Paeds · pain-palliative-and-end-of-life-care
Chronic primary and secondary pain in children
Also known as Chronic pain in children · Chronic primary pain · Chronic secondary pain · Nociplastic pain · Central sensitisation · Juvenile fibromyalgia · Complex regional pain syndrome
Fellowship guide to chronic primary and secondary pain in children. Covers the ICD-11 split of chronic pain into primary, where the pain is itself a nociplastic disease with distress and disability, and secondary, where pain arises from an identifiable cause; the three mechanisms of nociceptive, neuropathic and nociplastic pain; central sensitisation and the fear-avoidance cycle; the common primary syndromes of juvenile fibromyalgia, complex regional pain syndrome, chronic daily headache and functional abdominal pain; the biopsychosocial assessment centred on function; the red-flag screen; and the interdisciplinary rehabilitation plan built on graded physical reactivation, cognitive behavioural and acceptance therapies, sleep and a planned return to school, with opioids avoided for chronic primary pain.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A thirteen-year-old girl arrives with eight months of daily widespread aching, broken sleep, worsening headaches, and a school attendance that has slid to two days a week. Her mother brings a folder of normal blood tests and scans and asks for "stronger painkillers." This is the classic shape of chronic primary pain in an adolescent, and it is one of the most common, most missed, and most mishandled problems in general paediatrics. The skill is not to find a hidden disease or to escalate analgesia. It is to recognise the pattern, screen once for the serious causes, explain pain in a way that reframes it from damage to a wound-up nervous system, and build a rehabilitation plan around sleep, movement, mood and school.[7]
Overview & Definition
Chronic pain is defined by time. Pain that persists or recurs for more than three months is chronic; everything shorter is acute, and the three-month cut-off is the one used by the International Association for the Study of Pain and built into ICD-11.[1] The threshold matters because something changes at three months. Acute pain is a symptom that signals threat and resolves as tissue heals. Chronic pain, especially chronic primary pain, stops behaving like a warning bell and starts behaving like a disease in its own right, one driven by a nervous system that has become sensitised and keeps generating pain after the original trigger has gone.[2]
The single most useful idea for a candidate to hold is the ICD-11 split of chronic pain into two families. Chronic primary pain is pain in one or more body regions, lasting more than three months, that is associated with significant emotional distress and significant functional disability and is not better explained by another chronic pain condition. Here the pain is the diagnosis; the nervous system is the problem. Chronic secondary pain is pain that follows from an underlying disease, such as juvenile arthritis, inflammatory bowel disease, cancer, or a nerve injury; here the disease drives the pain and you treat the disease, although the pain can still take on a life of its own.[1][3]
This split is not academic. It changes everything you do at the bedside. A child with chronic primary pain does not need more scans or stronger opioids; they need a biopsychosocial explanation and a rehabilitation plan. A child with chronic secondary pain needs the underlying disease treated, and then the residual pain managed on its own terms. Mixing the two up, by over-investigating primary pain or under-treating secondary pain, is the commonest error in this area.[7]
Classification
