Paeds · pain-palliative-and-end-of-life-care
Opioid stewardship and complex analgesia
Also known as Paediatric opioid stewardship · Patient- and nurse-controlled analgesia in children · Opioid rotation and equianalgesic conversion in children · Opioid tolerance dependence and weaning · Naloxone for opioid-induced respiratory depression
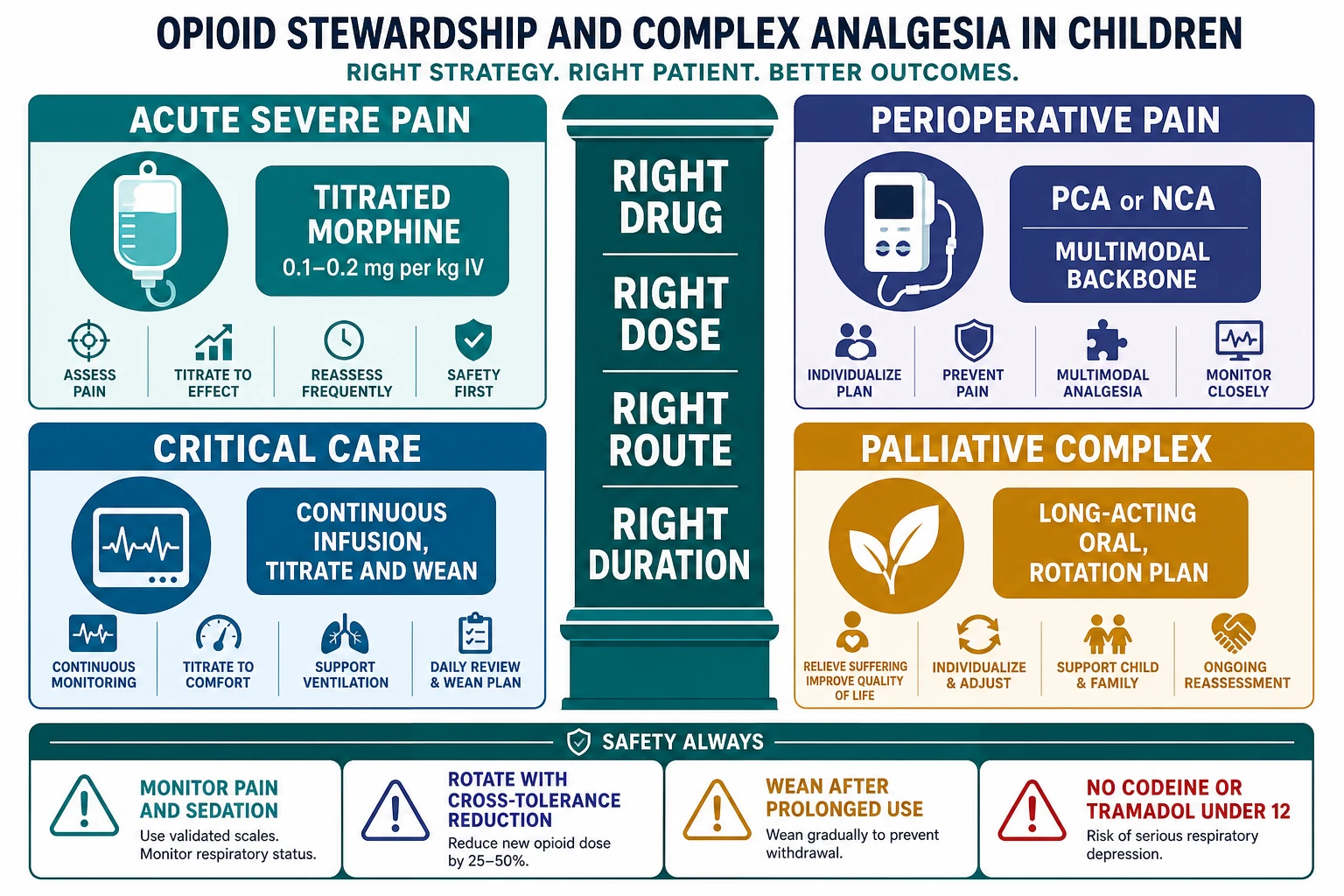
A fellowship approach to opioid stewardship and complex analgesia in a child: give the right opioid at the right weight-based dose by the right route for the right duration, anchor it on a non-opioid multimodal backbone, monitor with a pain score and a sedation score, rotate with the equianalgesic principle and the incomplete cross-tolerance reduction, and wean after prolonged use to avoid tolerance, withdrawal and opioid-induced hyperalgesia. Morphine is the first-line strong opioid at 0.1 to 0.2 mg per kg intravenously or 0.2 to 0.5 mg per kg orally every four hours. Patient- and nurse-controlled analgesia uses a morphine bolus of 10 to 20 microgram per kg with a 5 to 10 minute lockout and an optional low background infusion. Opioid rotation uses the equianalgesic principle that 10 mg intravenous morphine approximates 30 mg oral morphine, and the calculated new-opioid dose is reduced by 25 to 50 per cent for incomplete cross-tolerance; methadone conversion is non-linear and specialist-only. Naloxone for therapeutic over-sedation is 0.5 to 2 microgram per kg intravenously titrated to the respiratory rate. After about a week of continuous opioid, wean by 10 to 20 per cent of the established dose every one to two days. Codeine and tramadol are contraindicated under 12 and after tonsillectomy because a CYP2D6 ultrarapid metaboliser converts the prodrug to a fatal morphine overdose.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the child first. A seven-year-old wakes up after orthopaedic surgery with a backslab on a fractured femur, an opioid infusion running, and a pain score that is climbing. The question at the bedside is not "is this child on an opioid," because they already are — it is whether the opioid is the right drug, at the right dose, for the right duration, with the right monitoring, the right plan to rotate it if it stops working, and the right plan to wean it off. That bundle of judgements is opioid stewardship: the same idea as antibiotic stewardship, applied to the most effective and most dangerous analgesics we have. [10] [11]
An opioid relieves pain by agonising the mu-opioid receptor in the brain and spinal cord. Morphine is the prototype and the first-line strong opioid in children. Complex analgesia is the layer above simple weight-based dosing: it is what you do when a child needs an infusion, a patient- or nurse-controlled analgesia device, a rotation from one opioid to another, a structured wean after prolonged use, or a multimodal plan to spare opioid exposure. The discipline of this topic lives in four stewardship questions the prescriber asks at every handover: is the opioid still needed, is the dose right for the weight and the response, is the child being monitored for over-sedation, and is there a plan to stop it. [1] [11]
The unifying idea is that the opioid is powerful and unforgiving, and most of the harm is preventable. A child who is over-sedated, a child rotated without the cross-tolerance reduction, a child sent home with leftover opioid, and a child whose prolonged infusion is stopped abruptly are all the same failure in different costumes — the opioid was started without a plan for the whole journey. The exam answer is the workflow and the safety boundaries, not the arithmetic of a single dose: weigh, score the pain and the sedation, choose and titrate, monitor, rotate with the cross-tolerance reduction, and wean by a schedule. [10] [12]
Classification
Classify the opioid decision by the clinical job it has to do, because the job decides the agent, the route and the monitoring. Four jobs cover almost every child. Acute severe pain needs a titrated opioid, usually morphine, given in the emergency department, the ward or theatre. Perioperative and procedure-related pain needs a planned, multimodal, opioid-sparing pathway with a low-dose opioid for breakthrough and often a patient- or nurse-controlled analgesia device. Critical-care analgesia needs a continuous infusion, usually morphine or fentanyl, titrated to the pain and the sedation and weaned as the child recovers. Palliative and complex chronic pain needs long-acting oral morphine or a continuous infusion, breakthrough doses, and an explicit rotation and weaning plan with the specialist team. [1] [12]
Acute severe pain
Morphine IV, titrated
- Morphine 0.1 to 0.2 mg per kg intravenously, titrated to the pain score
- Monitor respiratory rate and sedation after every dose
- First-line for sickle crisis, severe trauma, postoperative breakthrough, renal colic
- Calculate from a measured weight, cap at the adult maximum, double-check
Perioperative pain
PCA or NCA + multimodal
