Paeds · paediatric-dermatology
Psoriasis in children
Also known as Childhood psoriasis · Plaque psoriasis · Guttate psoriasis · Scalp psoriasis · Napkin psoriasis · Juvenile psoriatic arthritis
Fellowship topic on psoriasis in children: the plaque, guttate, scalp, nail, facial and napkin forms and their paediatric-specific presentations; the IL-23 and Th17 and IL-17 immune pathophysiology with HLA-Cw6 genetics, streptococcal and Koebner triggers; the differential from atopic and seborrhoeic dermatitis, tinea and pityriasis rosea; a clinical diagnosis with severity measured by body surface area, PASI and the Children's Dermatology Life Quality Index; stepwise treatment from emollients and potency-matched topical corticosteroid plus calcipotriol through narrowband UVB phototherapy to systemic methotrexate, cyclosporin and acitretin and the biologic agents etanercept, ustekinumab and the IL-17 and IL-23 inhibitors, grounded in the landmark paediatric etanercept trial and the recent biologics network meta-analysis; the obesity, metabolic, juvenile psoriatic arthritis and psychosocial comorbidities; and the ANZ, UK and North American guidance including the joint AAD-NPF paediatric psoriasis guideline.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The IL-23 / Th17 / IL-17 engine and its targets
Overview & Definition
Picture an eight-year-old brought in with thick, scaly patches on the elbows and scalp that have come and gone for a year, itchy and embarrassing at school. Or a twelve-year-old who, two weeks after a sore throat, breaks out in hundreds of small, teardrop spots over the trunk. Both are psoriasis — the most common immune-mediated skin disease of childhood after atopic dermatitis, and a condition whose visible burden can quietly shape a child's schooling, friendships and self-image. [2] [3]
Psoriasis is a chronic, relapsing, immune-mediated inflammatory skin disease in which a dysregulated IL-23 and Th17 and IL-17 immune response drives keratinocytes to proliferate excessively, producing the well-demarcated, scaly erythematous plaques that are its hallmark. It runs in families, reflects a strong polygenic susceptibility led by the HLA-Cw6 allele, and is triggered by streptococcal infection, skin trauma (the Koebner phenomenon), stress, obesity and certain drugs. In children it has its own patterns — more facial and scalp involvement, the distinctive guttate form after strep, and napkin-area disease in infants. [1] [2]
The clinician's task has three layers. The first is recognition — distinguishing psoriasis from atopic and seborrhoeic dermatitis, tinea and pityriasis rosea, and the rare but dangerous erythrodermic and pustular forms from severe eczema. The second is severity-matched treatment, climbing from emollients and topical therapy through phototherapy to systemic and biologic agents, while protecting the child from the harms of strong steroids, cumulative ultraviolet light and immunosuppression. The third is the whole-child layer — screening for obesity, metabolic risk, juvenile psoriatic arthritis and the psychosocial burden, because psoriasis in a child is a skin disease whose consequences reach far beyond the skin. [1] [11]
Classification
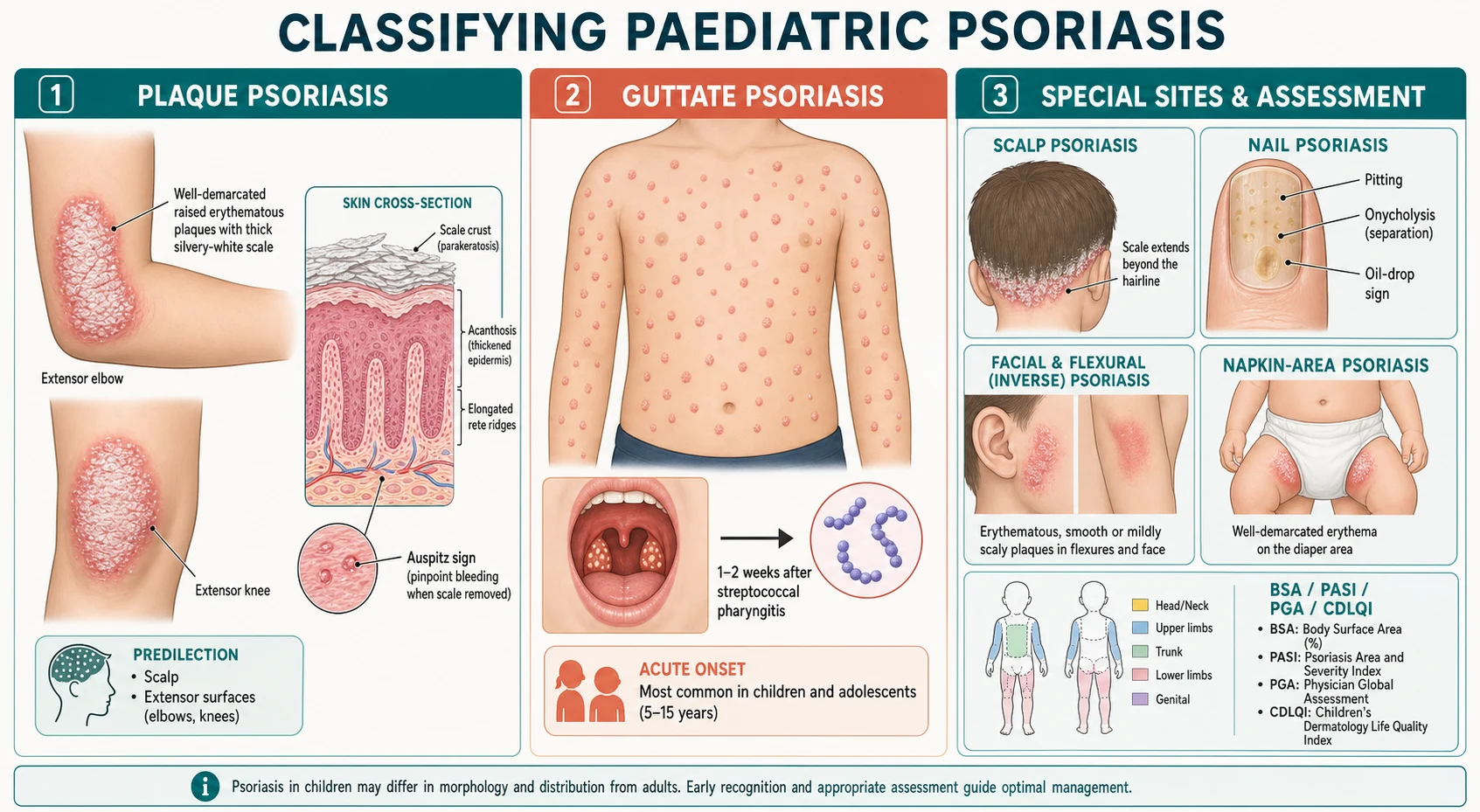
Think of paediatric psoriasis by the shape of its lesions and where it sits, because each pattern carries its own trigger, prognosis and treatment emphasis. Chronic plaque psoriasis is the commonest form in children, as in adults: sharply demarcated, raised, erythematous plaques with a thick silvery-white scale, favouring the extensor elbows and knees, the scalp and the lumbosacral area. Removing the scale reveals the Auspitz sign — tiny bleeding points from the dilated capillaries in the elongated dermal papillae — and plaques appear in lines of scratching or injury, the Koebner phenomenon. It runs a chronic, relapsing course and often carries a family history. [2] [3]
Guttate psoriasis is the acute paediatric pattern every examiner wants named. An abrupt eruption of small, round or teardrop-shaped, salmon-pink papules with fine scale, scattered symmetrically over the trunk and proximal limbs, appears one to two weeks after group A streptococcal pharyngitis (and occasionally perianal strep). It is most common in children and young adults, it is often the first presentation of psoriasis, and unlike chronic plaque disease it frequently remits spontaneously over weeks to months, though it can seed chronic plaque psoriasis later. A throat swab and antistreptolysin-O titre help confirm the trigger. [7] [3]
The remaining paediatric patterns are defined by site. Scalp psoriasis is a frequent first or only site, with thick scale that extends beyond the hairline. Nail psoriasis shows pitting, onycholysis, the oil-drop or salmon-patch discolouration and subungual hyperkeratosis, and is easily missed. Facial involvement is commoner in children than adults and is easily mistaken for seborrhoeic or atopic dermatitis. Flexural or inverse psoriasis affects the axillae, groin and genitalia with less scale. Napkin (diaper-area) psoriasis in infants is a well-demarcated, glossy erythema in the nappy area that often spares the folds and may progress to generalised plaque disease. [2] [3]
