, and blistering and skin loss from birth at friction sites, worsening with handling, is epidermolysis bullosa. [6] [10] [8] [9]
Differential Diagnosis
For a pustule in a well neonate, the differential turns on morphology, timing and distribution. Erythema toxicum is follicular, sits on an erythematous base, peaks at 24 to 48 hours and spares the palms and soles. Transient neonatal pustular melanosis is present at birth, has no erythema, involves the palms and soles and leaves pigmentation. Neonatal cephalic pustulosis is confined to the face in a well baby in the first weeks. A smear of the pustule contents confirms a benign diagnosis: eosinophils in erythema toxicum, neutrophils in transient neonatal pustular melanosis, and culture-negative in both. [2] [3]
For a pustule in an ill neonate, the dangerous group takes over: staphylococcal impetigo, disseminated herpes simplex, congenital syphilis, neonatal candidiasis, and — if the eruption is refractory, crusted and sits in a seborrhoeic and nappy-area distribution — Langerhans cell histiocytosis. The ill appearance of the baby, the failure of the pustule to fit a benign pattern, and any systemic sign override the temptation to label a pustule benign. [11] [12]
For a vesicle or bulla, the dangerous differential is wide. Herpes simplex clusters on an erythematous base and may disseminate. Staphylococcal scalded skin syndrome gives widespread tender peeling with spared mucosae. Incontinentia pigmenti follows the lines of Blaschko in a female, staging through vesicular then verrucous then pigmented phases. Epidermolysis bullosa blisters at friction sites from birth. The decisive bedside discriminator is simple in principle and non-negotiable in practice: an ill or febrile neonate, any vesicle that does not fit a benign pattern, blistering from birth at friction sites, or widespread skin loss moves the baby straight to the investigate-and-treat pathway. [6] [10] [8] [9]
Clinical & Bedside Assessment
The assessment begins with the neonatal and maternal history and a careful look at the skin in good light. Establish the gestation and birth details, the mode of delivery, whether the membranes were ruptured for a prolonged period, whether a scalp electrode was used, the maternal genital HSV history and whether there was a lesion or fever at delivery, the antenatal syphilis and HSV serology, the day of life the eruption began, and how the baby is feeding and behaving. These details reframe the same lesion: a vesicle on the scalp of a day-ten neonate born to a mother with a primary genital HSV lesion is herpes until proven otherwise. [6] [7]
Examine the whole skin, not just the obvious lesion. Characterise the primary lesion — is it a pustule, a vesicle or a bulla? Note its base (erythematous or not), its distribution (trunk, face, palms, soles, nappy area, or linear and blaschkoid), and whether the lesions are all at the same stage or in different stages. Look specifically at the palms and soles, because their involvement or sparing separates erythema toxicum from transient neonatal pustular melanosis. Look at the mucosae, because their sparing points to staphylococcal scalded skin syndrome and their involvement to Stevens-Johnson syndrome and herpes. Look for skin fragility at friction sites, the hallmark of epidermolysis bullosa. [2] [9]
Assess the baby's wellness directly. Neonates do not localise infection well, so use a neonatal assessment approach — temperature instability, tone, feeding, perfusion, respiratory effort and behaviour. An ill-appearing or febrile neonate with a blister overrides any benign label and mandates a sepsis evaluation, because the well-or-ill call is the single most powerful discriminator this topic teaches. A benign-looking pustule on a sick baby is still a sick baby. [1] [6]