The ICD-11 chronic pain classification, finalised through an International Association for the Study of Pain working group and field-tested internationally, divides chronic pain into one primary and seven secondary categories.[1][4]
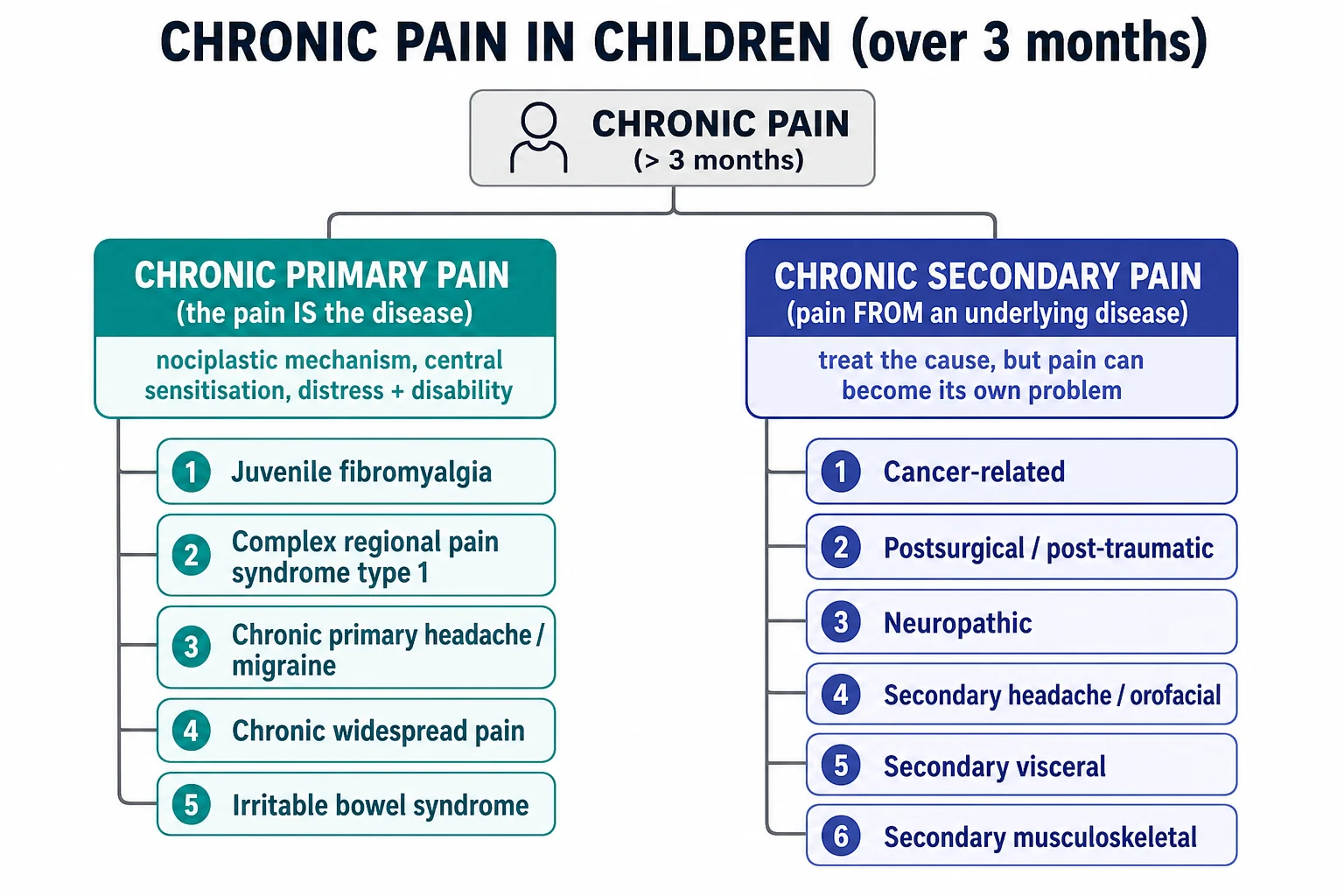
The seven secondary categories, each tied to a body system or cause, are chronic cancer-related pain, chronic postsurgical or posttraumatic pain, chronic neuropathic pain, chronic secondary headache or orofacial pain, chronic secondary visceral pain, and chronic secondary musculoskeletal pain. A child can have more than one, and secondary pain can become complicated by central sensitisation until it behaves like primary pain; the classification allows you to code both the cause and the pain that has emerged on top of it.[1]
Epidemiology & Risk Factors
Chronic pain in children is common, and most paediatricians underestimate how common. A systematic review of population studies found that chronic pain, variously defined, affects between roughly one in nine and one in three children and adolescents, with headache, abdominal pain and musculoskeletal pain the most frequent sites.[5] Prevalence rises through childhood and peaks in adolescence, and girls are affected more often than boys, especially for widespread and nociplastic patterns.[5]
What matters clinically is not the number who hurt but the number who are disabled by it. Around one in twenty school-age children has chronic pain severe enough to be highly disabling, with frequent school absence, sleep disruption and interference with daily life.[6] Functional abdominal pain disorders alone, the best-studied nociplastic model, affect around one in eight children, with the irritable bowel syndrome pattern in roughly two to three per cent.[12]
Chronic primary pain is best understood as a biopsychosocial problem. The risk factors cluster into three streams. Biologically, a child who has had an earlier painful condition or injury, who is female, pubertal, or who sleeps poorly is more vulnerable. Psychologically, anxiety, low mood, pain catastrophising and a tendency to fear and avoid movement all amplify and maintain pain. Socially, a family with its own pain history, parental catastrophising and over-protection, school stress, bullying, adverse childhood experiences and socioeconomic disadvantage all raise the risk that acute pain becomes chronic and disabling.[7][5]
The maintaining factors are the ones a candidate can actually act on. School absence, social withdrawal, disturbed sleep, deconditioning from inactivity, and a family increasingly organised around the pain form a vicious cycle: the child does less, hurts more, sleeps worse, feels lower, and withdraws further. Breaking that cycle, not eliminating the pain, is the aim of treatment.[7]
Pathophysiology
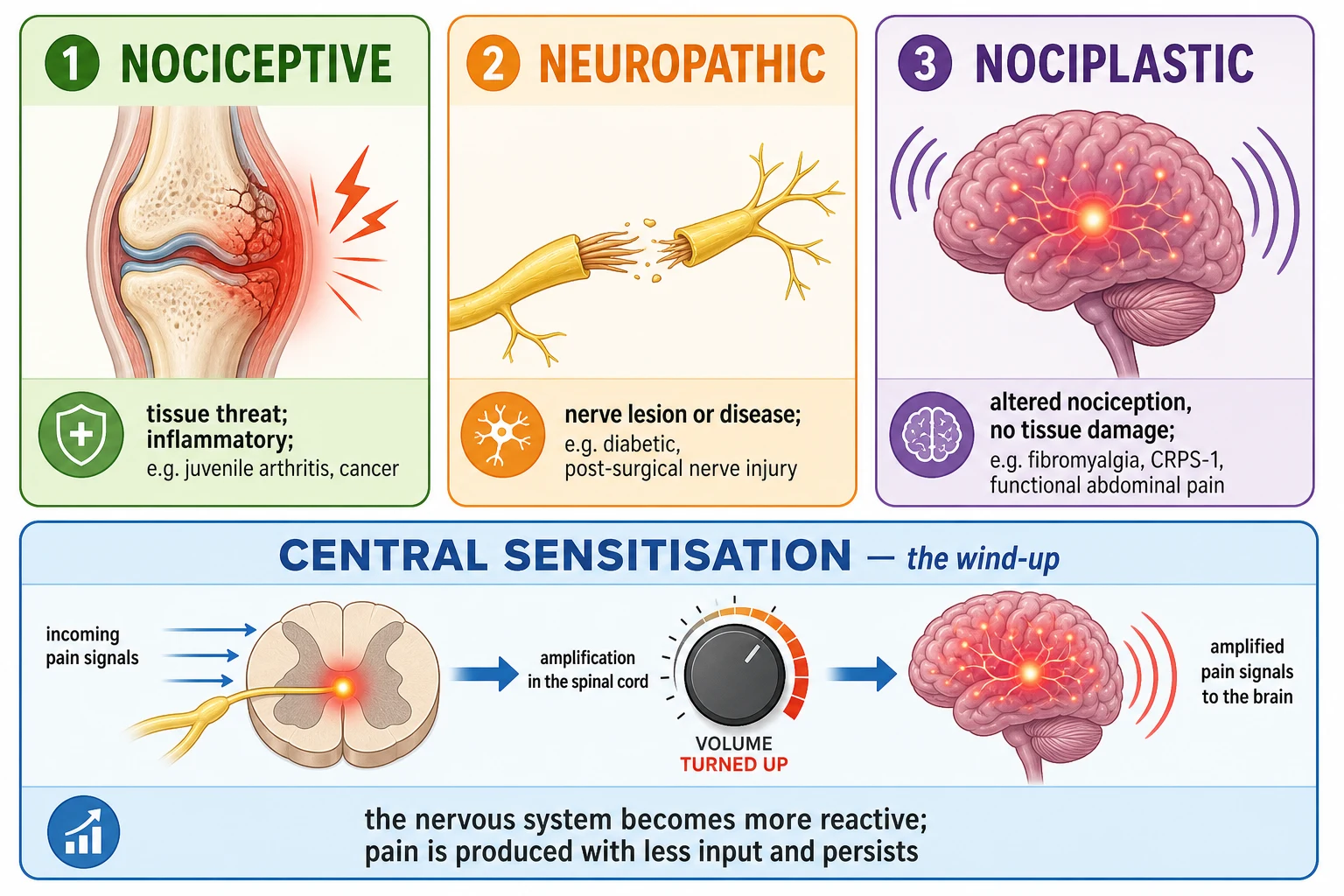
If a parent asks why their child still hurts when every scan is normal, the honest and accurate answer is that the nervous system itself has changed. Central sensitisation is the core mechanism. After repeated or prolonged nociceptive input, the spinal cord and brain become more responsive to incoming signals. The threshold for a stimulus to be felt as pain drops, mildly unpleasant stimuli become painful (allodynia), and painful stimuli hurt more than they should (hyperalgesia). The pain amplifier has been turned up, and it stays up.[1][2]
Central sensitisation is the biological substrate of nociplastic pain, the mechanism that defines chronic primary pain. Unlike nociceptive pain, which signals ongoing tissue damage, and unlike neuropathic pain, which signals a lesion of the nerves themselves, nociplastic pain arises from altered nociceptive function in a structurally intact nervous system. There is no torn tissue and no transected nerve; there is a system that has learned to produce pain. This is why a normal magnetic resonance image is not a contradiction of the child's pain; it is entirely consistent with it.[1]
