Paeds · paediatric-dermatology
Tinea and fungal skin infection
Also known as Tinea · Dermatophytosis · Ringworm · Tinea capitis · Kerion
Fellowship guide to tinea and fungal skin infection in children: the annular scaly ringworm plaque of tinea corporis with its active advancing border, the prepubertal bald scaly patch of tinea capitis and the boggy inflammatory kerion, the black-dot and ectothrix or endothrix hair invasion, confirmation by potassium hydroxide (KOH) microscopy showing branching septate hyphae and by Wood's lamp green fluorescence for Microsporum, the species-specific oral therapy of tinea capitis with griseofulvin (favoured for Microsporum) versus weight-banded terbinafine (favoured for Trichophyton), the topical treatment of corporis, cruris and pedis, kerion management with an oral antifungal and corticosteroid without incision, household carrier screening and pet source control, and the emerging terbinafine-resistant Trichophyton indotineae.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the seven-year-old who itches at an expanding pink ring on her forearm. The edge is raised and scaly, the centre has cleared, and over two weeks it has slowly grown outward. This is tinea corporis, the archetypal ringworm lesion, and the pattern of an active advancing border with central clearing is the single most useful clue that a scaly patch is fungal rather than eczema or psoriasis. [6]
Now picture a different child: a four-year-old with a patch of hair loss and broken-off stubs on his scalp, a little scaly, with a firm lump of enlarged nodes at the back of his neck. The hair loss is not alopecia areata, and the lump is not a bacterial abscess — this is tinea capitis, the one dermatophyte infection that lives inside the hair shaft and that a cream can never reach. [1]
Tinea, also called dermatophytosis or ringworm, is a superficial infection of keratinised tissue — the stratum corneum, the hair shaft and the nail plate — by a small group of fungi called dermatophytes. They belong to three genera: Trichophyton, Microsporum and Epidermophyton. Dermatophytes digest keratin using secreted keratinases, so they live in dead keratinised tissue and do not invade living skin, which is why the disease stays superficial but keeps spreading outward across the skin surface. The name ringworm describes the expanding annular lesion and has nothing to do with a worm. [1] [6]
Three ideas anchor the whole topic for a fellowship candidate. First, the site decides the name and the treatment: scalp disease is capitis and always needs tablets, whereas body and groin disease usually needs only a cream. Second, the infecting species guides the drug: terbinafine works better for Trichophyton and griseofulvin better for Microsporum. Third, this is a contagious household and community problem: untreated carriers, siblings, classmates and pets keep reinfecting the child, so curing one child often means looking at the whole family. [2] [3]
Classification
The most useful way to sort a child's tinea is by where it sits on the body, because the site tells you the likely organism and whether a cream will work or tablets are needed. [6]
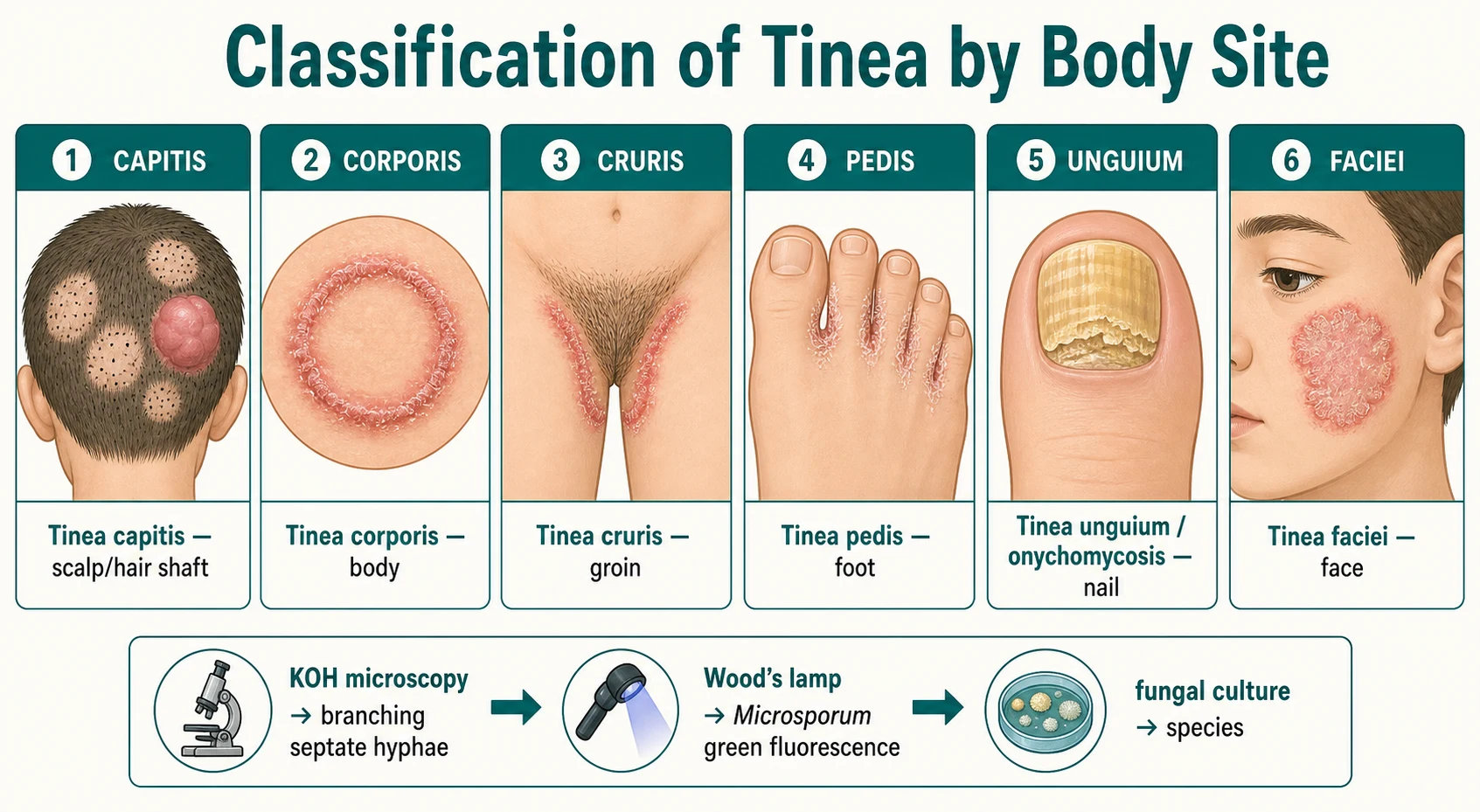
On the scalp and hair the disease is tinea capitis, the form that lives inside the hair shaft and that a topical cannot penetrate. On smooth body skin it is tinea corporis, the classic annular ring. In the groin creases it is tinea cruris, between the toes tinea pedis, and on the hand tinea manuum. The face carries tinea faciei, the beard area of an adolescent tinea barbae, and the nail tinea unguium, more often called onychomycosis. [6] [7]