Two rare but serious forms must be recognised as emergencies. Generalised pustular psoriasis presents with widespread sterile pustules on a background of fiery erythema, with fever, malaise and skin pain, and erythrodermic psoriasis covers most of the body surface in erythema with scaling, shedding and temperature and fluid dysregulation. Both are uncommon in children but need admission, supportive care and urgent specialist therapy. [1] [3]
Epidemiology & Risk Factors
Psoriasis affects about one per cent of children and adolescents, with prevalence rising through childhood to peak in late adolescence; the global burden analysis confirms a substantial and consistent worldwide prevalence that has changed little over decades. Onset clusters in two peaks in adults, but childhood psoriasis concentrates in late childhood and adolescence, and early-onset disease (before about forty years) is strongly associated with the HLA-Cw6 allele and a positive family history. Around thirty to fifty per cent of children with psoriasis have a first-degree relative affected, and concordance is much higher in monozygotic than dizygotic twins. [4] [6] [5]
The principal trigger is streptococcal infection. Group A streptococcal pharyngitis precipitates guttate psoriasis in genetically susceptible children, and perianal streptococcal infection can do the same. Skin trauma produces new plaques along the line of injury — the Koebner phenomenon — which is why plaques appear at sites of scratching, abrasion, surgical scars or sunburn. Stress, obesity and certain drugs (lithium, beta-blockers, antimalarials, non-steroidal anti-inflammatories, and systemic corticosteroid withdrawal) are recognised triggers or exacerbators, and infections such as human immunodeficiency virus can unmask disease. [2] [7]
Obesity is the comorbidity that both reflects and drives paediatric psoriasis. Children with psoriasis are more likely to be overweight or obese than their peers, obesity worsens severity and treatment response, and the excess weight is part of a cluster of metabolic and cardiovascular risk markers — including dyslipidaemia, hypertension and insulin resistance — that begin in childhood. This is why a comprehensive paediatric psoriasis assessment includes weight, body mass index, blood pressure and, in severe disease, lipids and glucose. [11] [4]
In Australia and Aotearoa New Zealand, psoriasis care for children is delivered through a mix of public hospital paediatric dermatology, private dermatology and telehealth, with marked inequity of access for rural, remote and disadvantaged families. Specialist paediatric dermatology services concentrate in major centres, so a child in a remote community may wait many months to see a dermatologist and to access phototherapy or biologics. The Therapeutic Guidelines and trans-Tasman specialist practice guide topical, phototherapy and systemic therapy, with public funding pathways (such as the Pharmaceutical Benefits Scheme in Australia) governing access to the more costly biologic agents. Culturally safe, equitable access to specialist care is part of the management, not an afterthought. [1] [2]
Pathophysiology
The engine of psoriasis is a dysregulated innate and adaptive immune response in which IL-23 drives Th17 T-cells to release IL-17 and IL-22, and these cytokines act on keratinocytes to drive excessive proliferation and abnormal differentiation. Dendritic cells in the skin release IL-23 and tumour necrosis factor alpha; Th17 cells amplify the loop; and the keratinocyte response — hyperproliferation, retention of nuclei in the stratum corneum (parakeratosis), and recruitment of neutrophils — produces the visible plaque. This IL-23 and Th17 and IL-17 axis is the reason the modern biologics are so effective, because each one interrupts the loop at a defined point. [2] [1]
Genetics sets the stage. Psoriasis is polygenic, and the strongest single association is the HLA-Cw6 allele within the PSORS1 locus on chromosome 6, which is tightly linked to early-onset disease and to guttate psoriasis after strep. A positive family history is common, and the heritability is substantial, but expression depends on the triggers — infection, trauma, stress, drugs and obesity — that ignite the immune loop in a susceptible child. [2] [3]
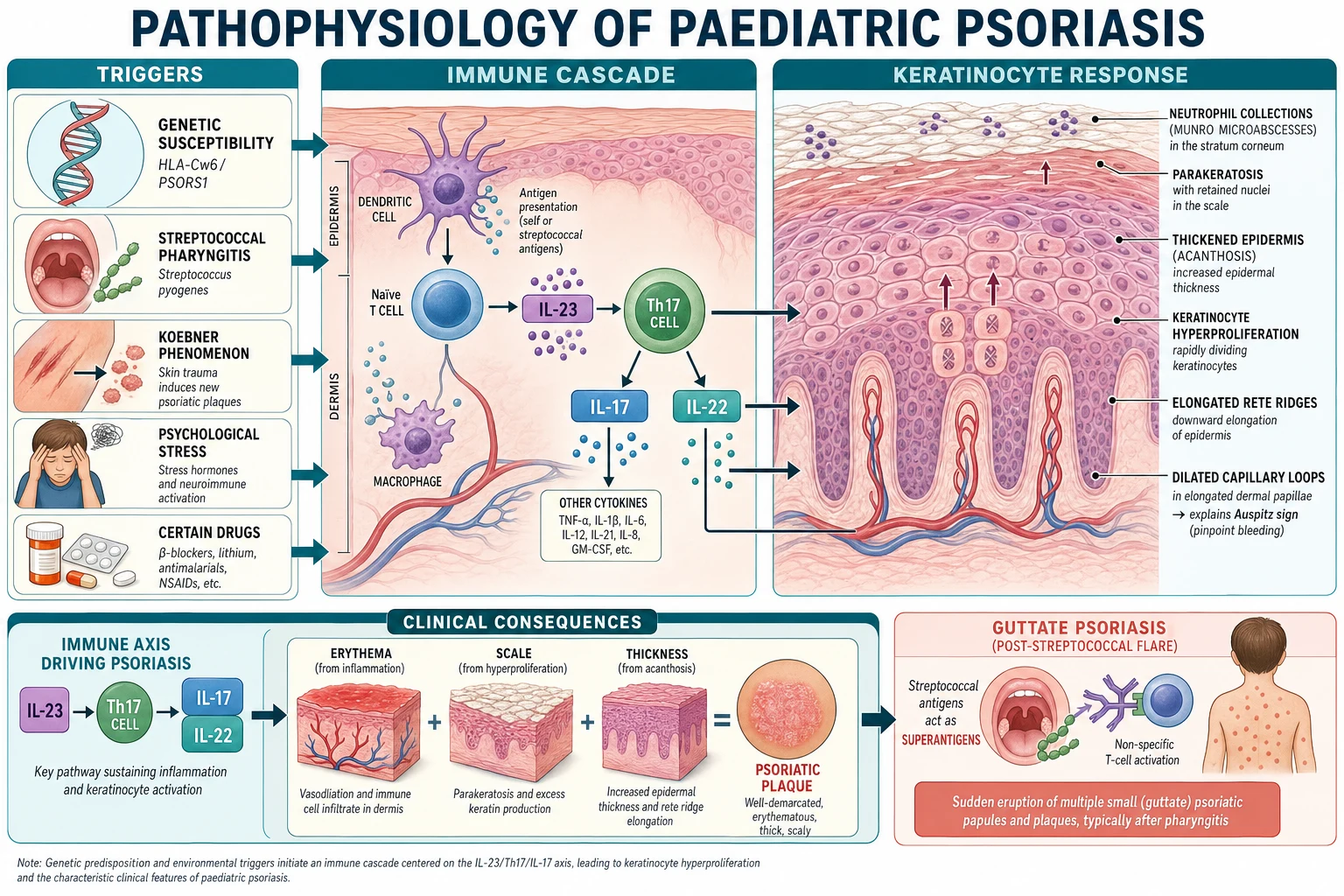
The histology mirrors the pathophysiology and explains the clinical signs. Acanthosis (epidermal thickening) and elongated rete ridges give the plaque its elevation; parakeratosis with retained nuclei and Munro microabscesses (neutrophil collections in the stratum corneum) give the silvery scale; and dilated, tortuous capillary loops in the elongated dermal papillae explain why lifting the scale produces the pinpoint bleeding of the Auspitz sign. Keratinocyte turnover is compressed from the normal twenty-eight days to as little as three to five days, so cells arrive at the surface still nucleated and sticky. [2] [3]