- Regular paracetamol and an NSAID, a regional or local technique, a low-dose opioid
- PCA morphine bolus 10 to 20 microgram per kg, lockout 5 to 10 minutes
- Nurse-controlled analgesia for the child who cannot use a PCA
- The explicit goal is to minimise total opioid exposure
Critical-care analgesia
Continuous infusion
- Morphine or fentanyl infusion, titrated to pain and sedation scores
- Tolerance develops after about a week of continuous use
- Plan a structured wean or a methadone conversion before stopping
- Withdrawal is scored on the WAT-1 scale and avoided by a slow taper
Palliative complex pain
Long-acting oral or infusion
- Long-acting oral morphine or a continuous infusion for background pain
- Immediate-release opioid for breakthrough, at 10 to 20 per cent of the daily dose
- Rotation and weaning planned with the specialist palliative and pain team
- The opioid is one part of a biopsychosocial plan
The classification matters because it tells the candidate which safety boundaries bind. The child on an infusion or a PCA device is at risk of over-sedation and needs a sedation score. The child on a week or more of continuous opioid is at risk of tolerance and withdrawal and needs a wean. The child being rotated from one opioid to another is at risk of an over-conversion and needs the cross-tolerance reduction. And the child going home is at risk of leftover opioid and needs a limited quantity and a disposal plan. The agent changes; the stewardship loop does not. [4] [7]
Epidemiology & Risk Factors
Opioids are among the most commonly prescribed and most commonly implicated medicines in serious paediatric adverse drug events, and almost every event is preventable. The risk is concentrated in predictable children: the postoperative child on a PCA device, the PICU child on a prolonged infusion, the child with neurodisability who cannot report pain reliably, the oncology child with mucositis, and the adolescent discharged with a large opioid prescription after surgery. The 2024 AAP clinical practice guideline reframed the outpatient prescribing question precisely because leftover opioid from a surgical prescription is a leading entry point to adolescent opioid misuse and diversion. [10]
Child factors
- Pre-verbal or cognitively impaired children carry the highest risk of under-recognised pain and of over-sedation, because they cannot report either reliably
- Airway and sleep-disordered breathing (obstructive sleep apnoea) compound opioid respiratory depression
- Renal or hepatic impairment changes morphine metabolite clearance and pushes the dose down
- The neonate has immature clearance and accumulates active morphine metabolites
Drug and process factors
- A continuous opioid for about a week or more drives tolerance, dependence and withdrawal
- Equianalgesic rotation without the cross-tolerance reduction over-doses the child
- Parent-controlled analgesia by proxy (a parent pressing the button) has caused fatal over-sedation
- A large discharge prescription leaves leftover opioid in the home
System factors
- PCA errors from pump mis-programming or wrong concentration
- Care transitions where the monitoring and the wean are not re-handed-over
- Out-of-hours and remote prescribing with limited pharmacist and pain-team review
- Absence of a structured opioid-stewardship programme with audit and feedback
The pharmacogenetic risk sits in a subgroup the prescriber cannot identify at the bedside, which is why it is treated as a population-wide restriction. Codeine and tramadol are prodrugs activated by the cytochrome P450 enzyme CYP2D6. In a CYP2D6 ultrarapid metaboliser — roughly 5 to 10 per cent of people, varying by ancestry — a standard codeine or tramadol dose generates a flood of morphine, and the child develops opioid respiratory depression and apnoea. Because the genotype is invisible at the bedside, the FDA, the MHRA and the TGA contraindicate codeine and tramadol in children under 12 and in any child after tonsillectomy or adenoidectomy. The restriction governs every escalation step in this topic: there is no "weak opioid" rung for a young child, and morphine is used instead. [8]
Pathophysiology
Morphine agonises the mu-opioid receptor in the brain and spinal cord, dampening the perception of pain and the affective response to it. The same receptor sits on the respiratory centre in the medulla, and that is the single fact that makes opioids dangerous: the dose that relieves pain and the dose that depresses breathing are not far apart, and in a child the margin is narrower than in an adult. There is no analgesic ceiling for morphine, which is why it is titrated to the pain score and gated by a sedation score rather than capped at a fixed number. [8]
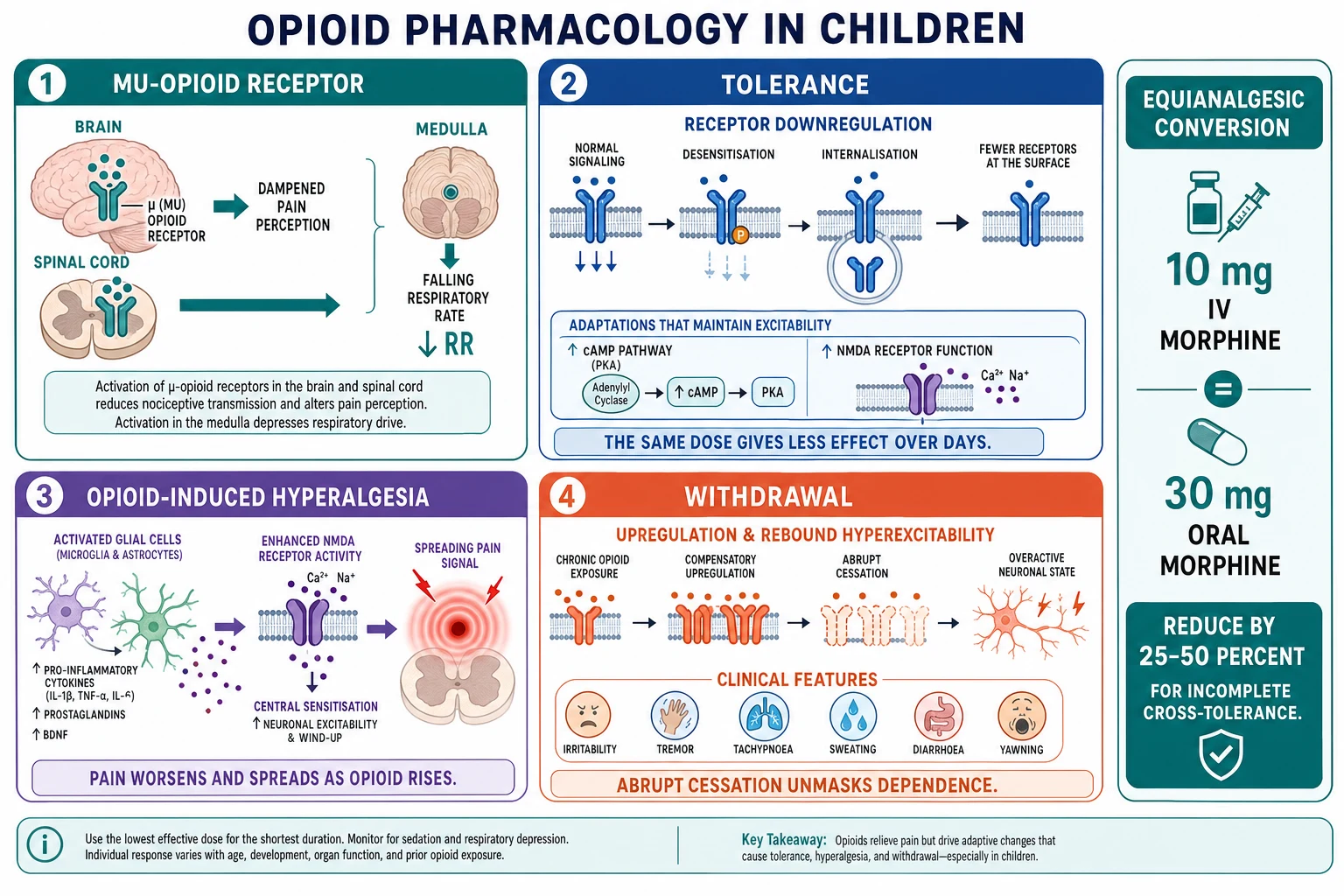
