Paeds · pain-palliative-and-end-of-life-care
Paediatric palliative care principles and referral
Also known as Paediatric palliative care · Children's palliative care · Palliative care principles in children · PPC referral and the parallel-care model · ACT categories of life-limiting conditions · Together for Short Lives framework
Fellowship-level approach to the principles and referral of paediatric palliative care: the WHO definition, the parallel-care model, the four Together for Short Lives (ACT) categories of life-limiting and life-threatening conditions, the epidemiology of serious paediatric suffering, the referral triggers including the Paediatric Palliative Screening Scale (PaPaS), the whole-child and family assessment across the four domains, care across home, hospital and hospice, bereavement follow-through, and the regional models across ANZ, the UK, the US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture the eight-year-old six months into treatment for high-risk neuroblastoma whose pain is now waking him at night, the four-year-old with severe cerebral palsy and recurrent aspiration pneumonia whose mother is exhausted, and the neonate with a prenatally diagnosed trisomy 18 in the delivery room. These three children share one thing: each has a life-limiting or life-threatening condition that would be eased by a palliative approach, and each is at risk of receiving it too late. [1] [3]
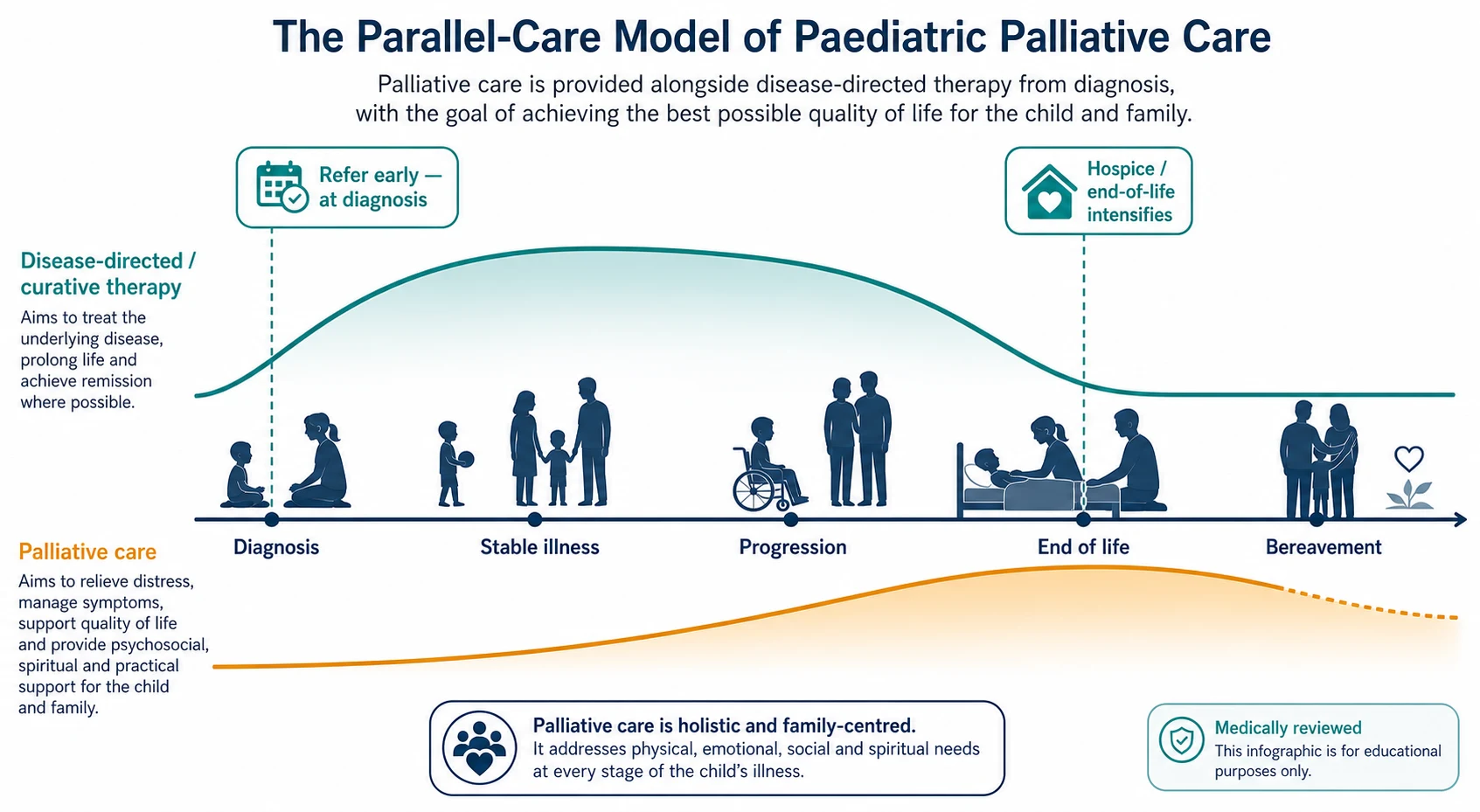
The World Health Organization defines palliative care for children as the active total care of the child's body, mind and spirit, and it adds that this care also involves giving support to the family. It begins when illness is diagnosed, and it continues regardless of whether a child receives treatment directed at the disease. That last clause is the whole point: palliative care is not what you switch to when cure fails — it is a layer you add at diagnosis and carry through the illness. [5] [7]
The discipline rests on three commitments. It relieves suffering in four interacting domains — physical symptoms, psychological distress, social and family circumstance, and spiritual or existential concern. It treats the family as the unit of care, because the child's suffering and the family's coping shape each other. And it is delivered by a multidisciplinary team, in whatever setting best meets the child's needs — home, ward, intensive care, hospice or school. [4] [5]
Classification
The fastest way to decide whether a child needs a palliative approach is to ask what kind of serious illness they have and what its trajectory looks like. The Together for Short Lives framework (originally the ACT categories) sorts life-limiting and life-threatening conditions into four groups by the shape of the illness, and each group tells you when palliative care fits. [10]
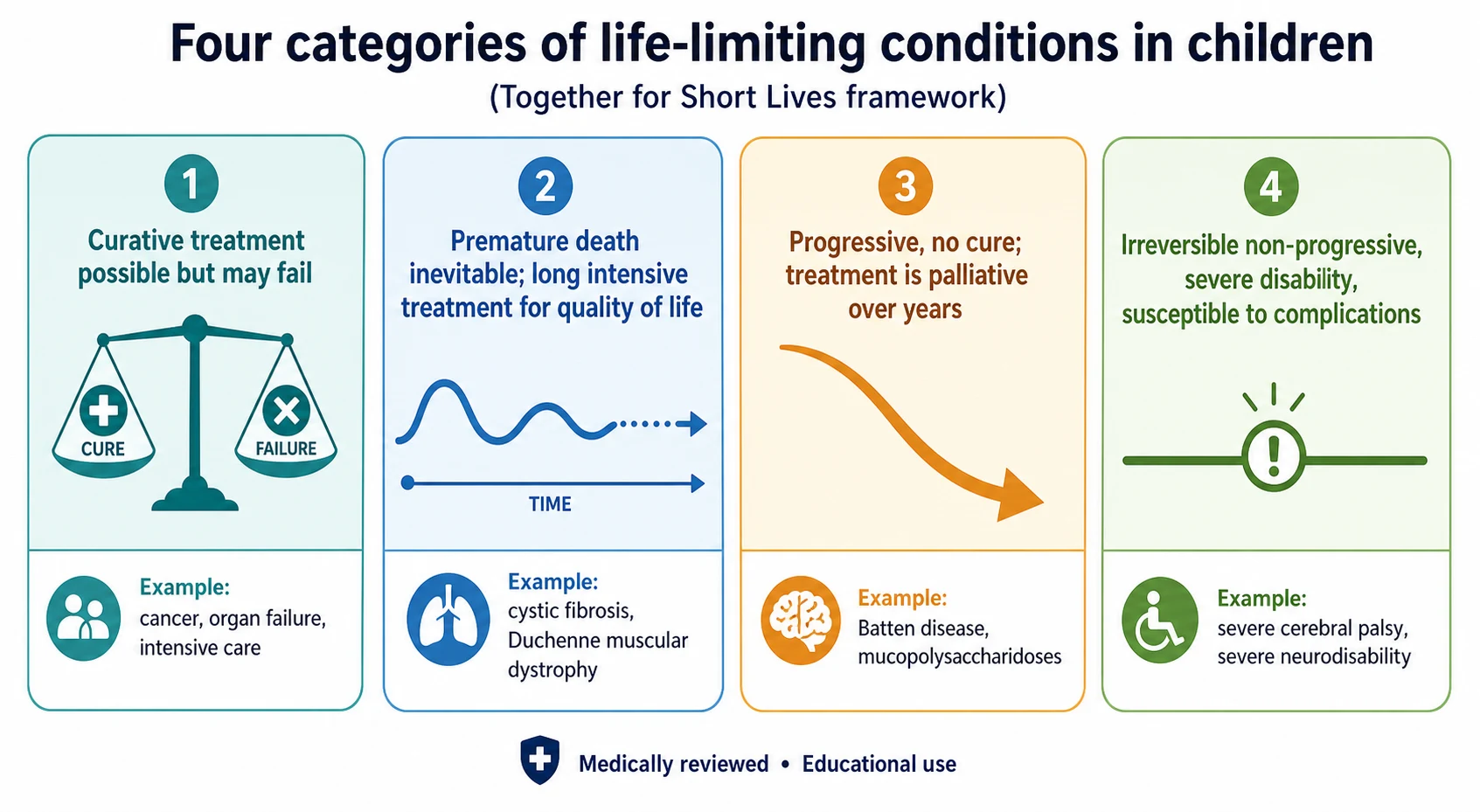
The four Together for Short Lives (ACT) categories
Group 1 — curative treatment may be feasible but can fail
- Condition for which curative or life-prolonging treatment exists but may fail
- Palliative care runs alongside cure-directed therapy, and intensifies if treatment fails
- Worked examples: cancer, irreversible organ failure, the child in intensive care
- Refer at diagnosis so that PPC is already in place if the curative path fails
Group 2 — premature death inevitable; long intensive treatment
- Premature death is inevitable, with long periods of intensive treatment aimed at quality of life
- Palliative care is layered on through years of a known life-shortening course
- Worked examples: cystic fibrosis, Duchenne muscular dystrophy
- Refer at diagnosis; the long horizon is exactly where PPC adds most
Group 3 — progressive, no cure; treatment is palliative