A second axis, less obvious but clinically decisive, is the source of the organism. Anthropophilic species spread from person to person and cause quiet, chronic lesions. Zoophilic species, above all Microsporum canis caught from kittens and puppies, provoke a brisk inflammatory response and are the usual cause of the angry, boggy kerion. Geophilic species come from soil. Knowing the source matters because a zoophilic infection with a pet source will recur until the animal is treated. [1] [2]
Capitis
scalp and hair
- Prepubertal children
- Lives inside the hair shaft
- Always needs an oral antifungal
- Black-dot or grey-patch patterns; kerion
Corporis
body skin
- Annular ring with central clearing
- Active scaly advancing border
- Topical antifungal usually enough
- Wrestlers, animal contact
Cruris and pedis
groin and foot
- More common after puberty
- Topical antifungal first line
- Two-feet-one-hand pattern
- Dry between toes, treat footwear
Unguium
nail
- Thickened crumbly discoloured nail
- Less common in young children
- Oral therapy when treatment needed
- Specialist guidance for paediatric dosing
Epidemiology & Risk Factors
Tinea capitis is overwhelmingly a disease of prepubertal children, peaking between three and seven years of age. At puberty the sebaceous glands begin to secrete fungistatic fatty acids, which is why capitis becomes rare in adolescence even as tinea pedis and cruris become more common. [1] [3]
Transmission is by direct skin-to-skin contact and by sharing contaminated objects — hats, combs, brushes, towels, headsets, helmets and bedding. Outbreaks sweep through schools, households and wrestling teams, where tinea corporis gladiatorum is a recognised problem. Warm, humid weather, occlusive footwear, swimming-pool changing rooms and undiagnosed household pets all raise the risk. Children who are immunocompromised carry a greater burden and more recalcitrant disease. [6] [7]
The species story is regional. Trichophyton species, especially Trichophyton tonsurans, predominate in North America and the United Kingdom, while Microsporum species such as Microsporum canis and Microsporum audouinii remain the leading global cause with marked regional variation. Over the last decade a new and worrying pathogen, terbinafine-resistant Trichophyton indotineae, has spread from South Asia and now causes extensive, itchy, recalcitrant corporis and cruris that fail standard treatment. [1] [12]
Pathophysiology
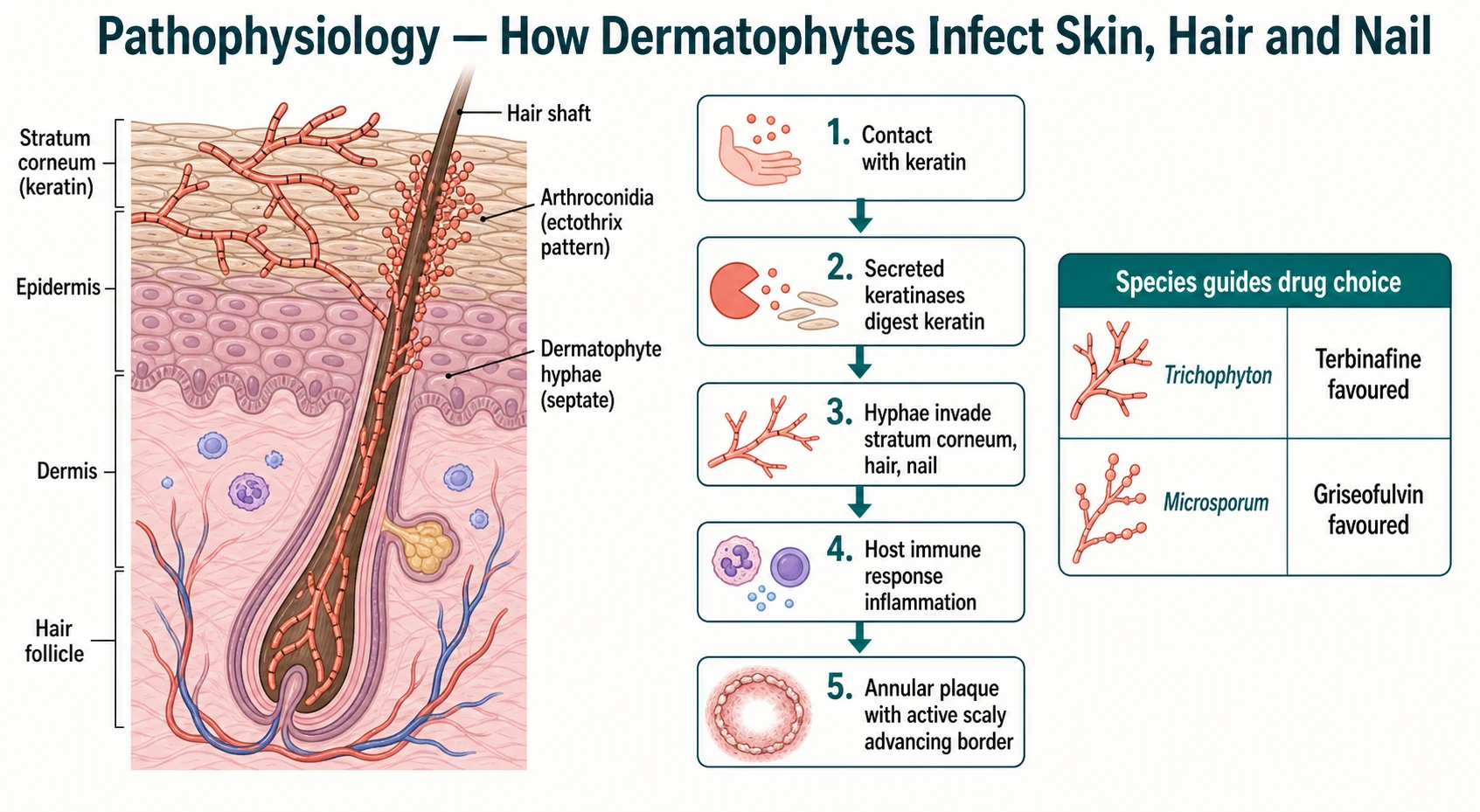
To understand why tinea looks the way it does, follow the fungus into the keratin. A dermatophyte lands on the skin surface, secretes keratinases that dissolve keratin, and sends branching septate hyphae down into the stratum corneum, into the hair shaft and into the nail plate. Because it lives on dead keratin and not living tissue, the infection stays superficial — but it keeps migrating outward across the skin, feeding on keratin as it goes. [6]
The annular lesion is a direct read-out of this behaviour. The raised red scaly advancing border is the active front, where hyphae are migrating into fresh keratin and the immune system is fighting back. The central clearing is where the host response has largely cleared the fungus behind the front. This is why sampling the edge, not the centre, gives the best yield for microscopy and culture. [6]
