Paeds · paediatric-dermatology
Petechiae, purpura and vasculitic rashes
Also known as Petechiae · Purpura · Non-blanching rash · Immune thrombocytopenia · ITP · IgA vasculitis · Henoch-Schönlein purpura · Purpura fulminans · Meningococcaemia · Disseminated intravascular coagulation
Fellowship topic on the non-blanching rash in children — petechiae, purpura and vasculitic eruptions — framed as a triage problem. The first split is sick versus well: a febrile, toxic child with a rapidly evolving purpuric rash is meningococcal sepsis or purpura fulminans until proven otherwise and needs immediate antibiotics and resuscitation, while a well child with isolated petechiae and a normal examination is most likely immune thrombocytopenia (ITP). Cover the glass-test confirmation of non-blanching, the ISTH disseminated intravascular coagulation score and purpura fulminans, IgA vasculitis (Henoch-Schönlein purpura) with its palpable dependent purpura and mandatory renal follow-up, the haemolytic uraemic syndrome, leukaemia presenting as pancytopenia with blasts rather than isolated thrombocytopenia, and the safeguarding assessment of bruising using the TEN-4 FACES pattern. Diagnostic and triage focus throughout, cross-linking the dedicated sepsis, rash-approach and systemic-disease topics rather than duplicating their full protocols.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
PALPABLE — the hallmarks of a small-vessel vasculitis
Overview & Definition
Picture an eighteen-month-old brought in with a fever and a handful of tiny red spots that did not fade when her mother pressed a glass against them. Within two hours the spots have become dark purple patches spreading up her legs, her peripheries are cold, and she is grunting. This is the scenario that petechiae and purpura exist to make you think about, because the difference between a five-minute and a one-hour antibiotic is the difference between life and death in meningococcal disease. The clinician's job is to run the sick-versus-well split in the first minute, confirm the rash is genuinely non-blanching, and then move down a short, fast differential. [8]
Petechiae are tiny pinpoint haemorrhages under about two millimetres, purpura are larger flat bruises from a few millimetres to roughly a centimetre, and ecchymoses are larger still. All three represent blood outside the vessel lumen, which is why they do not blanch when you press them with a glass — the so-called glass test or tumbler test. Their causes span platelet problems (too few or dysfunctional), vessel-wall problems (vasculitis, infection, trauma) and coagulation problems, and the art is to read the child's wellness, the rash morphology and the tempo together rather than to chase a single diagnosis. [8]
The triage frame has three layers. The first is how sick is the child — fever, toxicity, shock and rapid progression mark the emergencies. The second is what does the rash look like — petechial versus purpuric, flat versus palpable, dependent versus generalised, necrotic versus fresh. The third is the blood count and film — isolated thrombocytopenia points one way, pancytopenia with blasts another, and a coagulopathy a third. Run all three and the differential narrows fast. [1] [9]
Classification
Sorting non-blanching lesions by size and by what they say about the child is the first step, because size and morphology predict mechanism. Petechiae are pinpoint, under about two millimetres, and usually reflect capillary bleeding from thrombocytopenia, raised intravascular pressure (coughing, vomiting, the face and upper chest after a paroxysm), or infection. Purpura are larger, and when they are palpable they point to inflammation of the vessel wall — a vasculitis. Ecchymoses are larger bruises, and in the wrong distribution they raise the question of trauma, accidental or otherwise. [5] [12]
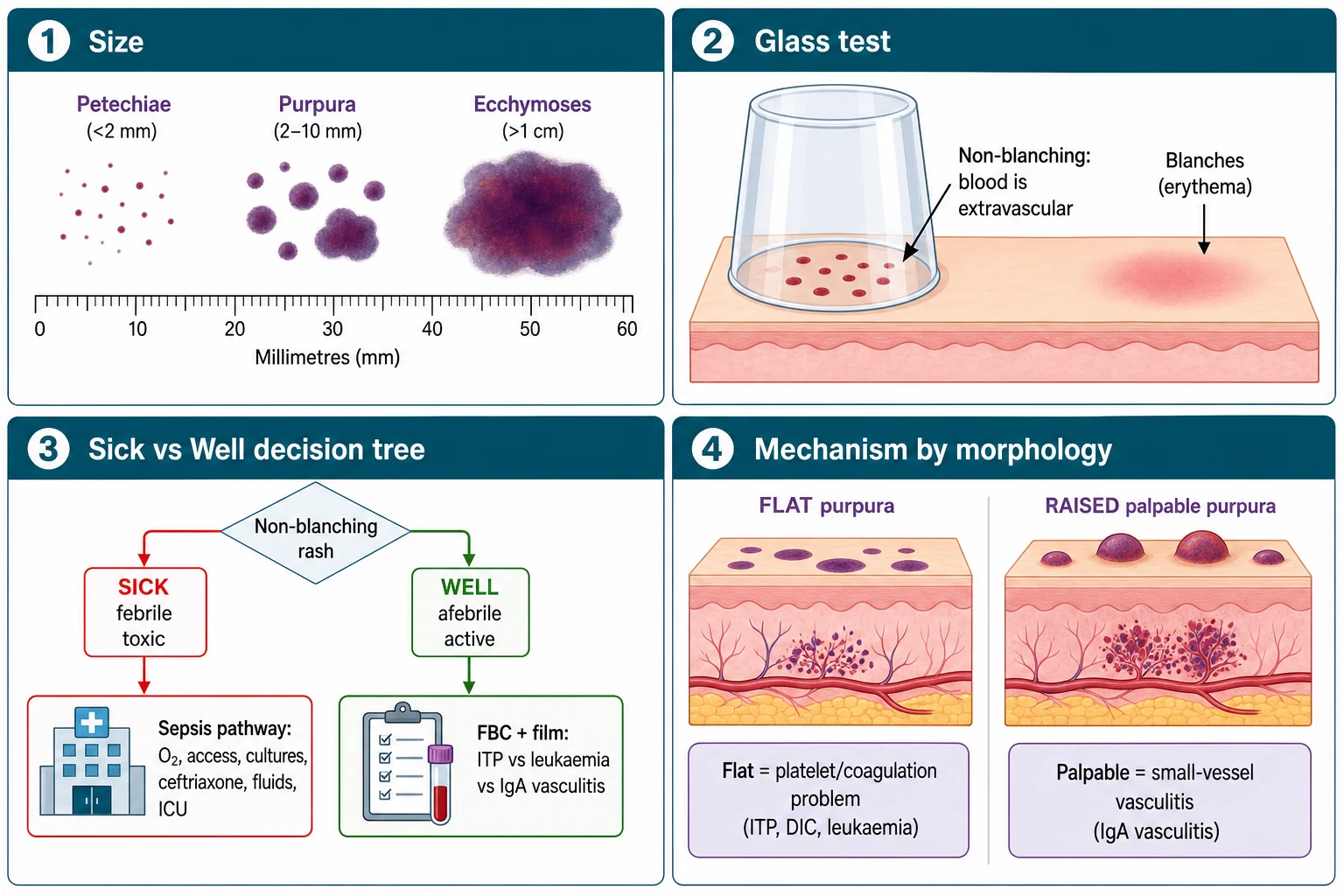
The most useful clinical classification is not by size alone but by the mechanism the morphology implies. A flat, non-palpable petechial or purpuric rash suggests a platelet or coagulation problem — ITP, leukaemia, disseminated intravascular coagulation, or a haemolytic uraemic syndrome. A raised, palpable purpura in dependent areas suggests a small-vessel vasculitis, of which IgA vasculitis is by far the commonest in children. A rapidly progressive, necrotic, map-like purpura with dusky grey centres signals purpura fulminans, whether from meningococcal sepsis, disseminated intravascular coagulation, or an inherited or acquired protein C or S deficiency. Reading the morphology this way turns a long differential into three short lists. [9] [10]