Guttate psoriasis is the post-streptococcal variant of the same mechanism. Streptococcal superantigens and cross-reactive antibodies activate T-cells in a genetically susceptible (often HLA-Cw6-positive) child, igniting the IL-23 and Th17 and IL-17 loop in dozens of small lesions at once. This is why a throat infection, not skin trauma, is the trigger, why guttate disease appears so abruptly, and why it often remits once the streptococcal drive is removed. [7] [2]
Clinical Presentation
The classic plaque presentation lives on the extensor limbs and scalp of a school-age child or adolescent. Sharply demarcated, raised, erythematous plaques with a thick, silvery-white scale appear on the elbows, knees, scalp and lumbosacral skin, and are often symmetric. They itch variably, sometimes bleed when scratched, and run a chronic relapsing course with remissions and flares. Auspitz sign and Koebner phenomenon are the two bedside signs that confirm the diagnosis, and scalp involvement — with scale that extends beyond the hairline — is a frequent first or accompanying site. [2] [3]
Guttate psoriasis presents very differently. Over a few days, one to two weeks after a sore throat, a crop of small, round or teardrop-shaped, salmon-pink papules with fine scale erupts symmetrically across the trunk and proximal limbs. The child may still have signs of pharyngitis or be asymptomatic, and the lesions are smaller and finer-scaled than chronic plaques. Guttate disease is often the first presentation of psoriasis in a child or young adult, and it carries a better chance of spontaneous remission than chronic plaque disease, though it can evolve into chronic plaque psoriasis over time. [7] [3]
Nail involvement is common and frequently overlooked. Look for pitting, onycholysis (separation of the nail plate from the bed), the oil-drop or salmon-patch discolouration under the nail, and subungual hyperkeratosis. Nail psoriasis accompanies scalp and plaque disease, predicts juvenile psoriatic arthritis, and is a source of real distress for older children and adolescents. Examine the nails of every child with suspected psoriasis. [2] [3]
Ask explicitly about the joints. Joint pain, early-morning stiffness, swelling of a single joint or a whole digit (dactylitis), and nail dystrophy together signal juvenile psoriatic arthritis, which can precede, accompany or follow the skin disease and is easily missed if not specifically sought. A child with psoriasis and any joint complaint needs a careful musculoskeletal examination and early referral, because untreated arthritis erodes quality of life and risks permanent joint damage and uveitis. [1] [2]
Differential Diagnosis
For a scaly plaque on the elbow or knee, the differential turns on morphology and distribution. Atopic dermatitis is flexural, poorly demarcated and intensely itchy, with a personal or family atopy history; psoriasis is extensor, sharply demarcated and thick-scaled, though the two can coexist and psoriasis can be impetiginised. Seborrhoeic dermatitis produces greasy, yellowish scale on the scalp, nasolabial folds and eyebrows rather than the dry, silvery, well-demarcated scale of psoriasis, though scalp and facial psoriasis can overlap with it ( Sebopsoriasis ). Tinea is annular with an advancing scaly edge and a central clearing, and confirms with potassium hydroxide examination of skin scrapings. [2] [3]
For a guttate or papular eruption, the differential is acute and infective. Pityriasis rosea begins with a herald patch and follows skin lines in a Christmas-tree pattern on the trunk, with an oval, finely scaled plaque. Secondary syphilis produces a papulosquamous eruption including the palms and soles, with generalised lymphadenopathy and risk factors. Viral exanthems and drug eruptions enter when the history fits. For the infant with napkin-area erythema, distinguish psoriasis from irritant nappy dermatitis (sparing the folds, worse over convexities), candidal nappy dermatitis (bright red with satellite pustules) and seborrhoeic dermatitis. [2] [3]
For scalp scaling, distinguish scalp psoriasis from tinea capitis (alopecia, broken hairs, lymphadenopathy, potassium hydroxide positivity) and seborrhoeic dermatitis. For a single, atypical or non-responsive lesion, consider nummular eczema, pityriasis rubra pilaris and, rarely, cutaneous T-cell lymphoma in an adolescent with a persistent, treatment-resistant plaque. A biopsy is reserved for genuinely atypical or non-responsive disease. [2] [1]
Clinical & Bedside Assessment