- Progressive condition without curative option, where treatment is exclusively palliative over many years
- Palliative care is the principal medical framework from early in the course
- Worked examples: Batten disease, the mucopolysaccharidoses, severe neurodegenerative disease
- Refer early; symptom control and family support dominate the care
Group 4 — irreversible, non-progressive, severe disability
- Irreversible but non-progressive condition causing severe disability and susceptibility to complications
- Premature death is likely from the complications — infection, respiratory failure, seizure
- Worked examples: severe cerebral palsy, severe neurodisability after brain or cord insult
- Refer for the recurrent suffering the trajectory produces, not a single terminal event
Shaw and colleagues proposed a complementary needs-based spectrum that classifies children by the palliative care need — a stable group needing occasional support, a deteriorating group needing increasing input, and a dying group needing intensive end-of-life care. The two frameworks sit together: the ACT category tells you why the child needs a palliative approach, and the needs-based spectrum tells you how much support they need right now. [10]
The numbers that anchor your viva
Epidemiology & Risk Factors
Paediatric palliative care is not rare — it is unrecognised. The children who need it are the children whose deaths and long hospital stays cluster around complex, chronic, technology-dependent illness. Feudtner and colleagues showed that deaths attributed to complex chronic conditions account for around half of paediatric deaths in the older child age band, and that this share rose over two decades as acute and infectious causes fell. These are exactly the children a general paediatrician looks after. [3] [9]
Simon and colleagues extended this picture to the living child: children with complex chronic conditions account for a disproportionate share of inpatient hospital days and costs, with readmissions, technology dependence and intensive-care use concentrated in a small, identifiable group. The child who is back on your ward for the third time this year with the same neurodisability-related respiratory failure is the child who needs a palliative care referral, not another reactive admission. [9]
The global picture is starker. The Lancet Commission on palliative care (Knaul and colleagues) found that more than 25 million people die each year with serious health-related suffering, and that children are disproportionately affected in low- and middle-income countries — where access to palliative care and even basic pain relief, including morphine, is absent for the majority who need it. The access gap is the single largest equity failure in the field. [6]
The consistent finding, in every health system, is that referral is too late and too narrow. Children are referred in the last days or weeks of life, after the months in which palliative care could have relieved suffering, supported decision-making, and helped a family plan. The epidemiology frames the problem; the remedy is early referral. [1] [2]
Pathophysiology
To understand why palliative care must run in parallel, picture two trajectories on the same timeline. The disease-directed (curative) trajectory rises as treatment intensifies and may fall back if the disease responds — or continue to fall if it does not. The palliative trajectory starts at a low level at diagnosis and rises steadily as the disease progresses, peaking around end of life and continuing briefly into bereavement. The two lines run together. That is the parallel-care model, and it is the mechanism that makes early referral work. [5] [7]