Three related but distinct phenomena drive the "complex" in complex analgesia, and the candidate must separate them before escalating a dose. Tolerance is the pharmacodynamic adaptation in which the same dose produces less effect over time: the mu-opioid receptor desensitises, downregulates and internalises, and downstream cAMP and NMDA signalling adapt, so the child needs more opioid for the same analgesia. Tolerance develops after about a week of continuous or regular opioid, most classically in the PICU child on a morphine or fentanyl infusion. Physical dependence is the matched adaptation that produces withdrawal if the opioid is stopped abruptly. Opioid-induced hyperalgesia is the paradoxical opposite of tolerance: as the opioid increases, the pain worsens and spreads, driven by glial activation and NMDA-mediated central sensitisation, and the correct response is to rotate or reduce the opioid and add an NMDA antagonist, not to escalate. [8]
The withdrawal syndrome is the unmasking of an upregulated signalling cascade when the opioid is removed too fast. The child becomes irritable and tremulous, sweats and yawns, breathes fast, develops diarrhoea and a rigid or hypertonic posture, and sleeps poorly. In the PICU this is scored on the WAT-1 (Withdrawal Assessment Tool version 1), a validated scale whose rising score tells the prescriber to slow the wean. The clinical point is that dependence is an expected pharmacological consequence of a legitimate treatment, not a moral failing and not addiction, and the defence against it is a structured, scheduled wean rather than an abrupt stop. [4]
The naloxone mechanism closes the pathophysiology. Naloxone is a competitive mu-opioid receptor antagonist that displaces morphine (and the other opioids) from the receptor, restoring the drive to breathe. Its half-life is shorter than the opioid it reverses — about 30 to 80 minutes against morphine's several hours — so a child who wakes up after a naloxone bolus can become over-sedated again as the antidote wears off. That single pharmacokinetic fact is why naloxone is given titrated to the respiratory rate in small increments, with repeat boluses or an infusion ready, rather than as a single "wake-up" dose. [8] [9]
Clinical Presentation
A child who needs complex analgesia presents in one of four ways, and the prescriber's first move is to recognise which. The first is the child with severe acute pain — the sickle crisis, the major trauma, the renal colic, the postoperative child — who needs a titrated opioid now. The second is the child on a PCA or NCA device after surgery, whose pain and sedation must be scored and whose device parameters must be understood. The third is the PICU child on a prolonged infusion who is recovering and needs a wean, or who is showing signs of tolerance or withdrawal. The fourth is the child with palliative or complex chronic pain whose opioid plan must be built around background analgesia, breakthrough doses and a rotation strategy. [1] [12]
The crucial bedside skill is to tell, within each presentation, the child who is comfortably analgesed from the child who is over-sedated or under-treated. The child who is comfortably analgesed has a controlled pain score and a normal or only mildly reduced sedation score, a normal respiratory rate for age, and is rousable. The over-sedated child has a rising sedation score, a falling respiratory rate, a small or unreactive pupil, and is hard to rouse — and this is the child who needs naloxone. The under-treated child has a high pain score but is fully awake, and this is the child who needs an opioid dose adjustment, not naloxone. The distinction is made on the combination of the pain score and the sedation score, never on either alone. [8] [9]
Comfortably analgesed
- Controlled pain score at the target
- Normal or mildly reduced sedation score, rousable
- Normal respiratory rate for age
- Plan continues; reassess at the expected onset
Over-sedated
- Rising sedation score, hard to rouse
- Falling respiratory rate, small or unreactive pupil
- Stimulate, support airway and breathing, give naloxone titrated to respiratory rate
- Monitor for recurrence; the opioid outlasts naloxone
Under-treated pain
- High pain score but fully awake and rousable
- Normal respiratory rate and sedation score
- Adjust the opioid dose or device parameters; reassess at onset
- Look for a worsening pain source or opioid-induced hyperalgesia
Withdrawing
- Irritability, tremor, sweating, tachypnoea, diarrhoea, yawning, hypertonia
- Rising WAT-1 score after a wean or abrupt cessation
- Slow or pause the wean; give the next opioid dose or a longer-acting agent
- Distinguish withdrawal from pain before escalating
Opioid tolerance and hyperalgesia declare themselves at the bedside in opposite directions. The tolerant child needs an escalating infusion to hold the same pain score, because the receptor has adapted; the hyperalgesic child has pain that worsens and spreads beyond the original site as the opioid increases, because the central nervous system has sensitised. The trap is to read both as "needs more opioid" — correct for tolerance, harmful for hyperalgesia. The discriminator is the pattern: tolerance raises the dose for the same analgesia at the same site; hyperalgesia spreads the pain and lowers the pain threshold everywhere, and it improves when the opioid is reduced or rotated and an NMDA antagonist such as ketamine is added. [8]
