Paeds · pain-palliative-and-end-of-life-care
Acute nociceptive pain management
Also known as Acute pain management in children · WHO two-step analgesic ladder for children · Paediatric multimodal analgesia · Morphine titration and PCA in children · Postoperative and sickle-cell pain management
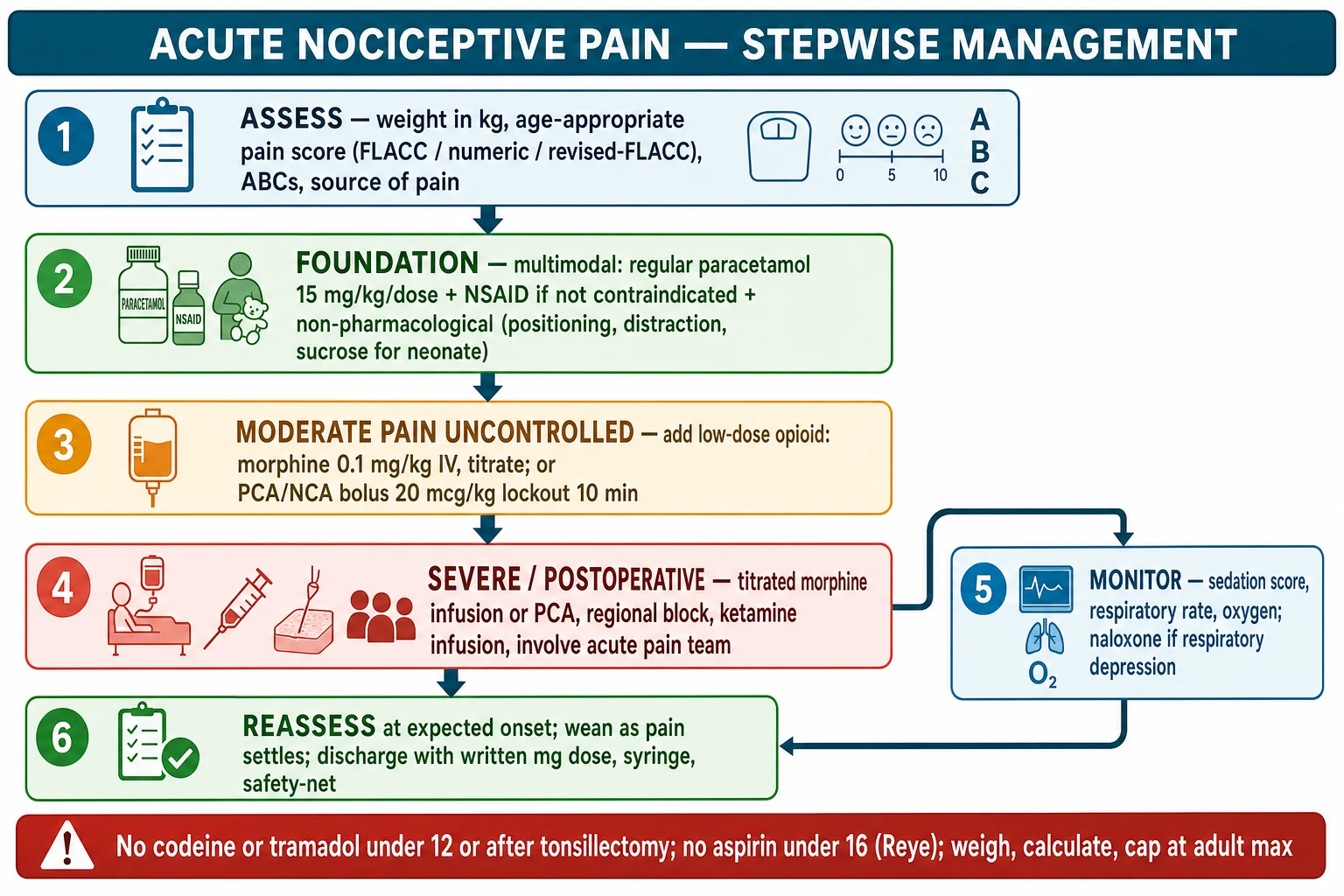
A fellowship approach to acute nociceptive pain in a child: score the pain with an age-appropriate tool, build a multimodal foundation of regular paracetamol (15 mg per kg per dose, max 60 mg per kg per day, adult max 1 g per dose and 4 g per day) and an NSAID (ibuprofen 5 to 10 mg per kg per dose, max 30 mg per kg per day, from three months and over 5 kg), and escalate up the WHO two-step ladder to morphine 0.1 mg per kg intravenously for moderate-to-severe pain. The 2025 JAMA Pediatrics network meta-analysis places NSAIDs first-line for acute paediatric pain. Severe or postoperative pain is run with a titrated opioid by patient- or nurse-controlled analgesia, a regional block and opioid-sparing adjuvants, with the sedation score and respiratory rate monitored and naloxone available. Codeine and tramadol are contraindicated under 12 and after tonsillectomy.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Acute nociceptive pain is the normal, time-limited protective response to a defined tissue injury — a fracture, a surgical wound, a burn, a sickle-cell vaso-occlusive crisis, a needle — with an expected trajectory of healing. The pain is the symptom, the injury is the cause, and the analgesia is one half of the plan; the other half is finding and fixing the source. A child who is given good analgesia but is still sent home from the emergency department with a missed torsion has been failed twice over, so analgesia never substitutes for diagnosis. [8]
The work begins with one question: how much does it hurt, and how do you know? Pre-verbal and cognitively impaired children cannot tell you in words, so a validated, age-appropriate pain score stands in for the words. The FLACC scale (Face, Legs, Activity, Cry, Consolability, each scored 0 to 2 for a total of 0 to 10) is the standard for the infant and pre-verbal child; the revised FLACC extends the same framework to children with cognitive impairment by adding individualised behaviours; the school-age child uses a 0-to-10 numeric or faces scale. The score is taken before the drug, and again at the expected onset of action, because a documented reassessment is the safeguard against both under-treatment and over-treatment. [10]
The unifying principle is the right drug, at the right weight-based dose, capped at the adult maximum, combined across classes, and judged on the child by a repeat pain score. The modern standard is multimodal and opioid-sparing: regular paracetamol and an NSAID carry most of the load, a regional or local anaesthetic technique targets the surgical site, and an opioid is titrated only for breakthrough or severe pain. The goal is a comfortable, breathing, recovering child — not a silenced one — and the sedation score is watched as closely as the pain score. [11] [12]
Classification
Two classifications matter at the bedside, and both change the first drug and the route. The first is by mechanism: somatic pain from skin, bone and muscle is well-localised and sharp, and responds to NSAIDs and regional blocks; visceral pain from a hollow organ is dull and poorly localised, and often needs an opioid early; procedural pain is brief but real and is anchored in non-pharmacological measures plus topical or short-acting agents. The second is by clinical context and severity: postoperative, traumatic or fracture, burn, sickle-cell vaso-occlusive, mucositis and procedural pain each have a typical trajectory and a typical regimen, and severity (mild, moderate, severe) sets the ladder step. [8] [11]
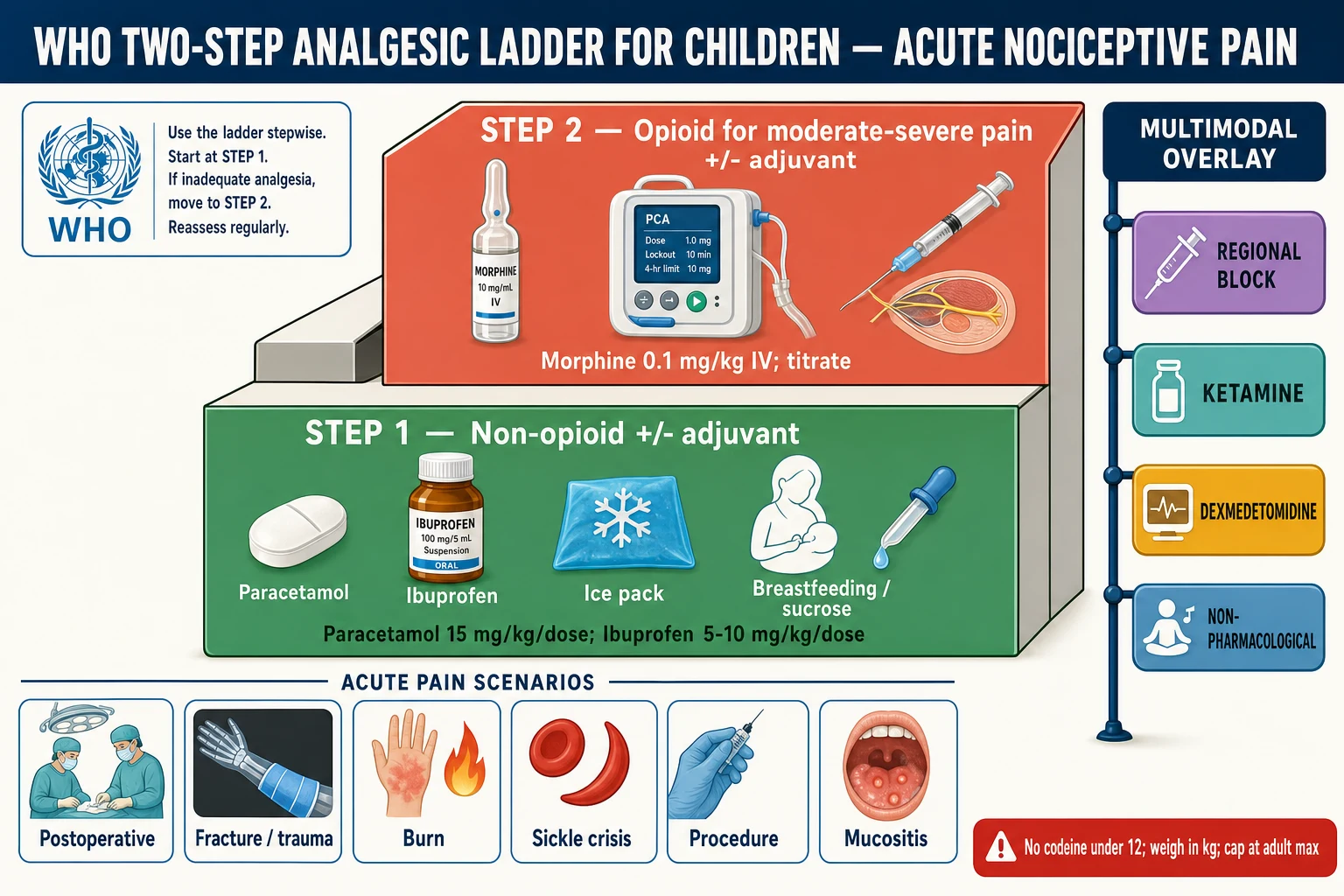
The WHO two-step analgesic ladder adapted for children is the spine of the topic. Step one is a non-opioid (paracetamol, with an NSAID where not contraindicated) plus an adjuvant and non-pharmacological measures. Step two is an opioid for moderate-to-severe pain, again with an adjuvant. The 2012 WHO revision deliberately removed the historical intermediate "weak-opioid" step (codeine, tramadol), because the prodrug opioids are unpredictable and now contraindicated in young children; the modern step-two opioid is morphine. The ladder is climbed by the clock (regular dosing, not as-needed, for established pain), by the child (the weight-based dose, capped at the adult maximum), and by the ladder (move up when the current step is inadequate). [1] [8]
