Paeds · paediatric-dermatology
Stevens-Johnson syndrome and toxic epidermal necrolysis
Also known as Stevens-Johnson syndrome · SJS · Toxic epidermal necrolysis · TEN · Lyell syndrome · SJS-TEN overlap · Mycoplasma-induced rash and mucositis
Fellowship topic on Stevens-Johnson syndrome (SJS), SJS-TEN overlap and toxic epidermal necrolysis (TEN) in children: a severe, usually drug-induced, T-cell-mediated mucocutaneous reaction causing full-thickness epidermal necrosis and detachment, classified by the percentage of body-surface-area detached (under 10, 10 to 30, over 30); the allopurinol, anticonvulsant, sulfonamide and nevirapine culprits and the HLA-B pharmacogenetic associations including HLA-B*15:02 for carbamazepine; the granulysin, Fas-FasL and perforin-granzyme effector mechanisms; the Mycoplasma-induced rash and mucositis syndrome distinct from drug-induced SJS; the differential from staphylococcal scalded skin syndrome where mucosae are spared; SCORTEN severity scoring with its seven risk factors and mortality bands; and management centred on immediate withdrawal of the culprit drug, burn-unit or PICU supportive care, meticulous eye care, and the lack of proven survival benefit for IVIG, cyclosporine and corticosteroids.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
SCORTEN — seven risk factors, one mortality ladder
Overview & Definition
Picture a seven-year-old who started lamotrigine six weeks ago for new-onset epilepsy and now arrives with fever, painful red eyes, blistering lips and tender purple target lesions spreading across the trunk, the skin wrinkling and shearing where you touch it. This is Stevens-Johnson syndrome in its classic drug-induced form — one of the true dermatological emergencies of childhood, where the speed of recognition, the withdrawal of the offending drug and the quality of supportive care decide whether the child survives and whether they keep their sight. The clinician's task is to recognise the reaction, grade its severity, remove the cause, and deliver burns-grade supportive care while an honest eye is kept on the ocular surface. [6] [2]
Stevens-Johnson syndrome and toxic epidermal necrolysis are a single disease spectrum of severe, usually drug-induced, mucocutaneous reaction characterised by full-thickness necrosis and detachment of the epidermis. They are uncommon — an incidence of the order of one to two per million people per year in children — but they carry mortality up to around 30 percent for TEN in mixed cohorts, and they leave a heavy burden of long-term sequelae in survivors, above all in the eye. [6] [7]
The clinician's task has three layers. The first is recognition — distinguishing SJS and TEN from their mimics, above all staphylococcal scalded skin syndrome where the mucosae are spared, and from Mycoplasma-induced rash and mucositis where the skin is relatively spared. The second is grading and resuscitation — calculating SCORTEN, stopping the culprit drug, and escalating the child to a burn-capable or intensive-care setting. The third is the long view — protecting the ocular surface from the first hours, anticipating the metabolic and infectious stresses of extensive skin loss, and counselling the family on lifelong drug avoidance and HLA pharmacogenetic screening. [1] [10]
Classification
Sorting the SJS-TEN spectrum by how much skin is detached matters because extent drives severity, disposition and prognosis. The agreed classification turns on the percentage of body-surface-area with epidermal detachment, taken together with atypical target lesions and mucosal involvement at two or more sites. Stevens-Johnson syndrome is defined as detachment of less than 10 percent of body surface area. SJS-TEN overlap occupies 10 to 30 percent. Toxic epidermal necrolysis is detachment of more than 30 percent of body surface area, and may be further described by whether widespread non-confluent target lesions are present (TEN with spots) or absent (TEN without spots). [1] [8]
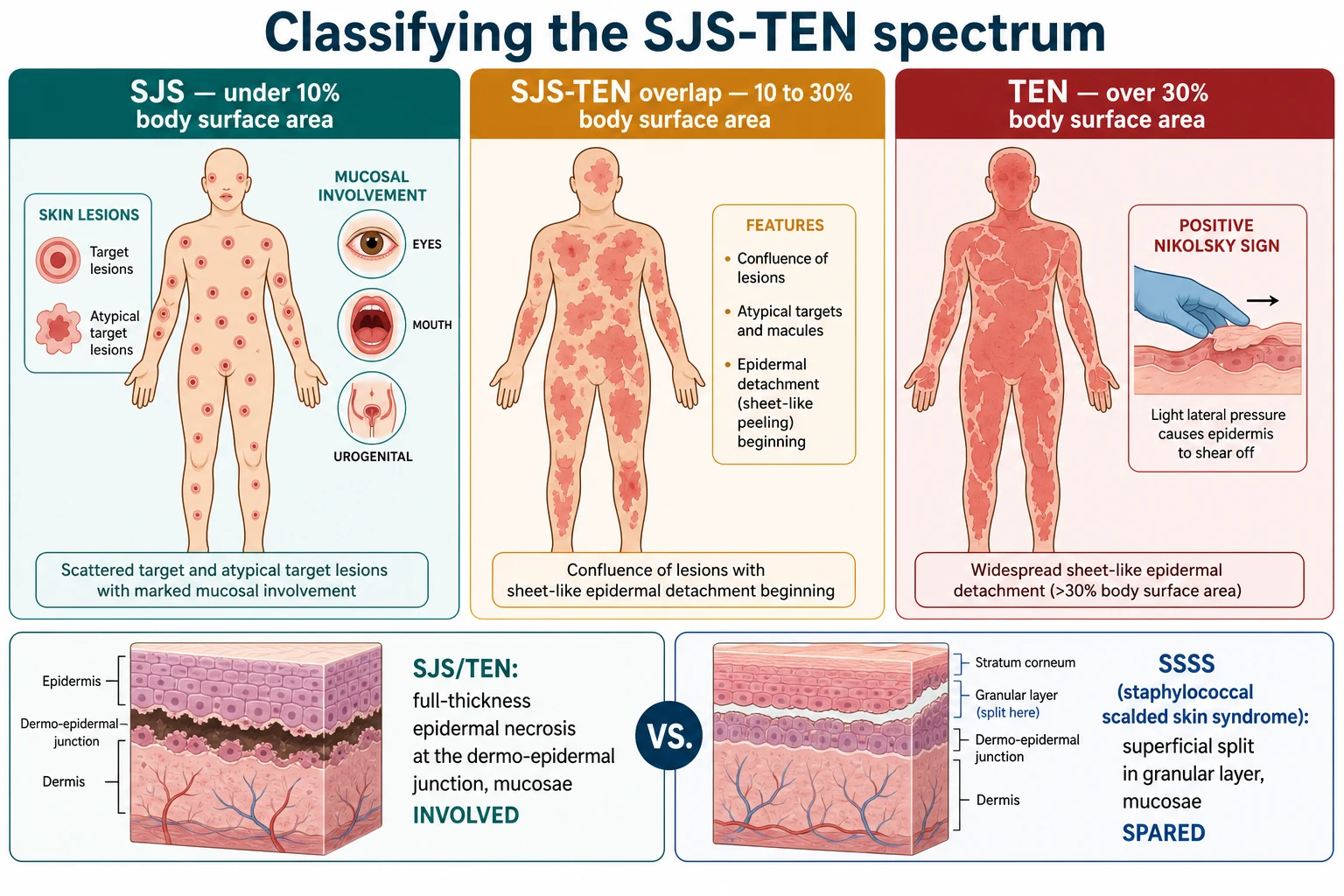
The morphological hallmarks are consistent across the spectrum. The primary skin lesions are atypical target lesions — purpuric, dusky macules with or without a blistering centre that do not have the tidy three-zone ring of classic erythema multiforme — together with flaccid bullae and areas of confluent erythema that detach with light pressure (the Nikolsky sign). Mucosal involvement is obligatory and usually affects at least two of the ocular, oral and urogenital surfaces, producing painful erosions, crusting of the lips and difficulty eating or urinating. [12] [5]