Begin with a focused history of the eruption — onset, evolution, distribution, itch, and any trigger in the preceding weeks. Ask specifically about sore throat or fever one to two weeks before an acute guttate flare, about skin trauma at sites of new plaques (Koebner), about stress and new medications, and about the family history of psoriasis, psoriatic arthritis or autoimmune disease. Ask about the joints — morning stiffness, joint swelling, a swollen digit — and about the impact on school, friendships, sleep and mood, because the psychosocial burden is part of the disease, not a footnote. [1] [2]
Examine the whole skin in good light. Map the distribution (extensor, scalp, face, flexural, napkin), describe the primary lesion (well-demarcated erythematous plaque with silvery scale; droplet papules), and elicit Auspitz and Koebner signs. Examine the scalp beyond the hairline, the nails for pitting, onycholysis and oil-drop change, the ears and the genitalia, and weigh and measure the child to calculate body mass index. Perform a focused joint examination for swelling, tenderness, reduced range and dactylitis. [2] [3]
Measure severity consistently, because treatment intensity follows it. Estimate the body surface area involved, record a Physician Global Assessment or, where trained, a Psoriasis Area and Severity Index, and capture quality of life with the Children's Dermatology Life Quality Index (CDLQI) or the dermatology life quality index in older adolescents. A child with limited skin disease but a devastated CDLQI may warrant more aggressive therapy than the surface area alone suggests, because the disability is lived in the schoolyard and the bedroom, not on the skin. [1] [2]
Screen for comorbidity at the bedside. Measure body mass index and blood pressure, ask about snoring and physical activity, and in moderate to severe disease arrange lipids and fasting glucose. Screen mood and ask about bullying and school refusal, because depression and anxiety are commoner in children with psoriasis and are treatable. Document the joint examination findings even when normal, so that later change is detectable. [11] [4]
Investigations
Psoriasis is a clinical diagnosis. The well-demarcated, silvery-scaled plaque on an extensor surface, with Auspitz and Koebner signs, scalp and nail involvement and a family history, needs no investigation to confirm. A skin biopsy is reserved for the genuinely atypical, non-responsive or diagnostically uncertain case — for example, to distinguish psoriasis from cutaneous T-cell lymphoma or pityriasis rubra pilaris — and histopathology then shows the characteristic acanthosis, parakeratosis, Munro microabscesses and elongated rete ridges. [1] [2]
For suspected guttate psoriasis after a sore throat, confirm the streptococcal trigger with a throat swab and, if needed, an antistreptolysin-O titre or anti-DNase B. Treating the streptococcal infection is good practice, though the Cochrane evidence that antistreptococcal therapy or tonsillectomy reliably clears established guttate psoriasis is limited and inconsistent, so these interventions are adjuncts, not stand-alone cures. [7] [8]
Comorbidity screening in moderate to severe disease is where the investigations matter. Measure height, weight and body mass index; check blood pressure; and arrange fasting lipids and glucose in severe or widespread disease. For joint symptoms, request inflammatory markers and, with rheumatology guidance, imaging of affected joints. Before starting a systemic or biologic agent, baseline tests are required — full blood count, liver and renal function, and screening for tuberculosis, hepatitis B and C, and (for some agents) HIV — because each therapy carries its own monitoring and safety obligations. [1] [10]
In Australia and New Zealand, the publicly funded access pathway for biologic agents requires documentation of severe disease and the failure of, or contraindication to, conventional systemic therapy, supported by a specialist dermatologist. This means the pre-biologic work-up — confirming severity, documenting prior therapy, and completing the infectious-disease and comorbidity screen — is part of delivering equitable, guideline-based care, particularly for rural and remote families who may access the specialist only through outreach or telehealth. [1] [10]
Management — Resuscitation
Resuscitation belongs to the rare but dangerous end of the paediatric psoriasis spectrum. The red flags are a child with erythrodermic psoriasis — erythema and scaling covering most of the body, with shivering, tachycardia, hypothermia or hyperthermia and fluid and electrolyte disturbance — and a child with generalised pustular psoriasis — widespread sterile pustules on fiery erythema with fever, malaise and skin pain. Both are dermatological emergencies: admit, assess and stabilish temperature, fluid and electrolyte balance, exclude infection and sepsis, and involve dermatology urgently for systemic therapy. [1] [3]