Two further pieces complete the picture. First, the brain's descending inhibitory pathways, which normally dampen pain, become less effective in chronic primary pain, so the brake comes off as well as the accelerator turning up. Second, pain is processed alongside emotion and cognition in shared brain networks, which is why mood, attention, expectation and sleep so powerfully modulate how much a chronic pain hurts. Pain is never a pure sensory event.[2]
The behavioural counterpart is the fear-avoidance cycle. A child interprets pain as a sign of damage, becomes afraid of movement, and avoids activity. Avoidance leads to stiffness, weakness and deconditioning, which produce more pain on the rare occasions the child does move, which confirms the belief that movement is dangerous. The child spirals into disability and school absence. Understanding this loop is what allows you to explain, credibly, why the way out is to move more, not less.[7]
This mechanism also explains a treatment truth that candidates must state plainly: chronic primary pain responds poorly to conventional analgesics. Opioids, paracetamol and non-steroidal anti-inflammatories target nociceptive or inflammatory input that, in nociplastic pain, is not the main problem. The effective levers are the ones that retrain the nervous system, namely graded reactivation, psychological therapy and restored sleep.[7]
Clinical Presentation
The child with chronic primary pain usually arrives after months of symptoms and multiple normal tests. The presentation is dominated less by a crisp physical finding than by a pattern: persistent or recurring pain lasting more than three months, in one or several body regions, accompanied by a growing cluster of sleep difficulty, fatigue, low mood or anxiety, and declining participation in school, sport and friendships.[7][5]
Common primary presentations include widespread aching with fatigue and unrefreshing sleep, the juvenile fibromyalgia pattern; a limb that is painful, cold, swollen or avoided after a minor injury, the complex regional pain syndrome pattern; daily or near-daily headache, often with medication overuse; and recurring abdominal pain with a normal work-up, the functional abdominal pain pattern. Many children have more than one site, and a history of "the pain has moved around" or "first the stomach, now the head and legs" is a clue to a nociplastic process rather than a new disease in each location.[7][11]
In Australia and Aotearoa New Zealand, adolescents with this presentation are often referred on after normal paediatric and sometimes rheumatology work-up. The pitfall in ANZ practice, as elsewhere, is the cascade of repeated imaging and multiple subspecialty opinions that delays rehabilitation; the ANZ expectation is a single, thorough, red-flag-screened assessment followed by a clear biopsychosocial explanation and referral to a paediatric chronic pain service when function is impaired.[7]
Adolescents bring additional features. Chronic pain in adolescence overlaps heavily with anxiety, depressive symptoms and disordered sleep, and it frequently coincides with school refusal, social withdrawal and family conflict. The young person may have read extensively online, may be frightened of permanent damage, and may be caught between a parent pressing for more investigation and another urging them to "push through." Capturing this in the history is part of the diagnosis.[7]
A child with chronic secondary pain presents against the background of the underlying disease: a child with juvenile arthritis and a swollen hot joint, a child with inflammatory bowel disease and abdominal pain, a child with cancer and bony pain, or a child with a nerve injury after surgery. The pain is real and often mixed, and severe secondary pain can itself drive sensitisation until a nociceptive problem acquires nociplastic features.[1]