The non-drug form worth naming separately is Mycoplasma-induced rash and mucositis (MIRM). Triggered by Mycoplasma pneumoniae rather than a drug, it predominantly affects children and young adults, produces striking mucositis at two or more sites — especially the mouth, eyes and urogenital tract — with sparse or absent skin lesions, and follows a respiratory prodrome with fever. The systematic review distinguishing it from classic drug-induced SJS found a younger median age, prominent mucositis, relative skin sparing, frequent recurrence and a markedly better prognosis. Recognising MIRM matters because the management centres on the infection and supportive care rather than drug withdrawal. [5]
Epidemiology & Risk Factors
Stevens-Johnson syndrome and toxic epidermal necrolysis are rare but not vanishingly so — the estimated incidence is of the order of one to two cases per million people per year in children, rising in adults, with no clear sex predominance. They account for the bulk of severe cutaneous adverse drug reactions seen in tertiary paediatric centres, and the burden is concentrated in the weeks after a new medicine is started. The single strongest risk factor is therefore a recently introduced drug, typically one to eight weeks before onset, and a careful drug history is the highest-yield investigation in any suspected case. [2] [6]
The pooled analysis of medications as risk factors in children identified a defined set of high-risk drug classes. The commonest culprits in paediatric practice are the aromatic anticonvulsants (carbamazepine, lamotrigine, phenytoin and phenobarbital), sulfonamide antibiotics (sulfamethoxazole-trimethoprim), allopurinol, nevirapine and, in some series, aminopenicillins and cephalosporins and the oxicam non-steroidal anti-inflammatories. Allopurinol emerged as the single most frequent cause of SJS and TEN in the large European and Israeli case-control series, a finding that has reshaped how the drug is initiated, especially in older children and those with renal impairment. [2] [6]
In Australia and Aotearoa New Zealand, and across the broader Asia-Pacific, the HLA pharmacogenetic associations are clinically central because they track population ancestry. HLA-B*15:02 confers a strong risk of carbamazepine-induced SJS/TEN and is common in Han Chinese, Thai, Malay, Filipino and Indonesian populations; pre-prescription HLA screening before carbamazepine is recommended in at-risk groups and is embedded in many regional formularies. HLA-B*58:01 confers a strong risk of allopurinol-induced SJS/TEN. Aboriginal, Torres Strait Islander, Maori, Pasifika, South-East Asian and South Asian children presenting with a new blistering mucocutaneous reaction should have both their recent drug history and their pharmacogenetic risk considered together. [4] [3]
The host risk factors beyond the drug are a reactive immune system and, in some cases, active infection or immune activation. Children with concomitant Mycoplasma pneumoniae infection are over-represented in the MIRM subgroup. Slow acetylator status, renal impairment (relevant to allopurinol dosing) and co-existing viral infection such as Epstein-Barr virus or HIV are described cofactors. In infants under twelve months the disease is rare but carries a high mortality, and the culprits and clinical features differ in proportion from older children. [7] [5]
Pathophysiology
Why does a medicine a child has taken for weeks suddenly begin to kill their epidermis? The answer is a drug-specific, cell-mediated immune attack that drives widespread keratinocyte death through a small family of cytotoxic molecules. The reaction is a type IV, delayed hypersensitivity process dominated by drug-specific CD8-positive cytotoxic T lymphocytes that infiltrate the epidermis and release effector molecules against keratinocytes presenting the offending drug or its metabolite. [12] [9]
The mechanism is pharmacogenetically shaped. The culprit drug or its reactive metabolite interacts with the peptide-binding groove of a specific HLA class I molecule and is presented to T cells, which explains why particular HLA alleles confer dramatic risk for particular drugs. The landmark discovery was HLA-B*15:02 as a strong predictor of carbamazepine-induced SJS in Han Chinese, a finding that introduced HLA screening into prescribing. The European study extended the pharmacogenetic map to five high-risk drugs and confirmed that the association is drug-specific rather than a general SJS susceptibility. [4] [3]
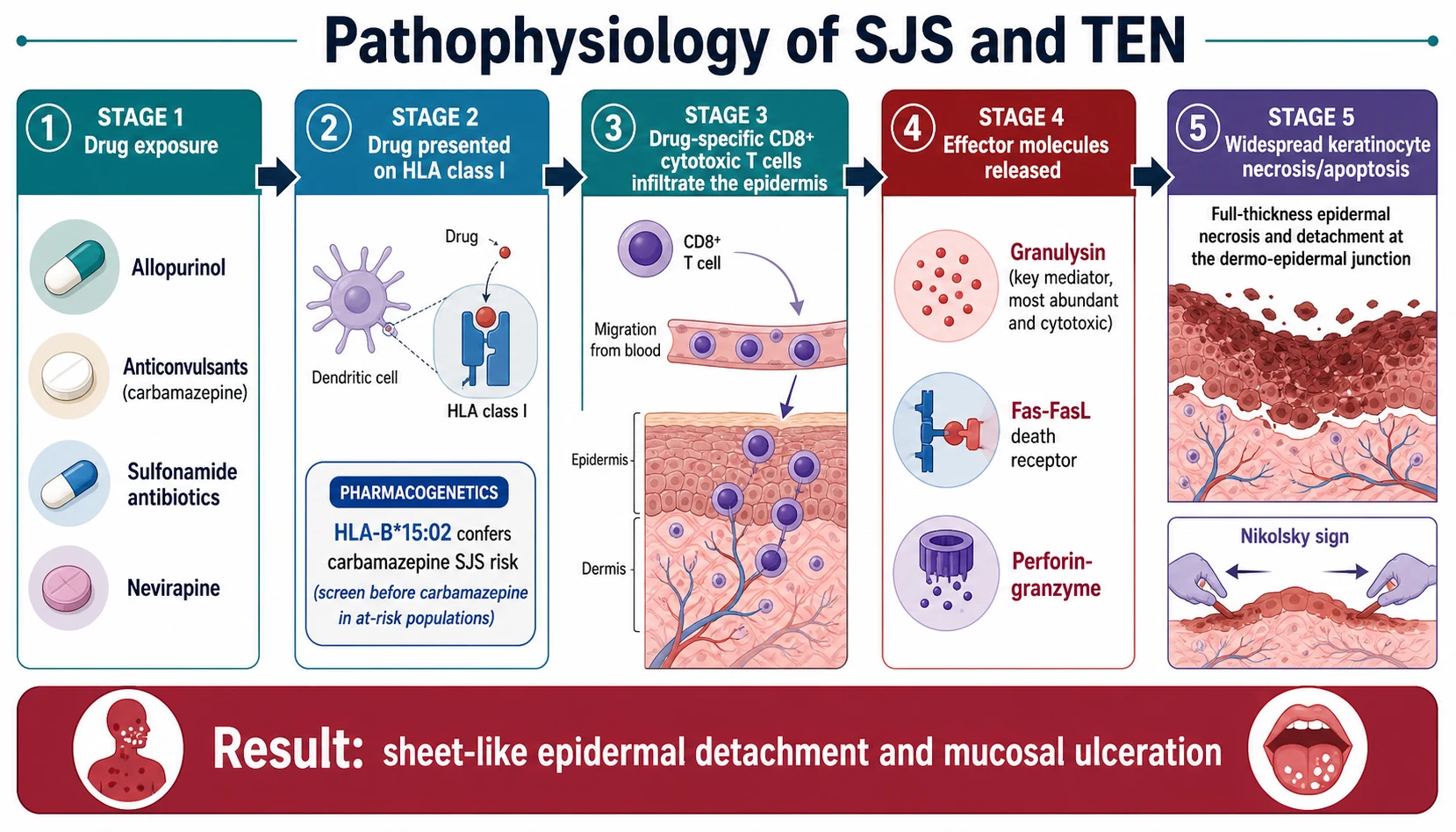
The effector molecules do the killing, and of these granulysin is the key mediator. Granulysin, released by cytotoxic T cells and natural killer cells, is the most abundant and most cytotoxic of the molecules found in early SJS/TEN blister fluid, far exceeding perforin and the soluble Fas ligand. The Fas-FasL death-receptor pathway and the perforin-granzyme pathway also contribute to keratinocyte apoptosis and necrosis. The net effect is full-thickness necrosis of the epidermis at the dermo-epidermal junction, leaving a denuded dermis that weeps, loses heat and water, and is vulnerable to infection and to the adhesions and scarring that ruin the ocular surface. [12]