In the hair shaft the pattern of invasion matters. In an ectothrix infection, common with Microsporum, a sheath of arthroconidia forms on the outside of the hair; the infected hair is weakened, breaks off a few millimetres above the scalp, and some Microsporum species fluoresce green under a Wood's lamp. In an endothrix infection, typical of Trichophyton tonsurans, the conidia pack inside the hair shaft, the hair breaks flush with the scalp surface, and the result is the tell-tale black-dot pattern of broken hair stubs. Neither pattern fluoresces with Trichophyton tonsurans, so a negative Wood's lamp never rules capitis out. [1] [3]
The boggy kerion is the immune system overreacting. Faced with a zoophilic organism such as Microsporum canis, the host mounts an intense delayed hypersensitivity response: the scalp becomes swollen, boggy and studded with pustules, and the regional nodes enlarge. The pus is mostly inflammation, not bacterial load, which is why kerion is managed with antifungals and anti-inflammatories rather than a knife. [1] [2]
Clinical Presentation
The ring of tinea corporis is hard to forget once seen. It is a well-demarcated, annular plaque with a red, scaly, raised advancing border and paler central clearing. It expands slowly outward, may merge with neighbouring rings, and is often itchy. The child may have a single lesion or several, sometimes in satellite clusters. [6]
Tinea capitis is more varied, and the variation is the teaching. A grey-patch pattern shows scaly, grey, round or oval patches of hair loss with broken-off hair stubs. A black-dot pattern shows dotted stubs of hair broken flush with the scalp. Cervical or occipital lymphadenopathy is common and useful — its presence favours tinea capitis over a non-infectious scalp dermatosis. And the kerion is the dramatic end of the spectrum: a painful, boggy, purulent, inflamed mass that oozes and crusts and that families (and unwary clinicians) mistake for an abscess. [1] [3]
On the foot, tinea pedis most often sits between the toes as white, macerated, peeling skin that itches, and it can spread to the sole. The two-feet-one-hand pattern — scaling on both feet with one inflamed hand — is a classic stem: the child transfers the fungus from foot to hand by scratching. Tinea cruris forms a symmetrical, scaly, half-moon border that extends from the groin crease down the inner thigh but characteristically spares the scrotum, unlike candidal intertrigo. Tinea unguium thickens, discolours and crumbles the nail edge. Tinea faciei is an annular plaque on the face that is frequently misdiagnosed because the border can be indistinct. [7] [8]
Differential Diagnosis
The trap with any scaly annular patch is reaching for a topical steroid. The differential for a ring-shaped lesion is wide — atopic or nummular eczema, psoriasis, pityriasis rosea with its herald patch and collarette scale, granuloma annulare, a fixed drug eruption, erythema migrans of Lyme disease, and secondary syphilis — and several of these improve with steroid, which is exactly what makes the misdiagnosis sticky. [6]
Tinea corporis
fungal
- Active scaly advancing border
- Central clearing
- Slow expansion, mild itch
- KOH positive
Nummular eczema
inflammatory
- Coin-shaped, weeping crusts
- No central clearing
- Multiple, symmetric
- Atopic history, KOH negative
Pityriasis rosea
self-limiting
- Herald patch first
- Collarette scaling
- Trunk in fir-tree pattern
- Resolves in weeks
Granuloma annulare
non-infectious
- Ring of skin-coloured papules
- No scale on the border
- Hands, feet
- KOH negative
For the scaly bald scalp the differential is alopecia areata (smooth, non-scaly, exclamation-mark hairs, no nodes), seborrhoeic dermatitis, atopic dermatitis, psoriasis, traction alopecia, trichotillomania, and bacterial folliculitis or abscess for kerion. The discriminating features are the broken hair stubs and the lymphadenopathy of capitis against the clean smooth skin and absent nodes of alopecia areata. [1] [2]