The severity that matters is functional severity, not the number on a pain scale. A child who rates their pain nine out of ten but still attends school, sleeps and sees friends is less urgent than a child who rates it six but has stopped going to school and is awake half the night. Function is the vital sign of chronic pain.[7]
Differential Diagnosis
The differential has two layers. The first is to decide which chronic primary syndrome a child has; the second, and the more important, is to make sure a serious or treatable cause has not been missed. The red-flag screen exists precisely to separate pain that needs investigation from pain that needs rehabilitation.[7]
The features that most reliably point away from primary pain and towards a serious cause are systemic: weight loss, fever, night sweats, fatigue out of proportion, and persistent raised inflammatory markers. Night pain that wakes a child from sleep and pain that is steadily worsening rather than fluctuating also demand explanation. Morning stiffness lasting more than thirty minutes points to inflammatory rather than mechanical or nociplastic pain.[7]
Two benign conditions are commonly over-medicalised into chronic pain diagnoses and should be recognised and normalised. Benign joint hypermobility is common in children and usually asymptomatic; it becomes a problem only when it is accompanied by pain and disability, and even then the management is reactivation, not escalating investigation. Growing pains are bilateral, evening or night leg pain in young children with a normal examination and no daytime symptoms; they are benign and self-limiting, though they sometimes foreshadow a pain-vulnerable phenotype.[7]
Clinical & Bedside Assessment
The assessment of chronic pain is a biopsychosocial history more than a physical hunt. The aim is to build a formulation that explains why this child, with this nervous system and this life, has developed persistent disabling pain now. Cover seven domains: the pain itself (site, character, onset, course, triggers, relievers), mood and anxiety, sleep, school attendance and activity, the family's response and pain history, prior investigations and treatments, and the child's own understanding and goals.[7]
The examination has two purposes: to screen for the serious mimics, and to demonstrate to the family that the child has been properly examined. Do a general examination including growth and pubertal staging, a full musculoskeletal screen for joint swelling, warmth, range of movement and a gait observation, and a neurological screen including tone, power, reflexes, sensation and coordination. Look deliberately for the things that would change the plan: pallor, bruising, lymphadenopathy, organomegaly, a hot joint, focal neurological signs, and any midline spinal or back finding.[7]
A few tools help quantify what matters. A simple zero-to-ten numeric rating scale, or a faces scale in younger children, captures pain intensity. More important is function: the Functional Disability Inventory scores how much pain interferes with home, school, social and physical activity, and pain and sleep diaries over a week or two reveal the pattern far better than a single clinic number. Ask directly about school days missed in the last month; the answer is often the single most useful piece of data.[7]
Assess the family as carefully as the child. Parental catastrophising, the tendency to expect the worst from pain, and over-protective responses, such as taking over tasks and excusing the child from activity, are powerful maintainers of disability and are themselves targets for treatment. Equally, a parent with untreated chronic pain models the very behaviour you are trying to change.[7]