Two consequences follow that examiners test. First, the necrosis is full-thickness but the split is at the dermo-epidermal junction, so the dermis and its appendages survive — which is why the skin can re-epithelialise from hair follicles and why debridement is contraindicated. Second, the mucosae are involved, because the same cytotoxic attack targets mucosal epithelium, which is the bedside and pathological feature that separates SJS/TEN from staphylococcal scalded skin syndrome where mucosae are spared. [12] [5]
Clinical Presentation
The presentation unfolds in a recognisable sequence that begins days before the skin blisters. A one-to three-day prodrome of fever, malaise, upper-respiractory symptoms and stinging or burning eyes is followed by the abrupt appearance of skin lesions and mucositis. The prodrome is easily mistaken for a viral illness or an evolving drug reaction, and the index of suspicion must rise whenever a child on a new medicine develops unexplained fever and sore eyes. [6] [2]
The skin lesions are the signature. Atypical target lesions — dusky, purpuric macules, sometimes with a central blister, that lack the neat three rings of classic erythema multiforme — appear first, often on the trunk and proximal limbs, and coalesce. Flaccid, easily ruptured bullae form on confluent erythematous skin, and within hours to days the epidermis detaches, leaving moist, erythematous, painful denuded dermis. Gentle lateral pressure shears the epidermis (a positive Nikolsky sign). Detachment of less than 10 percent of body surface area is SJS, 10 to 30 percent is overlap, and more than 30 percent is TEN. [1] [12]
The mucositis drives much of the acute morbidity. Ocular involvement — conjunctival hyperaemia, erosions, pseudomembrane formation and corneal epithelial defects — is present in most children and is the single most important determinant of long-term disability, because inflammation and adhesions (symblepharon) progress to dry eye, corneal scarring and visual loss if untreated. Oral involvement causes pain, crusting and bleeding, prevents eating and drinking, and risks airway compromise when severe. Urogenital involvement produces dysuria, erosions and later urethral stricture. Respiratory and gastrointestinal epithelial involvement occurs in severe disease and worsens prognosis. [10] [7]
The Mycoplasma-induced form presents differently. After a respiratory prodrome with cough and fever, a child develops prominent mucositis at two or more sites — especially the mouth and eyes — with sparse or absent skin lesions, in contrast to the widespread detachment of drug-induced TEN. The systematic review found a median age in the second decade, frequent recurrence, and a markedly better prognosis than drug-induced SJS, though ocular sequelae still occur. [5]
Differential Diagnosis
The first fork is whether the blistering is toxin-mediated or immune-mediated. Staphylococcal scalded skin syndrome is the dangerous mimic in the neonate and young infant, caused by circulating exfoliative toxin that cleaves desmoglein-1 in the superficial granular layer. The split is superficial, the mucosae are spared, and the child has a staphylococcal focus rather than a new drug. Getting this distinction right changes everything: SSSS needs intravenous anti-staphylococcal therapy, while SJS/TEN needs drug withdrawal and burns-style care. [12] [5]
The second fork is within the immune-mediated blistering and target-lesion group. Erythema multiforme major produces classic three-zone target lesions, often on the extremities, with milder mucositis and is usually infection-related (herpes simplex, Mycoplasma); it runs a recurrent, generally benign course and is not the same disease as SJS. Staphylococcal scalded skin syndrome and toxic shock syndrome with desquamation are considered when a toxin source is plausible. Drug reaction with eosinophilia and systemic symptoms (DRESS) is delayed (two to eight weeks), has an erythematous rather than necrotic rash, eosinophilia and organ involvement, and rarely blisters. [5] [9]
In the neonate and infant the inherited blistering disorders enter the differential. Epidermolysis bullosa, especially the junctional and severe generalised junctional forms, presents from birth with blistering at sites of friction, but without the target lesions, mucosal pattern and drug tempo of SJS. The infantile SJS/TEN systematic review emphasises that SJS and TEN can occur in infants under twelve months — anticonvulsants and antibiotics are the usual culprits — and that the threshold to suspect and treat is low even though the disease is rare in this age group. [7]