Differential Diagnosis
When a child's pain or distress changes on an opioid, build the differential in a fixed order before changing the dose. First, is the pain source itself progressing — a surgical complication, an ischaemic limb, a new infection, a full bladder, a tight cast, constipation? Second, is the dose inadequate or under-titrated for the weight and the response? Third, has tolerance developed so the same dose no longer suffices, or has opioid-induced hyperalgesia developed so more opioid makes the pain worse? Fourth, is the child distressed for a non-pain reason — hypoxia, hypercapnia, hypoglycaemia, delirium, anxiety, separation — that the opioid will not fix? The disciplined answer changes the dose only after the source, the dose and the tolerance-or-hyperalgesia question have each been answered. [11] [12]
Pain source progressing
- Surgical complication, compartment syndrome, ischaemia, infection, fracture displacement
- Full bladder, tight cast, blocked catheter, constipation
- Examine the child and the site before escalating the opioid
- Source control is the definitive treatment, not the opioid
Dose inadequate
- Under-titration for weight or for the severity of the pain
- Wrong concentration or a pump mis-programmed on the PCA
- Dose given but not yet absorbed — onset is slower orally than intravenously
- Reassess at the expected onset and titrate to the score
Tolerance or hyperalgesia
- Tolerance: escalating dose for the same pain at the same site, over a week or more
- Hyperalgesia: pain worsens and spreads as the opioid rises, with allodynia
- Tolerance may justify an increase; hyperalgesia justifies rotation or reduction and an NMDA antagonist
- Review the cumulative opioid exposure and the duration
Non-pain distress
- Hypoxia, hypercapnia, hypoglycaemia, sepsis, delirium, anxiety, separation
- Check oxygen, glucose and the conscious level
- Treat the cause; an opioid will not fix hypoxia or delirium
- Distinguish sedation from over-sedation on the sedation score
The discriminator between withdrawal and pain in a PICU child who is agitated is the timing and the score. Withdrawal appears after a wean or an abrupt cessation, is scored on the WAT-1, and quiets with a dose of opioid or benzodiazepine; pain appears at the source, is scored on the pain tool, and quiets with analgesia directed at the source. A trial — pause the wean or give a breakthrough dose and observe — separates them, and the specialist team is involved early when the picture is mixed. The same disciplined approach keeps the prescriber from the two opposite errors of an over-sedated child (escalating when the answer was to look for the source) and a withdrawing child (escalating when the answer was to slow the wean). [4]
Clinical & Bedside Assessment
The bedside assessment of the opioid-exposed child rests on three numbers, taken together: the pain score, the sedation score, and the respiratory rate. Pain is scored with an age-appropriate, validated tool — FLACC or revised FLACC for the pre-verbal or cognitively impaired child, a numeric or faces scale for the school-age child — because the clinician's and carer's estimates systematically under-rate a child's pain. Sedation is scored with a structured tool such as the University of Michigan Sedation Scale or the Pasero Opioid Sedation Scale, because a rising sedation score is the earliest sign of opioid over-sedation and precedes the fall in respiratory rate. The respiratory rate for age is counted over a full minute. The next opioid bolus is gated on the combination: a high pain score with a low sedation score gets the next dose, a low pain score with a rising sedation score holds it. [1] [8]
The focused history frames the opioid choice and the monitoring. Establish the age and the measured weight; the source and the severity of the pain; the cumulative opioid exposure and the duration (to gauge tolerance and dependence); the renal and hepatic function; any concurrent sedative (benzodiazepines, antihistamines, anticonvulsants); airway and sleep-disordered breathing; allergy; and, for the child being rotated, the current opioid, its route, its dose and its duration. The synthesis the candidate speaks and documents is the problem representation: the child's age and weight, the pain problem and its score, the chosen opioid and the calculated dose, the route, the monitoring plan, the stewardship check (is it still needed, for how long), and the reassessment plan. Every prescription is written with a leading zero (0.5 mg, never .5 mg) and never a trailing zero (5 mg, never 5.0 mg), and every opioid is double-checked independently. [10] [11]
Investigations