The distinction from chronic and neuropathic pain matters because the plan is different. Acute nociceptive pain is time-limited and opioid-responsive, and the analgesia is weaned as the injury heals. Neuropathic pain (burning, shooting, allodynia) responds poorly to opioids and needs adjuvants such as gabapentinoids, and chronic pain is a biopsychosocial problem in which the opioid is rarely the whole answer. This page addresses the acute nociceptive child; the surrounding pages cover pain assessment, neuropathic pain, opioid stewardship and palliative symptom control. [9]
Epidemiology & Risk Factors
Acute pain is one of the most common reasons a child presents to or is admitted for care, and undertreated acute pain remains the commonest failure mode in paediatric analgesia. The risk of under-treatment is highest in the children who cannot describe it: the pre-verbal infant, the cognitively impaired child, and the child with a communication difficulty. These children depend on an observer who scores the pain with a validated tool and treats on the score — without that, their pain is systematically under-rated and under-dosed. [8] [10]
Child factors
- Pre-verbal or cognitively impaired children carry the highest risk of under-recognised, under-treated pain
- The opioid-naive child given a first opioid is at risk of respiratory depression; the post-tonsillectomy child with obstructive sleep apnoea is at highest risk
- Dehydration or renal impairment turns a safe NSAID into a nephrotoxin
- The neonate's immature liver and kidney lower the safe paracetamol ceiling and slow opioid clearance
Regimen factors
- A single drug given as-needed, rather than scheduled, leaves gaps in coverage
- An opioid titrated without a sedation score is the route to respiratory depression
- Failing to reassess the pain score at the expected onset hides a regimen that is not working
- Discharging on a large opioid supply with no wean plan invites harm
System factors
- An acute pain service, standardised infusion concentrations and PCA protocols reduce variability
- Night shifts and handovers are where monitoring gaps occur
- Rural and remote settings with limited access to a pain service or regional expertise
- Care transitions where the analgesic plan and the sedation score are not re-stated
The risk of opioid harm is concentrated and predictable. The opioid-naive child given a first dose, the child with obstructive sleep apnoea, the child on other sedatives, and the child on a morphine infusion or PCA at night are the groups in whom respiratory depression declares itself. The defence is institutional: a sedation score with a defined action threshold, continuous respiratory monitoring in the early hours, a standardised naloxone response, and an acute pain service that audits pain scores and adverse events. The modern literature on opioid-related adverse events in hospitalised children consistently shows that the harm tracks total opioid exposure — which is exactly why the opioid-sparing multimodal bundle is the standard. [9] [11]
Pathophysiology
Nociceptive pain follows a four-stage pathway from the injured tissue to the conscious brain, and each drug class acts at a different stage. The pathway is transduction, transmission, modulation and perception. Transduction begins at the peripheral nociceptor: tissue injury releases prostaglandins, bradykinin, ATP and hydrogen ions that either directly activate or sensitise the nociceptor endings. Transmission carries the signal along the fast, sharp A-delta fibres and the slow, dull C fibres into the dorsal horn of the spinal cord. Modulation occurs in the dorsal horn, where a spinal "gate" and a descending inhibitory pathway from the brainstem can amplify or dampen the signal. Perception is the conscious experience in the brain, with its sensory and emotional components. [3] [11]
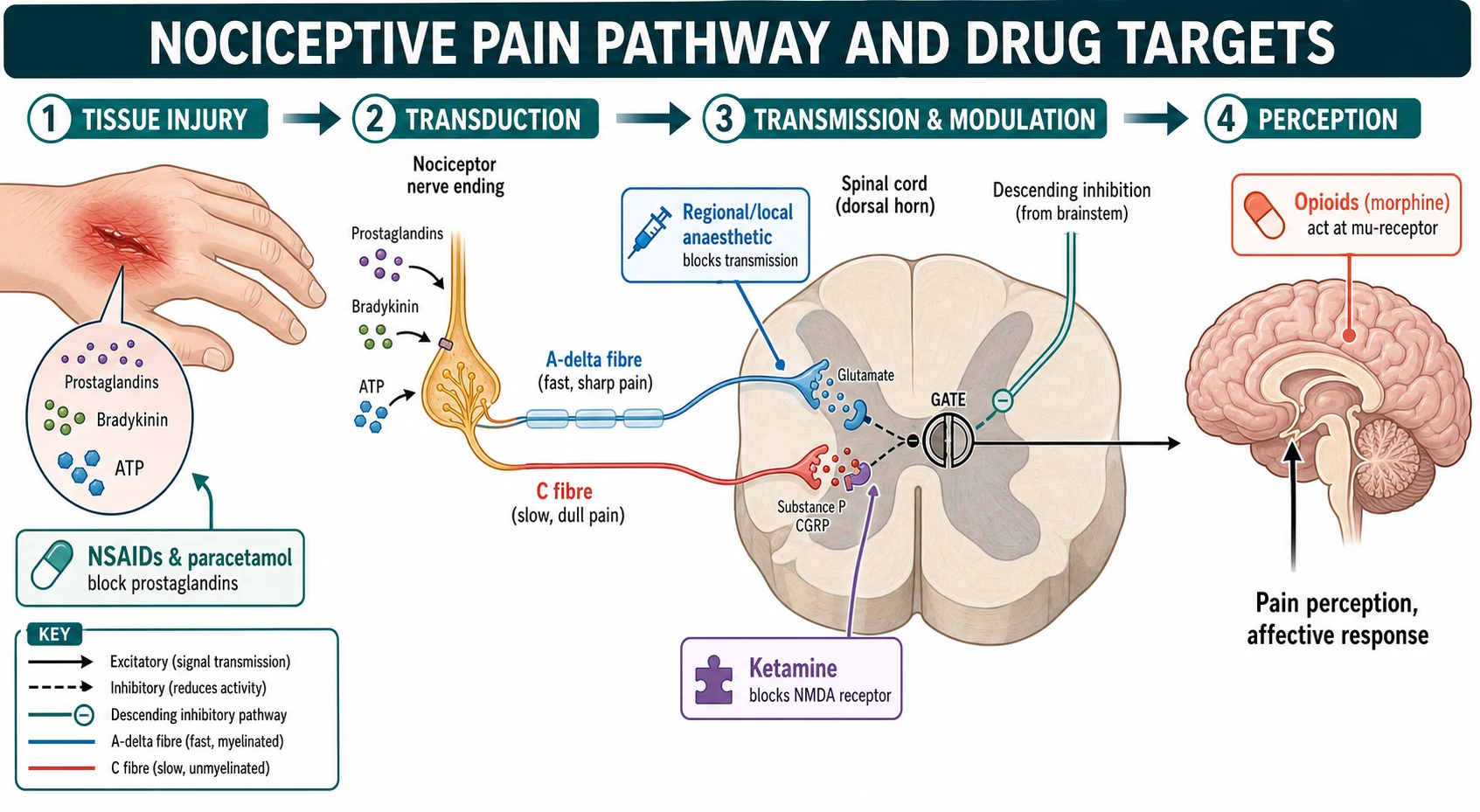
Mapping the drugs onto the pathway explains why combining them works. The NSAIDs and paracetamol act at the periphery and the central prostaglandin pathway, reducing transduction; this is the mechanistic reason NSAIDs give the greatest benefit with the least harm in acute pain, as the 2025 network meta-analysis confirmed. Local and regional anaesthetic blocks sodium-channel conduction along the nerve and in the dorsal horn, abolishing transmission from a defined territory. Ketamine blocks the NMDA receptor in the dorsal horn, dampening the central sensitisation that drives severe and refractory pain and opioid tolerance. Morphine agonises the mu-opioid receptor in the brain and spinal cord, dampening perception and the affective response to pain. [1] [11]