Where the diagnosis is genuinely in doubt, a smear of the pustule contents at the bedside moves the assessment forward. Erythema toxicum shows eosinophils on a Wright or Giemsa stain; transient neonatal pustular melanosis shows neutrophils; both are culture-negative. A bacterial pustule grows an organism; a herpetic vesicle may show multinucleated giant cells on a Tzanck smear. The smear is the bedside tool that converts uncertainty into a decision to reassure or to escalate. [2] [3]
Investigations
The well baby with a classic benign eruption needs no investigations. Confirming erythema toxicum or transient neonatal pustular melanosis is a clinical act, and where doubt remains, a smear of the pustule contents settles it. Over-investigating a well baby with a benign lesion is poor stewardship and exposes the neonate to unnecessary blood sampling — provided the safety-net is clear. [2] [3]
The dangerous or atypical neonate needs a full sepsis evaluation: a full blood count and differential, C-reactive protein, blood culture, urinalysis and urine culture (catheter or suprapubic), and a chest radiograph as indicated. These are the same tests that anchor any neonatal sepsis assessment, because the dangerous skin eruption is, at heart, a sepsis presentation. [1]
For suspected neonatal herpes simplex, the modern standard is HSV PCR taken from surface swabs of the conjunctiva, mouth, nasopharynx and rectum, from any skin vesicle, and from the blood and cerebrospinal fluid. PCR has replaced viral culture as the diagnostic test of choice because it is faster and more sensitive. Liver function tests look for the hepatitis of disseminated disease, and a lumbar puncture is performed for CSF cell count, protein, glucose and HSV PCR unless contraindicated. A vesicle may also be scraped for a Tzanck smear or direct fluorescent antibody, but these are adjuncts rather than replacements for PCR. [6] [7]
For suspected congenital syphilis, send maternal and neonatal syphilis serology (both treponemal and non-treponemal tests), obtain long-bone radiographs for the periostitis of early congenital syphilis, and examine the cerebrospinal fluid. For suspected neonatal candidiasis, send skin scrapings for microscopy and culture. For suspected epidermolysis bullosa, a skin biopsy with immunofluorescence mapping defines the level of the split and the subtype; for suspected incontinentia pigmenti, the clinical blaschkoid pattern and the peripheral eosinophilia, followed by IKBKG genetic testing, confirm the diagnosis. [11] [12] [9] [8]
Management — Resuscitation
Resuscitation belongs to the dangerous neonate, and in this topic that means the ill or febrile baby with a blister, any clustered or disseminated vesicle, widespread tender peeling, or blistering from birth at friction sites. Each of these warrants immediate assessment, intravenous access and senior review, because neonates deteriorate quickly and the dangerous causes do not wait for confirmatory tests. [6] [10]
For suspected neonatal herpes simplex, start intravenous aciclovir promptly after taking samples but without waiting for the results. The reasoning chain is direct: delayed aciclovir increases mortality and long-term neurodevelopmental morbidity, and the disease can disseminate or reach the central nervous system within hours, so the test result cannot be the gate to treatment. Admit the baby, monitor for disseminated disease (hepatitis, pneumonitis, disseminated intravascular coagulation), and involve paediatric infectious diseases for the duration of therapy and the follow-up plan. [6] [7]
Neonatal herpes simplex — empiric aciclovir (AAP Red Book / BNFc — confirm locally)