A second axis that examiners reward is the distribution. Petechiae confined to the face, neck and upper chest after prolonged coughing or vomiting are mechanical and benign. Purpura on the lower limbs and buttocks in a young child points to IgA vasculitis. Generalised petechiae and bruising with mucosal bleeding point to a platelet problem such as ITP. Bruising on the torso, ear, neck or face, or bruising in a non-mobile infant, points to non-accidental injury and triggers the safeguarding pathway. [12] [6]
Epidemiology & Risk Factors
Petechiae and purpura are common presentations, but their frequency is driven by a handful of conditions that vary by age and setting. Immune thrombocytopenia is the commonest cause of isolated, acute thrombocytopenia in an otherwise well child aged two to ten years, often one to four weeks after a viral illness. IgA vasculitis is the commonest childhood vasculitis, peaking between four and seven years and slightly more often in boys, typically following an upper-respiratory infection. Meningococcal disease is rare overall but remains the diagnosis that must never be missed in any febrile child with a rapidly progressive petechial rash, with the highest incidence in infants and adolescents. [1] [7]
The risk factors are best grouped by mechanism. For thrombocytopenia, a recent viral infection (especially Epstein-Barr virus, cytomegalovirus, or a simple respiratory virus) precedes ITP, and immunisation can rarely trigger it. For vasculitis, a preceding upper-respiratory infection is the rule in IgA vasculitis. For sepsis-related purpura, asplenia, complement deficiency, young infancy and crowding raise the risk of invasive meningococcal and pneumococcal disease. For purpura fulminans in the neonate and young infant, inherited protein C or protein S deficiency is the classic cause, while older children may develop an acquired form with anti-protein S antibodies after a varicella or streptococcal infection. [10] [8]
In Australia and Aotearoa New Zealand, the meningococcal B and W and Y strains co-circulate, and although vaccination has reduced the burden of serogroup C disease, meningococcaemia remains the emergency that frames every non-blanching-rash pathway. Aboriginal, Torres Strait Islander, Maori and Pasifika children, and children in remote and crowded households, carry higher rates of invasive bacterial disease and of post-streptococcal and rheumatological vasculitis, so a low threshold for antibiotics and blood cultures is part of culturally safe, equitable care. Refugee and migrant children may present with previously undiagnosed chronic thrombocytopenia or with bruising from inherited or nutritional causes, and an interpreter-mediated history is part of the workup. [8]
Pathophysiology
Why does blood appear outside the vessel? There are three broad mechanisms, and each maps onto a family of diagnoses. The first is a reduction in platelet number or function, so that everyday capillary shear leaks blood into the skin — this is the ITP, leukaemia and aplastic pathway. The second is damage to the vessel wall, either by inflammation in a vasculitis or by direct endothelial infection and injury in sepsis. The third is a failure of coagulation, so that bleeding is not arrested — this is the disseminated intravascular coagulation and inherited deficiency pathway. Most non-blanching rashes sit in one of these three buckets. [9] [1]
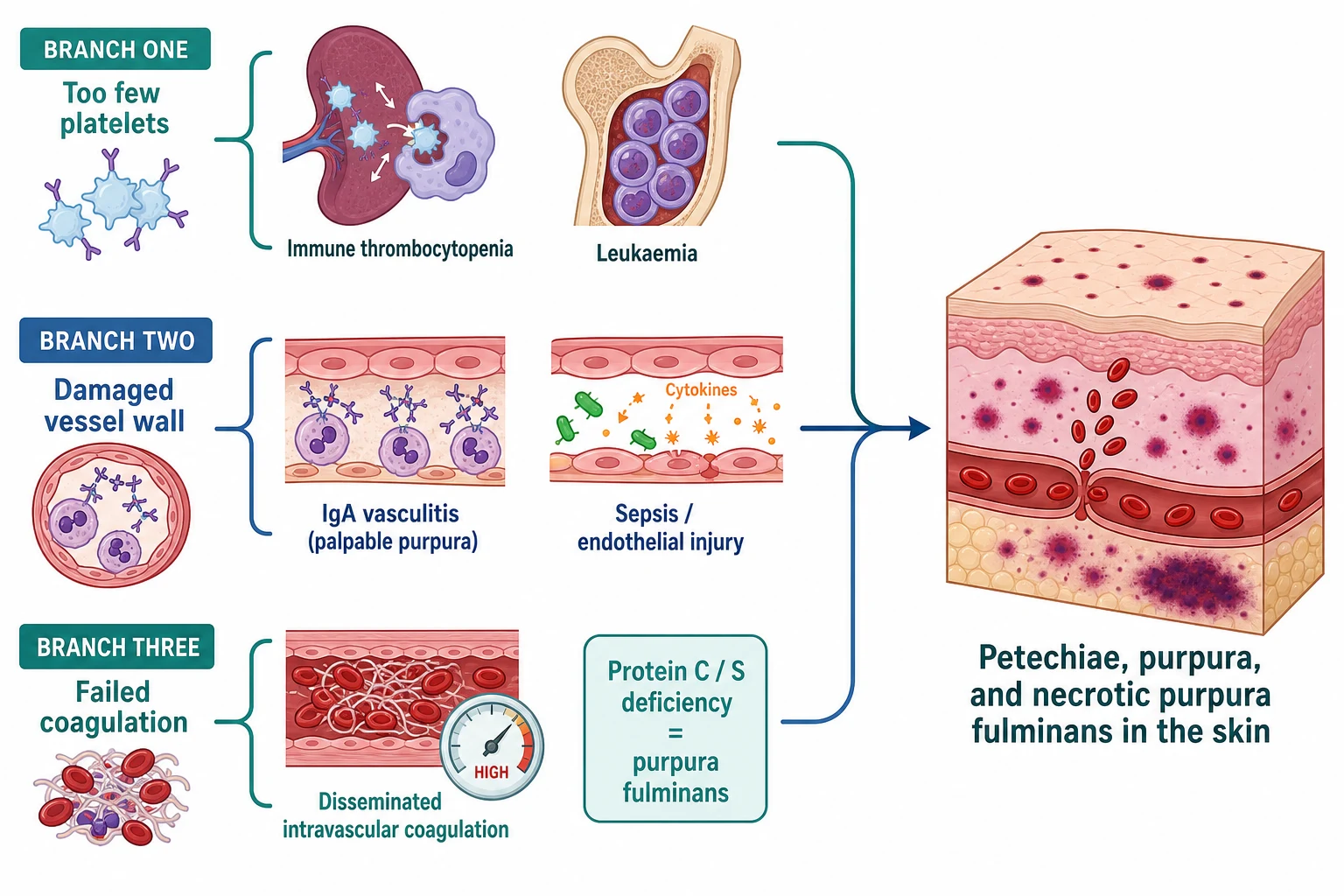
In immune thrombocytopenia, autoantibodies — usually IgG, often against glycoprotein IIb/IIIa — coat the platelets, which are then cleared by splenic macrophages. The platelet count falls abruptly, but the marrow responds normally with large, young platelets, which is why the bleeding is often mild relative to the count and why the peripheral film shows isolated thrombocytopenia with normal red and white cells. The definition deliberately excludes secondary causes, so a child with anaemia, neutropenia or blasts does not have primary ITP. [3] [4]