Two properties decide how each drug is used in practice. Paracetamol and the NSAIDs have a fixed ceiling: there is a maximum dose beyond which no further analgesia is gained and harm begins (hepatotoxicity for paracetamol, renal and gastrointestinal harm for NSAIDs), so they are given at a scheduled weight-based dose. Morphine has no analgesic ceiling: within the limit of respiratory depression, more morphine gives more analgesia, so it is titrated to the pain and to the sedation score. This single distinction is why the non-opioids form the scheduled backbone and the opioid is the titrated layer on top. The sickle-cell vaso-occlusive crisis shows the pathway in overdrive: ischaemia-reperfusion and infarction generate intense nociceptive and inflammatory input, central sensitisation sets in quickly, and the pain is severe, recurrent and opioid-responsive. [3] [11]
Clinical Presentation
A child with significant acute pain presents in one of several recognisable pictures, and the first move is to match the picture to a plan. The postoperative child guards the wound, splints on movement, and is reluctant to cough or breathe deeply; without good analgesia this becomes atelectasis and poor recovery. The fracture or trauma child holds the limb still, refuses to move it, and is tearful and tachycardic. The burn child has a constant background pain from the wound plus sharp procedural breakthrough during dressing changes. The sickle-cell child in vaso-occlusive crisis is still and guarded, with deep, gnawing pain in the back, chest, abdomen or long bones. The procedural discomfort of a cannula or venepuncture is brief but real, and anticipatory anxiety amplifies it. [8]
The crucial skill is to tell, within each picture, the child who is in pain from the child who is becoming unsafe on the analgesia. The postoperative or trauma child whose pain score is rising despite the regimen needs the ladder climbed, but the same child who becomes sedated with a falling respiratory rate needs the opioid held and naloxone considered. The discriminator is the sedation score: a child who is easy to rouse, breathing normally and comfortable is doing well; a child who is somnolent, bradypnoeic or unresponsive is in opioid-induced respiratory depression until proven otherwise. The sedation score is more sensitive than the pain score for the early detection of opioid harm, because sedation precedes respiratory depression. [9]
Pain uncontrolled
- Rising pain score, splinting, refusal to move or cough, tachycardia, agitation
- Climb the ladder: add or titrate the opioid, check the regional block, add an adjuvant
- Reassess at the expected onset of the new dose
- Re-diagnose if escalating — compartment syndrome, torsion, chest syndrome, intra-abdominal emergency
Opioid over-sedation
- Falling respiratory rate, increasing sedation, miosis, unresponsiveness
- Hold the opioid, stimulate, support the airway and breathing
- Naloxone titrated to the respiratory rate, not full reversal
- Monitor for recurrence — naloxone is shorter-acting than the opioid
Distress that is not pain
- Hypoxia, hypoglycaemia, sepsis, a full bladder, a tight cast, separation anxiety
- Check oxygen, glucose and observations before attributing distress to pain
- Agitation in the PICU may be delirium, not pain
- Treat the cause; do not reflexively escalate the opioid
Refractory pain
- Severe pain despite a correct multimodal regimen
- Consider ketamine infusion, a regional technique, and the acute pain team
- Check for opioid-induced hyperalgesia in the opioid-tolerant child
- Pain-team and specialist review before further opioid escalation
The neonate and the cognitively impaired child present the greatest detection challenge. The neonate in pain may cry inconsolably, flex and arch the legs, or become still and hypotonic; the FLACC behaviours are the structured way to read this. The cognitively impaired child may show the pain through individualised behaviours — grimacing, breath-holding, agitation or withdrawal — which is why the revised FLACC adds behaviours specific to that child. In both groups, the default is a low threshold to treat and a documented reassessment, because under-treated pain is the failure mode and a structured tool is the defence. [10]
Differential Diagnosis