For suspected staphylococcal scalded skin syndrome, admit and treat as a burn. Start intravenous anti-staphylococcal therapy — flucloxacillin, with vancomycin where the child is critical or methicillin-resistant Staphylococcus aureus is plausible — and provide meticulous fluid, electrolyte and temperature management, non-adherent wound care and adequate analgesia. The superficial skin loss behaves like a partial-thickness burn even though the split is high in the epidermis, because the compromised barrier weeps and loses heat and water. Identify and treat the primary staphylococcal focus. [10]
For the septic neonate, give empiric intravenous broad-spectrum antibiotics early — covering group B streptococcus, Escherichia coli and Listeria — and add aciclovir wherever HSV is plausible. Escalate to neonatal intensive care for the shocked, apnoeic or failing baby. Keep resuscitation separate from reassurance in your mind: the well baby with a confirmed benign eruption needs nothing but explanation, while the ill or atypical baby needs the hospital, the intravenous line and the empirical antimicrobial bundle. [1] [6]
Management — Definitive & Stepwise
Definitive management runs as a two-pathway decision, and the wellness of the baby plus the morphology decide the pathway. A well baby with a clearly benign eruption is reassured and safety-netted; an ill or atypical baby is investigated and treated. The art is choosing the least intervention that is safe, and no less. [1]
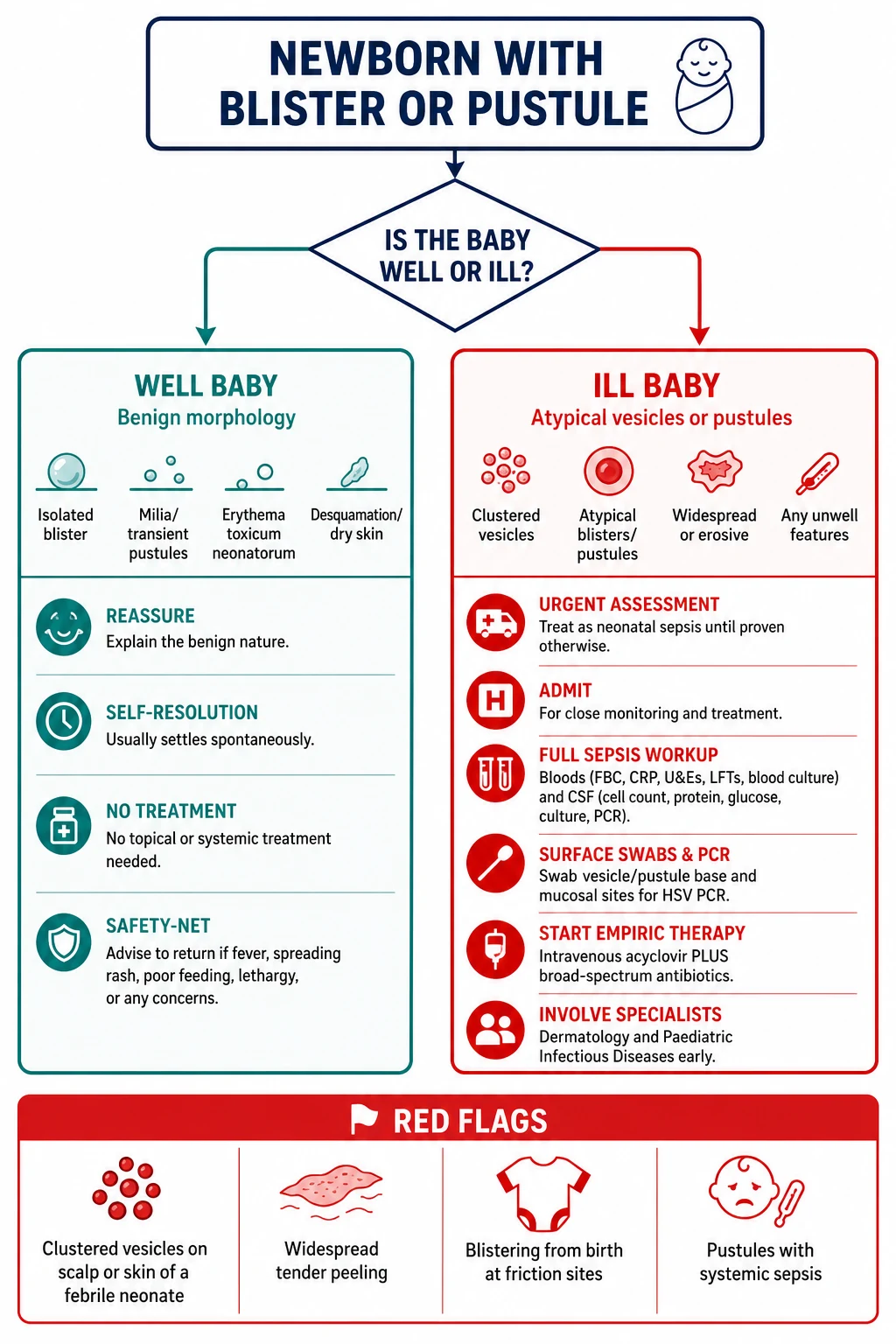
For a confirmed benign pustular eruption — erythema toxicum, transient neonatal pustular melanosis, neonatal cephalic pustulosis — give no active treatment. Explain the natural history and the expected self-resolution, and provide a clear safety-net: return immediately for fever, poor feeding, lethargy, or any change in the lesions. Reassurance is the correct stewardship when the diagnosis is secure; the only error is reassuring an insecure diagnosis. [2] [3] [4]
For neonatal herpes simplex, give intravenous aciclovir for the full recommended course — 14 days for skin-eye-mouth disease and 21 days for central-nervous-system and disseminated disease — at 20 mg/kg every eight hours, with the dose, duration and follow-on suppressive therapy guided by the current AAP Red Book and national guidance and by paediatric infectious diseases. The disease category dictates the course length, and the follow-up surveillance for recurrence and neurodevelopment is part of the treatment, not an add-on. [6] [7]
For staphylococcal scalded skin syndrome, deliver intravenous anti-staphylococcal therapy and burn-style supportive care, identify and treat the primary staphylococcal focus (often conjunctival, umbilical or a skin site), and de-escalate to oral therapy as the child recovers. The outcome in children is good with prompt treatment, in contrast to the high mortality seen in adults, because the split is superficial and the deeper epidermal stem cells regenerate. [10]
For the genodermatoses, the general paediatric role is recognition, protection of the skin, and referral rather than definitive subtyping. In suspected epidermolysis bullosa, minimise friction and trauma, use non-adherent dressings, avoid adhesive tapes, handle the baby gently, and arrange skin biopsy with immunofluorescence mapping and referral to the specialist epidermolysis bullosa centre. In suspected incontinentia pigmenti, involve dermatology, arrange IKBKG genetic testing, and screen the eyes (for the retinal vascular changes that threaten vision), the teeth and the central nervous system. The skin eruption is the visible tip; the extracutaneous disease is what harms. [9] [8]
The two-pathway triage of a neonatal blister or pustule
Assess the baby's wellness first: an ill or febrile neonate overrides any benign label and goes to the urgent pathway.