Most children on an opioid are managed on the pain and sedation scores without specific investigations, because the analgesic decision is clinical. Investigations serve two purposes: to frame the safety of the opioid, and to identify the cause of a changing pain picture. Renal function matters because morphine is cleared to active metabolites (morphine-3-glucuronide and morphine-6-glucuronide) that accumulate in renal impairment and prolong respiratory depression; fentanyl, by contrast, has no active metabolites and is preferred in renal failure. Liver function matters because the opioid and the paracetamol that sits alongside it are both hepatically handled. A coagulation screen matters if a regional technique is planned. [3] [11]
For the child on an infusion or a PCA device at raised risk, continuous monitoring is added. Pulse oximetry is the floor, but it is a late and unreliable signal of opioid over-sedation, because a child retainers of carbon dioxide can keep oxygen saturations near normal until late. Capnography (end-tidal carbon dioxide) detects the rising carbon dioxide of early respiratory depression earlier and is used for the high-risk child — the infant on an infusion, the child on a background infusion, the child on a combination of opioid and sedative. The WAT-1 or the Sophia Observation withdrawal Symptoms scale is scored daily during a wean to detect withdrawal early and adjust the taper. A bedside glucose is taken early in any over-sedated or altered child, because hypoglycaemia mimics opioid sedation and is rapidly reversible. [4] [8]
Management — Resuscitation
Resuscitation in this topic is the immediate management of opioid-induced respiratory depression. The approach is constant and the order is fixed: assess and support the airway and breathing, then reverse the opioid. Stimulate the child, open and position the airway, give bag-valve-mask support with oxygen if the respiratory effort is inadequate, and call for senior or intensive-care help for the young, the deeply sedated, or the child who is not responding. Only then is naloxone given, and it is given titrated to the respiratory rate, not to full reversal. [8] [9]
The reasoning behind titration is the reasoning behind the whole topic. A child given a large naloxone bolus to "wake them up" is thrust into acute pain and withdrawal, the opioid is displaced all at once, and the analgesic work of hours is undone; within a short time the naloxone wears off and the child is over-sedated again, now in a worse state. The titrated approach gives just enough naloxone to restore the drive to breathe, leaves the analgesia intact, and pairs the reversal with a plan to reduce the opioid and address the cause. A non-opioid cause of deterioration — hypoxia, hypoglycaemia, sepsis, raised intracranial pressure — is excluded in parallel, because attributing an altered child to the opioid without checking the glucose and the oxygen is a classic error. [8] [9]
Management — Definitive & Stepwise
Definitive management is built in four layers, each of which the candidate must be able to recite: the weight-based opioid, the PCA or NCA device, the multimodal opioid-sparing backbone, and the rotation and weaning plan. The first layer is the weight-based opioid. Morphine is the first-line strong opioid: 0.1 to 0.2 mg per kg intravenously, titrated to the pain score and monitored for sedation and respiratory rate, or 0.2 to 0.5 mg per kg orally every four hours. Oxycodone is an alternative oral opioid at 0.1 to 0.2 mg per kg every four to six hours. Fentanyl, 0.5 to 1 microgram per kg intravenously, is preferred for short procedural analgesia and in renal failure. Every dose is calculated from a measured weight and capped at the adult maximum. [1] [10]
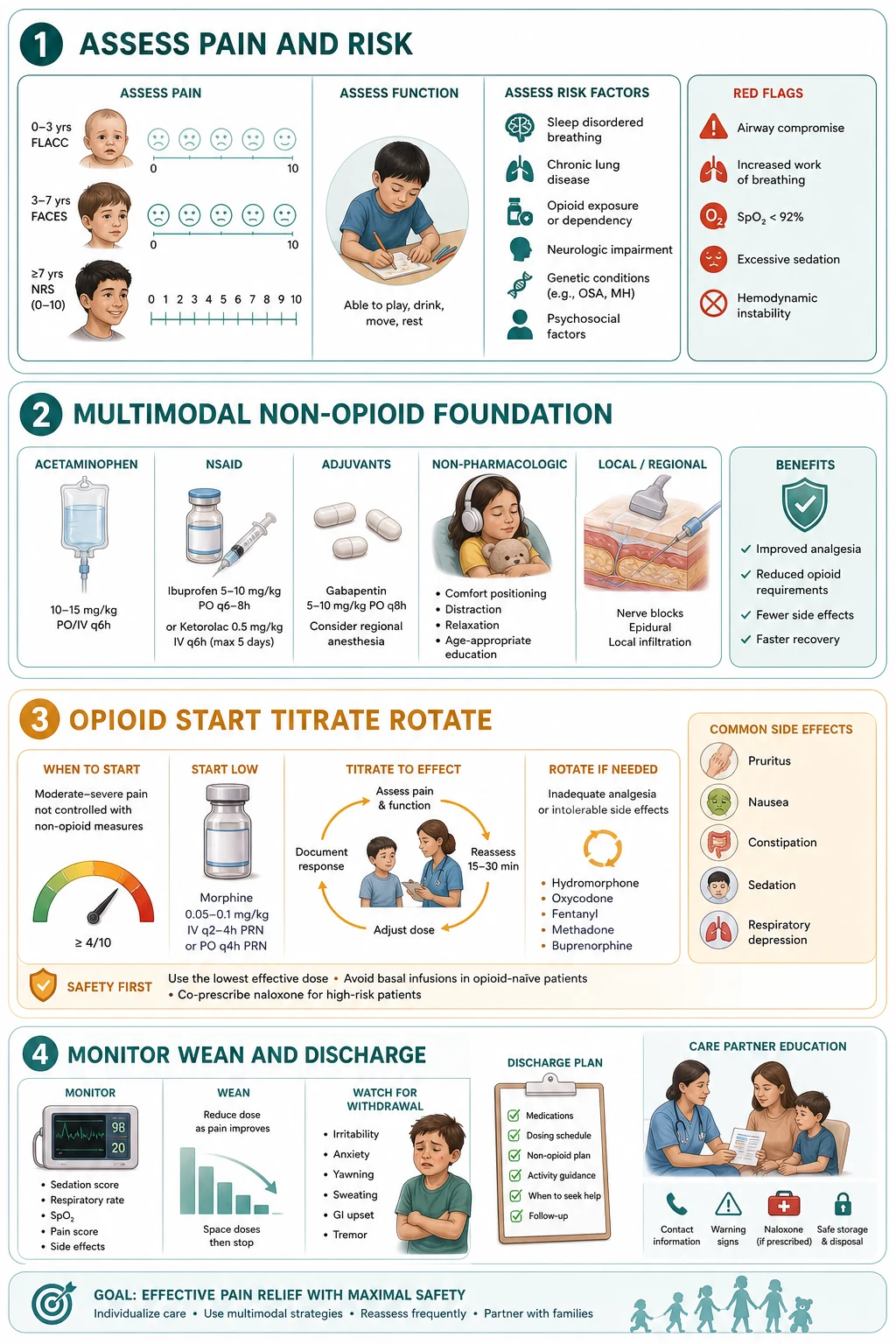
The second layer is the PCA or NCA device, which is the modern standard for postoperative and ongoing moderate-to-severe pain in a child old enough, or supervised closely enough, to use one. A patient-controlled analgesia (PCA) device delivers a morphine bolus of 10 to 20 microgram per kg on demand, with a lockout of 5 to 10 minutes that prevents re-dosing within the window, and an optional low background infusion of 0 to 4 microgram per kg per hour for some children. The safety logic of PCA is that the child presses the button, and a child who is becoming over-sedated stops pressing — the device has a built-in feedback loop. A nurse-controlled analgesia (NCA) extends the same principle to the infant or young child, or the child who cannot understand the device: the nurse assesses the child and presses the button, and a background infusion is more often used. Parent-controlled analgesia by proxy is restricted: a parent pressing the button for a child has broken the safety feedback loop and has caused fatal over-sedation, so parent-by-proxy is not permitted outside an approved nurse- or parent-controlled protocol with strict criteria. [1] [2]
Layer 1 — Weight-based opioid
Morphine 0.1 to 0.2 mg per kg intravenously, titrated to the pain score and gated by the sedation score, or 0.2 to 0.5 mg per kg orally every four hours. Oxycodone 0.1 to 0.2 mg per kg orally every four to six hours as an alternative; fentanyl 0.5 to 1 microgram per kg intravenously for procedures or renal failure. Calculate from a measured weight, cap at the adult maximum, double-check.