The second emergency is not on the skin. A child or adolescent with psoriasis in severe psychological distress — depression, anxiety, self-harm thoughts, school refusal or bullying — needs immediate psychosocial assessment and support, because the visible, chronic, stigmatising nature of psoriasis carries a real suicide and depression risk that is disproportionate to the surface area involved. A screen for mood and self-harm is part of the acute assessment when the distress is evident, and referral to psychology or child and adolescent mental health should be prompt, not deferred to the next routine visit. [1] [2]
Keep resuscitation separate from routine care in your mind. The vast majority of children with psoriasis are well, with limited plaque disease managed in the outpatient or community setting, and need no acute intervention at all. The danger lives in the erythrodermic and pustular forms, the joint disease that threatens permanent damage, and the psychological collapse — each a reason to move beyond topical therapy and involve the specialist urgently. [1] [3]
Management — Definitive & Stepwise
Definitive management runs as a severity-matched ladder, climbing from skin care and topical therapy through phototherapy to systemic and biologic agents, with comorbidity and psychosocial care running alongside at every step. The joint AAD-NPF paediatric psoriasis guideline frames this as a stepwise, shared decision with the family that weighs disease severity, quality-of-life impact, comorbidity and the risks of each therapy. The art is to match the intensity to the disease and its burden, not to escalate reflexively. [1] [2]
The foundation for every child is skin care and trigger avoidance. Generous, frequent emollients reduce scale, itch and irritation; gentle, fragrance-free washes protect the barrier; sun protection prevents Koebner flares from sunburn; and identification and management of triggers — streptococcal infection, stress, skin trauma, obesity and exacerbating drugs — reduces flares. Education and a written management plan anchor long-term adherence, which is the single biggest determinant of outcome in a chronic relapsing disease. [1] [2]
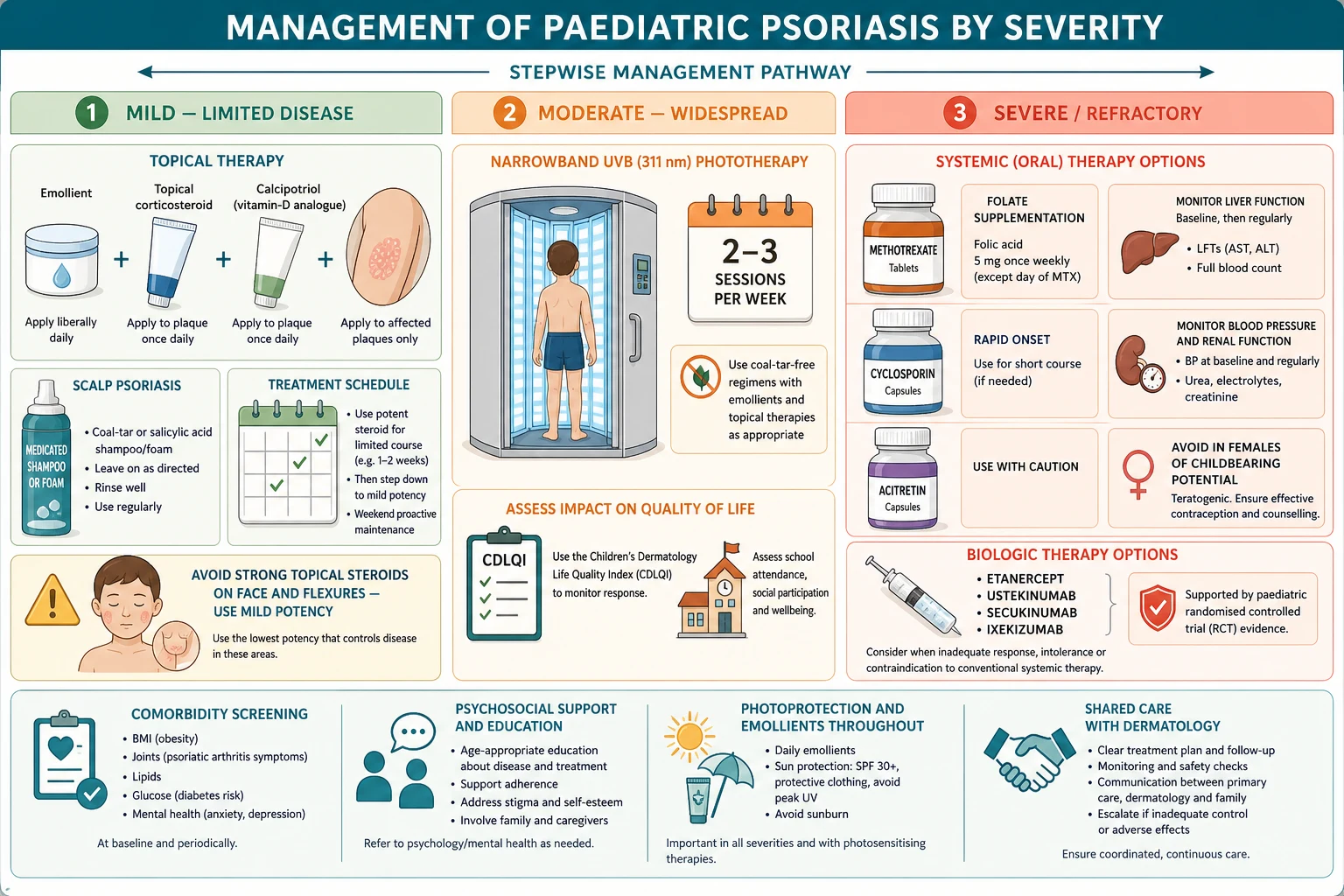
For mild to moderate limited plaque disease, first-line is a potency-matched topical corticosteroid combined with a vitamin-D analogue such as calcipotriol. A potent corticosteroid (for example betamethasone or mometasone) suits trunk and limb plaques for a limited course, while a mild corticosteroid such as hydrocortisone 1 per cent is used on the face, flexures and genitals to avoid atrophy. Calcipotriol is applied once or twice daily and is steroid-sparing, and a combined calcipotriol and betamethasone preparation simplifies adherence. After control, step down to calcipotriol or weekend proactive maintenance to reduce flare. [1] [2]
Paediatric psoriasis therapy ladder (AAD-NPF paediatric guideline; confirm local formularies)
For moderate to widespread plaque disease, the first-line second step is narrowband UVB phototherapy at 311 nm, delivered two to three times weekly in a dermatology service. It is effective and well tolerated in children old enough to cooperate (often school-age and older), and it avoids the systemic risks of oral therapy, though cumulative ultraviolet exposure and a lifetime skin-cancer consideration limit its use. For acute, extensive guttate psoriasis, a short course of narrowband UVB can accelerate clearance alongside emollients and topical therapy. [1] [2]
For severe, refractory or quality-of-life-destroying disease, systemic therapy steps in. Methotrexate is the usual first systemic choice — given once weekly (approximately 0.1 to 0.4 mg/kg/week, up to about 25 mg/week) by mouth or subcutaneously, supplemented with folic acid, with monitoring of full blood count and liver function. Cyclosporin gives rapid short-course control for the child who needs stabilising quickly, with blood pressure and renal monitoring, before transition to a maintenance agent. Acitretin, an oral retinoid, suits pustular and palmoplantar patterns but is strongly teratogenic, so it is avoided or used with rigorous contraception in adolescent girls of childbearing potential. [1] [2]
The biologics have transformed severe paediatric psoriasis. The landmark etanercept trial in children and adolescents with plaque psoriasis — subcutaneous etanercept at 0.8 mg/kg weekly — showed clear benefit over placebo and established the paediatric evidence base in 2008. Ustekinumab (blocking IL-12 and IL-23), secukinumab and ixekizumab (blocking IL-17A), and guselkumab and risankizumab (blocking IL-23) now extend the options, with age-specific approvals and a growing paediatric evidence base synthesised in the recent biologics network meta-analysis. A biologic is considered for severe, refractory disease or where conventional systemic therapy fails or is unsuitable, after a baseline infectious-disease screen and within a specialist service. [9] [10]
The stepwise paediatric psoriasis pathway
Assess severity and impact: body surface area, Physician Global Assessment or PASI, and the Children's Dermatology Life Quality Index; screen weight, blood pressure, joints and mood.