Characterise the lesion: pustule, vesicle or bulla; erythematous base or not; palms and soles involved or spared; linear or blaschkoid; from birth or later; friction-related or not.
Well baby with classic benign morphology (erythema toxicum, transient neonatal pustular melanosis, neonatal cephalic pustulosis): confirm clinically, smear if in doubt, reassure with a safety-net.
Ill or febrile baby, atypical vesicle, or widespread skin loss: full sepsis workup, HSV PCR from surface swabs and CSF, start empiric intravenous aciclovir and broad-spectrum antibiotics.
Suspected staphylococcal scalded skin syndrome: admit, intravenous anti-staphylococcal therapy, burn-style fluid and wound care, identify and treat the primary focus.
Suspected epidermolysis bullosa: minimise friction, non-adherent dressings, biopsy with immunofluorescence mapping, refer to the EB specialist centre.
Suspected incontinentia pigmenti: dermatology and IKBKG testing, and screen the eyes, teeth and central nervous system.
Safety-net every reassured family: return for fever, poor feeding, lethargy or any change in the lesions.
Specific Subtypes & Scenarios
A day-two term neonate with scattered follicular pustules on an erythematous base, well and feeding. This is the everyday erythema toxicum. Confirm clinically — follicular, erythematous base, sparing the palms and soles, peaking at 24 to 48 hours. A smear is only needed if doubt remains; it shows eosinophils and is culture-negative. Reassure the family, explain the self-resolution, and give the safety-net. No treatment is required. [2]
A Black newborn with present-at-birth pustules leaving collarettes and pigmentation on the trunk, palms and soles, well. This is transient neonatal pustular melanosis. The key features — present at birth, no erythematous base, involvement of the palms and soles, and the evolution through collarette to hyperpigmentation — separate it from erythema toxicum. Reassure the family; the pigmentation fades over months and no treatment is needed. [3]
A two-week-old with papules and pustules on the cheeks and chin, well. This is neonatal cephalic pustulosis (neonatal acne). It lacks comedones, sits on the face of a well baby, and resolves over weeks. Reassurance is the rule; an occasional case benefits from a short course of a topical agent, but most need nothing. [4]
A ten-day-old febrile neonate with clustered vesicles on the scalp and lethargy. This is the neonatal herpes simplex presentation that must never be missed. Take a full sepsis evaluation, HSV PCR from surface swabs (conjunctiva, mouth, nasopharynx, rectum) and any vesicle, blood PCR, liver function tests and CSF PCR, and start intravenous aciclovir at 20 mg/kg every eight hours without waiting for results. The risk of delayed treatment is disseminated and central-nervous-system disease, which carry the worst outcomes. [6] [7]
A three-week-old with widespread tender erythema, flaccid bullae and perioral peeling, irritable. This is staphylococcal scalded skin syndrome. Admit for intravenous anti-staphylococcal therapy (flucloxacillin, or vancomycin where MRSA is plausible), burn-style fluid and wound care, and analgesia. Identify and treat the primary focus — often conjunctival, umbilical or a skin site. The mucosae are spared, which separates it from Stevens-Johnson syndrome and toxic epidermal necrolysis. [10]
A female neonate with linear vesicles following the lines of Blaschko on a limb and trunk. This is incontinentia pigmenti. The linear, swirling pattern in a female, the staged evolution (vesicular then verrucous then pigmented then atrophic), and a peripheral eosinophilia are the clues. Arrange dermatology review and IKBKG genetic testing, and screen the eyes (retinal vascular changes threaten vision), the teeth and the central nervous system. The skin eruption is the first sign of a multisystem disease. [8]