When a child's pain is not controlled by the current regimen, work through a fixed list rather than reaching reflexively for more opioid. First, is the dose adequate for the weight? An under-dose given on an estimated weight is the commonest reason a pain "does not respond." Second, is the route failing — an intramuscular dose poorly absorbed, a dislodged intravenous cannula, a clamped or migrated epidural? Third, is the source of pain changing — a new compartment syndrome under a cast, a developing sickle chest syndrome, an intra-abdominal emergency behind postoperative pain? Fourth, could this be opioid-induced hyperalgesia in a child on high or prolonged opioid exposure, where more opioid makes the pain worse? Fifth, and most commonly missed, is the distress actually pain at all? [8] [9]
Separating a child in unrecognised pain from a child agitated for another reason is a recurring ward judgement. The agitated child on the ward or in the PICU may be hypoxic, hypoglycaemic, septic, delirious, holding a full bladder, or in a tight cast — each of these masquerades as pain until it is directly addressed. The disciplined move is to check the oxygen saturation, the bedside glucose, the bladder and the observations before escalating any opioid, because opioid given to a hypoxic or delirious child causes harm rather than relief. A chest syndrome in a sickle-cell child, a compartment syndrome in a casted limb, and a testicular torsion are the dangerous diagnoses that hide behind "pain not controlled," and each needs re-diagnosis, not more morphine. [3] [9]
Clinical & Bedside Assessment
The bedside assessment rests on two measurements: a scored pain assessment and a measured weight in kilograms. The pain is scored with an age-appropriate validated tool, because the carer's and clinician's estimates systematically under-rate a child's pain. The FLACC scale (Face, Legs, Activity, Cry, Consolability), each domain scored 0 to 2 for a total of 0 to 10, is the standard for infants and pre-verbal children. The revised FLACC extends the same framework to children with cognitive impairment by adding individualised behaviours drawn from the parents' knowledge of the child, which improves both reliability and validity. The verbal school-age child uses a 0-to-10 numeric rating scale or a faces scale, and the adolescent a numeric or verbal rating as an adult would. [10]
The weight is measured on a calibrated scale, recorded in kilograms, and never estimated unless it is a true emergency, because every analgesic dose is calculated from it and capped at the adult maximum. The focused history frames the choice: the age and weight; the source and expected trajectory of the pain; prior opioid exposure; renal and hepatic function; asthma, allergy and bleeding risk; obstructive sleep apnoea; and concurrent sedatives or other analgesics. A child who is already on a chronic opioid, or who has had a tonsillectomy, changes the plan at the first assessment. [8] [11]
The synthesis the candidate speaks and documents is the problem representation: the child's age and weight, the pain problem and its score, the chosen ladder step, the calculated drug doses with the caps, the reassessment time, and the sedation-monitoring plan. Every dose is written with a leading zero (0.5 mg, never .5 mg) and never a trailing zero (5 mg, never 5.0 mg), double-checked independently for opioids, and accompanied by a documented reassessment. The sedation score is charted with the pain score and the respiratory rate, because the three together — pain, sedation, breathing — are the safety triangle of acute opioid management. [9]
Investigations
Most acute pain is managed without investigations beyond the bedside, because the analgesic decision is clinical and driven by the score. Investigations serve two purposes: to frame the safety of the drug, and to frame the source of the pain. A renal panel and electrolytes before an NSAID in the dehydrated or unwell child protects the kidney. A coagulation screen before a regional block frames the bleeding risk. A full blood count in the child on a chronic opioid, the sickle-cell child, or the febrile child frames the broader picture. A bedside glucose is taken early in any child with altered behaviour or a reduced conscious level, because hypoglycaemia mimics and compounds sedation and distress. [8] [9]