In IgA vasculitis, IgA-dominant immune complexes deposit in the small-vessel walls of the skin, gut and kidneys, activating complement and recruiting neutrophils. The vessel wall becomes inflamed, leaky and palpable, producing the classic dependent purpura, while identical deposition in the renal mesangium causes the IgA nephritis that can surface weeks later as haematuria, proteinuria and hypertension. In meningococcal disease and other sepsis, circulating endotoxin and cytokines damage the endothelium directly, and in severe cases trigger disseminated intravascular coagulation: microthrombi form, consume platelets and clotting factors, and the skin infarcts — the pathological basis of purpura fulminans. [5] [9]
Clinical Presentation
The presentation is read through the sick-versus-well lens, and the two ends look completely different. The sick child with sepsis or purpura fulminans has fever, irritability or drowsiness, tachycardia, cold mottled peripheries, a prolonged capillary refill and often hypotension, and the rash appears and spreads over minutes to hours — petechiae first, then dark purpuric patches that may become confluent, dusky and necrotic, sometimes in map-like or geographic shapes. This child is in the emergency pathway now. [8]
The well child with ITP looks entirely different — afebrile, active and cheerful, with sudden bruising and a petechial rash that may be dramatic but sits on an otherwise normal child. There may be mucosal bleeding, epistaxis or menorrhagia, but the examination apart from the rash is normal: no hepatosplenomegaly, no lymphadenopathy, no dysmorphism. The bleeding severity in ITP tracks the count loosely rather than tightly, and serious bleeding such as an intracranial haemorrhage is uncommon. [1] [2]
[3] [4]The IgA vasculitis presentation is distinctive. A young child, often after a viral upper-respiratory illness, develops palpable purpura on the lower limbs and buttocks — the lesions are raised, do not blanch, and appear in crops. Alongside the rash there may be colicky abdominal pain (sometimes with bleeding, intussusception or, rarely, perforation), arthritis or arthralgia of the knees and ankles, and renal involvement shown by haematuria, proteinuria or hypertension. The tetrad is palpable purpura, abdominal pain, arthritis and renal involvement, but not every child has all four at once. [7] [5]
The disseminated intravascular coagulation and purpura fulminans presentation overlaps with sepsis: a sick child with oozing from puncture sites, a falling platelet count, prolonged clotting and the necrotic purpura described above. Neonatal purpura fulminans from protein C or S deficiency appears in the first days of life with widespread necrotic lesions and a catastrophic coagulopathy, while the acquired, post-infectious form with anti-protein S antibodies presents in older infants and children after varicella or streptococcal infection. [10] [9]
Differential Diagnosis
The differential is best built around the sick-versus-well split, because the dangerous diagnoses live on the sick side. In the febrile, unwell child, meningococcaemia is the must-not-miss diagnosis, but the same pathway includes pneumococcal and other bacterial sepsis, viral haemorrhagic fevers, and any cause of septic shock with disseminated intravascular coagulation. Purpura fulminans from inherited protein C or S deficiency or from acquired anti-protein S antibodies sits here too. A rapidly enlarging purpuric lesion in a febrile child is sepsis until the cultures prove otherwise. [8] [10]
In the well child, the differential of isolated thrombocytopenia is led by ITP, but the clinician must actively exclude leukaemia (pancytopenia, blasts, hepatosplenomegaly), aplastic anaemia, secondary ITP from autoimmune disease or immunodeficiency, and inherited platelet disorders. A thorough history and examination for lymphadenopathy, hepatosplenomegaly, pallor and warts, together with the film, separate these. The update on paediatric ITP emphasises distinguishing primary ITP from inherited platelet disorders and primary immunodeficiencies, because mislabelling a marrow disorder as ITP delays the right treatment. [4] [1]