A neonate with blistering and skin loss at the feet, hands and oral cavity from birth, worsening with handling. This is epidermolysis bullosa. Minimise friction and trauma, avoid adhesive tapes, use non-adherent dressings, handle the baby gently, and arrange skin biopsy with immunofluorescence mapping and referral to the specialist epidermolysis bullosa centre. The general paediatric role is protection and referral; the subtyping and the long-term pathway are specialist-led. [9]
Complications & Pitfalls
The complications of the dangerous causes are the reason this topic matters. Disseminated herpes simplex causes hepatitis, pneumonitis, disseminated intravascular coagulation and encephalitis; the disseminated and central-nervous-system forms carry the highest mortality and the worst long-term neurodevelopmental outcome, and the risk rises the longer aciclovir is delayed. Staphylococcal scalded skin syndrome causes fluid, electrolyte and heat loss and secondary infection, behaving like a partial-thickness burn. Congenital syphilis and neonatal candidiasis can each be the skin sign of systemic disease. Severe epidermolysis bullosa brings chronic pain, scarring, infection, failure to thrive and, in some subtypes, a risk of squamous-cell carcinoma in later life. [6] [10] [9]
The cardinal pitfall is dismissing a neonatal blister or pustule as benign without assessing the baby. The single most powerful discriminator this topic teaches is the well-or-ill call, and an ill or febrile neonate — or any vesicle that does not fit a benign pattern — is herpes or sepsis until proven otherwise. A benign-looking lesion on a sick baby is still a sick baby, and reassuring it is the error that harms. [1] [6]
A second pitfall is treating a well baby with unnecessary antibiotics. The smear of a benign pustule is culture-negative and shows eosinophils or neutrophils, which should spare the baby a sepsis workup when the diagnosis is secure. Over-investigation of the well baby is poor stewardship; the correct discipline is to confirm clinically, smear if in doubt, and reassure with a clear safety-net. [2] [3]
A third pitfall is fixing on a single lesion in incontinentia pigmenti. The diagnosis is in the pattern — the linear, blaschkoid distribution and the staged evolution from vesicular through verrucous to pigmented — and the extracutaneous disease (eyes, teeth, central nervous system) is what harms. Missing the pattern, or treating the skin in isolation without the extracutaneous screen, fails the baby. [8]
A fourth pitfall is rough handling of suspected epidermolysis bullosa. Adhesive tapes, friction and shearing forces worsen the blistering and the skin loss, and a delay in adopting gentle handling, non-adherent dressings and EB-centre referral adds preventable harm. The handling is part of the diagnosis and part of the treatment. [9]
The final pitfall is ignoring the safeguarding dimension. Most neonatal herpes reflects vertical transmission, but atypical or recurrent lesions — especially in an older baby or in an inconsistent history — should prompt discussion with the safeguarding team, because disguised-commission and non-accidental infection are real, if uncommon, presentations. The skin sign is sometimes the first sign of harm. [7]
Prognosis & Disposition
The benign pustular eruptions resolve without treatment and without scarring — within days for erythema toxicum, and over weeks to months for the pigmentation of transient neonatal pustular melanosis. The disposition for a well baby with a confirmed benign eruption is primary care or outpatient reassurance with a clear safety-net, and the family should leave understanding what to watch for. [2] [3]
The prognosis of the dangerous causes depends on the speed of recognition and treatment. Neonatal herpes simplex is graded by disease category: skin-eye-mouth disease has the best outlook, while disseminated and central-nervous-system disease carry substantial mortality and neurodevelopmental morbidity even with treatment, and the risk climbs the longer aciclovir is delayed. Staphylococcal scalded skin syndrome has a good prognosis in children with prompt treatment, because the split is superficial and the deeper epidermis regenerates, in contrast to the high mortality seen in adults. [6] [10]