Pain itself is treated as a vital sign: a documented pain score is charted with the other observations, and a documented reassessment after each intervention is the audit standard for an acute pain service. The sedation score is the primary safety monitor during any opioid infusion or PCA, not the pain score, because sedation precedes respiratory depression. A typical four-point sedation score runs from "easy to rouse" through "easy to rouse but drifts off" to "difficult to rouse" and "unrousable"; a defined threshold (commonly a sedation score indicating the child is difficult to rouse, or a respiratory rate below the age-normal range) triggers an opioid reduction, a pause and a review. [9]
Each measured response — the pain score, the sedation score, the respiratory rate — feeds back into the next titration decision, which is why acute pain management is a cycle rather than a single act. The acute pain service exists to run that cycle reliably across a ward, to catch the child whose pain is not settling and the child who is becoming over-sedated, and to standardise the concentrations, the protocols and the monitoring that make titration safe. [11]
Management — Resuscitation
Resuscitation in acute pain is the recognition and immediate management of the child in severe pain and the child who has become unsafe on the analgesia. The general approach is constant: assess the airway, breathing and circulation; score the pain; give the weight-based dose of the right class; identify and treat the source; and escalate to senior help, the acute pain service, intensive care and retrieval when the child is seriously ill. Severe pain is treated promptly and in its own right, because a child in unrelieved severe pain is physiologically stressed, but the analgesia is given alongside, never instead of, the search for and treatment of the cause. [8] [9]
For severe pain, the first opioid is morphine 0.1 mg per kg intravenously, titrated in small increments to the pain score and the sedation score, with the airway, breathing and oxygen monitored throughout. Intramuscular morphine is avoided when intravenous access is possible, because absorption is unpredictable and the titration is lost; where intravenous access is genuinely impossible, intranasal fentanyl is an option in the emergency setting. The child who has received naloxone is observed for recurrence, because the opioid outlasts the antidote by hours. After any opioid adverse event, the child is made safe first, then the regimen, the monitoring and the concentrations are reviewed, and the event is reported. [8] [9]
Management — Definitive & Stepwise
Definitive management is the WHO two-step analgesic ladder adapted for children, delivered as a multimodal bundle and titrated to the score. The ladder is climbed stepwise, by the clock (regular scheduled dosing for established pain), by the child (the weight-based dose capped at the adult maximum), and by the ladder (move up when the current step is inadequate). The paediatric version places non-pharmacological measures at the foundation, because comfort, sucrose, breastfeeding, distraction and positioning are analgesic in their own right and reduce the total drug load — a point the adult ladder underplays and the paediatric prescriber must not. [1] [8]
Step 1 — Multimodal foundation
Regular paracetamol 15 mg per kg per dose every 4 to 6 h (max 60 mg per kg per day, adult max 1 g per dose and 4 g per day) and ibuprofen 5 to 10 mg per kg per dose every 6 to 8 h (max 30 mg per kg per day, from 3 months and over 5 kg), plus non-pharmacological measures (sucrose for the neonate, distraction, positioning). The 2025 network meta-analysis places NSAIDs first-line for acute pain.
Step 2 — Add a titrated opioid
For moderate-to-severe pain not controlled by step one, morphine 0.1 mg per kg intravenously, titrated in increments to the pain score and sedation score. The historical weak-opioid step (codeine, tramadol) is replaced by morphine because the prodrug opioids are contraindicated under 12 and after tonsillectomy.
Step 3 — PCA, NCA, regional and adjuvants
For severe or postoperative pain, run a titrated opioid by patient-controlled analgesia (morphine bolus about 20 mcg per kg, 10-minute lockout) or nurse-controlled analgesia for the child too young to trigger, add a regional or local anaesthetic block, and add ketamine or dexmedetomidine as opioid-sparing adjuvants. Involve the acute pain team.
Monitor, reassess, wean
Chart the sedation score and respiratory rate with naloxone available. Reassess the pain score at the expected onset of each intervention. Wean the opioid as the pain settles — convert infusion or PCA to scheduled oral, then as-needed, then stop — keeping the multimodal backbone to protect the wean.