[1] [4]The vasculitic and thrombotic differentials round out the well-to-moderately-unwell group. IgA vasculitis is the commonest, but consider other small-vessel vasculitides in the older child, and in the child with thrombocytopenia, anaemia and acute kidney injury think of haemolytic uraemic syndrome — a thrombotic microangiopathy with the triad of microangiopathic haemolytic anaemia, thrombocytopenia and acute kidney injury, usually after a bloody diarrhoeal illness. Drug-induced thrombocytopenia and Henoch-Schönlein mimics such as atypical infections complete the list. [11] [6]
Finally, safeguarding belongs in every differential of bruising. Bruises in non-mobile infants, bruises on the torso, ear, neck or face, patterned bruises, and bruises whose history does not fit the developmental stage all raise the question of non-accidental injury. The validated bruising literature shows that the distribution and the developmental stage of the child discriminate abuse from accidental injury, so a bruise in the wrong place on the wrong child is a referral, not a reassurance. [12]
Clinical & Bedside Assessment
Begin at the bedside with the airway, breathing and circulation of the sick child, because a febrile child with purpura and shock can die while the history is being taken. Assess the capillary refill, peripheral temperature, heart rate, blood pressure and conscious level, and calculate a paediatric early-warning or sepsis score. If the child is shocked, give oxygen, establish intravenous or intraosseous access, take blood cultures, and give a broad-spectrum parenteral antibiotic and a fluid bolus — do not wait for the rash to be classified. [8]
Confirm the rash is genuinely non-blanching with the glass test. Press a clear glass or a transparent tumbler firmly over a lesion and look: petechiae and purpura remain visible through the glass, whereas erythematous inflammatory lesions fade. Then describe the rash precisely — petechial, purpuric or ecchymotic, flat or palpable, the distribution (dependent, generalised, face and upper chest), the colour (fresh red, dark purple, dusky grey-black necrotic), and whether it is evolving while you watch. Photograph the rash, because progression is diagnostic and the record supports the clinical and safeguarding assessment. [8] [12]
Take a focused history aimed at the tempo, the prodrome and the bleeding. Ask when the rash began and how fast it is spreading, about fever and systemic upset, recent viral illness or immunisation, preceding diarrhoea (pointing to haemolytic uraemic syndrome), joint and abdominal symptoms (pointing to IgA vasculitis), and bleeding from gums, nose, gut or urine. Ask about medications that can cause thrombocytopenia, and — without judgement — take a careful developmental and social history, because bruising in a non-mobile infant or an inconsistent injury story is a safeguarding signal. [7] [12]
Examine the whole child for the clues that shift the differential. Look for pallor, lymphadenopathy and hepatosplenomegaly (pointing to leukaemia), hypertension and oedema (pointing to nephritis), joint swelling and abdominal tenderness (IgA vasculitis), and the distribution and pattern of the bruises. Measure the blood pressure in every child with a vasculitic or thrombocytopenic rash, and examine the joints, abdomen and skin in full. The examination is what separates the well child with ITP from the unwell child with sepsis or marrow disease. [4] [6]
Investigations
The investigations split into the emergency panel for the sick child and the diagnostic panel for the well child, and the two must not be confused. In the febrile, toxic child with purpura, send blood cultures, a full blood count and film, coagulation studies, C-reactive protein, electrolytes, lactate and blood gas, and a meningococcal polymerase-chain-reaction where available, and treat empirically before the results return. The coagulation studies and falling platelet and fibrinogen levels identify disseminated intravascular coagulation, scored with the ISTH criteria. [8] [9]
In the well child with suspected ITP, the essential test is a full blood count and a blood film. The diagnosis of ITP is one of isolated thrombocytopenia with otherwise normal lines and a normal film, so the film is reviewed to exclude blasts and other abnormalities. Routine bone-marrow biopsy is not required in a typical presentation, but it is indicated if there are atypical features — cytopenias in other lines, hepatosplenomegaly, or an abnormal film — because these point away from ITP toward leukaemia or aplasia. [3] [2]