The synthesis is a one-sentence biopsychosocial formulation: "This is a thirteen-year-old with a pain-vulnerable, sensitised nervous system, a family history of chronic pain, broken sleep, and growing school avoidance, in whom a thorough screen has excluded serious disease." That sentence frames the plan and, said aloud to the family, is often the first step of treatment.[7]
Investigations
The guiding principle for investigation in chronic pain is restraint. A targeted screen to exclude the serious mimics is appropriate and reassuring; a cascade of repeated imaging and panels is harmful, because every additional normal scan reinforces the family's belief that a hidden disease is still being missed and that more looking is the answer.[7]
A reasonable first screen, tailored to the presentation, includes a full blood count, inflammatory markers such as C-reactive protein and erythrocyte sedimentation rate, and basic biochemistry. Add targeted tests only as the history demands: coeliac serology and a faecal calprotectin for recurrent abdominal pain, a sickle screen where relevant, autoimmune and urinalysis where the pattern suggests it. Imaging is reserved for focal, red-flag, or progressive findings, not for diffuse chronic pain with a normal examination.[7]
How a normal result is communicated matters as much as the test itself. "All the tests are normal and there is nothing wrong" lands as dismissal and drives the family to seek another opinion. "The tests are normal, which is exactly what we expected; it confirms that there is no dangerous disease and that the problem is a sensitised nervous system that we can retrain" lands as validation and a plan. The same result, two very different outcomes.[7]
Allied health input is part of the work-up, not an add-on. A physiotherapy assessment of strength, range and conditioning, and where available a psychology assessment of mood, catastrophising and function, complete the picture and directly inform the rehabilitation plan.[7]
Management — Resuscitation
Chronic pain is rarely a resuscitation problem, but two situations demand immediate action. The first is the child who carries a red flag that has been missed: new weight loss, night pain, neurological signs, or systemic features in a child labelled as chronic primary pain. This is not primary pain until the serious cause is excluded, and the immediate step is targeted investigation and, where indicated, urgent imaging or referral, not a pain plan.[7]
The second is the child in functional decompensation: complete school refusal, near-total withdrawal from activity, severe sleep disruption, or a level of disability that the family cannot manage. This child needs prompt escalation to an interdisciplinary paediatric chronic pain service or, where available, an intensive rehabilitation program, rather than months of waiting and escalating analgesia. The urgency is functional, and the treatment is structured rehabilitation.[7]
Management — Definitive & Stepwise
The definitive management of chronic primary pain is interdisciplinary rehabilitation, delivered by a team that typically includes a paediatrician, a psychologist, a physiotherapist, and a nurse or social worker, working with the school and the family. The goal is stated up front and returned to often: restored function, sleep, mood, school attendance and participation. Pain may persist, but life comes back. Chasing a pain score of zero is not the goal, and saying so reframes the whole enterprise for the family.[7][8]
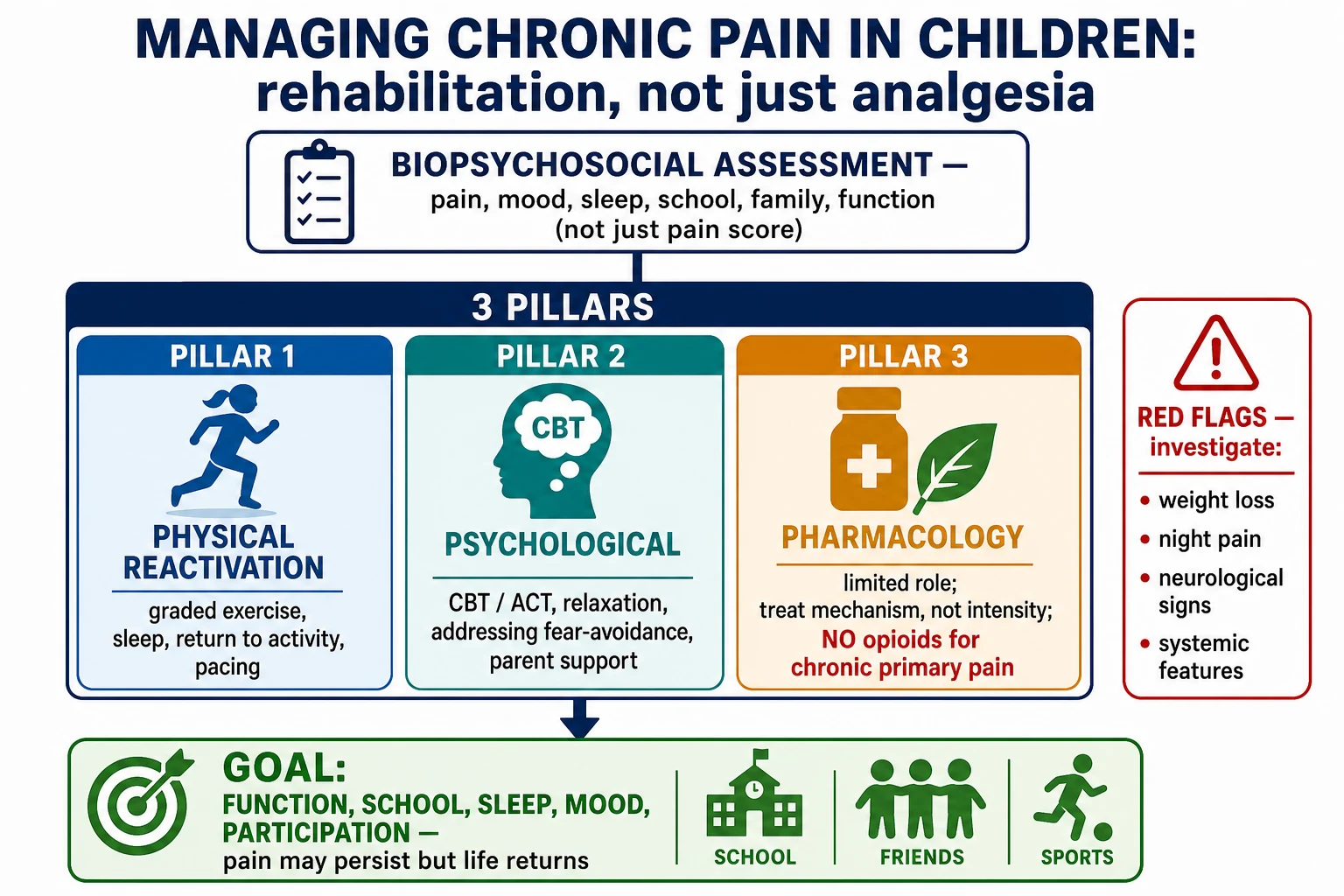
The plan rests on three pillars.[7]
The three pillars of chronic pain rehabilitation
Pillar one — physical reactivation: graded, paced return to movement and activity, a sleep and routine plan, and a staged return to school. The nervous system is retrained by doing, not by resting.