The error that no fellowship candidate should make is prescribing a topical corticosteroid — alone or in a steroid–antifungal combination cream — for an undiagnosed annular lesion. The steroid suppresses the inflammatory border and the itch, so the child feels better, but it does nothing to the fungus. The lesion changes shape, loses its characteristic border, and spreads unchecked in a modified form called tinea incognito, which is harder to recognise and harder to treat. [6] [2]
Clinical & Bedside Assessment
Start with the story: when the lesion began, how fast it has spread, whether it itches, what creams have already been used (ask specifically about steroid-containing combinations), and whether there are pets, farm animals, or siblings and classmates with similar lesions. A child who has just acquired a kitten and then develops an inflamed scaly patch has a zoophilic Microsporum canis infection until proven otherwise. [2] [6]
Examine the lesion for the active scaly advancing border and central clearing, and look for satellite lesions that mark autoinoculation. For a suspected capitis, part the hair systematically, look for broken stubs and black dots, palpate for cervical and occipital lymphadenopathy, and feel for a boggy kerion. Always examine the whole child — the feet, groin, nails and body — because the scalp lesion may be only one of several sites, and the cause of a persistent corporis may be an untreated foot. [1] [7]
When a household source is likely, examine the contacts and ask about pets. Asymptomatic scalp carriage of Trichophyton tonsurans is common among family members of an infected child, and an untreated carrier or animal will reinfect the treated patient within weeks. Building the family and pet history into the assessment is what separates a single cure from lasting control. [10] [11]
Investigations
Most tinea is confirmed at the bedside with a potassium hydroxide (KOH) preparation. Scrape the scaly active border — not the cleared centre — onto a slide, add potassium hydroxide to dissolve the keratin, and look under the microscope for branching septate hyphae and arthroconidia. A positive KOH is enough to start treatment; it is quick, cheap, and far more useful than treating blind. [1] [6]
The Wood's lamp is selective, not universal. Some Microsporum species — Microsporum canis and Microsporum audouinii — produce a bright green fluorescence of infected hairs under ultraviolet light, which is a fast way to confirm an ectothrix capitis and to screen contacts. Trichophyton tonsurans, now the dominant capitis organism in many regions, does not fluoresce, so a negative Wood's lamp examination does not exclude tinea capitis. [3] [11]
Send a fungal culture to identify the species, because the species guides the drug choice and the source-tracing. Culture is also the way to detect the emerging terbinafine-resistant Trichophyton indotineae. The drawback is speed: dermatophyte culture takes two to four weeks. Where available, a dermatophyte polymerase chain reaction test gives a faster answer, but microscopy and culture together remain the diagnostic backbone. [3] [12]
Management — Resuscitation
Tinea is rarely a time-critical emergency, but three situations need prompt action. A kerion is painful, swollen and disfiguring, and the longer the inflammation runs the greater the risk of permanent scarring alopecia, so start an oral antifungal early. Extensive, rapidly spreading or highly inflamed corporis needs oral rather than topical therapy to get control. And any sign of secondary bacterial infection — crusting, weeping, surrounding cellulitis — needs an antistaphylococcal antibiotic added to the antifungal. [1] [2]