The second mechanism is total suffering in four interacting domains. Unrelieved pain amplifies anxiety and existential distress; a frightened child feels more pain; a family in conflict or financial stress carries the child's suffering harder. Treating the physical symptom without the psychological, social and spiritual context leaves the suffering half-treated, which is why the assessment must span all four. [5] [7]
The third mechanism is the family as the unit of care. The illness and its trajectory act on parents, siblings and grandparents — on a mother's sleep, a sibling's schoolwork, a family's finances and a grandparent's grief. The child's experience of suffering is shaped by the family's coping, culture, language and resources, so a care plan built for the child alone will fail the child. [4] [5]
The fourth mechanism is dynamic symptom burden. Pain, fatigue, dyspnoea, nausea, anxiety, sleep disturbance and secretions cluster in serious paediatric illness, and they change as the disease moves. A static plan written once will drift out of date, so the symptom assessment is repeated and the plan revised as the trajectory shifts. [1] [7]
Clinical Presentation
The child who would benefit from a palliative approach reaches you through a small number of presentations, and each is a referral trigger. [4] [7]
A new diagnosis of a life-limiting or life-threatening condition — a high-risk cancer, a neuromuscular degeneration, a hypoplastic left heart, a prenatally diagnosed lethal anomaly — is the cleanest trigger, and it is the one most often missed. The palliative referral belongs at the diagnosis meeting, not months later. [4]
Recurrent or prolonged hospitalisation, especially a third admission in a year for the same complication of a chronic condition, signals that the reactive model is failing and a palliative layer is needed. Escalating or refractory symptoms — pain that is breaking through, dyspnoea at rest, uncontrolled seizures — are a direct call for symptom expertise. Technology dependence (tracheostomy, long-term ventilation, feeding tubes) brings a long horizon of complex care that palliative services co-manage. [9]
The red-flag presentations that demand prompt palliative involvement are refractory pain or dyspnoea, a child who has just been told their disease is no longer curable, repeated unplanned admissions in a progressive condition, and any family asking the two questions that mean they are ready to talk — "what will happen to my child?" and "how long does she have?". [1] [7]
The atypical and difficult presentations deserve attention. The child with non-progressive severe neurodisability (ACT group 4) is the one whose suffering is easiest to under-recognise, because recurrent infections and pain are attributed to baseline. The adolescent with a life-limiting condition is struggling with autonomy, identity, intimacy and the fear of dying young, and needs a developmentally-led conversation. A family in conflict about the goals of care, or a parent carrying heavy anticipatory grief, is itself a palliative presentation. [5] [7]
Differential Diagnosis
The differential in this topic is best framed as one question: does this child have a life-limiting or life-threatening condition that fits a Together for Short Lives category? If yes, the palliative approach applies, and the task is to decide how much specialist input is needed. [4] [10]
Distinguish the child in group 1 (curable but treatment may fail — cancer, organ failure, intensive care) from the child in group 2 (premature death inevitable with long intensive treatment — cystic fibrosis, Duchenne). Both need a palliative layer, but the timing and the intensity differ: group 1 brings it in as insurance against failure, group 2 carries it through years. [10]