Foundation for all: emollients, fragrance-free washes, trigger identification (strep, stress, trauma, drugs, obesity) and a written management plan.
Mild to moderate limited plaque: potency-matched topical corticosteroid plus calcipotriol; mild steroid (hydrocortisone 1%) on face and flexures; scalp preparations as needed.
Moderate to widespread: narrowband UVB phototherapy (311 nm), two to three times weekly in dermatology.
Severe, refractory or quality-of-life-destroying: methotrexate once weekly with folic acid and monitoring; cyclosporin for rapid short courses; acitretin with strict pregnancy avoidance.
Failure or unsuitability of conventional systemic therapy: refer for a biologic (etanercept, ustekinumab, IL-17 and IL-23 inhibitors) after baseline TB and infection screening.
Comorbidity and psychosocial care throughout: weight and metabolic management, joint surveillance for juvenile psoriatic arthritis, and mental-health support.
Guttate flare: confirm and treat streptococcal pharyngitis; phototherapy or short topical therapy; tonsillectomy only in selected recurrent cases.
Specific Subtypes & Scenarios
A school-age child with chronic plaque psoriasis. This is the bread-and-butter case. Confirm the clinical diagnosis, measure severity and quality of life, and start a potency-matched topical corticosteroid plus calcipotriol for trunk and limb plaques, with a mild steroid on any facial involvement. Emollients and a written plan anchor adherence, and a step-down to calcipotriol or weekend proactive maintenance reduces flare. Screen for obesity, joints and mood at each visit, and set the expectation of a chronic relapsing course managed in partnership with the family and, where needed, a dermatologist. [1] [2]
An adolescent with acute guttate psoriasis after a sore throat. Confirm the streptococcal trigger with a throat swab and antistreptolysin-O titre and treat the pharyngitis. Explain that guttate psoriasis often remits over weeks to months, and manage with emollients and a mild to moderate topical steroid for comfort; a short course of narrowband UVB accelerates clearance in extensive disease. Warn the family that guttate disease can be the first presentation of psoriasis and may evolve into chronic plaque disease, so ongoing review matters. [7] [3]
An infant with napkin or diaper-area psoriasis. Recognise the well-demarcated, glossy erythema in the nappy area, often sparing the deep folds, and distinguish it from irritant and candidal nappy dermatitis. Use a mild topical steroid with or without calcipotriol cautiously, and emphasise barrier protection and frequent nappy changes. Napkin psoriasis may resolve or may progress to generalised plaque disease, so follow the infant over time and reassure the family about the generally good prognosis. [2] [3]
A child with scalp and nail psoriasis. Scalp disease responds to potent topical steroids (for example clobetasol) in a scalp formulation for limited periods, combined with calcipotriol scalp application and coal-tar or salicylic-acid shampoos to lift scale. Nail disease is stubborn and slow to respond, and it predicts juvenile psoriatic arthritis, so examine the joints and refer early if there is any joint complaint. Both scalp and nail involvement carry a heavy psychosocial burden for older children and adolescents. [2] [1]
A child with juvenile psoriatic arthritis. Joint pain, morning stiffness, swelling or dactylitis in a child with psoriasis — or nail dystrophy and a family history even before obvious skin disease — signals juvenile psoriatic arthritis. Refer early to paediatric rheumatology, because untreated disease risks permanent joint damage and uveitis; screen for uveitis as guided by the rheumatology team. The skin and the joints are treated in partnership between dermatology and rheumatology, and a biologic that addresses both (such as a TNF-alpha or IL-17 or IL-23 agent) may be preferred. [1] [2]
A child with erythrodermic or generalised pustular psoriasis. This is the emergency end. Admit for temperature, fluid and electrolyte support, exclude infection and sepsis, and involve dermatology urgently for systemic therapy (such as cyclosporin for rapid control, a biologic, or methotrexate). The child is at risk of hypothermia, dehydration, secondary infection and high-output cardiac stress from the compromised skin barrier, so supportive care runs alongside the disease-specific therapy. [1] [3]
Complications & Pitfalls
The comorbidities are the complications that every examiner probes. Obesity and metabolic syndrome cluster with paediatric psoriasis — dyslipidaemia, hypertension and insulin resistance begin in childhood and carry forward to adult cardiovascular risk, so weight, body mass index, blood pressure, lipids and glucose are part of the assessment. Juvenile psoriatic arthritis affects a meaningful minority and risks permanent joint damage and uveitis if missed. Depression, anxiety and reduced quality of life are commoner in children with psoriasis, with a suicide and self-harm risk that is disproportionate to the surface area involved. [11] [4]
The first pitfall is misdiagnosing psoriasis as eczema or seborrhoeic dermatitis, particularly facial, scalp and napkin disease in children. The well-demarcated, thick, silvery scale, the extensor distribution, Auspitz and Koebner signs and the nail changes distinguish psoriasis, and missing them delays the right treatment and the comorbidity screen. When a child's "eczema" is not responding, reconsider the diagnosis. [2] [3]
The second pitfall is overusing potent topical corticosteroids, especially on the face, flexures and genitals and over large body surface areas. The result is skin atrophy, telangiectasia and, with very potent agents under occlusion or over a large area, hypothalamic-pituitary-adrenal axis suppression. Match the potency to the site — mild on the face and flexures, potent on trunk and limbs — use limited courses, and step down to calcipotriol or weekend proactive maintenance once controlled. [1] [2]
The third pitfall is ignoring the psychosocial burden. A child with limited skin disease but a devastated quality of life needs more than a reassurance and a cream; the visible, chronic, stigmatising nature of psoriasis shapes schooling, friendships and mood, and unaddressed distress leads to non-adherence and worse outcomes. Screen mood and ask about bullying and school refusal at every visit, and refer to psychology or child and adolescent mental health when the burden is clear. [1] [2]