For the otherwise well child with localised tinea corporis, cruris or pedis, there is no resuscitation step: reassure the family, confirm the diagnosis at the bedside, and start a topical antifungal. Arrange prompt dermatology review for kerion, for extensive or recalcitrant disease, for suspected resistant species, and for any immunocompromised child. [6] [7]
Management — Definitive & Stepwise
The single most important rule in paediatric tinea is that tinea capitis always requires an oral antifungal. A cream cannot penetrate the hair shaft, so topical treatment of capitis fails, the hair loss continues, and the child keeps shedding spores to siblings and classmates. Oral therapy is the rule regardless of how mild the scalp looks. [1] [2]
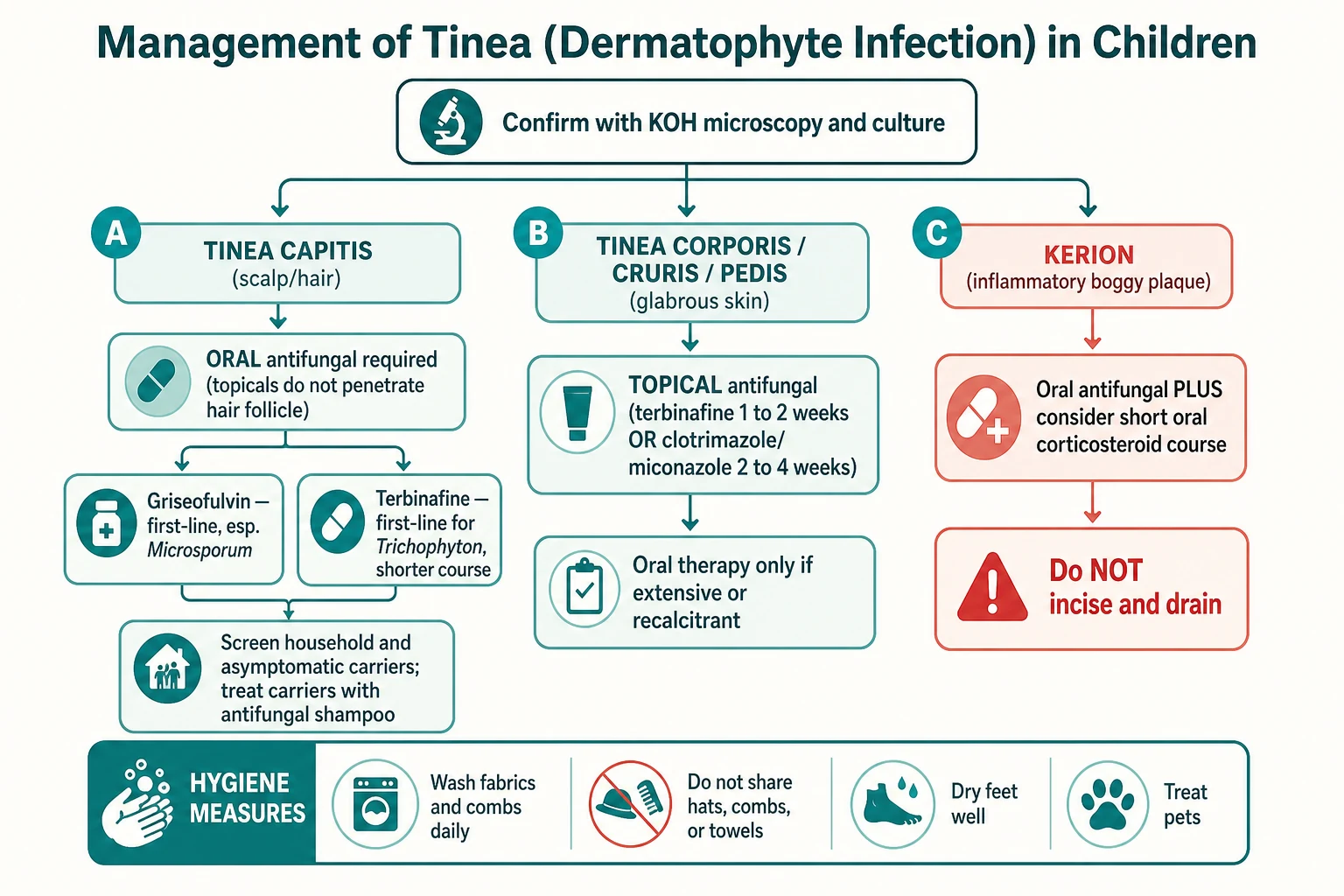
For capitis the two first-line agents are griseofulvin and terbinafine, and the choice follows the species. Griseofulvin is given at 10 mg per kilogram per day of the microsize formulation for 6 to 8 weeks and is the preferred agent when Microsporum is the cause. Terbinafine is dosed by weight band — 62.5 mg daily for a child under 20 kg, 125 mg daily for 20 to 40 kg, and 250 mg daily for over 40 kg — for 4 weeks, and is preferred for Trichophyton because it gives a shorter, more convenient course. [2] [5]
The evidence for species-guided choice comes from meta-analyses of randomised trials. Griseofulvin is statistically superior for Microsporum species (p = 0.04), while terbinafine is superior for Trichophyton species (p = 0.04). Because Trichophyton tonsurans now dominates in many regions, terbinafine's shorter course has made it first-line for those infections, but griseofulvin remains the better choice where Microsporum is confirmed or likely. [4] [5]
Confirm capitis with potassium hydroxide microscopy and send fungal culture to identify the species
Start an oral antifungal: griseofulvin for 6 to 8 weeks if Microsporum, weight-banded terbinafine for 4 weeks if Trichophyton
Add a short tapering course of oral corticosteroid for kerion to reduce inflammation and scarring
Screen and treat household contacts and asymptomatic scalp carriers, and treat infected pets
Advise hygiene measures and review at the end of therapy to confirm clinical and mycological cure
For the glabrous-skin forms, a topical antifungal is first-line and oral therapy is reserved for extensive, recalcitrant or immunocompromised disease. Apply terbinafine 1 per cent cream once or twice daily for 1 to 2 weeks, or an imidazole such as clotrimazole 1 per cent or miconazole 2 per cent twice daily for 2 to 4 weeks, to the lesion and a margin of normal skin beyond it. Continue for one week after the lesion clears to prevent relapse. Terbinafine and the naftifine-type allylamines generally work faster than the azoles. [6] [7] [8]
Adjunctive hygiene measures make cure durable. Wash hats, combs, brushes, towels and bedding in hot water, and do not share headgear, combs or towels. Dry the feet thoroughly and treat occlusive footwear. Wash the scalp with an antifungal shampoo such as ketoconazole or selenium sulphide two to three times weekly to reduce shedding of spores while the oral therapy takes effect. Treat infected household pets with a veterinarian. These measures matter most in capitis, where untreated carriers and pets are the engine of reinfection. [2] [10]
Specific Subtypes & Scenarios