Clinical & Bedside Assessment
The assessment begins with a focused history aimed at the drug, the timing and the system involvement. Ask about every medicine started in the previous one to eight weeks, including over-the-counter, herbal and intermittent agents, and note the date of onset of the prodrome relative to each. Ask about preceding respiratory illness (pointing to Mycoplasma), about eye, mouth and urinary symptoms, and about systemic upset. A complete and dated drug history is the single most useful bedside investigation and drives both the diagnosis and the counselling. [6] [2]
Examine the whole skin and all mucosae. Describe the primary lesion (atypical target, bulla, denudation), the percentage of body-surface-area detached, the presence of a Nikolsky sign, and the number and severity of mucosal sites involved. Examine the eyes carefully — conjunctival injection, erosion, pseudomembrane or corneal defect — and record the findings, because the ocular examination on day one sets the baseline for the ophthalmologist. Document oral, urogenital and, where feasible, respiratory involvement. [10] [1]
Assess severity directly with the SCORTEN variables. Record heart rate, the percentage of body-surface-area detached, serum urea, bicarbonate and glucose, age, and any active malignancy, so that the score can be calculated on day one and re-checked on day three. Tachycardia over 120, detachment over 10 percent, a rising urea or a falling bicarbonate are the markers that move a child toward the burn unit or PICU. Assess hydration, temperature control, pain and the airway, because extensive skin loss behaves like a burn and demands the same supportive discipline. [1] [8]
Document the public-health and safety essentials at the bedside. Record the suspected culprit drug, the family drug-allergy history, and the child's ancestry and HLA-screening status where relevant, because these drive the avoidance advice, the MedicAlert and the pharmacogenetic counselling. A complete and forward-looking record at the first encounter prevents the late realisation that a culprit drug was missed or that an at-risk relative is about to receive it. [4] [3]
Investigations
There is no single confirmatory blood test for SJS or TEN. The diagnosis is clinical, built from the temporal relationship to a drug, the morphology of the lesions, the extent of detachment and the pattern of mucosal involvement. The role of investigation is to confirm the severity, exclude mimics, identify the culprit and screen for complications — not to delay drug withdrawal and supportive care. [10] [6]
The core blood panel supports SCORTEN and screens for organ involvement: full blood count, urea, electrolytes, bicarbonate, glucose, liver function, C-reactive protein and blood cultures when sepsis is suspected. Serum urea over 10 mmol per litre, bicarbonate under 20 mmol per litre and glucose over 14 mmol per litre are SCORTEN variables, so they must be measured on day one. Skin swabs and blood cultures guide only the management of suspected secondary infection — prophylactic antibiotics are not given. [1] [8]
A skin biopsy is reserved for the genuinely ambiguous case where the differential between SJS/TEN, staphylococcal scalded skin syndrome and another blistering disorder cannot be settled clinically. Histopathology shows full-thickness epidermal necrosis with detachment at the dermo-epidermal junction and a sparse inflammatory infiltrate, in contrast to the superficial granular-layer split of SSSS. In a classic drug-induced presentation with a clear culprit and characteristic morphology, treatment must not wait for biopsy. [12] [5]
SCORTEN — seven risk factors (1 point each, scored on day 1 and re-checked day 3)
Drug patch testing and in-vitro assays have a role, but only after the acute episode has settled. Patch testing can help confirm the culprit when several drugs overlap, and a systematic review confirms its place in selected cases with the highest yield for anticonvulsants and some antibiotics. It is performed weeks to months after recovery and never during the acute illness, because re-challenge in the acute phase can be fatal. [11]
Management — Resuscitation
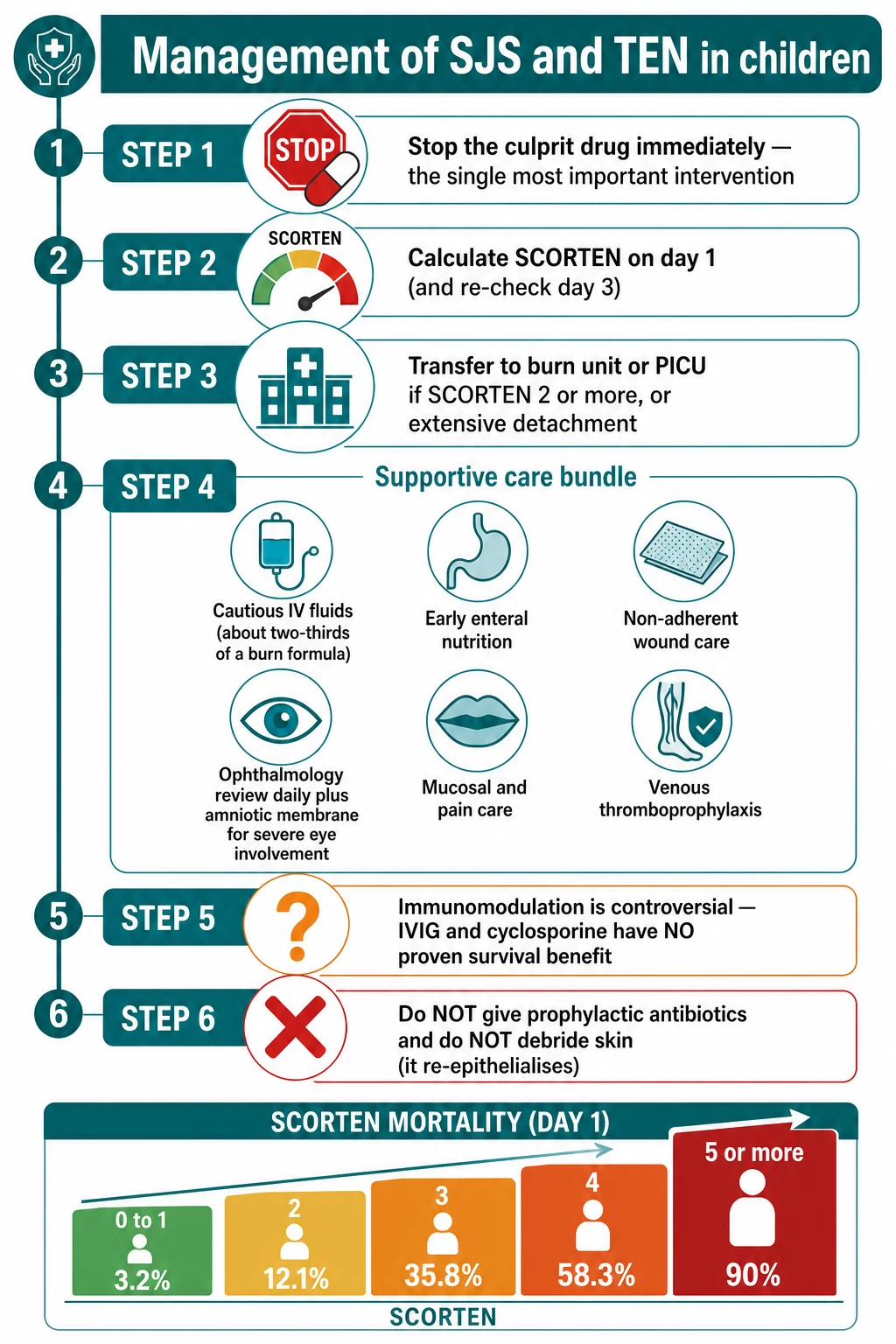
Resuscitation belongs to the sick, blistering child, and in SJS and TEN the first resuscitation act is the simplest and the most powerful: stop the culprit drug immediately. The case-control evidence is that earlier withdrawal of the offending drug is associated with better survival, and a continued drug exposure keeps driving keratinocyte necrosis. Withdraw every non-essential medicine started in the previous two months, treat the suspected culprit as guilty until proven innocent, and document the withdrawal and the reason in the chart and the discharge summary. [6] [9]