ISTH overt disseminated intravascular coagulation score (5 points possible)
In suspected IgA vasculitis, the diagnosis is clinical, built from the palpable purpura and the accompanying features; the EULAR/PRINTO/PRES criteria require palpable purpura or petechiae plus at least one of abdominal pain, arthritis, renal involvement or IgA deposition on biopsy. Check the urinalysis and blood pressure at presentation and regularly for six to twelve months, because nephritis can declare late, and send a full blood count, coagulation, urea, electrolytes, creatinine and albumin to assess gut and renal involvement. Renal biopsy is reserved for persistent, heavy or atypical nephritis. [5] [6]
Where the picture fits haemolytic uraemic syndrome, send a full blood count and film (for schistocytes), coagulation, lactate dehydrogenase, haptoglobin, creatinine and urinalysis, and a stool sample for shiga-toxin or the organism, confirming the triad of microangiopathic haemolytic anaemia, thrombocytopenia and acute kidney injury. In the safeguarding assessment of bruising, the investigations are those of a child-protection workup — a clotting screen to explain bruising medically where relevant, and skeletal survey and further imaging as guided by the child-protection team — not a search for a benign rash. [11] [12]
Management — Resuscitation
Resuscitation belongs to the sick, purpuric child, and the principle is that suspected meningococcal or septic purpura is treated before it is confirmed. Within the first hour, give high-flow oxygen, establish intravenous or intraosseous access, take blood cultures, give a broad-spectrum parenteral antibiotic such as ceftriaxone, and administer a 10 to 20 mL per kilogram crystalloid bolus for shock, repeated with reassessment and escalation to intensive care for refractory shock. Antibiotic delay costs lives, so the threshold is deliberately low in any febrile child with a spreading petechial rash and signs of sepsis. [8]
In purpura fulminans and disseminated intravascular coagulation, resuscitation runs alongside correction of the coagulopathy and the underlying cause. Give supportive care in a paediatric intensive-care setting, treat the sepsis or the inherited deficiency, and use fresh-frozen plasma, platelets and, in selected inherited cases, protein C concentrate guided by haematology. Necrotic skin lesions need surgical and burn-unit input for debridement and reconstruction once the child is stable, because the skin loss behaves like a major burn. [9] [10]
The well child with ITP rarely needs resuscitation, but life-threatening bleeding — above all an intracranial haemorrhage — is the emergency that justifies treatment. Any child with ITP and suspected serious bleeding receives urgent intravenous immunoglobulin, high-dose corticosteroids and a platelet transfusion, with haematology and intensive-care involvement, because the immediate aim is to raise the platelet count and stop the bleed. This is the one situation in ITP where speed dominates. [1] [2]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway that branches at the sick-versus-well fork, and the art is to match the intensity of treatment to the risk of bleeding while never losing sight of the emergencies. [1] [9]
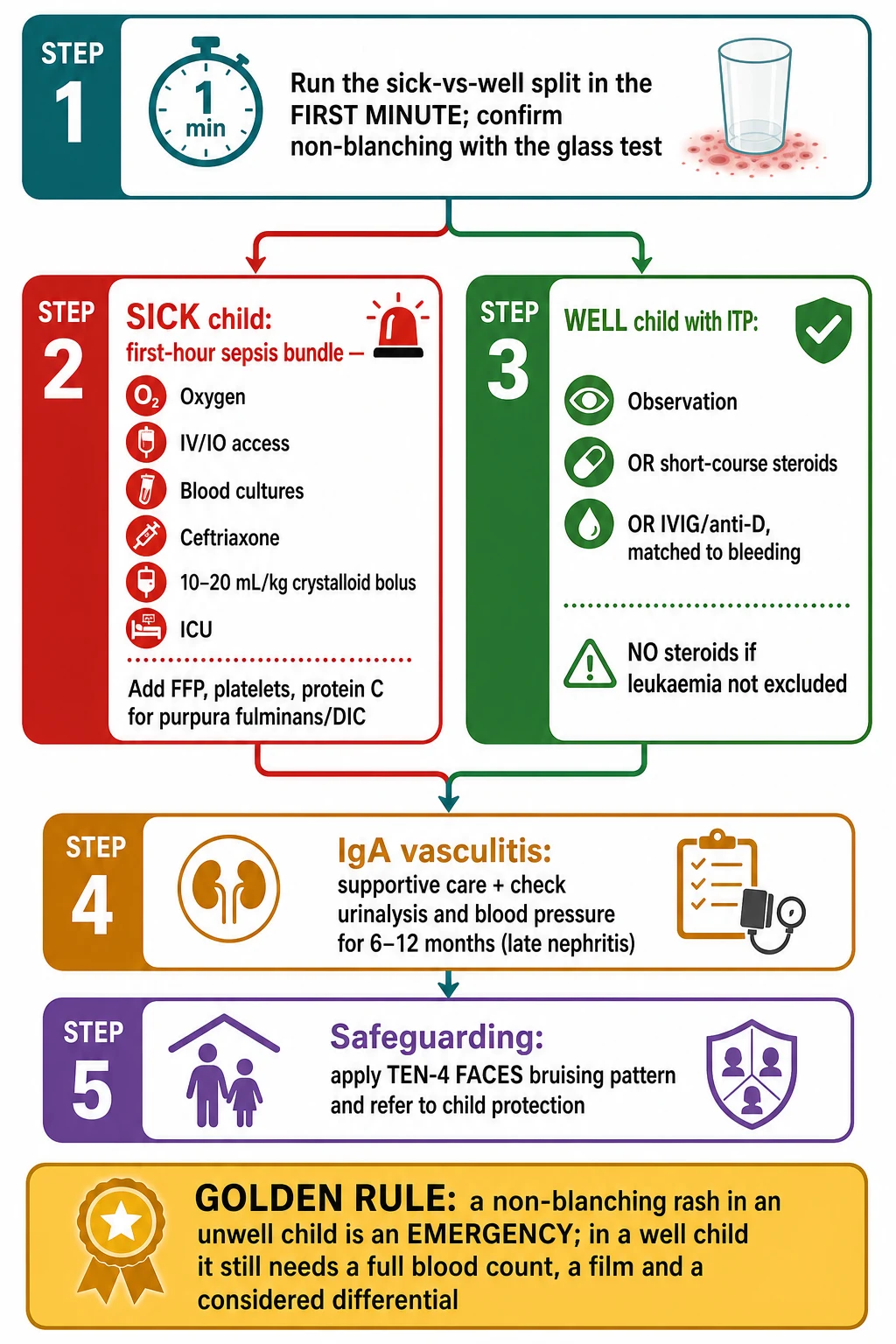
For immune thrombocytopenia, the ASH 2019 guidelines and the international consensus report frame a risk-based approach. Most children need only observation and safety-netting when the count is acceptable and there is no significant bleeding. When treatment is indicated — for a very low count, active bleeding, or high-risk activities — first-line options are short-course corticosteroids, intravenous immunoglobulin, or anti-D immunoglobulin in Rh-positive, non-splenectomised children. Second-line and refractory disease is managed with haematology, and splenectomy is now rare in children. Crucially, steroids are avoided if leukaemia has not been excluded, because they can transiently mask a marrow diagnosis. [2] [1]
The stepwise ITP pathway
Confirm isolated thrombocytopenia (platelets under 100 × 10⁹ per litre) with a normal film and exclude secondary causes and leukaemia.