The anchor doses never change. Paracetamol is 15 mg per kg per dose every four to six hours, maximum 60 mg per kg per day in a child and an adult ceiling of 1 g per dose and 4 g per day. Ibuprofen is 5 to 10 mg per kg per dose every six to eight hours, maximum 30 mg per kg per day, from three months and over 5 kg. Morphine is 0.1 mg per kg intravenously, or 0.2 to 0.5 mg per kg orally, titrated and monitored. Each is calculated from a measured weight, capped at the adult maximum, and rounded to an available formulation. The PCA morphine bolus is about 20 micrograms per kilogram with a 10-minute lockout, and a nurse-controlled bolus is used for the child too young to trigger the device. [8] [11]
PACED
The opioid-sparing principle is the modern standard, and it rests on the multimodal bundle. Regular paracetamol and an NSAID, a regional or local anaesthetic technique for the surgical site, and an adjuvant such as ketamine or dexmedetomidine together reduce total opioid exposure, which both improves recovery and reduces opioid-related adverse effects. The opioid is then titrated for breakthrough or moderate-to-severe pain, rather than carrying the whole load. The regional techniques — a wound infiltration, a peripheral nerve or fascial-plane block, a caudal or epidural — are the opioid-sparing core of postoperative analgesia, and their growing use in complex paediatric patients is one of the clearest advances in the field. [11] [12]
In Australia and Aotearoa New Zealand, the Royal Children's Hospital Melbourne Clinical Practice Guidelines and the AMH Children's Dosing Companion are the bedside references: paracetamol 15 mg per kg per dose (max 60 mg per kg per day, adult max 4 g per day), ibuprofen 5 to 10 mg per kg per dose (max 30 mg per kg per day) from three months and over 5 kg, and morphine 0.1 mg per kg intravenously titrated. ANZ acute pain services run standardised PCA and nurse-controlled analgesia protocols with mandatory sedation scoring. [8]
Specific Subtypes & Scenarios
The postoperative child is the archetype of planned, multimodal, opioid-sparing analgesia. Regular paracetamol and an NSAID (where not contraindicated) form the backbone, a regional or local anaesthetic technique targets the surgical site, and a low-dose opioid — morphine by PCA, or oxycodone orally — is reserved for breakthrough or moderate-to-severe pain, titrated and monitored with a sedation score. The explicit goal is to minimise total opioid exposure, which improves recovery and reduces opioid-related adverse effects, and the regimen is weaned on a planned schedule as the pain settles. The 2016 postoperative pain guideline from the American Pain Society and the anaesthesia societies sets the multimodal, opioid-sparing standard that paediatric practice follows. [11] [12]
The fracture or trauma child is managed with early weight-based analgesia, because splinting and immobilisation are analgesic in their own right and should accompany the drug. Ibuprofen carries the inflammatory component, paracetamol adds the background, and a titrated opioid is given for severe pain; intranasal fentanyl is an option in the emergency setting while intravenous access is established. The trap under a cast is compartment syndrome, which declares itself as pain rising out of proportion, pain on passive stretch, and increasing analgesic requirement — and the correct response is to escalate the limb, not the opioid. A child whose pain is escalating despite a correct regimen has a new problem until proven otherwise. [8]
Postoperative
- Planned multimodal: regular paracetamol and NSAID, regional technique, titrated opioid by PCA
- Opioid-sparing is the standard; wean on a planned schedule
- Monitor sedation score, respiratory rate and oxygen
- Watch for atelectasis and ileus from under-treated pain
Burn
- Two pains: constant background plus procedural breakthrough at dressing changes
- Background: scheduled paracetamol, NSAID and a long-acting opioid where appropriate
- Procedural: pre-procedional opioid or ketamine, nitrous oxide, distraction, the burn team
- Opioid tolerance and hyperalgesia are common; involve the pain team early
Sickle crisis
- Early weight-based opioid and a regular NSAID where not contraindicated
- Hydration and incentive spirometry to prevent chest syndrome
- Individualised pain plan from the haemoglobinopathy team (ASH 2020)
- Ketamine and PCA have a role in severe or recurrent crisis
Procedural
- Plan the procedure, the analgesia and the child's position together
- Topical amethocaine or EMLA, sucrose for the neonate, distraction and positioning
- Child-life involvement reduces anxiety and pain
- Nitrous oxide or low-dose opioid or ketamine where the procedure warrants
The burn child carries two distinct pains that must be separated, because they need different treatment. A constant background pain from the wound itself is managed with scheduled paracetamol, an NSAID and a long-acting opioid where appropriate. A sharp procedural breakthrough occurs during dressing changes and debridement, and is managed with a pre-procedural opioid or low-dose ketamine, nitrous oxide, distraction and the burn team. Opioid tolerance and opioid-induced hyperalgesia are common in the burn child because of repeated high exposure, which is why the pain team is involved early and the adjuvants (ketamine in particular) have a defined role. [4]
The sickle-cell vaso-occlusive crisis is a severe acute pain that is also recurrent, and it is managed by an individualised plan. Early weight-based opioid (morphine) and a regular NSAID where not contraindicated form the foundation; hydration and incentive spirometry protect against the acute chest syndrome, which is the leading cause of death in sickle-cell disease; and an individualised pain action plan, held by the family and the haemoglobinopathy team, shortens the time to effective analgesia and reduces the adversarial dynamic that has historically surrounded sickle-cell pain. The 2020 American Society of Hematology guideline sets out the evidence-based management of acute and chronic sickle-cell pain, and acknowledges that effective relief must be balanced against the risks of repeated opioid exposure. Ketamine and patient-controlled analgesia have a role in severe or recurrent crisis. [2] [3]
The procedural pain of a cannula, venepuncture, urethral catheter or lumbar puncture is brief but real, and is managed by planning the procedure, the analgesia and the child's position together. For the neonate, oral sucrose (about 0.1 to 2 mL of 24 per cent sucrose given two minutes beforehand, with non-nutritive sucking and breastfeeding) reduces the behavioural pain response to heel lancing and venepuncture, and breastfeeding or breast milk itself reduces procedural pain in neonates. For the older child, topical amethocaine or EMLA applied 30 to 60 minutes beforehand, distraction, positioning and child-life involvement carry much of the load; where the procedure warrants it, nitrous oxide or a low-dose opioid or ketamine is given under monitoring. Non-pharmacological measures are not optional add-ons — they are a genuine analgesic layer with their own evidence base. [5] [6]
Complications & Pitfalls