The fourth pitfall is missing juvenile psoriatic arthritis. Joint symptoms can precede obvious skin disease, nail dystrophy alone may be the clue, and dactylitis is easily overlooked. A child with psoriasis and any joint complaint needs a careful musculoskeletal examination and early rheumatology referral, because the window to prevent permanent joint damage closes with delay. [1] [2]
The fifth pitfall is teratogenicity with acitretin and pregnancy risk with systemic therapy in adolescent girls. Acitretin is strongly teratogenic and requires robust contraception and pregnancy avoidance, and methotrexate is also avoided in pregnancy. Counselling adolescent girls about contraception and pregnancy prevention is part of prescribing these agents, and the choice of therapy in a girl of childbearing potential may favour an alternative. [1] [3]
Prognosis & Disposition
Psoriasis is a chronic, relapsing disease, and the disposition is overwhelmingly outpatient and community-based for the majority of children. Most children with limited plaque disease are managed by their general practitioner and a dermatologist with topical therapy, phototherapy where needed, and comorbidity and psychosocial care, with a good quality of life when the disease is controlled. Guttate psoriasis carries a better prognosis, with spontaneous remission over weeks to months in many children, though it can evolve into chronic plaque disease. [1] [3]
Admit the rare emergency presentations — erythrodermic and generalised pustular psoriasis, and the child with acute, severe psychological distress or self-harm risk — for stabilisation, supportive care and urgent specialist therapy. Escalate to a specialist dermatology service for moderate to severe disease needing phototherapy or systemic or biologic therapy, and to paediatric rheumatology for juvenile psoriatic arthritis. The threshold to involve specialists is lower for the very young, the severely affected and those with significant comorbidity or psychosocial burden. [1] [2]
At each review, re-measure severity and quality of life, screen for comorbidity (weight, blood pressure, joints, mood), and adjust therapy to the current disease burden. A chronic disease demands a long-term partnership: education, a written management plan, adherence support, and clear safety-netting for the red flags of erythroderma, pustular change, joint symptoms and psychological collapse. Early-onset disease tends to persist into adulthood, so the relationship built in childhood shapes the adult outcome. [2] [11]
Special Populations
Infants most often present with napkin or diaper-area psoriasis, and the priority is gentle, barrier-protective care and a mild topical steroid, with avoidance of potent agents on the thin infant skin. Distinguish napkin psoriasis from irritant and candidal nappy dermatitis, and follow the infant over time, because it may resolve or progress. The threshold to involve a dermatologist is low for an infant with widespread or atypical disease. [2] [3]
Adolescents carry the heaviest psychosocial burden and the most complex therapeutic decisions. Body image, bullying, intimate relationships and adherence all shape the disease, and contraception and pregnancy prevention govern the choice of systemic therapy in girls of childbearing potential. Treat the adolescent with respect for autonomy, screen mood and self-harm, and involve psychology and dermatology for moderate to severe disease, because this is the age where the lifetime pattern of disease and its management is set. [1] [2]
Children with obesity have more severe, more treatment-resistant disease and a greater metabolic and cardiovascular comorbidity burden. Weight management — through family-based behavioural change, physical activity and nutrition support — is part of psoriasis care, not a separate problem, because weight loss can improve disease severity and reduces the long-term metabolic risk. Address the weight at the same consultation as the skin. [11] [4]
Children in rural, remote and disadvantaged communities, and Indigenous families, face real inequity of access to specialist dermatology, phototherapy and biologics, with long waits and travel that compound the burden of a chronic disease. Deliver care through outreach and telehealth where possible, ensure culturally safe and equitable access to specialist therapy, and advocate for the public-funding and service pathways that make guideline-based care achievable where the family lives. Disadvantage and distance should never be the reason a child with severe psoriasis cannot access a biologic. [1] [2]
Immunocompromised children with psoriasis need coordinated care between dermatology and the treating immunology, oncology or transplant team, because the systemic and biologic therapies carry infection risk and interact with the underlying condition. A biologic may still be appropriate but only after careful infectious-disease screening and within a specialist multidisciplinary framework. [1] [10]
Evidence, Guidelines & Regional Differences
The treatment evidence for paediatric psoriasis is anchored by the joint AAD-NPF guideline for psoriasis in pediatric patients, which sets out the severity-matched, stepwise approach — emollients and topical therapy, phototherapy, conventional systemic agents and biologics — with explicit attention to paediatric-specific issues such as growth, psychosocial development and school. The evolving-perspectives and childhood-psoriasis reviews consolidate the clinical forms, the paediatric-specific presentations and the therapeutic ladder that guides practice. [1] [2] [3]
Etanercept for children and adolescents with plaque psoriasis
Population: Children and adolescents aged 4 to 17 years with moderate to severe plaque psoriasis, in a randomised, placebo-controlled trial of subcutaneous etanercept at 0.8 mg/kg weekly.
Key finding
Etanercept significantly improved plaque psoriasis in children and adolescents compared with placebo, with a safety profile consistent with that seen in adults, establishing the paediatric evidence base for biologic therapy.
Practice change
Etanercept opened the door to biologic therapy in children with severe plaque psoriasis, and it underpins the modern stepwise approach in which biologics follow or replace conventional systemic therapy for severe, refractory disease.