Pillar two — psychological therapy: cognitive behavioural therapy or acceptance and commitment therapy to address fear-avoidance, catastrophising, low mood and anxiety, with parent-focused strategies to reduce over-protection.
Pillar three — judicious, mechanism-based pharmacology: limited role; treat the mechanism, not the intensity; no opioids for chronic primary pain.
Physical reactivation is the engine of recovery. The child starts below their pain threshold and increases activity on a fixed schedule regardless of pain, using pacing to avoid the boom-and-bust cycle of overdoing it on a good day and crashing the next. Sleep is addressed directly, with consistent sleep and wake times, screen restriction before bed, and treatment of any anxiety or mood problem that is keeping the child awake. A planned, staged return to school is negotiated with the school, beginning with partial days or favoured subjects and building up; school return is both a marker and a driver of recovery.[7]
Psychological therapy has the strongest evidence of any intervention in paediatric chronic pain. Cochrane systematic reviews find that psychological therapies, principally cognitive behavioural therapy, reduce pain and disability in children and adolescents with chronic and recurrent pain, and that remotely delivered (internet-based) programmes extend access with comparable benefit.[9][10] Acceptance and commitment therapy works on a different lever, helping the young person commit to valued activity alongside pain rather than fighting to eliminate it, and is increasingly used in adolescent programmes.[7]
Pharmacology has a limited, mechanism-based role. For genuine nociceptive flares, such as an inflamed joint or post-injury pain, paracetamol and non-steroidal anti-inflammatories at standard weight-based paediatric doses are reasonable short-term adjuncts. For neuropathic pain, a gabapentinoid such as gabapentin or pregabalin, or a tricyclic such as amitriptyline, titrated to weight and effect, may help. For chronic primary, nociplastic pain, analgesics are generally ineffective, and the risk is that prescribing them reinforces the disease model.[7]
The WHO 2020 guidelines frame this clearly: physical and psychological therapies are the recommended core, the pharmacological evidence in children is thin and heavily weighted toward caution, and the default is to do the least medicine and the most rehabilitation consistent with restoring function.[7]
The World Health Organization 2020 guidelines on the management of chronic pain in children recommend physical therapy (including therapeutic exercise) and psychological therapy (cognitive behavioural, behavioural and acceptance-based approaches) and caution that the evidence for pharmacological interventions in children is limited; the guidelines do not recommend initiating strong opioids for chronic primary pain.[7]
Specific Subtypes & Scenarios
Juvenile fibromyalgia is the archetypal chronic primary pain syndrome of adolescence. It presents with widespread musculoskeletal pain for more than three months, severe fatigue, unrefreshing sleep, and cognitive complaints such as difficulty concentrating, often with headache, abdominal pain and mood symptoms. Examination is normal apart from tenderness. Diagnosis is clinical, after exclusion of inflammatory and endocrine disease; the emphasis is on confirming the diagnosis, validating the experience, and beginning an aerobic exercise, sleep and cognitive behavioural programme, which improves function even when pain persists.[11]
Complex regional pain syndrome type one follows a minor injury, sometimes so minor it is barely recalled, and presents with limb pain that is strikingly disproportionate to the stimulus, accompanied by sensory changes such as allodynia, vasomotor changes such as colour and temperature difference, and motor changes such as weakness or a guarded, held posture. There is no nerve lesion, which distinguishes type one from type two. The cornerstone is early, active mobilisation and graded sensory-motor therapy; prolonged immobilisation and escalating procedures worsen outcomes, and prompt interdisciplinary referral is key.[7]
Functional abdominal pain disorders are classified within the disorders of gut-brain interaction framework (Rome criteria). They present with recurrent abdominal pain, a normal work-up, and a pattern such as functional dyspepsia, irritable bowel syndrome, abdominal migraine or functional abdominal pain not otherwise specified. They affect around one in eight children and are managed with reassurance, a normal-eating, normal-activity approach, psychological therapy where disability is significant, and a deliberately limited role for medication.[12]
Chronic daily headache and chronic migraine in a child often involve medication overuse, typically of analgesics taken on fifteen or more days a month. The first step is to identify and withdraw the overused medication, establish a regular sleep, hydration and meal routine, and consider a preventive such as a tricyclic or, in older adolescents, an evidence-based modern preventive, alongside psychological therapy and a headache diary.[7]
Chronic secondary pain is managed alongside its cause. A child with chronic cancer-related pain is managed within a palliative and oncology framework with appropriate analgesia; a child with chronic postsurgical or posttraumatic pain combines treatment of any remediable cause with early rehabilitation to prevent sensitisation; a child with chronic neuropathic pain from a nerve injury receives mechanism-based therapy. In each, the secondary pain may need its own rehabilitation once the disease is controlled.[1][8]
Complications & Pitfalls