Distinguish the child in group 3 (progressive, no cure, treatment is palliative over years — Batten disease, the mucopolysaccharidoses) from the child in group 4 (irreversible, non-progressive, severe disability susceptible to complications — severe cerebral palsy, severe neurodisability). Group 3 needs palliative care as the principal medical framework; group 4 needs it for the recurrent suffering the trajectory produces. [10]
The other differential is between supportive care delivered by the treating team and specialist paediatric palliative care referral. A general paediatrician can and should deliver basic symptom control, communication and coordination. Refer to the specialist team when the symptoms are refractory, the family need is complex, the trajectory is deteriorating, or end-of-life care is approaching. The two are complementary, not alternatives. [4] [7]
Clinical & Bedside Assessment
Before any referral, run a structured whole-child and family assessment across the four domains, because the assessment turns the presentation into a care plan. [5] [7]
Start with the physical domain. Assess pain, dyspnoea, fatigue, nausea, sleep, secretions, seizures and bowel and bladder function, using developmentally-appropriate and validated tools where they exist — and always elicit the child's own experience. For the pre-verbal or cognitively impaired child, combine observational tools with the family's expert reading, because the family often knows first when something has changed. [7]
Move to the psychological domain — the child's mood, fears, understanding of the illness, and coping, and the family's mental health and prior losses. Then the social and family domain — who is at home, who is the primary carer, what are the siblings' needs, what is the school situation, what are the finances, travel and housing, and what are the language and cultural needs (always use a trained interpreter, never a family member, for high-stakes conversations). Finally the spiritual or existential domain — what gives the child's and family's life meaning, what are their religious or cultural practices around illness and death, and what are their hopes and fears for the future. [4] [5]
Synthesise the assessment into a problem list and shared goals of care. The child (where developmentally able), the family and the team should share the same understanding of where the illness is, what matters most now, and what the plan is. Document it so that it travels with the child — across the ward, the emergency department and the community — as an advance care plan. [4] [11]
[5] [7]Investigations
Paediatric palliative care does not depend on a prognosis threshold, a blood test or a score. The trigger is clinical: the presence of a life-limiting or life-threatening condition, identified by the history, the examination and the Together for Short Lives category. [4] [7]
The named, validated screening tool is the Paediatric Palliative Screening Scale (PaPaS) of Bergstraesser and colleagues. It scores the child on the trajectory of the disease, the burden of symptoms and care, and the expected care needs, to flag the child who would benefit from a palliative care referral. It is a screening aid for the generalist at the bedside, not a gatekeeper — a child who clearly fits an ACT category is referred regardless of the score. [8]
Investigations still have a role when they answer a question that changes comfort: a reversible cause of pain, an infection that is treatable, an electrolyte disturbance driving delirium. The principle is to investigate only when the answer would change what you do for the child's suffering. In the imminently dying child, investigation and monitoring that add burden without benefit are set aside. [7]