Layer 2 — PCA or NCA device
Morphine bolus 10 to 20 microgram per kg, lockout 5 to 10 minutes, optional low background infusion 0 to 4 microgram per kg per hour. PCA for the child who can use the device (commonly from about six or seven years); NCA for the infant or young child. No parent-controlled analgesia by proxy outside an approved protocol.
Layer 3 — Multimodal opioid-sparing backbone
Regular paracetamol and an NSAID (where not contraindicated), a regional or local anaesthetic technique, an NMDA antagonist such as ketamine, and an alpha-2 agonist such as dexmedetomidine or clonidine, with gabapentinoids for neuropathic pain. The explicit goal is to reduce total opioid exposure.
Layer 4 — Rotation and weaning plan
Rotate with the equianalgesic principle (10 mg intravenous morphine to 30 mg oral morphine), reducing the calculated new-opioid dose by 25 to 50 per cent for incomplete cross-tolerance; methadone is specialist-only and non-linear. After about a week of continuous opioid, wean by 10 to 20 per cent of the established dose every one to two days, guided by the WAT-1 score.
Safety boundaries at every layer
Write a leading zero and no trailing zero, double-check every opioid, monitor the pain and the sedation score, restrict parent-by-proxy to NCA, avoid codeine and tramadol under 12 and after tonsillectomy, and keep naloxone at the bedside for the infusion and the PCA child.
The third layer is the multimodal opioid-sparing backbone, and it is the single most evidence-based stewardship move. Regular paracetamol and an NSAID (where not contraindicated by renal impairment, bleeding risk or aspirin-sensitive asthma) form the backbone; a regional or local anaesthetic technique targets the surgical site; an NMDA antagonist such as ketamine reduces opioid tolerance and opioid-induced hyperalgesia; an alpha-2 agonist such as dexmedetomidine or clonidine adds analgesia and sedation; and a gabapentinoid helps where neuropathic pain is a feature. The explicit goal is to minimise total opioid exposure, which both improves recovery and reduces opioid-related adverse effects — the postoperative pain guideline made multimodal opioid-sparing analgesia the standard for exactly this reason. [11]
The fourth layer is the rotation and weaning plan, and this is where "complex" earns its name. Opioid rotation is moving from one opioid to another when the first is ineffective or producing adverse effects, and it rests on the equianalgesic principle: as a working figure, 10 mg of intravenous morphine is approximately equianalgesic to 30 mg of oral morphine. The crucial safety step, and the one the examiner tests, is that the calculated equianalgesic dose of the new opioid is then reduced by 25 to 50 per cent for incomplete cross-tolerance, because a child tolerant to one opioid is not fully tolerant to another, and a straight equianalgesic conversion over-doses them. Methadone is the exception: its conversion ratio to morphine is non-linear (it steepens as the prior opioid dose rises) and its long and variable half-life accumulates, so methadone rotation is specialist-only, in palliative and complex-care settings, with the specialist pain or palliative team. [5] [7]
In Australia and Aotearoa New Zealand, the Royal Children's Hospital Melbourne guidelines and the AMH Children's Dosing Companion are the bedside references: morphine 0.1 to 0.2 mg per kg intravenously or 0.2 to 0.5 mg per kg orally every four hours; PCA morphine bolus 10 to 20 microgram per kg with a 5 to 10 minute lockout and an optional low background; fentanyl 0.5 to 1 microgram per kg intravenously. Naloxone is dosed at 0.5 to 2 microgram per kg intravenously titrated to respiratory rate. The TGA restricts codeine and tramadol in children under 12 and after tonsillectomy. [1] [9]
Specific Subtypes & Scenarios
The postoperative child is the archetype of modern opioid-sparing analgesia. Regular paracetamol and an NSAID form the backbone, a regional or local anaesthetic technique targets the surgical site, and a low-dose opioid — morphine by PCA where the child is old enough, or oxycodone orally — is reserved for breakthrough. The explicit goal is to minimise total opioid exposure, and the historical "weak opioid" rung (codeine, tramadol) is replaced by low-dose morphine because the prodrug opioids are restricted. The child on a PCA is monitored with a pain score, a sedation score and a respiratory rate, and the device parameters are reviewed at every handover. [1] [11]
The PICU child on a prolonged infusion is the archetype of tolerance and weaning. After about a week of continuous morphine or fentanyl, the child is tolerant and physically dependent, and stopping abruptly produces withdrawal. The structured approach, supported by the systematic review of paediatric critical-care weaning protocols, is to convert the intravenous opioid to an oral long-acting equivalent (or to methadone by a validated protocol) and to taper by about 10 to 20 per cent of the established dose every one to two days, guided by the WAT-1 score. The methadone protocols developed for this purpose — the pharmacist-managed taper and the exposure-based methadone and lorazepam weaning protocol — reduce the wean length and the withdrawal burden when used by a specialist team. [4] [5] [6]
Postoperative child
- Multimodal opioid-sparing: paracetamol, NSAID, regional technique
- Low-dose morphine by PCA or oxycodone orally for breakthrough
- No codeine or tramadol
- Monitor pain score, sedation score and respiratory rate; review at handover
PICU prolonged infusion
- Tolerant and dependent after about a week of continuous opioid
- Convert to oral long-acting morphine or methadone by protocol
- Taper 10 to 20 per cent every one to two days, guided by the WAT-1
- Avoid abrupt cessation — withdrawal is iatrogenic and preventable
Oncology and mucositis
- Severe mucositis pain managed with morphine by PCA or NCA
- Background infusion more often used for continuous severe pain
- Systematic review supports PCA and NCA safety with monitoring
- Coordinate with oncology and the specialist pain team
Palliative and complex chronic
- Long-acting oral morphine or a continuous infusion for background pain
- Immediate-release opioid for breakthrough at 10 to 20 per cent of the daily dose
- Rotation and weaning planned with the palliative and pain team
- Methadone as a specialist non-linear option
The oncology child with severe mucositis is managed with morphine by PCA or NCA, and the systematic review of intravenous opioids for chemotherapy-induced mucositis pain confirms that PCA and NCA, with structured monitoring, are effective and safe for this severe, continuous pain. A background infusion is more often used here because the pain is constant, and the breakthrough doses are matched to the mucositis course, with the specialist pain and oncology teams coordinating. The neonate is dosed with weight-banded figures from a neonatal formulary, with careful monitoring for apnoea, because the morphine metabolites accumulate and clearance is immature; sucrose and non-pharmacological measures anchor procedural pain, and the Cochrane review of systemic opioid regimens for neonatal postoperative pain underpins the cautious, monitored approach. [2] [3]