Kerion demands early, combined treatment. Start an oral antifungal immediately — griseofulvin or terbinafine by species, as above — and add a short tapering course of oral corticosteroid (for example prednisolone at around 1 to 2 mg per kilogram per day for one to two weeks) to dampen the intense inflammation and reduce the risk of permanent scarring alopecia. Reassure the family that the pus is inflammatory rather than a sign of bacterial abscess, and explicitly do not incise and drain. If there is genuine secondary bacterial infection, add an antistaphylococcal antibiotic, but the backbone is the antifungal. [1] [2]
Onychomycosis (tinea unguium) is less common in children than in adults and should be confirmed mycologically before treatment, because several non-fungal nail dystrophies mimic it. When treatment is warranted, oral terbinafine for about 6 weeks for fingernails and 12 weeks for toenails, or itraconazole, is the standard, given under specialist guidance and weighed against the low paediatric prevalence and the drug exposure. [9]
The emerging terbinafine-resistant Trichophyton indotineae is the modern reason to culture. It produces extensive, highly itchy, recalcitrant lesions on the body and groin, often in adolescents and young adults, frequently with a personal or family link to South Asia. Standard terbinafine regimens fail, so send culture and request susceptibility testing, then switch to itraconazole or another agent guided by the mycology result. Recognising it early spares the child weeks of ineffective topical therapy. [12]
Asymptomatic household carriage is the hidden driver of capitis recurrence. Screening of household contacts of a child with tinea capitis finds a high rate of asymptomatic scalp carriage, and treating those carriers — along with antifungal shampoo for the index case and contacts — is what breaks the reinfection cycle. When a zoophilic species is identified, examine and treat the family pets as well. [10] [11]
Complications & Pitfalls
The preventable complications of tinea are largely the cost of delay and misuse. Kerion left undertreated leaves permanent scarring alopecia in the affected patches. Onychomycosis allowed to persist can produce permanent nail dystrophy. Any weeping lesion can develop secondary bacterial infection with Staphylococcus aureus. And the visible lesions and hair loss of capitis carry a real burden of psychosocial distress and stigma at school, which is part of why prompt, complete treatment matters. [1] [9]
The defining iatrogenic pitfall is tinea incognito. A topical corticosteroid — alone, or hidden inside a popular steroid–antifungal–antibiotic combination cream — suppresses the immune border and the itch, so the lesion looks better and feels better. But the fungus is unopposed and spreads, the classic ring is lost, and the lesion becomes atrophic, red and oddly pustular. The diagnosis is missed for months. The lesson is absolute: never treat an undiagnosed scaly annular lesion with a steroid. [6] [2]
The remaining pitfalls are management errors. Treating capitis with a topical alone fails because no cream reaches the hair shaft. Using a combination cream hides the diagnosis. Failing to screen and treat household carriers and pets guarantees recurrence. Stopping oral therapy early when the scalp looks better but before the course is complete invites relapse. And choosing terbinafine for a confirmed Microsporum infection, or griseofulvin for Trichophyton, misses the species-specific advantage that the evidence supports. [2] [5]
Prognosis & Disposition