Assess the bleeding severity, not just the count — most children with dry purpura need observation and safety-netting alone.
If treatment is indicated, give a short course of corticosteroids, intravenous immunoglobulin or anti-D (Rh-positive, non-splenectomised) as first-line therapy.
Avoid steroids before the diagnosis is secure if any atypical feature is present, because they can mask leukaemia.
For life-threatening bleeding, give urgent intravenous immunoglobulin, high-dose corticosteroids and a platelet transfusion, with haematology and intensive care.
Educate the family on bleeding precautions, avoid intramuscular injections and contact sports when the count is low, and safety-net for head injury, excessive bleeding and petechial spread.
Arrange haematology follow-up and refractory-disease pathways, with splenectomy now rare in children.
For IgA vasculitis, management is predominantly supportive — analgesia, hydration, rest, and monitoring of the abdomen, joints, blood pressure and urinalysis. The SHARE initiative recommends treating severe gastrointestinal disease, severe nephritis, or heavy proteinuria with corticosteroids and, for severe renal involvement, immunosuppression under specialist guidance, while recognising that steroids do not reliably prevent nephritis. The long-term priority is the kidney: monitor the blood pressure and urinalysis regularly for six to twelve months, because IgA nephritis can appear late and determines the prognosis. [6] [7]
For haemolytic uraemic syndrome, management is supportive renal care — fluid and electrolyte management, blood-pressure control, dialysis where needed, and transfusion for symptomatic anaemia — with plasma exchange reserved for atypical, complement-mediated disease. Antibiotics and antimotility agents are generally avoided in shiga-toxin-associated disease. For purpura fulminans, treat the cause (sepsis, inherited or acquired protein C or S deficiency), correct the coagulopathy, and involve surgery and the burn unit for necrotic skin. [11] [10]
Specific Subtypes & Scenarios
A febrile toddler with a spreading petechial rash and shock. This is meningococcal septicaemia until proven otherwise. Within the first hour give oxygen, access, blood cultures, a broad-spectrum parenteral antibiotic such as ceftriaxone, and a fluid bolus, and escalate to intensive care. Treat purpura fulminans and disseminated intravascular coagulation with haematology-guided blood-product support. Notify public health for contact prophylaxis. The diagnosis is clinical and the antibiotic comes first. [8]
A well four-year-old with sudden bruising and a platelet count of 8 × 10⁹ per litre. This is classic acute ITP if the film and the other lines are normal and the child is well. With only dry purpura, observation and safety-netting may suffice; with wet purpura or a very low count, give a short course of corticosteroids or intravenous immunoglobulin. Exclude leukaemia first — any pallor, lymphadenopathy, organomegaly, anaemia or blasts takes this out of the ITP pathway and into urgent haematology. Counsel the family on bleeding precautions and head-injury safety-netting. [1] [2]
A six-year-old with palpable purple spots on the legs and buttocks, ankle swelling and colicky abdominal pain. This is IgA vasculitis (Henoch-Schönlein purpura), confirmed by the palpable dependent purpura plus abdominal pain or arthritis. Check the blood pressure and the urinalysis now, send a full blood count, renal function and albumin, and arrange regular urinalysis and blood-pressure monitoring for six to twelve months. Give supportive care, treat severe gut or renal involvement with corticosteroids under guidance, and warn the family about intussusception and late nephritis. [5] [6]
A four-month-old, not yet mobile, with a bruise on the arm. Any bruise in a non-mobile infant is abnormal and warrants a safeguarding assessment. Apply the TEN-4 FACES pattern — bruising on the Torso, Ear or Neck, any bruise in an infant four months or younger, and Facial bruising (Frenum, Angle of the mouth, Cheek, Eyelid, Subconjunctiva) — and escalate to a child-protection referral. Take a careful, non-judgemental history, examine fully for other injuries, and involve the child-protection team for the workup; bruising in a pre-mobile infant is almost never accidental. [12]
A neonate with widespread necrotic purpura in the first days of life. This is neonatal purpura fulminans from severe inherited protein C or protein S deficiency until proven otherwise. It is a haematological emergency: involve haematology and neonatal intensive care urgently, correct the coagulopathy with fresh-frozen plasma and, where confirmed, protein C concentrate, investigate the inherited deficiency, and counsel the family. The acquired, post-infectious form with anti-protein S antibodies presents later, after varicella or streptococcal infection. [10]
A three-year-old, two weeks after bloody diarrhoea, with pallor, oliguria and petechiae. This is the haemolytic uraemic syndrome — the triad of microangiopathic haemolytic anaemia, thrombocytopenia and acute kidney injury. The film shows schistocytes, and management is supportive renal care with fluid and electrolyte control, blood-pressure management, dialysis where needed, and transfusion for symptomatic anaemia; avoid antibiotics and antimotility agents in the shiga-toxin-associated form. [11]
Complications & Pitfalls
The gravest complication is death from delayed sepsis treatment. A febrile child with a spreading petechial rash who is managed as a viral illness, or whose antibiotic is withheld pending cultures, is the classic preventable death in paediatrics. The defence is a low threshold for the sepsis pathway and an antibiotic within the first hour whenever sepsis is plausible. The rash is a warning sign, not a diagnostic formality. [8]
The cardinal pitfall in the well child is labelling leukaemia as ITP. A child given steroids for presumed ITP who actually has leukaemia has the marrow diagnosis masked and the definitive treatment delayed. The protection is the film and the lines: isolated thrombocytopenia with a clean film and normal haemoglobin, white cells and neutrophils is ITP; anything else is not, and steroids wait until haematology has secured the diagnosis. [4] [1]
A second pitfall is underestimating IgA vasculitis nephritis. The rash and the abdominal pain settle, the family is reassured, and the late nephritis is missed because no one monitored the urinalysis and blood pressure. The protection is scheduled urinalysis and blood-pressure checks for six to twelve months, because renal involvement can appear weeks after the rash and is what determines the long-term outcome. [6] [7]