The investigation that matters most is the advance care plan itself. It is a living document that records the shared goals, the resuscitation and escalation status, the preferred place of care and death, and the symptom preferences — and it travels with the child so that an out-of-hours crisis does not trigger default care against the family's wishes. [4] [11]
Management — Resuscitation
In an acute deterioration of a child with a serious illness, the first priority is to relieve suffering now. Assess and treat pain, dyspnoea, agitation and secretions with the right agent, dose, route and timing — and do not wait for a diagnosis, a plan or a referral to make the child comfortable. The detailed drug ladders belong to the symptom-control page; the principle here is that comfort is never contingent. [1] [7]
The parallel priority is leadership and communication. Ensure a named senior clinician is leading, that the family knows who to call at any hour, and that an honest, jargon-free conversation about the situation has begun or is scheduled. A family that is kept informed through a crisis is a family that can participate in the decisions that follow. [4] [5]
The third priority is safety. Confirm the resuscitation and escalation status is documented and communicated to the whole team, so that an arrest does not trigger default full resuscitation against the child's best interests. Critically, the resuscitation decision and the palliative referral are separate acts: a child can have full escalation status and still benefit from palliative care, and a child with a limitation order still receives active comfort care. Conflating the two is a common and harmful error. [4] [7]
Management — Definitive & Stepwise
The definitive pathway runs from identification through bereavement, and the general paediatrician owns the first three steps. [4] [7]
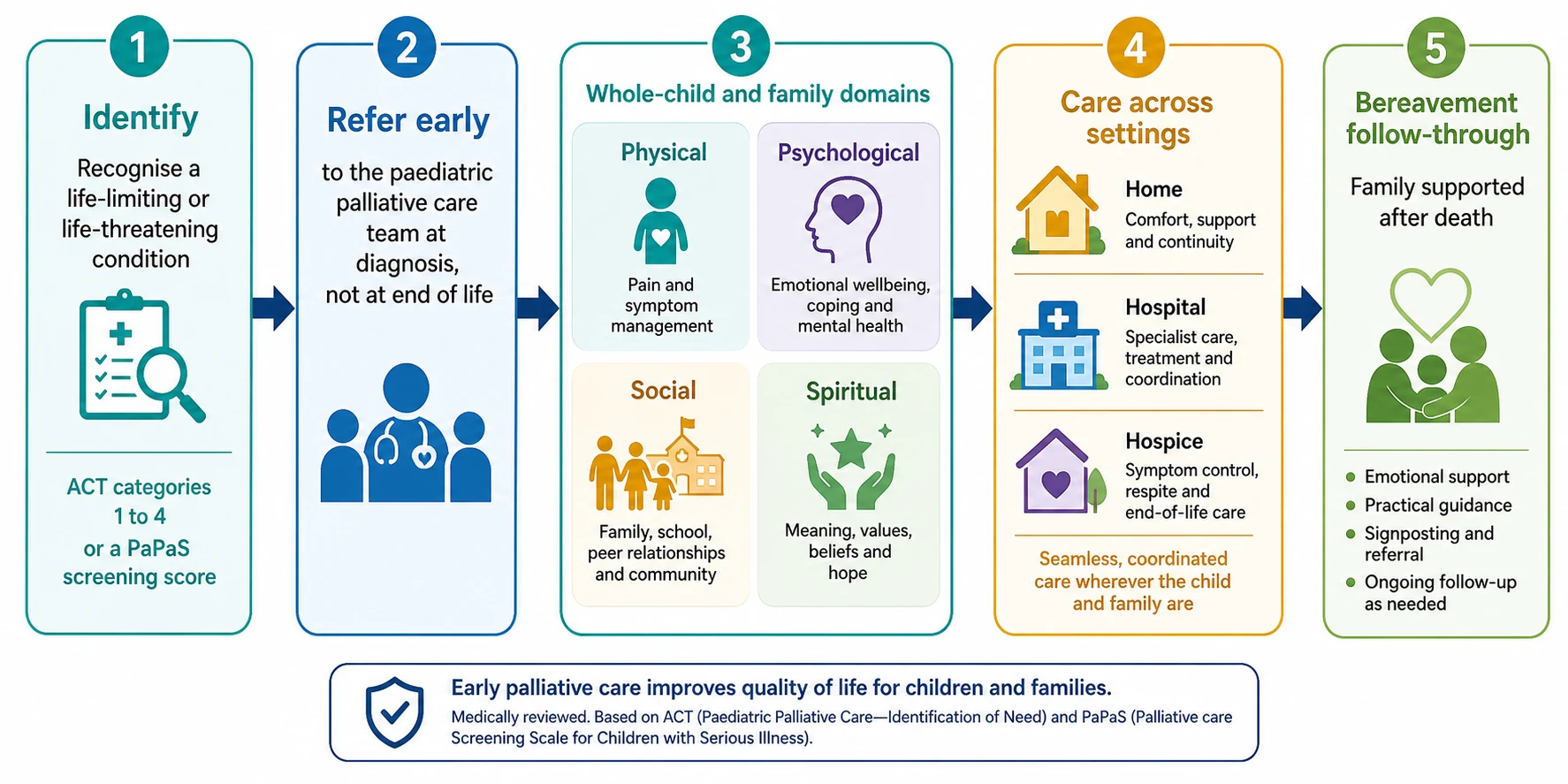
The paediatric palliative care referral and care pathway
Identify — recognise the life-limiting or life-threatening condition (Together for Short Lives category 1 to 4) or a PaPaS screen that flags need
Refer early — to the paediatric palliative care team at diagnosis, not at end of life; the two teams then work in parallel
Assess — complete the whole-child and family assessment across the four domains of suffering
Plan — build a shared advance care plan covering goals, resuscitation and escalation status, preferred place of care, and symptom preferences
Deliver — care across home, hospital, hospice and school, by the multidisciplinary team, with after-hours support
Follow through — bereavement care for the family, with structured follow-up of parents and siblings in the weeks and months after the death
The multidisciplinary team is the delivery engine. It brings together the paediatrician and palliative care physician, nursing (community and inpatient), social work, psychology, chaplaincy or spiritual care, play and child life therapy, and the school and community services. No single clinician can meet the four-domain need; the team is the intervention. [4] [7]
Care is delivered across settings — home, hospital (ward and intensive care), hospice and school — wherever best meets the child's and family's needs. For most families, home is the preferred place for ongoing care, and often for end-of-life care, though the right setting is the one the family chooses with good support. Bluebond-Langner and colleagues found that families' preferred place of death is shaped by support, resources and the child's symptoms, and that a documented, supported preference is more likely to be achieved. [11]