The palliative and complex chronic pain child extends the framework upward and sideways rather than simply increasing the opioid. Background analgesia uses a long-acting oral morphine or a continuous infusion; breakthrough doses are an immediate-release opioid at about 10 to 20 per cent of the total daily dose; and the rotation and weaning plan is built with the specialist palliative and pain team, because the opioid is one part of a biopsychosocial plan that includes non-pharmacological measures, disease-modifying therapy, psychological support, and the family. The principle that unifies all four scenarios is the same: the right opioid at the right dose for the right duration, on a multimodal backbone, with a rotation and weaning plan, monitored at every step. [12]
Complications & Pitfalls
The preventable errors cluster at predictable points, and naming them is half of avoiding them. The first is over-sedation and respiratory depression, prevented by gating every opioid bolus on the sedation score and keeping naloxone at the bedside for the infusion and the PCA child. The second is the equianalgesic rotation without the cross-tolerance reduction, which over-doses the child; the defence is the 25 to 50 per cent reduction every time, with methadone left to the specialist. The third is abrupt cessation after prolonged use, which produces withdrawal; the defence is the structured 10 to 20 per cent wean. The fourth is parent-controlled analgesia by proxy outside an approved NCA protocol, which has caused fatal over-sedation; the defence is the rule that only the nurse (or a trained parent in a strict protocol) presses the button. [1] [7]
OPIATE
The tolerance-versus-hyperalgesia trap deserves restating, because it is the error that escalates the opioid when the answer is to reduce it. A child whose pain worsens as the opioid rises may have opioid-induced hyperalgesia, not tolerance, and the discriminator is the spread of pain beyond the original site with allodynia. The correct response is to rotate or reduce the opioid and add an NMDA antagonist such as ketamine, not to escalate the dose. The discharge trap is the child sent home with a large opioid prescription and no disposal plan; the AAP clinical practice guideline reframed outpatient prescribing around the smallest effective quantity, a written dose in milligrams, and clear advice to dispose of leftover opioid, because the home prescription is a leading entry point to adolescent misuse and diversion. [8] [10]
Prognosis & Disposition
Outcome in opioid-induced respiratory depression is driven almost entirely by the speed of naloxone and the availability of monitoring. A child who is stimulated, supported and given titrated naloxone early, with monitoring for recurrence, does well — the episode is reversed and the analgesia is preserved. Delay, a large "wake-up" naloxone bolus that throws the child into pain and withdrawal, or a missed non-opioid cause of the deterioration (hypoxia, hypoglycaemia), shift the outcome toward harm. The disposition of the over-sedated child is therefore conservative: reverse to a breathing child, reduce the opioid, address the cause, and observe for the duration the opioid can recur — longer for the long-acting agents and methadone. [8] [9]
For the tolerant and dependent child, the prognosis is driven by the structure of the wean. A planned, scheduled taper by 10 to 20 per cent every one to two days, guided by the WAT-1 score and supported by the specialist team, produces a smooth transition off the opioid with minimal withdrawal. An abrupt stop or a too-rapid wean produces a withdrawal syndrome that sets the recovery back and erodes trust. The disposition includes an outpatient follow-up plan and, for the palliative or complex-chronic child, a written opioid-rotation and weaning plan shared with the family and the GP. The discharge safety-net names the features that should bring the child back — increasing drowsiness, slow or shallow breathing, unrousability, worsening pain — and a disposal plan for any leftover opioid. [4] [10]
Special Populations
The neonate is dosed with weight-banded figures from a neonatal formulary, with careful monitoring for apnoea, because the morphine glucuronide metabolites accumulate in the immature kidney and clearance is prolonged. Sucrose, breastfeeding and non-nutritive sucking anchor procedural pain, and the Cochrane review of systemic opioid regimens for neonatal postoperative pain underpins the cautious, monitored approach to neonatal opioid therapy. The child with neurodisability or cognitive impairment is assessed with the revised FLACC, carries a low threshold to treat pain, and benefits from a written opioid plan shared across carers and settings, because under-treated pain and unrecognised over-sedation are both failure modes and a structured plan is the defence. [3] [11]
The child with renal impairment is managed without the active morphine metabolites where possible — fentanyl is preferred to morphine in renal failure because it has no active metabolites — and the opioid is titrated carefully and monitored, because the metabolites that accumulate in renal failure prolong respiratory depression. The child with hepatic impairment carries a lower clearance and a cautious titration. The adolescent is managed with attention to safe prescription quantity, leftover-opioid risk and transition to adult services, because the discharge prescription is the leading entry point to misuse and the codeine and tramadol restriction still applies. The Indigenous, remote, migrant or socioeconomically disadvantaged family is supported with clear dosing instructions, accessible language, follow-up the family can reach, and culturally safe communication, because the safety-net only closes if the family can act on it, and the home-disposal plan is part of the prescription. [10] [12]
Evidence, Guidelines & Regional Differences
The evidence base is strongest where the stakes are highest. The AAP opioid-prescribing clinical practice guideline (Hadland 2024) reframed outpatient prescribing around the smallest effective quantity for acute pain, the avoidance of codeine and tramadol, and the safe disposal of leftover opioid, because the home prescription is a leading entry point to adolescent misuse. The Cochrane review of opioid switching (Quigley 2004) established that switching opioids can improve pain relief and tolerability in the tolerant patient, while cautioning that the evidence base for the conversion ratios is limited and the cross-tolerance reduction is mandatory. The methadone weaning protocols (Steineck 2014; Wilson 2021) showed that a structured, pharmacist- or exposure-based methadone taper shortens the wean and reduces the withdrawal burden in the PICU child. [5] [7] [10]
Opioid prescribing for acute pain in children (Hadland 2024, AAP clinical practice guideline)
Key finding
The AAP clinical practice guideline recommends the smallest effective opioid quantity for acute paediatric pain, preferential non-opioid multimodal analgesia, the avoidance of codeine and tramadol in children under 12 and after tonsillectomy, and explicit counselling and disposal of leftover opioid.