The second resuscitation act is to grade severity and choose the setting. Calculate SCORTEN on day one and re-check on day three, and admit to a burn unit or PICU when the score is 2 or more, the detachment is extensive (over 10 percent of body surface area), or there is airway, fluid, electrolyte or eye compromise. Children with extensive TEN behave like major burns: they lose fluid, electrolytes and heat, they are at risk of sepsis and thrombosis, and they need the monitoring and wound-care expertise of a burn-capable centre. Retrieval should be mobilised early for the deteriorating child. [1] [8]
The supportive bundle is the core of management and is where outcomes are won or lost. Give cautious intravenous fluid resuscitation, recognising that SJS/TEN generally needs about two-thirds of the volume calculated for a thermal burn of the same area to avoid fluid overload. Provide early enteral nutrition wherever possible, because the catabolic stress is high and the gut usually works. Apply non-adherent wound care with appropriate dressings, treat pain aggressively, give venous thromboprophylaxis, and monitor for secondary infection with targeted — not prophylactic — antibiotics. [10] [9]
The eye is the priority within the supportive bundle. Involve ophthalmology within hours of suspected SJS or TEN, because untreated ocular inflammation progresses within days to symblepharon, corneal scarring and irreversible visual loss. Daily ophthalmology review, preservative-free lubricants, topical antibiotics, lysis of early adhesions and, for severe disease, amniotic membrane transplantation in the first few days all reduce the long-term ocular burden. The child who survives TEN but loses their sight has not been well managed, and protecting the ocular surface is the difference between a good and a poor long-term outcome. [10] [7]
Management — Definitive & Stepwise
Definitive management is a stepwise pathway built on drug withdrawal and burns-grade supportive care, with immunomodulation reserved as an uncertain adjunct. The art is to do the things that work — stop the drug, support the child, protect the eye — and to resist the temptation to substitute an unproven immunomodulator for sound supportive care. [9] [10]
The first four steps are non-negotiable. Stop the culprit drug and all non-essential recent medicines. Calculate SCORTEN on day one and again on day three to guide setting and prognosis. Escalate to a burn unit or PICU for a score of 2 or more, extensive detachment, or airway, fluid or eye compromise. Deliver the supportive bundle — cautious fluids at about two-thirds of a thermal-burn formula, early enteral nutrition, non-adherent wound care, analgesia, thromboprophylaxis, and targeted antibiotics only for proven infection. [1] [10]
The mucosae need structured care alongside the skin and the eye. Oral care with antiseptic and analgesic mouthwashes and soft diet or nasogastric feeding maintains nutrition and comfort. Urogenital care with topical emollients, sterile urethral catheterisation for severe involvement, and early urology input reduces the risk of stricture. Respiratory and airway involvement demands humidified oxygen, physiotherapy and, in the rare child with epiglottic or bronchial epithelial necrosis, anaesthetic and intensive-care support. Each surface is managed on its own terms. [10] [7]
The stepwise SJS-TEN pathway
Recognise the reaction: a new drug within one to eight weeks, atypical target lesions, detachment and mucositis at two or more sites.
Stop the culprit drug immediately and withdraw all non-essential recent medicines.
Calculate SCORTEN on day one and re-check on day three; assess hydration, temperature, airway and pain.
Escalate to a burn unit or PICU if SCORTEN is two or more, detachment is over 10 percent body surface area, or there is airway, fluid or eye compromise.
Deliver the supportive bundle: cautious fluids at about two-thirds of a burn formula, early enteral nutrition, non-adherent wound care, analgesia, thromboprophylaxis.
Involve ophthalmology within hours; daily review, lubricants, topical antibiotics, amniotic membrane transplantation for severe ocular involvement.
Manage mucosae: oral hygiene and nutrition, urogenital care with catheterisation if needed, airway support for respiratory epithelial involvement.
Avoid prophylactic antibiotics and avoid skin debridement; use targeted antibiotics only for proven infection.
Consider immunomodulation (IVIG, cyclosporine, corticosteroids) as unproven and controversial; do not let it delay supportive care.
Plan long-term follow-up: ocular surveillance, skin and nail sequelae, drug avoidance, MedicAlert, HLA pharmacogenetic screening and family counselling.