A third pitfall is over-treating ITP and ignoring the bleeding risk. Treating a well child with a moderately low count and no bleeding exposes them to steroid and immunoglobulin side effects without clear benefit, while failing to safety-net the family for head injury and serious bleeding leaves the rare but catastrophic intracranial haemorrhage unprepared for. The ASH guidelines frame this as a risk-based decision — match the treatment to the bleeding, not just the number. [2]
A fourth pitfall is missing safeguarding. Attributing bruises in a non-mobile infant to a fall that the child's development cannot produce, or failing to recognise the TEN-4 FACES distribution, leaves a child at risk of further harm. The protection is to apply the bruising pattern to every bruise, take a developmental history, and refer to the child-protection team when the pattern or the story does not fit. [12]
A fifth pitfall is confusing haemolytic uraemic syndrome with ITP or sepsis. The child with pallor, oliguria, thrombocytopenia and a diarrhoeal prodrome has a thrombotic microangiopathy, not a simple low platelet count, and the management is renal support rather than immunoglobulin. The schistocytes on the film and the acute kidney injury make the diagnosis. [11]
Prognosis & Disposition
Disposition follows the sick-versus-well fork. The sick, septic or purpura-fulminans child is admitted to paediatric intensive care or retrieved to a tertiary centre, with ongoing resuscitation, blood-product support and, where needed, surgical and burn-unit care. The mortality of meningococcal septicaemia and purpura fulminans is driven by the speed of antibiotic and resuscitation, and survivors may carry skin, limb and neurological sequelae. [8] [10]
The well child with ITP is managed as an outpatient when the count is acceptable and there is no significant bleeding, with clear safety-netting for head injury, excessive bleeding and increasing petechiae, and avoidance of contact sports and intramuscular injections when the count is low. Most acute childhood ITP resolves within months, and chronic disease (over twelve months) is managed with haematology. Serious bleeding such as intracranial haemorrhage is uncommon but is the event the safety-netting exists to catch. [1] [2]
The IgA vasculitis child is usually managed as an outpatient with supportive care and scheduled renal monitoring, admitted for severe abdominal pain, intussusception, severe nephritis or hypertension. The long-term prognosis is driven by the kidney: most children recover fully, but persistent nephritis, heavy proteinuria and hypertension mark those who need long-term nephrology follow-up. [6] [7]
At discharge, complete the safety-netting in writing — return immediately for fever with a spreading rash, increasing bruising or petechiae, heavy bleeding, headache or altered consciousness, reduced urine output, or abdominal pain — and arrange the follow-up the diagnosis demands: haematology for refractory or chronic ITP, nephrology for IgA vasculitis nephritis, and the child-protection team where safeguarding concerns have been raised. [8] [12]
Special Populations
Infants under four months need particular care on two fronts. Neonatal purpura fulminans from protein C or S deficiency is a haematological emergency presenting in the first days of life, and any bruise in a non-mobile infant is a safeguarding concern until assessed. The threshold to investigate, involve haematology and child protection, and admit is deliberately low. [10] [12]
Immunocompromised children — those post-transplant, on chemotherapy, or with primary immunodeficiency — can present with thrombocytopenia, marrow failure or opportunistic infection causing purpura, and warrant a high index of suspicion and early haematology and infectious-disease input. Secondary ITP and drug-induced thrombocytopenia are more common here, and the differential is wider. [4]
Indigenous, refugee and migrant children may carry a higher burden of invasive bacterial disease, post-infectious vasculitis and undiagnosed chronic conditions, and may have delayed presentations. Culturally safe, interpreter-mediated assessment, a low threshold for antibiotics and blood cultures, and attention to social determinants and safeguarding are part of equitable care. [8]
Children in rural and remote settings depend on pre-hospital recognition and retrieval. The non-blanching rash in an unwell child is a reason to start the sepsis pathway and mobilise retrieval immediately, with telehealth support for the referring clinician while the team arrives. The first antibiotic and the first bolus are given locally, not deferred to the tertiary centre. [8]
Children with suspected non-accidental injury are managed through the child-protection pathway, with a multi-disciplinary assessment, a clear and contemporaneous record, and the involvement of the safeguarding team. The clinician's role is to recognise the pattern, document it, and refer — not to adjudicate — and the TEN-4 FACES pattern is the tool that turns a bruise into a referral. [12]
Evidence, Guidelines & Regional Differences
The sepsis and emergency evidence anchors the sick side of the pathway. The clinical review of meningococcal disease in children sets out the rapid progression from petechiae to purpuric fulminans and the mortality cost of antibiotic delay, which underpins the first-hour antibiotic principle that structures every paediatric sepsis guideline. The ISTH disseminated intravascular coagulation scoring paper gives the five-component score — platelets, fibrin markers, prothrombin time and fibrinogen — that quantifies the coagulopathy driving purpura fulminans. [8] [9]
ISTH overt-DIC score (Taylor et al.)
Population: An international consensus approach to defining, diagnosing and scoring overt disseminated intravascular coagulation from clinical and laboratory criteria.
Key finding
A simple five-component score — platelet count, fibrin-related markers, prothrombin time and fibrinogen — identifies overt disseminated intravascular coagulation and stratifies severity, providing a reproducible bedside and laboratory tool.
Practice change
The ISTH score is the standard approach to diagnosing and grading disseminated intravascular coagulation in the sick purpuric child, guiding blood-product support alongside treatment of the cause.