Bereavement care is a core deliverable, not an optional extra. The team that knew the child and the family is best placed to support them after the death, with a follow-up contact, a review of the family's needs, and structured support for parents and siblings in the months that follow. [4] [11]
CARE
Specific Subtypes & Scenarios
The palliative approach flexes around the illness, and four scenarios recur in exams and in practice. [4] [7]
In cancer, palliative care is involved early alongside oncology, managing pain and the treatment-related symptoms (mucositis, nausea, neuropathy) and holding the space for a shift in focus if cure-directed therapy fails. Wolfe's two cohorts frame the evidence: in 2000, children who died of cancer suffered substantially; by 2008, earlier palliative involvement was associated with reduced suffering. The lesson is to involve the team while curative treatment is still active. [1] [2]
In neurodisability and genetic disease, the horizon is long and the child is often non-verbal. The work is recognising suffering that is easy to attribute to baseline, and managing spasticity, seizures, feeding difficulty, respiratory compromise and recurrent infection over years. ACT group 4 children belong here, and their suffering is the most under-recognised in paediatrics. [5] [9]
In the neonate and in intensive care, the presentation is perinatal palliative care when a life-limiting diagnosis is made antenatally, and palliative involvement when limitation of life-sustaining treatment is being considered in the NICU or PICU. The palliative team supports the antenatal counselling, the goals-of-care conversation, the symptom control at the bedside, and the bereavement follow-up — and it works alongside, not instead of, the treating unit. [4] [7]
In the adolescent and young adult, the work is developmentally-led: autonomy, assent and confidentiality, identity and intimacy, the fear of dying young, and — when prognosis extends beyond childhood — a planned transition to adult palliative care services. The young person should be invited into the conversation at a level their development allows, and their voice should carry weight in the goals of care. [5] [7]
Complications & Pitfalls
The central pitfall — and the one examiners test — is equating palliative care with giving up. The fear that a palliative referral means abandoning treatment keeps clinicians and families from engaging, and the result is late referral, under-treated suffering, and a family that feels abandoned in the very way they feared. The remedy is the parallel-care framing: palliative care is additive, not a replacement. [2] [5]
The mirror pitfall is abandoning disease-directed care when palliative care is introduced. A child can continue curative treatment and receive a palliative layer; the two are not exclusive. Withdrawing active treatment is a separate, best-interests decision, not a consequence of the palliative referral. [4]
The third pitfall is under-recognising suffering in the non-verbal, cognitively impaired or severely disabled child. Pain attributed to baseline, distress attributed to the condition, and recurrent infections treated reactively without a palliative plan all leave group 4 children under-served. Observational tools and the family's expert reading are the safeguards. [5] [9]
The fourth pitfall is a poor bereavement pathway. A family that loses contact with the team at the death — no follow-up call, no review of the siblings, no offer of bereavement support — is left to grieve alone. Bereavement care is a core PPC deliverable, with structured follow-up of parents and siblings in the weeks and months after the death. [4] [11]
Prognosis & Disposition