The immunomodulation decision is the one most often mis-handled by candidates. The systematic review and meta-analysis of systemic immunomodulating therapies — covering intravenous immunoglobulin, corticosteroids, cyclosporine and other agents — found no convincing evidence of a survival benefit for any of them, with heterogeneous and conflicting trial results. IVIG, often dosed at 1 gram per kilogram per day for three days, is still used in some centres but cannot be regarded as standard of care. Cyclosporine has shown some signal in smaller studies. Corticosteroids are associated in some series with increased sepsis and delayed healing. The honest position is that supportive care is the standard and immunomodulation is an uncertain adjunct discussed with the burns or intensive-care team. [9]
Two interventions must be explicitly avoided. Prophylactic systemic antibiotics are not given, because they do not prevent infection and drive resistance; antibiotics are reserved for proven or strongly suspected secondary infection, guided by cultures. Surgical debridement of the skin is contraindicated, because the dermis and its appendages survive the full-thickness epidermal necrosis and the skin re-epithelialises from follicular stems; debridement destroys that regenerative capacity. [10] [9]
Specific Subtypes & Scenarios
A school-age child on carbamazepine with target lesions and mucositis. This is the classic drug-induced SJS presentation. Stop the carbamazepine immediately, calculate SCORTEN, involve ophthalmology, and admit to a burn-capable setting if detachment exceeds 10 percent of body surface area or the score is 2 or more. Counsel the family on lifelong carbamazepine avoidance, cross-reactive aromatic anticonvulsant avoidance (oxcarbazepine, phenytoin, lamotrigine), MedicAlert identification, and HLA-B*15:02 screening of at-risk relatives before any aromatic anticonvulsant is given. [4] [3]
An adolescent with extensive TEN from allopurinol. Allopurinol is the single most frequent culprit in European and Israeli series and produces severe disease. Stop the drug, deliver full burns-grade supportive care in a burn unit or PICU, calculate SCORTEN (expect a high score with extensive detachment), protect the eye with amniotic membrane transplantation if needed, and screen for the HLA-B*58:01 association and counsel family members. Renal impairment at the time allopurinol was started is a recognised cofactor, and a low starting dose with renal-function-based dosing reduces risk. [6] [9]
A child with Mycoplasma-induced rash and mucositis (MIRM). The picture is striking mucositis at two or more sites — mouth, eyes, urogenital — with sparse skin lesions, following a respiratory illness. There is no culprit drug to stop, so management centres on treating the Mycoplasma infection where indicated, supportive mucosal and eye care, and pain control. The prognosis is better than drug-induced SJS, but ocular sequelae still occur and ophthalmology involvement is essential. Recurrence is described and the family should be warned. [5]
An infant under twelve months with blistering and mucositis. Infantile SJS and TEN are rare but real, and the systematic review of children aged twelve months and under found antibiotics and anticonvulsants to be the usual culprits, with a high mortality. The threshold to suspect, stop medicines, biopsy if ambiguous and admit is low. Distinguishing SJS from staphylococcal scalded skin syndrome (mucosae spared) and from inherited epidermolysis bullosa (friction blisters from birth, no target lesions) is critical. [7]
An indigenous or South-East-Asian child needing an anticonvulsant. The pharmacogenetic risk is central here. HLA-B*15:02 screening before carbamazepine is recommended in populations of Han Chinese, Thai, Malay, Filipino and Indonesian ancestry and is increasingly embedded in regional formularies. A child who has survived carbamazepine-induced SJS must never receive carbamazepine again, and cross-reactive aromatic anticonvulsants are avoided, with levetiracetam or valproate often chosen instead. The prescribing decision is a pharmacogenetic decision as much as a seizure-control one. [4] [3]
Complications & Pitfalls
The most important complication is ocular sequelae, the commonest and most disabling long-term burden of SJS and TEN. Untreated ocular inflammation progresses to symblepharon, dry eye, corneal neovascularisation and scarring, and ultimately to visual impairment or blindness, and these changes can develop within the first few days. Early and sustained ophthalmology involvement, preservative-free lubricants, lysis of adhesions and amniotic membrane transplantation for severe disease reduce the burden; late corneal rehabilitation is difficult and often unsatisfactory, so prevention in the acute phase is everything. [10] [7]
The cardinal pitfall is failure to recognise the reaction early and to stop the culprit drug. A clinician who treats the fever and the rash with a new or continuing antibiotic, who attributes the sore eyes to conjunctivitis, or who waits for a biopsy before withdrawing a clearly implicated drug has delayed the single most effective intervention. The drug history is the diagnosis, and the response to withdrawal is part of the management. [6] [9]
A second pitfall is over-reliance on immunomodulation at the expense of supportive care. IVIG, cyclosporine and corticosteroids are commonly reached for, but the meta-analysis shows no convincing survival benefit, and corticosteroids may increase sepsis. The clinician who administers a high-dose immunomodulator but under-resuscitates the child, under-protects the eye or leaves a culprit drug running has mistaken the theatre for the play. Supportive care is the standard. [9]
A third pitfall is fluid overload from applying a full thermal-burn formula. The detached epidermis in SJS/TEN loses less fluid than a deep dermal burn, and children given full burn-fluid volumes develop pulmonary and tissue oedema. The taught principle is about two-thirds of the burn-calculated volume, titrated to perfusion and urine output, and re-assessed frequently. [10] [8]
A fourth pitfall is debriding the skin or giving prophylactic antibiotics. The skin re-epithelialises from surviving follicular stems, so debridement destroys regenerative capacity; prophylactic antibiotics do not prevent infection and select resistant organisms. The detached skin is dressed, not removed, and antibiotics are targeted to proven infection. [10]
A fifth pitfall is misclassifying MIRM as drug-induced SJS and attributing it to a medicine the child needs. Mycoplasma-induced rash and mucositis is infection-triggered, drug-independent and carries a better prognosis; over-attributing it to a drug leads to the unnecessary lifelong avoidance of a needed medicine and to family anxiety. The respiratory prodrome, prominent mucositis and sparse skin lesions point to MIRM. [5]
The final pitfall is failing to counsel the family on lifelong avoidance and screening. A child who has had SJS or TEN must never receive the culprit drug again, cross-reactive agents are identified, MedicAlert identification is arranged, and at-risk relatives are offered HLA pharmacogenetic screening where relevant. The acute admission is also the start of a lifelong prescribing-safety conversation. [4] [11]
Prognosis & Disposition
Prognosis is driven by SCORTEN and by the quality of supportive care. The original SCORTEN derivation gave a mortality of about 3 percent at a score of 0 to 1, 12 percent at 2, 36 percent at 3, 58 percent at 4, and 90 percent at 5 or more, and the RegiSCAR validation confirmed the score's calibration in a large cohort. Children generally do better than adults — the age and malignancy points are usually absent — but extensive detachment, tachycardia and metabolic derangement mark the children who do poorly. [1] [8]