Disposition follows the pathway. Admit any ill or febrile neonate, any suspected neonatal herpes simplex, any staphylococcal scalded skin syndrome, and any neonate with widespread blistering. Manage in the community the well baby with a confirmed benign eruption, with a clear safety-net for fever, poor feeding, lethargy or changing lesions. The threshold to admit the very young, the premature and the immunocompromised is deliberately low. [1] [6]
The genodermatoses require ongoing specialist care. Epidermolysis bullosa is managed through a specialist EB centre, and incontinentia pigmenti through dermatology with ophthalmology, dental and neurodevelopmental surveillance. The general paediatrician's role is to recognise, protect the skin, refer, and coordinate the long-term multidisciplinary pathway. [9] [8]
Special Populations
Premature and low-birth-weight neonates are more vulnerable to disseminated infection and may show blunted or atypical skin signs, which lowers the threshold for sepsis evaluation and empiric aciclovir. A preterm baby with a pustule that does not fit a benign pattern warrants a lower, not a higher, threshold to investigate. [6] [1]
A neonate born to a mother with a primary genital herpes lesion near delivery carries the highest risk of neonatal HSV, because primary infection sheds high viral loads and the maternal antibody has not yet developed. The management of maternal HSV and the mode of delivery — the upstream prevention — is a shared obstetric, neonatal and infectious-diseases decision, and it is where most neonatal HSV is prevented. [6] [7]
Black and darker-skinned newborns more commonly show transient neonatal pustular melanosis with its characteristic residual hyperpigmentation. Recognising the normal variant prevents over-investigation and the anxiety of an uncertain label, and the pigmentary change should be anticipated and explained. [3]
A neonate with suspected non-accidental injury or disguised-commission infection — for example, atypical, recurrent or inconsistently explained lesions — must be discussed with the safeguarding team alongside the dermatology and infectious-diseases assessment. The skin sign is sometimes the first sign of harm, and the safeguarding lens belongs in the differential. [7]
Rural and remote neonates need clear safety-netting and early retrieval pathways, because the dangerous causes deteriorate quickly and the reassuring diagnosis must never delay escalation. A clear written safety-net, a low threshold to retrieve, and access to specialist dermatology and infectious-diseases advice by telehealth shape a plan that is deliverable where the baby lives. [1]
Evidence, Guidelines & Regional Differences
The recent comprehensive neonatal dermatology reviews frame the benign-versus-dangerous approach to neonatal pustular and vesiculobullous eruptions, consolidating the morphology-based differential and the bedside smear as the practical tools of triage. The detailed reviews of neonatal herpes simplex set the PCR-based diagnostic standard and the aciclovir treatment course by disease category, and the review of paediatric staphylococcal scalded skin syndrome consolidates the toxin-mediated mechanism and the burn-style supportive care. [1] [6] [7] [10]
The modern neonatal HSV diagnostic and treatment standard
Population: Neonates with suspected or confirmed herpes simplex virus disease, reviewed to define the diagnostic approach and the treatment course by disease category (skin-eye-mouth, central-nervous-system, disseminated).
Key finding
HSV PCR from surface swabs, blood and cerebrospinal fluid is the diagnostic standard; intravenous aciclovir at 20 mg/kg every eight hours for 14 days (skin-eye-mouth) or 21 days (central-nervous-system and disseminated) is the treatment course, with the longer course and follow-on suppression for the most severe disease.
Practice change
The diagnostic and treatment standard is PCR-first and prompt-aciclovir; the disease category sets the course length, and delayed treatment worsens mortality and neurodevelopmental outcome.