The preventable errors in acute pain management cluster at predictable points, and naming them is half of avoiding them. The first is failing to reassess: a dose is given but the pain score is not re-checked at the expected onset, so a regimen that is not working is allowed to run on. The second is escalating an opioid without checking the sedation score: a child who is agitated may be hypoxic, delirious or in opioid-induced hyperalgesia rather than in pain, and more opioid in that state causes harm. The third is giving an NSAID to a dehydrated child, which precipitates acute kidney injury. The fourth is giving codeine or tramadol to a young or post-tonsillectomy child, which is simply not done because the prodrug opioids are restricted. [9] [11]
Under-treatment
- Estimated weight, an under-dose, or a single as-needed drug leaves gaps
- Pre-verbal or cognitively impaired child with an unrecognised, under-scored pain
- Failing to reassess at the expected onset hides a failing regimen
- The defence is a scored assessment, a scheduled regimen and a documented reassessment
Over-treatment
- Opioid titrated without a sedation score leads to respiratory depression
- Agitation treated as pain without checking oxygen or glucose
- A large discharge opioid supply with no wean plan
- The defence is the sedation score, the safety triangle and a written wean
Wrong drug
- Codeine or tramadol in a child under 12 or after tonsillectomy
- An NSAID in a dehydrated or renally impaired child
- Aspirin in a febrile child under 16 (Reye syndrome)
- The defence is the named restriction applied every time
Missed diagnosis
- Compartment syndrome under a cast treated as uncontrolled pain
- Sickle chest syndrome, testicular torsion, an intra-abdominal emergency
- Refractory pain treated with more opioid instead of source control
- The defence is to re-examine and re-diagnose when pain escalates
The discharge pitfall deserves its own sentence, because it is where acute pain management meets opioid stewardship. A child sent home on a large opioid supply with no wean plan, a liquid medicine in millilitres rather than milligrams, and no safety-net, is set up for both a home error and a persistent opioid exposure. The defence is a written discharge dose in milligrams, a dosing syringe, a stated maximum daily dose, a wean schedule where relevant, and a safety-net naming the features that should bring the child back — increasing pain despite the analgesia, sedation or unrousability, reduced feeding or fluids, and any new red-flag feature. The opioid-stewardship principle, developed further in the surrounding page, is that every opioid has a start date and a stop date. [11]
Prognosis & Disposition
Outcome in an acute opioid adverse event is driven almost entirely by the speed of naloxone and the availability of monitoring. A child who is stimulated, supported and given naloxone titrated to the respiratory rate promptly recovers, but is observed for recurrence because naloxone is shorter-acting than the opioid; a child in whom respiratory depression is detected late, or who is hypoxic at the time, has a worse course. The disposition of a child who has received naloxone is therefore continued monitoring, with repeat boluses or an infusion available, and a review of the regimen, the concentrations and the monitoring that allowed the event. [9]
For the postoperative child, the source and expected trajectory of the pain drive the disposition. A child after a minor day-case procedure with a written multimodal plan and a safety-net goes home. A child after major surgery, or a child with a high-risk comorbidity such as obstructive sleep apnoea, is admitted with an acute pain service review and overnight monitoring. The child with obstructive sleep apnoea given a postoperative opioid needs overnight monitoring because the apnoea and the opioid interact, and the threshold for escalation to a higher-acuity bed is low. The wean is planned: convert infusion or PCA to scheduled oral, then to as-needed, then stop, keeping the multimodal backbone to protect the wean. [11]
The sickle-cell child is admitted for the vaso-occlusive crisis and discharged on a weaning plan coordinated with the haemoglobinopathy team, with the individualised pain action plan updated for the next episode. The burn child is managed across a long trajectory with the burn and pain teams, with the regimen adjusted to the wound and the dressing schedule. In every case, the discharge communication closes the loop: a written dose in milligrams, a dosing syringe, a stated maximum daily dose, a wean plan where relevant, and a safety-net the family can act on. [2] [4]
Special Populations
The neonate is dosed with weight-band figures from a neonatal formulary, a lower paracetamol daily ceiling reflecting hepatic immaturity, and opioids given cautiously with monitoring for apnoea, because the clearance is slow and the respiratory centre is sensitive. Procedural pain is anchored in non-pharmacological measures — oral sucrose, breastfeeding and non-nutritive sucking — which have their own evidence base in this group. The child with cognitive impairment or communication difficulty is assessed with the revised FLACC, carries a low threshold to treat pain, and benefits from a written pain plan shared across carers and settings, because under-treated pain is the failure mode and a structured, individualised tool is the defence. [7] [10]
The child with sickle cell disease is managed with an individualised pain action plan, the haemoglobinopathy team, and the ASH 2020 guidance that balances effective relief against the risks of repeated opioid exposure. The opioid-tolerant child — chronic pain, palliative care, or a sickle-cell child on long-term opioid — is managed in the acute setting by continuing the baseline opioid and adding titrated breakthrough, never by abruptly stopping the baseline, with the pain team involved early. The Indigenous, remote, migrant or socioeconomically disadvantaged family is supported with clear dosing instructions, a dosing syringe, accessible language and teach-back, follow-up that the family can reach, and culturally safe communication — because the discharge plan only closes if the family can act on it. [2] [8]
Evidence, Guidelines & Regional Differences
The evidence base is strongest where the stakes are highest. The 2025 JAMA Pediatrics network meta-analysis (Olejnik et al., 41 trials, 4935 children) found that NSAIDs, ketamine and mid- to high-potency opioids all reduced acute paediatric pain compared with placebo, but that NSAIDs provided the greatest benefit with the least harm, and were the only class that reduced the need for rescue medication. The analysis placed NSAIDs as the first-line therapy for acute painful conditions in children — a clear, contemporary evidence statement that anchors step one of the ladder. Neither NSAIDs nor paracetamol increased short-term gastrointestinal adverse events in this analysis. [1]
Pharmacologic management of acute paediatric pain (Olejnik 2025, JAMA Pediatrics)
Key finding
In a network meta-analysis of 41 trials and 4935 children, NSAIDs, ketamine and mid- to high-potency opioids each reduced acute pain versus placebo. NSAIDs gave the greatest benefit with the least harm and were the only class that reduced the need for rescue medication (relative risk about 0.3).