The biologic evidence base has grown rapidly. The recent network meta-analysis of biologics for paediatric plaque psoriasis synthesises the randomised evidence across the IL-17, IL-23 and TNF-alpha classes, ranking the agents by efficacy and tolerability and confirming that several biologics now have age-specific paediatric approvals for moderate to severe disease. Ustekinumab (IL-12 and IL-23), secukinumab and ixekizumab (IL-17A), and guselkumab and risankizumab (IL-23) extend the options first opened by etanercept, with the choice guided by severity, comorbidity, prior therapy and the infectious-disease and psychosocial profile. [10] [2]
The comorbidity evidence is equally important. The systematic review and meta-analysis of cardiovascular and metabolic comorbidities in paediatric psoriasis confirms that children with psoriasis carry a greater burden of obesity, dyslipidaemia, hypertension and insulin resistance than their peers, justifying routine comorbidity screening. The epidemiology studies — from Germany, the United States and the Global Burden of Disease analysis — establish the prevalence, the family-history association and the worldwide consistency of the disease. [11] [4] [5] [6]
For guttate psoriasis, the Cochrane review of non-antistreptococcal interventions for acute guttate psoriasis highlights the limited and inconsistent evidence for many treatments, and the tonsillectomy review confirms that tonsillectomy can improve psoriasis in selected recurrent, streptococcal-triggered cases but is not a stand-alone cure. Treating the streptococcal trigger and using phototherapy or topical therapy remain the practical approach to the acute guttate flare. [7] [8]
The regional policy structure is consistent in principle and varies in access. In the United Kingdom, NICE guidance (CG153) sets the assessment and stepwise management of psoriasis across severity. In the United States and Canada, the joint AAD-NPF paediatric guideline and the American and Canadian specialist guidance frame the topical-to-systemic-to-biologic ladder. In Australia and New Zealand, the Therapeutic Guidelines and trans-Tasman specialist practice guide the same stepwise approach, with public-funding pathways governing access to the more costly biologics and a focus on equitable access for rural and remote families. In every region the principle is the same: match the therapy to the severity and the burden, protect the child from the harms of treatment, screen for comorbidity, and address the psychosocial dimension. [1] [2]
The controversies are real and active: the optimal sequencing of systemic and biologic therapy in children; the long-term safety of biologics over a lifetime; the role of tonsillectomy in recurrent guttate disease; how aggressively to screen and intervene on metabolic comorbidity; and the inequities in access to specialist and biologic care that leave disadvantaged and remote children under-treated. The defence against each is the same: guideline-based, severity-matched therapy delivered in partnership with the family, with comorbidity and psychosocial care running alongside at every step. [1] [10]
Exam Pearls
- Childhood psoriasis is an immune-mediated, IL-23 and Th17 and IL-17 driven disease with HLA-Cw6 genetics; the two classic forms are chronic plaque (extensor, scalp, silvery scale, Auspitz and Koebner signs) and acute guttate (droplet papules one to two weeks after streptococcal pharyngitis). [2]
- Children differ from adults: facial involvement is commoner, the scalp is a frequent first site, and infants get napkin or diaper-area psoriasis. [3]
- The diagnosis is clinical; biopsy is for atypical or non-responsive disease, and severity is judged by body surface area, PASI or PGA, and the Children's Dermatology Life Quality Index (CDLQI). [1]
- First-line for limited plaque disease is emollients plus a potency-matched topical corticosteroid combined with calcipotriol — potent on trunk and limbs, mild (hydrocortisone 1%) on face and flexures to avoid atrophy and adrenal suppression. [2]
- Moderate to widespread disease takes narrowband UVB phototherapy (311 nm), two to three times weekly, as the first-line second step. [1]
- Severe or refractory disease takes methotrexate once weekly (approximately 0.1 to 0.4 mg/kg/week up to about 25 mg/week) with folic acid, cyclosporin for rapid short courses, and acitretin only with strict pregnancy avoidance in adolescent girls. [1]
- The landmark paediatric biologic trial is etanercept 0.8 mg/kg weekly (Paller, NEJM 2008); ustekinumab and the IL-17 and IL-23 inhibitors extend the options for severe disease. [9] [10]
- Guttate psoriasis after strep often remits spontaneously; treat the streptococcal trigger and use phototherapy or short topical therapy; tonsillectomy is only for selected recurrent cases. [7] [8]
- Screen the comorbidities at every visit: obesity and metabolic risk, juvenile psoriatic arthritis, and depression and quality-of-life burden. [11] [4]
- The emergencies are erythrodermic and generalised pustular psoriasis — admit, support, exclude sepsis, and involve dermatology urgently. [1] [3]
References
- [1]Menter A; Cordoro KM; Davis DMR; Feldman SR; et al Joint American Academy of Dermatology-National Psoriasis Foundation guidelines of care for the management and treatment of psoriasis in pediatric patients. J Am Acad Dermatol, 2020.PMID 31703821
- [2]Eichenfield LF; Paller AS; Tom WL; Lara-Corrales I; et al Pediatric psoriasis: Evolving perspectives. Pediatr Dermatol, 2018.PMID 29314219
- [3]Mahe E Childhood psoriasis. Eur J Dermatol, 2016.PMID 27900946
- [4]Augustin M; Glaeske G; Radtke MA; Christophers E; et al Epidemiology and comorbidity of psoriasis in children. Br J Dermatol, 2010.PMID 19922529
- [5]Paller AS; Singh R; Cloutier M; Gauthier-Loiselle M; et al Prevalence of psoriasis in children and adolescents in the United States: A claims-based analysis. J Drugs Dermatol, 2018.PMID 29462227
- [6]Mehrman S; Uppal P; Nedley N; Gwillim EC; et al The global, regional, and national burden of psoriasis in 195 countries and territories, 1990 to 2017: A systematic analysis from the Global Burden of Disease Study 2017. J Am Acad Dermatol, 2021.PMID 32376432
- [7]Maruani A; Samimi M; Stembridge N; McBride S; et al Non-antistreptococcal interventions for acute guttate psoriasis or an acute guttate flare of chronic psoriasis. Cochrane Database Syst Rev, 2019.PMID 30958563
- [8]Wu W; Debbaneh M; Moslehi H; Koo J; Liao W Tonsillectomy as a treatment for psoriasis: a review. J Dermatolog Treat, 2014.PMID 24283892
- [9]Paller AS; Siegfried EC; Langley RG; Gottlieb AB; et al Etanercept treatment for children and adolescents with plaque psoriasis. N Engl J Med, 2008.PMID 18199863
- [10]Aljalfan AA; Maniya MT; Sachedina D; Alavi A; et al Biologics for treatment of paediatric plaque psoriasis: A systematic review and network meta-analysis. J Eur Acad Dermatol Venereol, 2026.PMID 41090545
- [11]Phan K; Lee G; Fischer G Pediatric psoriasis and association with cardiovascular and metabolic comorbidities: Systematic review and meta-analysis. Pediatr Dermatol, 2020.PMID 32436322