Paediatric palliative care does not require a prognosis, and uncertainty about prognosis is itself a reason to involve the team. Waiting for a confident "weeks to months" estimate is one of the commonest causes of late referral; the parallel-care model is built to run under uncertainty. [5] [7]
Earlier palliative involvement is associated with better symptom control, less aggressive end-of-life care, earlier advance care planning, and greater family satisfaction. Wolfe's 2008 follow-up showed that the shift toward earlier palliative involvement was associated with reduced suffering in children with cancer at the end of life — the clearest evidence that timing matters. [1] [2]
The disposition principle is that care is delivered wherever best meets the child's and family's needs — home, hospice or hospital — with the preferred place of care and death elicited, documented and supported. Home and hospice are often preferred for ongoing and end-of-life care; hospital remains essential for the unstable child and for symptom crises that cannot be managed at home. [7] [11]
And palliative care continues through bereavement. The team that knew the child and the family is best placed to support them after the death, with a follow-up contact soon after, a review of the family's needs, and bereavement support for parents and siblings in the months that follow. [4] [11]
Special Populations
The palliative approach adapts to the population in front of you, and four groups need particular care. [5] [7]
The non-verbal and cognitively impaired child needs observational pain assessment, the family treated as the expert on the child's baseline, and vigilance for the treatable causes of distress (constipation, fracture, infection, urinary retention) that are easy to miss. Under-treatment of pain in this group is a recurring failure. [5]
Indigenous, migrant, refugee and culturally and linguistically diverse families need interpreter use (never a family member for high-stakes conversations), respect for cultural and spiritual practices around illness and death, and family-led decision-making that fits the family's structure. The model of care should flex to the family, not the reverse. [4]
Rural and remote families face distance, access and retrieval as central constraints. Telehealth, local community partnerships, shared care with the regional hospital, and clear after-hours pathways are the supports that make home and community care feasible far from the tertiary centre. [6]
The adolescent needs developmentally-appropriate communication, a voice in decisions proportionate to their capacity (with assent or consent handled correctly), attention to identity, intimacy and peer relationships, and a planned transition to adult palliative care when prognosis extends beyond childhood. [5]
Evidence, Guidelines & Regional Differences
The evidence base rests on three pillars. Wolfe's 2000 New England Journal study found that children who died of cancer suffered substantially in their last month of life; the 2008 follow-up showed that earlier palliative involvement was associated with reduced suffering. These two papers are the standard citations for why early palliative care matters. [1] [2]
The American Academy of Pediatrics 2013 policy on Paediatric Palliative Care and Hospice Care Commitments, Guidelines, and Recommendations sets out the US framework — the principles, the team, the settings, and the call for concurrent care so that a child can receive disease-directed and palliative care together. The Lancet Commission (Knaul 2018) frames the global access failure and the imperative of universal access to palliative care and pain relief. [4] [6]
Wolfe 2000 and 2008 — the suffering and the shift
Two-cohort observational study of children who died of cancer at a single centre, 1997–2004, with parent-reported suffering.