Patient- and nurse-controlled analgesia in a paediatric hospital (Donado 2019, 22-year experience)
Key finding
Over 22 years and many thousands of children, morphine by PCA and NCA was effective for moderate-to-severe pain with a low rate of serious adverse events when paired with structured monitoring, a sedation score, and the restriction of parent-by-proxy to approved nurse-controlled protocols.
Regional formularies converge on the doses but differ at the edges. The RCH Melbourne guidelines, the AMH Children's Dosing Companion and the BNFc agree on the morphine weight-based doses, the PCA parameters and the naloxone titration. They converge on the codeine and tramadol restriction under 12 and after tonsillectomy. They differ in the detail of background PCA infusions and in the local methadone protocol, which is governed by the specialist palliative or pain team and a written institutional pathway. The equianalgesic principle with the cross-tolerance reduction, and the structured wean after prolonged use, are the unifying framework across regions. Where the evidence is genuinely thin — the exact methadone conversion ratio, the routine use of background PCA infusions, the long-term neuropsychological outcomes of PICU opioid exposure — the prescriber names the uncertainty and defers to the specialist team and the local protocol. [5] [7]
Exam Pearls
Self-test — the rotation trap
A 10-year-old on a morphine infusion for a sickle crisis has rising pain despite escalating doses, and the pain is now spreading beyond the original site with allodynia. The registrar proposes a 1:1 equianalgesic rotation to oral morphine. What is wrong, and what is the correct plan? [7]
Two things are wrong. First, the pain pattern — worsening and spreading with allodynia as the opioid rises — is opioid-induced hyperalgesia, not simple tolerance, so escalating or rotating to a higher equianalgesic dose will worsen it; the correct first move is to reduce or rotate the opioid and add an NMDA antagonist such as ketamine. Second, any rotation must apply the incomplete cross-tolerance reduction: the calculated equianalgesic dose of the new opioid is reduced by 25 to 50 per cent, never given as a 1:1 conversion. Methadone would be specialist-only and non-linear. Reassess the pain source, address tolerance-versus-hyperalgesia, rotate with the cross-tolerance reduction, and involve the specialist pain team. [7] [8]
The high-yield one-liners: the opioid is titrated because there is no analgesic ceiling, and it is dangerous because the analgesic and the respiratory-depressant doses are close. Tolerance develops after about a week of continuous opioid; hyperalgesia worsens pain as the opioid rises and is treated by rotation or reduction, not escalation. The equianalgesic conversion always carries a 25 to 50 per cent cross-tolerance reduction; methadone is non-linear and specialist-only. Naloxone is titrated to the respiratory rate and the opioid outlasts it, so recurrence is expected and an infusion is readied. Parent-controlled analgesia by proxy is restricted to nurse-controlled analgesia. The discharge defence is the smallest effective quantity, a written dose in milligrams, and a disposal plan for the leftover opioid. And the single question that prevents most over-sedation disasters is the one the prescriber asks before every bolus: what is the sedation score, and what is the respiratory rate? [1] [9]
References
- [1]Donado C, Solodiuk J, Rangel SJ, et al. Patient- and Nurse-Controlled Analgesia: 22-Year Experience in a Pediatric Hospital Hospital Pediatrics, 2019.PMID 30655310
- [2]Walker SM, Selers EL, Jay MA, et al. Intravenous opioids for chemotherapy-induced severe mucositis pain in children: Systematic review and single-center case series of management with patient- or nurse-controlled analgesia (PCA/NCA) Paediatric Anaesthesia, 2022.PMID 34731511
- [3]Kinoshita M, Borges do Nascimento IJ, Styrmisdóttir L, et al. Systemic opioid regimens for postoperative pain in neonates Cochrane Database of Systematic Reviews, 2023.PMID 37018131
- [4]Bichaff P, Setani KT, Motta EHG, et al. Opioid tapering and weaning protocols in pediatric critical care units: a systematic review Revista da Associacao Medica Brasileira, 2018.PMID 30517238
- [5]Steineck KJ, Skoglund AK, Carlson MK, et al. Evaluation of a pharmacist-managed methadone taper Pediatric Critical Care Medicine, 2014.PMID 24448326
- [6]Wilson AK, Ragsdale CE, Sehgal I, et al. Exposure-Based Methadone and Lorazepam Weaning Protocol Reduces Wean Length in Children The Journal of Pediatric Pharmacology and Therapeutics, 2021.PMID 33424499
- [7]Quigley C Opioid switching to improve pain relief and drug tolerability Cochrane Database of Systematic Reviews, 2004.PMID 15266542
- [8]Bateman JT, Saunders SE, Levitt ES, et al. Understanding and countering opioid-induced respiratory depression British Journal of Pharmacology, 2023.PMID 34089181
- [9]Saari TI, Strang J, Dale O, et al. Clinical Pharmacokinetics and Pharmacodynamics of Naloxone Clinical Pharmacokinetics, 2024.PMID 38485851
- [10]Hadland SE, Agarwal R, Raman SR, et al. Opioid Prescribing for Acute Pain Management in Children and Adolescents in Outpatient Settings: Clinical Practice Guideline Pediatrics, 2024.PMID 39344439
- [11]Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of Postoperative Pain: A Clinical Practice Guideline From the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists' Committee on Regional Anesthesia, Executive Committee, and Administrative Council The Journal of Pain, 2016.PMID 26827847
- [12]Norris S, Minkowitz S, Scharbach K, et al. Pediatric Palliative Care Primary Care, 2019.PMID 31375193