The complications of chronic primary pain are mostly iatrogenic, and naming them is part of the answer an examiner wants. The first is over-investigation: each repeated normal scan and each additional subspecialty referral reinforces the family's search for a hidden disease and the child's sick role, delays rehabilitation, and consumes years of the child's life. A confident, thorough, single assessment with a clear biopsychosocial explanation is the antidote.[7]
The second is opioid prescribing. An opioid started for chronic primary pain rarely helps and frequently harms, producing dependence, sedation, constipation, endocrine effects with long-term use, and a slide into lower function. The current consensus and the WHO 2020 guidance is to avoid initiating opioids for chronic primary pain in children and to deprescribe them where they have crept in.[7]
The third is reinforcing disability through the family and the system. Parental catastrophising and over-protection, a school that excuses all attendance, and a clinician who signs escalating medical certificates all entrench the sick role. The rehabilitation plan must actively realign all three around function and return to activity.[7]
The fourth is the opposite error: invalidation and dismissal. Telling a child with genuine central sensitisation that "it is all in your head" or "there is nothing wrong" breaks trust, drives the family away, and worsens outcomes. The skilful version is full validation of the pain as real and biologically generated, paired with a confident, evidence-based rehabilitation plan.[7]
Finally, medicalising normal variants such as benign joint hypermobility into a pain diagnosis can itself create disability where none existed; recognition and normalisation, with reactivation for any genuine symptoms, is the safer course.[7]
Prognosis & Disposition
Chronic primary pain in children is treatable, and many improve substantially with an interdisciplinary rehabilitation approach, though complete pain elimination is uncommon and should not be promised. The strongest predictor of persistence into adulthood is ongoing disability, untreated mood and anxiety, and school absence at the time of presentation, which is precisely why function, rather than pain intensity, is treated as the outcome that matters.[7][5]
Functional outcomes define success: a return to full-time school, restored sleep, re-engagement with friends and activity, and improved mood. A child who still has pain but is back at school, sleeping and socialising has had a successful treatment, and framing it this way for the family sets realistic, motivating goals.[7]
Most children with mild to moderate chronic primary pain can be managed in primary care or general paediatrics with a clear explanation, a graded activity and sleep plan, and access to psychology and physiotherapy. Referral to a specialist paediatric chronic pain service is indicated when the pain is severe, when disability is significant (especially school absence), when initial management has not worked, or when there are complex psychological or family factors. A small group with profound disability benefits from an intensive interdisciplinary rehabilitation programme, which shows gains in function and school return even when pain persists.[7][8]
The safety-net is explicit: the family is told the red flags that would warrant urgent review, and a scheduled follow-up is arranged to review function and adjust the plan, rather than an open door for escalating analgesia.[7]
Special Populations
Younger children express chronic pain differently, often through behaviour, sleep disturbance, school or nursery refusal, and parental report, and their management leans more on the family, simple distraction and play-based reactivation, and less on formal psychological therapy. Adolescents bring the full complexity of identity, school, peers, mood and online information, and benefit most from cognitive behavioural or acceptance-based therapy and a collaborative, autonomy-respecting approach.[7]
Chronic pain travels with, and is worsened by, anxiety, depression and neurodiversity. Children with autism, attention deficit hyperactivity disorder and learning disability may have atypical sensory and pain processing, and their plan must be adapted to their communication and sensory profile. These comorbidities are not distractions from the pain; they are part of its mechanism and its treatment.[7]
Adverse childhood experiences, maltreatment and socioeconomic disadvantage shape chronic primary pain through sustained stress-system activation and reduced access to the very resources, sleep, safety and routine, that recovery depends on. A trauma-informed approach and attention to the social determinants are part of competent care, not optional extras.[7]
In a child with a life-limiting illness, the frame shifts from primary to secondary and palliative pain. Here the disease is the driver, appropriate analgesia including opioids is legitimate and often necessary, and the goal shifts from rehabilitation to comfort and quality of life. The principles of this topic, the biopsychosocial assessment, attention to mood and family, and function-centred goals, still apply, but alongside active disease-directed and palliative symptom control.[8]
Transition to adult care is a high-risk moment. Adolescents with chronic primary pain entering adult services can fall between paediatric rehabilitation and adult pain medicine, lose their function, and be re-prescribed opioids. A planned transition, with a clear summary, a current rehabilitation plan, and a warm handover to an adult chronic pain service, protects the gains made in paediatrics.[7]
Evidence, Guidelines & Regional Differences
The intellectual foundation of this topic is the ICD-11 chronic pain classification, developed by an International Association for the Study of Pain task force, which for the first time gave chronic primary pain its own diagnostic home and was field-tested internationally with good clinician agreement.[1][3][4] The epidemiology rests on King and colleagues' systematic review and Huguet and Miro's severity study, which together establish both the high prevalence and the substantial minority with disabling pain.[5][6]