Disposition follows severity. Admit to a burn unit or PICU for SCORTEN of 2 or more, detachment over 10 percent of body surface area, or any airway, fluid, electrolyte or ocular compromise. Manage the milder SJS case (limited detachment, normal SCORTEN, no eye involvement) on a paediatric ward with close monitoring and early ophthalmology input. The threshold to escalate is deliberately low, because the disease can progress within hours. [8] [10]
At discharge, complete the avoidance advice, arrange MedicAlert identification, document the culprit drug and the reaction in the chart and the patient record, and give the family a clear safety-net for return — fever, increasing pain, eye symptoms, reduced urine output or new detachment. Arrange ophthalmology follow-up from weeks to months regardless of apparent ocular recovery, because late ocular complications develop silently. Reinforce the pharmacogenetic screening of at-risk relatives. [4] [10]
Long-term sequelae are common and multisystem. Ocular dryness, scarring and visual impairment dominate; skin pigmentation change and nail dystrophy are frequent; mucosal strictures (urethral, oesophageal) and chronic oral erosions occur; and psychological sequelae are under-recognised. The systematic review of infantile disease confirms that even the youngest survivors carry a substantial long-term burden, and structured follow-up across dermatology, ophthalmology and psychology is part of the standard of care. [7]
Special Populations
Infants under twelve months carry a disproportionate mortality relative to their disease frequency. The infantile systematic review found antibiotics and anticonvulsants to be the usual culprits, a high case fatality, and the need to distinguish SJS from staphylococcal scalded skin syndrome and inherited epidermolysis bullosa. The threshold to admit, biopsy if ambiguous and deliver burns-grade care is low. [7]
Children with epilepsy on anticonvulsants are the classic paediatric risk group, because the aromatic anticonvulsants — carbamazepine, lamotrigine, phenytoin, phenobarbital — are common culprits and cross-react. A child who has had an anticonvulsant-induced SJS must avoid that drug and structurally related agents, with levetiracetam or valproate often chosen for ongoing seizure control, and HLA-B*15:02 screening considered for at-risk relatives before carbamazepine is prescribed. [4] [2]
Immunocompromised children — those with HIV on nevirapine, post-transplant on sulfonamides, or on chemotherapy — carry both higher exposure to culprit drugs and altered immune function, and warrant a high index of suspicion and rapid drug withdrawal. Nevirapine-induced SJS is well described in HIV care, and the choice and monitoring of antiretrovirals in a child who has reacted is specialist-led. [2] [9]
Indigenous, South-East Asian and South Asian children carry the HLA pharmacogenetic associations that should shape prescribing. HLA-B*15:02 screening before carbamazepine and HLA-B*58:01 awareness before allopurinol are part of safe prescribing in these populations, and culturally safe, family-centred counselling — using interpreters where needed — supports adherence to lifelong avoidance and screening. [4] [3]
Children in rural and remote settings need pathways that work where they live. Early recognition, immediate drug withdrawal, and retrieval to a burn-capable centre are the pre-hospital priorities, and telehealth with dermatology and ophthalmology can support the referring clinician while retrieval is mobilised. The skin and eye do not wait for geography, and the first hours of care often determine the long-term outcome. [10]
Evidence, Guidelines & Regional Differences
The severity-scoring evidence is anchored by the original SCORTEN derivation, which built and validated a seven-factor score for TEN mortality, and by the RegiSCAR validation cohort, which confirmed the score's calibration across the SJS-TEN spectrum. Together they established the day-one and day-three SCORTEN calculation that now structures triage and prognostic counselling worldwide. [1] [8]
SCORTEN derivation (Bastuji-Garin et al.)
Population: Patients with toxic epidermal necrolysis, from whom seven independent prognostic factors were derived and a severity score (SCORTEN) was built and validated against observed mortality.
Key finding
Seven factors — age over 40, malignancy, heart rate over 120, detachment over 10 percent body surface area, urea over 10 mmol per litre, bicarbonate under 20 mmol per litre and glucose over 14 mmol per litre — each added one point and stratified mortality from about 3 percent (score 0 to 1) to 90 percent (score 5 or more).
Practice change
SCORTEN is the standard severity score for SJS and TEN, calculated on day one and re-checked on day three, and it drives triage to a burn-capable or intensive-care setting and the prognostic conversation with the family.
The culprit-drug evidence reshaped prescribing. The EuroSCAR case-control series established allopurinol as the single most frequent cause of SJS and TEN in Europe and Israel, and the pooled analysis of medications as risk factors in children quantified the paediatric culprit profile — anticonvulsants, sulfonamides, allopurinol and nevirapine to the fore. These findings underpin the modern emphasis on a careful drug history and the principle that the commonest culprit is the one started most recently. [6] [2]
EuroSCAR — allopurinol as the leading culprit
Population: A multinational European and Israeli case-control study of Stevens-Johnson syndrome and toxic epidermal necrolysis, comparing drug exposures in cases and controls.
Key finding
Allopurinol was the single most frequent cause of SJS and TEN, with the risk concentrated in patients started on standard rather than renal-function-adjusted doses.
Practice change
Allopurinol initiation should use a low, renal-function-adjusted starting dose, and HLA-B*58:01 screening is considered in at-risk populations before its use.
The pharmacogenetic evidence transformed prevention. The discovery of HLA-B*15:02 as a strong predictor of carbamazepine-induced SJS introduced HLA screening into prescribing, and the European five-drug study extended the map. The drug patch-testing systematic review confirms a role for confirming the culprit in selected, recovered patients, with the highest yield for anticonvulsants and antibiotics. [4] [11]
The treatment evidence is sobering. The systematic review and meta-analysis of systemic immunomodulating therapies — IVIG, corticosteroids, cyclosporine and others — found no convincing survival benefit for any agent, with heterogeneous and conflicting results across trials. This is why supportive care remains the standard and immunomodulation an uncertain adjunct. [9]
Immunomodulating therapies meta-analysis (Zimmermann et al.)
Population: A systematic review and meta-analysis of systemic immunomodulating therapies — including intravenous immunoglobulin, corticosteroids and cyclosporine — for Stevens-Johnson syndrome and toxic epidermal necrolysis.
Key finding
Across heterogeneous studies, no immunomodulating therapy showed a convincing survival benefit; corticosteroids were associated in some analyses with increased sepsis and adverse outcomes.
Practice change
Supportive care — drug withdrawal, burns-grade fluid and wound care, eye protection and nutrition — remains the standard of care; immunomodulation is an uncertain adjunct to be discussed with the burns or intensive-care team, not a substitute.