The genodermatosis evidence has moved from histology-only diagnosis toward skin biopsy with immunofluorescence mapping for epidermolysis bullosa subtyping and IKBKG genetic testing for incontinentia pigmenti, replacing older approaches that could not define the split level or confirm the mosaic X-linked pattern. The clinical-practice guideline for the newborn with epidermolysis bullosa consolidates the gentle-handling, non-adherent-dressing and specialist-centre pathway. [9] [8]
The regional guidance structure is consistent in principle and varies in detail. The AAP Red Book (Kimberlin) sets the neonatal HSV aciclovir dose and duration and is the global reference; in the UK, NICE guidance on early-onset neonatal infection and the BNFc set the local antimicrobial and aciclovir pathways; in Australia and New Zealand, the Therapeutic Guidelines and the Royal Children's Hospital Melbourne guidelines set the local approach, alongside the resurgent-congenital-syphilis awareness. The AAP and RCPCH set the congenital syphilis framework. In every region the principle is the same: reassure the well baby with a benign eruption, escalate the ill or atypical baby with a full sepsis workup and empiric aciclovir, and refer the genodermatoses for biopsy-confirmed diagnosis. [6] [11] [1]
The controversies are real and active: the cases of neonatal HSV that present without a skin lesion, the role of empiric aciclovir in the septic neonate with no clear source, the optimal suppressive therapy after a treated episode, and the resurgent congenital syphilis that keeps syphilis in the differential of the unwell pustular neonate. These are decided with paediatric infectious diseases, never alone, and the defence against each is the same discipline: assess the baby first, confirm the benign diagnosis securely before reassuring, and treat the dangerous cause promptly while the tests are running. [7] [11]
Exam Pearls
- Erythema toxicum peaks at 24 to 48 hours, spares the palms and soles, sits on an erythematous base, and shows eosinophils on a smear — the commonest benign neonatal pustular eruption. [2]
- Transient neonatal pustular melanosis is present at birth, has no erythematous base, involves the palms and soles, and leaves hyperpigmentation; it is more common in Black newborns and shows neutrophils on a smear. [3]
- A vesicle on a neonate is herpes simplex until proven otherwise — clustered vesicles on an erythematous base in an ill baby demand PCR and intravenous aciclovir at 20 mg/kg every eight hours. [6]
- Staphylococcal scalded skin syndrome cleaves desmoglein-1, spares the mucosae, and is Nikolsky-positive — the mucosal sparing separates it from Stevens-Johnson syndrome and toxic epidermal necrolysis. [10]
- Incontinentia pigmenti is X-linked dominant (IKBKG), lethal in most males, follows the lines of Blaschko in females, and stages through vesicular, verrucous, pigmented and atrophic phases — screen the eyes, teeth and central nervous system. [8]
- Epidermolysis bullosa blisters at friction sites from birth; minimise handling, use non-adherent dressings, and refer for biopsy-confirmed subtyping. [9]
- The smear of a benign pustule is culture-negative: eosinophils in erythema toxicum, neutrophils in transient neonatal pustular melanosis. [2] [3]
- Maternal primary genital HSV near delivery carries the highest neonatal transmission risk; recurrent HSV has a much lower risk. [6]
- The single most powerful discriminator is the well-or-ill call — an ill or febrile neonate with a blister is herpes or sepsis until proven otherwise. [1]
- Aciclovir courses by category: 14 days for skin-eye-mouth disease, 21 days for central-nervous-system and disseminated disease. [7]
References
- [1]Wilson JL; Nanni SD Neonatal Dermatology. Prim Care, 2025.PMID 40835282
- [2]Schwartz RA; Janniger CK Erythema toxicum neonatorum. Cutis, 1996.PMID 8864602
- [3]Ramamurthy RS; Reveri M; Esterly NB; et al Transient neonatal pustular melanosis. J Pediatr, 1976.PMID 1271148
- [4]Bergman JN; Eichenfield LF Neonatal acne and cephalic pustulosis: is malassezia the whole story? Arch Dermatol, 2002.PMID 11843648
- [5]Ziemer M; Boer A Eosinophilic pustular folliculitis in infancy: not a distinctive inflammatory disease of the skin. Am J Dermatopathol, 2005.PMID 16148418
- [6]Pinninti SG; Kimberlin DW Neonatal herpes simplex virus infections. Semin Perinatol, 2018.PMID 29544668
- [7]Samies NL; James SH; Kimberlin DW Neonatal Herpes Simplex Virus Disease: Updates and Continued Challenges. Clin Perinatol, 2021.PMID 34030813
- [8]Herzum A; Viglizzo G; Gariazzo L; et al Neonatal incontinentia pigmenti. Ital J Dermatol Venerol, 2023.PMID 36930459
- [9]Lucky AW; Whalen J; Rowe S; et al Diagnosis and Care of the Newborn with Epidermolysis Bullosa. Neoreviews, 2021.PMID 34210808
- [10]Leung AKC; Barankin B; Leong KF Staphylococcal-scalded skin syndrome: evaluation, diagnosis, and management. World J Pediatr, 2018.PMID 29508362
- [11]Sankaran D; Partridge E; Lakshminrusimha S Congenital Syphilis-An Illustrative Review. Children (Basel), 2023.PMID 37628309
- [12]Aruna C; Seetharam K Congenital candidiasis. Indian Dermatol Online J, 2014.PMID 25506564