The ITP evidence is consolidated in the international consensus report and the ASH 2019 guidelines. The working-group standardisation paper fixed the terminology and the definition — a platelet count under 100 × 10⁹ per litre, isolated thrombocytopenia, and the distinction between newly diagnosed, persistent and chronic disease — and the ASH guidelines set out the risk-based management from observation through first-line therapy. The paediatric update that differentiates primary ITP from inherited platelet disorders and primary immunodeficiencies reinforces the need to exclude secondary causes before labelling a child. [3] [2]
The vasculitis evidence defines IgA vasculitis and its care. The EULAR/PRINTO/PRES Ankara 2008 criteria require palpable purpura plus at least one of abdominal pain, arthritis, renal involvement or IgA deposition, and the SHARE initiative sets the diagnosis and treatment recommendations, including the role of corticosteroids for severe gastrointestinal and renal disease and the centrality of renal monitoring. The evidence review frames IgA vasculitis as a predominantly supportive, kidney-focused illness. [5] [6]
EULAR/PRINTO/PRES IgA vasculitis criteria (Ozen et al.)
Population: A large multinational cohort of children with vasculitis, used to derive and validate classification criteria for Henoch-Schönlein purpura and other childhood vasculitides.
Key finding
Henoch-Schönlein purpura (IgA vasculitis) is classified by the presence of palpable purpura or petechiae (mandatory) plus at least one of abdominal pain, arthritis or arthralgia, renal involvement, or histopathology showing IgA deposition.
Practice change
These criteria are the standard for classifying childhood IgA vasculitis in clinical practice, trials and exams, anchoring the diagnosis on palpable dependent purpura with the accompanying tetrad.
The safeguarding evidence underpins the bruising assessment. The study of bruising characteristics discriminating physical child abuse from accidental trauma established that bruises in non-mobile infants and bruises on the torso, ear and neck are uncommon in accidental injury, forming the basis of the TEN-4 FACES bruising clinical decision rule that now guides child-protection referral. The regional policy structure is consistent: NICE sepsis guidance (NG51) and the Royal Children's Hospital Melbourne fever-and-petechiae guideline set the emergency pathway in the UK and ANZ, with child-protection frameworks sitting alongside them. [12] [8]
The controversies are real: the exact platelet threshold for treating ITP versus observing, the role of rituximab and thrombopoietin receptor agonists in chronic paediatric ITP, the optimal use of corticosteroids in IgA vasculitis nephritis, and the timing of antibiotics when sepsis is possible but unproven. The defence against each is the same — the sick-versus-well split, the glass test, the full blood count and film, and a low threshold for the sepsis pathway and for safeguarding referral. [2] [6]
Exam Pearls
- The first split is sick versus well: a febrile toxic child with a spreading non-blanching rash is meningococcal sepsis or purpura fulminans; a well afebrile child with isolated petechiae is most likely ITP. [8]
- The glass test confirms a non-blanching rash — petechiae and purpura do not fade under a clear tumbler because the blood is extravascular. [8]
- ITP is isolated thrombocytopenia under 100 × 10⁹ per litre with a normal film; pancytopenia, blasts, organomegaly or anaemia is leukaemia, not ITP, and steroids wait for a secure diagnosis. [3] [4]
- IgA vasculitis is the commonest childhood vasculitis: palpable purpura on the lower limbs and buttocks plus abdominal pain, arthritis or renal involvement; monitor the urinalysis and blood pressure for six to twelve months. [5] [6]
- Purpura fulminans and disseminated intravascular coagulation cause necrotic map-like purpura with shock; score with the ISTH criteria and treat the cause with blood-product support. [9] [10]
- Haemolytic uraemic syndrome is the triad of microangiopathic haemolytic anaemia, thrombocytopenia and acute kidney injury with schistocytes, after bloody diarrhoea; treat with supportive renal care. [11]
- Safeguarding: the TEN-4 FACES pattern — bruising on the Torso, Ear or Neck, any bruise in an infant four months or younger, and facial bruising — warrants a child-protection referral. [12]
- Treat suspected meningococcal purpura with a ceftriaxone-class antibiotic within the first hour; do not wait for cultures in the septic child. [8]
References
- [1]Provan D; Arnold DM; Bussel JB; et al Updated international consensus report on the investigation and management of primary immune thrombocytopenia. Blood Adv, 2019.PMID 31770441
- [2]Neunert C; Terrell DR; Arnold DM; et al American Society of Hematology 2019 guidelines for immune thrombocytopenia. Blood Adv, 2019.PMID 31794604
- [3]Rodeghiero F; Stasi R; Gernsheimer T; et al Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood, 2009.PMID 19005182
- [4]Grace RF; Lambert MP; et al An update on pediatric ITP: differentiating primary ITP, IPD, and PID. Blood, 2022.PMID 34479363
- [5]Ozen S; Pistorio A; Iusan SM; et al EULAR/PRINTO/PRES criteria for Henoch-Schönlein purpura, childhood polyarteritis nodosa, childhood Wegener granulomatosis and childhood Takayasu arteritis: Ankara 2008. Part II: Final classification criteria. Ann Rheum Dis, 2010.PMID 20413568
- [6]Ozen S; Marks SD; Brogan P; et al European consensus-based recommendations for diagnosis and treatment of immunoglobulin A vasculitis-the SHARE initiative. Rheumatology (Oxford), 2019.PMID 30879080
- [7]Reamy BV; Servey JT; Williams PM Henoch-Schönlein Purpura (IgA Vasculitis): Rapid Evidence Review. Am Fam Physician, 2020.PMID 32803924
- [8]Sabra A; Benger J Meningococcal disease in children: a clinical review. Turk J Pediatr, 2011.PMID 22272447
- [9]Taylor FB Jr; Toh CH; Hoots WK; et al Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb Haemost, 2001.PMID 11816725
- [10]Theron A; Dautremay O; Boissier E; et al Idiopathic purpura fulminans associated with anti-protein S antibodies in children: a multicenter case series and systematic review. Blood Adv, 2022.PMID 34788405
- [11]Boyer O; Niaudet P Hemolytic-Uremic Syndrome in Children. Pediatr Clin North Am, 2022.PMID 36880929
- [12]Pierce MC; Kaczor K; Aldridge S; et al Bruising characteristics discriminating physical child abuse from accidental trauma. Pediatrics, 2010.PMID 19969620