ASH 2020 sickle-cell disease pain management guideline (Brandow 2020, Blood Advances)
Key finding
The American Society of Hematology 2020 guideline set out evidence-based management of acute and chronic sickle-cell pain, including early opioid analgesia for the vaso-occlusive crisis, individualised pain plans, and a balance between effective relief and the risks of repeated opioid exposure.
The 2022 SCCM PADIS guideline for critically ill children applies the assess-prevent-manage principle in the PICU: pain is assessed with validated tools at defined intervals, prevented where possible (for instance with procedural analgesia), and managed with a stepped regimen, alongside the parallel management of agitation, neuromuscular blockade and delirium. The 2016 postoperative pain guideline from the American Pain Society and the anaesthesia societies sets the multimodal, opioid-sparing standard, and the growing use of regional anaesthesia in complex paediatric patients is one of the clearest recent advances in opioid-sparing care. The WHO guidelines on the pharmacological treatment of persisting pain in children remain the source of the two-step ladder and the removal of the weak-opioid step. [9] [11]
Regional practice converges on the doses and the ladder. The Royal Children's Hospital Melbourne guidelines, the AMH Children's Dosing Companion and the BNFc agree on paracetamol 15 mg per kg per dose with a 60 mg per kg per day ceiling, ibuprofen 5 to 10 mg per kg per dose from three months and over 5 kg, and morphine 0.1 mg per kg intravenously titrated. They converge on the codeine and tramadol contraindication under 12 and after tonsillectomy, and on aspirin avoidance in under-16s. Where the evidence is maturing — the opioid-sparing dose of dexmedetomidine, the optimal ketamine infusion for refractory pain, the role of regional anaesthesia in the smallest infants — the prescriber names the source and the local protocol rather than inventing a figure. [8] [12]
Exam Pearls
Self-test — the over-sedated postoperative child
A six-year-old is on a morphine PCA after appendicectomy. The nurse calls because he is "sleepy and not using the pump." His respiratory rate has fallen, he is difficult to rouse, and his pain score is now low. What is the diagnosis and the immediate action? [9]
This is opioid-induced respiratory depression, not well-controlled pain. The low pain score in a sedated, bradypnoeic child is a warning, not a triumph. Stimulate, support the airway and breathing, hold the PCA, and give naloxone titrated to the respiratory rate — not to full reversal. The goal is a breathing child who is still comfortable. Monitor for recurrence, because naloxone is shorter-acting than morphine, and review the regimen, the concentrations and the monitoring. The defence that should have caught it earlier is the sedation score charted with the pain score and the respiratory rate. [9] [11]
The high-yield one-liners: acute nociceptive pain is opioid-responsive and weans as the injury heals; the WHO two-step ladder replaced the three-step ladder by removing the weak-opioid step; NSAIDs are first-line for acute pain, with the greatest benefit and least harm; morphine is titrated and monitored because it has no analgesic ceiling; the sedation score, not the pain score, is the early warning for opioid harm; naloxone is titrated to the respiratory rate and repeated because it is shorter-acting than the opioid; sucrose for neonatal procedures is a small absolute volume, never millilitres per kilogram; and every opioid has a start date and a stop date. The candidate who can speak the dose, the cap, the cap's reason, and the monitoring that goes with it, is the candidate who passes the viva. [1] [11]
References
- [1]Olejnik L, Lima JP, Sadeghirad B, et al. Pharmacologic Management of Acute Pain in Children: A Systematic Review and Network Meta-Analysis JAMA Pediatr, 2025.PMID 39899301
- [2]Brandow AM, Carroll CP, Creary S, et al. American Society of Hematology 2020 guidelines for sickle cell disease: management of acute and chronic pain Blood Adv, 2020.PMID 32559294
- [3]Darbari DS The vaso-occlusive pain crisis in sickle cell disease: Definition, pathophysiology, and management Eur J Haematol, 2020.PMID 32301178
- [4]Ciornei B, Ciornei A, Girdon A, et al. Pain Management in Pediatric Burns: A Review of the Science behind It Glob Health Epidemiol Genom, 2023.PMID 37745034
- [5]Pillai Riddell R, Yamada J, Harrison D, et al. Non-pharmacological management of infant and young child procedural pain Cochrane Database Syst Rev, 2023.PMID 37314064
- [6]Shah PS, Aliwalas LL, Shah VS Breastfeeding or breast milk for procedural pain in neonates Cochrane Database Syst Rev, 2023.PMID 37643989
- [7]Stevens B, Yamada J, Ohlsson A, Halperin S, Chhor V Sucrose for analgesia in newborn infants undergoing painful procedures Cochrane Database Syst Rev, 2016.PMID 27420164
- [8]Krauss BS, Calligaris L, Green SM, Barbi E Current concepts in management of pain in children in the emergency department Lancet, 2016.PMID 26095580
- [9]Smith HAB, Besunder JB, Betz S, et al. 2022 Society of Critical Care Medicine Clinical Practice Guidelines for Prevention and Management of Pain, Agitation, Neuromuscular Blockade, and Delirium in Critically Ill Pediatric Patients Pediatr Crit Care Med, 2022.PMID 35119438
- [10]Malviya S, Voepel-Lewis T, Burke C, Merkel S, Tait AR The revised FLACC observational pain tool: improved reliability and validity for pain assessment in children with cognitive impairment Paediatr Anaesth, 2006.PMID 16490089
- [11]Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists J Pain, 2016.PMID 26827847
- [12]Dumbarton TC Regional anesthesia in complex pediatric patients: advances in opioid-sparing analgesia Can J Anaesth, 2024.PMID 37884770