The paediatric and infantile evidence fills in the age-specific picture. The Mycoplasma-induced rash and mucositis systematic review defined MIRM as a distinct, infection-triggered syndrome with prominent mucositis, sparse skin lesions and a better prognosis, and the infantile SJS/TEN review confirmed that the disease occurs in the first year of life with a high mortality and a substantial long-term burden. [5] [7]
The regional policy structure is consistent in principle. The guideline mapping systematic review synthesised the many national and society guidelines and found broad consensus on drug withdrawal, SCORTEN, burn-unit or PICU supportive care, ophthalmology involvement and the avoidance of prophylactic antibiotics and debridement, with persistent uncertainty on immunomodulation. In the UK, NICE and the Clinical Knowledge Summaries set the recognition and referral pathway. In Australia and New Zealand, the Royal Children's Hospital Melbourne guideline and Therapeutic Guidelines set the regional standard, with HLA pharmacogenetic screening embedded where relevant. In the US and Canada, burn-society and dermatology guidance mirror the supportive-care-centred approach. In every region the principle is the same: stop the drug, score the severity, support the child like a burn, and protect the eye. [10]
The controversies are real and active: the uncertain role of IVIG, cyclosporine and corticosteroids; the optimal timing and technique of amniotic membrane transplantation; the cost-effectiveness and reach of HLA screening; and the long-term rehabilitation of the ocular surface. The defence against each is the same: early recognition and drug withdrawal, severity scoring with SCORTEN, burns-grade supportive care, early ophthalmology, and a lifelong prescribing-safety and pharmacogenetic plan for the survivor and their family. [9] [10]
Exam Pearls
- Stevens-Johnson syndrome and toxic epidermal necrolysis are a single severe, usually drug-induced mucocutaneous reaction defined by full-thickness epidermal necrosis and detachment, classified as SJS (less than 10 percent BSA), overlap (10 to 30 percent) and TEN (more than 30 percent). [1]
- The defining features are atypical target lesions, a positive Nikolsky sign, and mucositis at two or more sites (eyes, mouth, urogenital). [12]
- The single most important action is to stop the culprit drug immediately — earlier withdrawal improves survival. [6]
- The common paediatric culprits are anticonvulsants (carbamazepine, lamotrigine, phenytoin), sulfonamides, allopurinol and nevirapine; allopurinol is the leading culprit in European series. [2] [6]
- The pharmacogenetic associations are HLA-B*15:02 with carbamazepine and HLA-B*58:01 with allopurinol; screen at-risk populations before prescribing. [4] [3]
- SCORTEN has seven one-point factors — age over 40, malignancy, heart rate over 120, detachment over 10 percent BSA, urea over 10 mmol/L, bicarbonate under 20 mmol/L, glucose over 14 mmol/L — scored on day one and re-checked on day three. [1]
- SCORTEN mortality rises from about 3 percent at 0 to 1, to 12 percent at 2, 36 percent at 3, 58 percent at 4 and 90 percent at 5 or more. [1] [8]
- The key pathogenetic mediator is granulysin, with Fas-FasL and perforin-granzyme contributing; CD8-positive T cells infiltrate the epidermis. [12]
- Management is burn-unit or PICU supportive care: cautious fluids at about two-thirds of a burn formula, enteral nutrition, non-adherent wound care, daily ophthalmology, amniotic membrane for severe eye disease, mucosal and pain care, thromboprophylaxis. [10]
- IVIG, cyclosporine and corticosteroids have no proven survival benefit; supportive care is the standard. [9]
- Do not give prophylactic antibiotics and do not debride the skin — the skin re-epithelialises from surviving follicular stems. [10]
- Ocular sequelae are the commonest and most disabling complication — involve ophthalmology within hours. [7]
- Mycoplasma-induced rash and mucositis (MIRM) is infection-triggered, with prominent mucositis and sparse skin lesions, and a better prognosis than drug-induced SJS. [5]
References
- [1]Bastuji-Garin S; Fouchard N; Bertocchi M; Roujeau JC; et al SCORTEN: a severity-of-illness score for toxic epidermal necrolysis. J Invest Dermatol, 2000.PMID 10951229
- [2]Levi N; Bastuji-Garin S; Mockenhaupt M; Roujeau JC; et al Medications as risk factors of Stevens-Johnson syndrome and toxic epidermal necrolysis in children: a pooled analysis. Pediatrics, 2009.PMID 19153164
- [3]Lonjou C; Borot N; Sekula P; Ledger N; et al A European study of HLA-B in Stevens-Johnson syndrome and toxic epidermal necrolysis related to five high-risk drugs. Pharmacogenet Genomics, 2008.PMID 18192896
- [4]Chung WH; Hung SI; Hong HS; Hsih MS; et al Medical genetics: a marker for Stevens-Johnson syndrome. Nature, 2004.PMID 15057820
- [5]Canavan TN; Mathes EF; Frieden I; Shinkai K Mycoplasma pneumoniae-induced rash and mucositis as a syndrome distinct from Stevens-Johnson syndrome and erythema multiforme: a systematic review. J Am Acad Dermatol, 2015.PMID 25592340
- [6]Halevy S; Ghislain PD; Mockenhaupt M; Fagot JP; et al Allopurinol is the most common cause of Stevens-Johnson syndrome and toxic epidermal necrolysis in Europe and Israel. J Am Acad Dermatol, 2008.PMID 17919772
- [7]Iriarte C; Karim SA; Nassim JS; Grenier PO; et al Infantile Stevens Johnson syndrome and toxic epidermal necrolysis: A systematic review of clinical features and outcomes in children ages 12 months and under. Pediatr Dermatol, 2022.PMID 35676891
- [8]Sekula P; Liss Y; Davidovici B; Dunant A; et al Evaluation of SCORTEN on a cohort of patients with Stevens-Johnson syndrome and toxic epidermal necrolysis included in the RegiSCAR study. J Burn Care Res, 2011.PMID 21228709
- [9]Zimmermann S; Sekula P; Venhoff M; Motschall E; et al Systemic Immunomodulating Therapies for Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Systematic Review and Meta-analysis. JAMA Dermatol, 2017.PMID 28329382
- [10]AlFada M; Alotaibi H; Alsharif S; Alani AH; et al Systematic review, methodological appraisal, and recommendation mapping of clinical practice guidelines for managing patients with Stevens-Johnson syndrome and toxic epidermal necrolysis. J Dermatolog Treat, 2025.PMID 40010698
- [11]Novack DE; Braskett M; Worswick SD; Adler BL Drug patch testing in Stevens-Johnson syndrome and toxic epidermal necrolysis: A systematic review. Ann Allergy Asthma Immunol, 2023.PMID 36649833
- [12]Chung WH; Hung SI Recent advances in the genetics and immunology of Stevens-Johnson syndrome and toxic epidermal necrosis. J Dermatol Sci, 2012.PMID 22541332