Localised tinea corporis, cruris and pedis treated with an appropriate topical or short oral course has an excellent prognosis, with cure within weeks and recurrence prevented by hygiene and source control. The child returns to school once treatment is underway, with lesions covered where practical. [6] [7]
Tinea capitis and kerion also cure completely with adequate oral therapy, provided the course is finished and the household is treated. The one caveat is kerion: even correct treatment can leave patchy permanent scarring alopecia in the most inflamed areas, and a shortened or wrongly chosen regimen risks relapse and ongoing transmission. Set the expectation with families early. [1] [2]
Disposition follows severity and complexity. Manage localised corporis, cruris and pedis in the community. Refer to dermatology for kerion, for extensive or recalcitrant disease, for suspected terbinafine-resistant Trichophyton indotineae, for paediatric onychomycosis, for any immunocompromised child, and when the diagnosis is uncertain after bedside testing. Always arrange review of household contacts and pets when capitis or a zoophilic species is involved. [2] [12]
Special Populations
In the prepubertal child, capitis dominates and always needs oral therapy. Use weight-banded terbinafine or weight-based griseofulvin, involve the family in carrier screening, and work with the school when an outbreak is identified, because exclusion policies and headgear hygiene drive control. Prepubertal children are also the group most vulnerable to the stigma of visible lesions and hair loss, so frame the management around a quick, complete cure. [1] [10]
In the immunocompromised child — whether from chemotherapy, transplantation or primary immunodeficiency — tinea is more extensive, more atypical and more recalcitrant. Lower the threshold for oral therapy, for culture and susceptibility testing, and for dermatology involvement, because topical therapy alone often fails and atypical presentations are easily missed. [1] [12]
The zoophilic and geophilic exposure histories change the lesion and the management. A new kitten or puppy, farm animals, or soil contact raises zoophilic Microsporum canis or geophilic species as the cause, with brisker inflammation including kerion. Treat the infected animal or environmental source to prevent reinfection. For migrant, refugee and Indigenous families, and for any family facing access barriers, build transport, follow-up and culturally safe education into the plan so that a correct diagnosis is not undone by an unfinished course. [2] [11]
Evidence, Guidelines & Regional Differences
The major guidance is concordant across regions. The British Association of Dermatologists 2014 guideline sets the capitis standard: oral griseofulvin or weight-banded terbinafine, topical therapy for glabrous-skin disease, household screening, and corticosteroid adjunct for kerion. The German S1 guideline on tinea capitis and the NICE Clinical Knowledge Summary on fungal skin and nail infections reach the same conclusions, and the American Academy of Pediatrics Red Book endorses oral therapy for capitis and species-guided drug choice. [2] [3]
The species-specific evidence base comes from two meta-analyses of randomised trials. Tey and colleagues found that griseofulvin and terbinafine had comparable overall efficacy but diverged by organism, and Gupta and Drummond-Main confirmed the genus effect with griseofulvin superior for Microsporum and terbinafine superior for Trichophyton (each p = 0.04). The practical consequence is that terbinafine's shorter, weight-banded course has become first-line for the Trichophyton tonsurans that dominates many regions, while griseofulvin retains its place for confirmed Microsporum. [4] [5]