Clinical evidence
Population: Children and adolescents with chronic and recurrent pain
Key finding
Small but consistent reductions in pain and disability; benefit greatest for headache
Practice change
Psychological therapy is the best-evidenced intervention in paediatric chronic pain and is a first-line pillar of rehabilitation
The strongest treatment evidence is for psychological therapy. Cochrane systematic reviews show that psychological therapies, mainly cognitive behavioural therapy, reduce pain and disability in children and adolescents with chronic and recurrent pain, and that internet-delivered programmes extend this benefit with greater access.[9][10] By contrast, the evidence for pharmacological interventions in children with chronic primary pain is thin; much of the guidance is extrapolated from adults or built on small paediatric studies, and this uncertainty is itself the reason for therapeutic caution.[7]
The WHO 2020 guidelines on the management of chronic pain in children are the most authoritative single document and recommend physical and psychological therapies as the core, note the limited pharmacological evidence, and do not recommend initiating strong opioids for chronic primary pain. They are a key reference for candidates across all regions.[7]
Regional differences are mostly in service configuration rather than principle. Australia and Aotearoa New Zealand have dedicated paediatric chronic pain services in major centres and increasingly intensive interdisciplinary programmes, with a strong rehabilitation ethos and a cautious prescribing culture. The United Kingdom, through the Royal College of Paediatrics and Child Health and NICE guidance, shares the biopsychosocial and opioid-cautious approach. The United States and Canada also endorse interdisciplinary care but contend with higher baseline opioid exposure in some settings, making deprescribing a more prominent task. The shared spine everywhere is the biopsychosocial model and the avoidance of opioids for chronic primary pain.[7]
Controversies remain. The diagnosis of complex regional pain syndrome continues to generate debate, with criteria revised and a recognised risk of over-procedural management. Cannabis-based products for chronic pain attract family interest but lack paediatric evidence and are not recommended. The boundary between a normal variant and a pain disorder (for example benign hypermobility) is genuinely fuzzy and requires clinical judgement rather than a test.[7]
Exam Pearls
- Chronic pain in a child is pain lasting more than three months.[1]
- Chronic primary pain is nociplastic: the pain is the disease, with distress and disability and no better explanation.[2]
- Central sensitisation is the nervous system "wound up," which is why pain persists despite normal scans.[1]
- The three mechanisms are nociceptive, neuropathic and nociplastic; chronic primary pain is nociplastic.[1]
- Opioids are not recommended for chronic primary, non-cancer paediatric pain; function, not pain intensity, is the outcome.[7]
- The classic exam trap is over-investigating and over-prescribing for chronic primary pain instead of starting rehabilitation.[7]
- Juvenile fibromyalgia pairs widespread pain with fatigue, unrefreshing sleep and cognitive fog, and is commonly missed.[11]
- Psychological therapy, chiefly cognitive behavioural therapy, is the best-evidenced intervention in paediatric chronic pain.[9]
- Red flags that demand investigation are weight loss, night pain, neurological signs and systemic features.[7]
- Functional abdominal pain disorders affect about one in eight children and are the best-studied nociplastic model.[12]
PAIN-FREE
References
- [1]Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11) Pain, 2019.PMID 30586067
- [2]Nicholas M, Vlaeyen JWS, Rief W, et al. The IASP classification of chronic pain for ICD-11: chronic primary pain Pain, 2019.PMID 30586068
- [3]Treede RD, Rief W, Barke A, et al. A classification of chronic pain for ICD-11 Pain, 2015.PMID 25844555
- [4]Barke A, Korwisi B, Kasch H, et al. Classification of chronic pain for the International Classification of Diseases (ICD-11): results of the 2017 international field trial Pain, 2022.PMID 33863861
- [5]King S, Chambers CT, Huguet A, et al. The epidemiology of chronic pain in children and adolescents revisited: a systematic review Pain, 2011.PMID 22078064
- [6]Huguet A, Miro J The severity of chronic pediatric pain: an epidemiological study J Pain, 2008.PMID 18088558
- [7]Friedrichsdorf SJ, Giordano J, Desai Dakoji K, Warmuth A, Daughtry C, Schulz C Chronic Pain in Children and Adolescents: Diagnosis and Treatment of Primary Pain Disorders in Pediatrics Children (Basel), 2016.PMID 27973405
- [8]Friedrichsdorf SJ, Postier A, Eull D, et al. Multimodal pediatric pain management (part 2) Pain Manag, 2017.PMID 28103764
- [9]Fisher E, Heathcote L, Palermo TM, de C Williams AC, Lau J, Eccleston C Psychological therapies for the management of chronic and recurrent pain in children and adolescents Cochrane Database Syst Rev, 2018.PMID 30270423
- [10]Fisher E, Law E, Dudeney J, Palermo TM, Stewart G, Eccleston C Psychological therapies (remotely delivered) for the management of chronic and recurrent pain in children and adolescents Cochrane Database Syst Rev, 2019.PMID 30939227
- [11]Kashikar-Zuck S, King C, Ting TV Juvenile fibromyalgia: current status of research and future developments Nat Rev Rheumatol, 2014.PMID 24275966
- [12]Korterink JJ, Diederen K, Benninga MA, Tabbers MM, Hilbink M, Deckers-Kocken JM Epidemiology of pediatric functional abdominal pain disorders: a meta-analysis PLoS One, 2015.PMID 25992621