The active controversy is the rise of terbinafine-resistant Trichophyton indotineae. Standard regimens fail, and the literature now stresses culture and susceptibility testing before committing to a drug, with a shift toward itraconazole or alternative agents guided by the mycology result. This is also the strongest argument against empiric, prolonged topical therapy for an unresponsive lesion — the right move is to stop, sample, and treat to the identified organism. [12]
Griseofulvin vs terbinafine for tinea capitis — meta-analyses of randomised trials
Mantel-Haenszel meta-analysis comparing 8 weeks of griseofulvin with 4 weeks of terbinafine in tinea capitis
Practice change
Identify the species, then choose the drug — terbinafine first-line for Trichophyton, griseofulvin for Microsporum
Exam Pearls
Tinea capitis always needs an oral antifungal, because no cream reaches the hair shaft — this is the most tested single fact in paediatric tinea. [1] [2]
The species guides the drug: terbinafine is superior for Trichophyton and griseofulvin for Microsporum, each with p = 0.04 in meta-analysis. [4] [5]
RINGS
Kerion is a hypersensitivity reaction, not an abscess: treat with an oral antifungal plus a short corticosteroid course and never incise it. [1] [2]
Wood's lamp gives green fluorescence for some Microsporum species but not for Trichophyton tonsurans, so a negative lamp never excludes tinea capitis; confirm with potassium hydroxide microscopy showing branching septate hyphae. [3] [11]
References
- [1]Gupta AK, Polla Ravi S, Wang T, et al. An update on tinea capitis in children. Pediatr Dermatol, 2024.PMID 39113245
- [2]Fuller LC, Barton RC, Mohd Mustapa MF, et al. British Association of Dermatologists' guidelines for the management of tinea capitis 2014. Br J Dermatol, 2014.PMID 25234064
- [3]Gupta AK, Friedlander SF, Simkovich AJ Tinea capitis: An update. Pediatr Dermatol, 2022.PMID 35075666
- [4]Tey HL, Tan AS, Chan YC Meta-analysis of randomized, controlled trials comparing griseofulvin and terbinafine in the treatment of tinea capitis. J Am Acad Dermatol, 2011.PMID 21334096
- [5]Gupta AK, Drummond-Main C Meta-analysis of randomized, controlled trials comparing particular doses of griseofulvin and terbinafine for the treatment of tinea capitis. Pediatr Dermatol, 2013.PMID 22994156
- [6]Leung AK, Lam JM, Leong KF, et al. Tinea corporis: an updated review. Drugs Context, 2020.PMID 32742295
- [7]Sahoo AK, Mahajan R Management of tinea corporis, tinea cruris, and tinea pedis: A comprehensive review. Indian Dermatol Online J, 2016.PMID 27057486
- [8]Leung AK, Barankin B, Lam JM, et al. Tinea pedis: an updated review. Drugs Context, 2023.PMID 37415917
- [9]Leung AKC, Lam JM, Leong KF, et al. Onychomycosis: An Updated Review. Recent Pat Inflamm Allergy Drug Discov, 2020.PMID 31738146
- [10]Dessinioti C, Papadogeorgaki E, Athanasopoulou V, et al. Screening for asymptomatic scalp carriage in household contacts of patients with tinea capitis during 1997-2011: a retrospective hospital-based study. Mycoses, 2014.PMID 24372570
- [11]White JM, Higgins EM, Fuller LC Screening for asymptomatic carriage of Trichophyton tonsurans in household contacts of patients with tinea capitis: results of 209 patients from South London. J Eur Acad Dermatol Venereol, 2007.PMID 17714125
- [12]Uhrlaß S, Verma SB, Gräser Y, et al. Trichophyton indotineae-An Emerging Pathogen Causing Recalcitrant Dermatophytoses in India and Worldwide-A Multidimensional Perspective. J Fungi (Basel), 2022.PMID 35887512