Key finding
In the 2000 cohort, about nine in ten children suffered a lot or a great deal from at least one symptom in their last month of life. In the 2008 follow-up, earlier palliative care involvement was associated with reduced suffering and less end-of-life medical intensity.
The controversies are real. There is no single agreed referral trigger, which is why the PaPaS scale and the ACT categories fill the gap. Service availability varies widely, both between and within countries, so the referral a generalist can make depends on local resource. There is an ethical tension around the timing of end-of-life conversations, held against the parallel-care principle. And the global gap in access to children's pain relief persists despite the evidence. [6] [8]
Exam Pearls
[5] [7] [8]The most common and most consequential error in this topic is referring late. The remedy is a reflex: when you make a diagnosis of a life-limiting or life-threatening condition, ask whether a palliative referral belongs in the same week. [1] [4]
Remember the four domains of suffering (physical, psychological, social, spiritual) and assess all four, every time, with the family as the unit of care. Remember that comfort is never contingent on a plan. And remember that the child who looks well can still be suffering — and that the non-verbal child is the one most often left in pain. [5] [7]
Self-test: a general paediatrician refers a 6-year-old with relapsed leukaemia to palliative care on the day of relapse. The oncologist asks why. What is your one-line defence?
Because palliative care runs in parallel from diagnosis of a life-limiting illness, not only at end of life. The child fits Together for Short Lives group 1; early involvement relieves suffering now, builds the advance care plan, and supports the family through whatever the disease trajectory brings — without abandoning curative treatment. The evidence is Wolfe 2000 and 2008: earlier palliative involvement reduces suffering. [1] [2]
References
- [1]Wolfe J, Grier HE, Klar N, Levin SB, Ellenbogen JM, Salem-Schatz J, Emanuel EJ, Weeks JC Symptoms and suffering at the end of life in children with cancer. N Engl J Med, 2000.PMID 10655532
- [2]Wolfe J, Hammel JF, Edwards KE, Duncan J, Comeau M, Breyer J, Aldridge SA, Grier HE, Berde C, Dussel V, Weeks JC Easing of suffering in children with cancer at the end of life: is care changing? J Clin Oncol, 2008.PMID 18375901
- [3]Feudtner C, Hays RM, Haynes G, Geyer JR, Neff JM, Koepsell TD Deaths attributed to pediatric complex chronic conditions: national trends and implications for supportive care services. Pediatrics, 2001.PMID 11389297
- [4]Section on Hospice and Palliative Medicine and Committee on Hospital Care Pediatric Palliative Care and Hospice Care Commitments, Guidelines, and Recommendations. Pediatrics, 2013.PMID 28448256
- [5]Himelstein BP, Hilden JM, Boldt AM, Weissman D Palliative care for infants, children, adolescents, and their families. J Palliat Med, 2006.PMID 16430356
- [6]Knaul FM, Farmer PE, Krakauer EL, De Lima L, Bhadelia A, Jiang Kwete X, Arreola-Ornelas H, Gómez-Dantés O, Rodriguez NM, Alleyne GAO, et al Alleviating the access abyss in palliative care and pain relief-an imperative of universal health coverage: the Lancet Commission report. Lancet, 2018.PMID 29032993
- [7]Klick JC, Hauer J Pediatric palliative care. Curr Probl Pediatr Adolesc Health Care, 2010.PMID 20638035
- [8]Bergstraesser E, Hahn CP, Kaiser G, Niggli F, Landolt MA, Lütolf K, Perren U, Rameil-Stalder N, Steiner R, Von Schuetz M, et al The Paediatric Palliative Screening Scale: Further validity testing. Palliat Med, 2014.PMID 24280277
- [9]Simon TD, Berry J, Feudtner C, Stone BL, Sheng X, Bratton SL, Dean JM, Srivastava R Children with complex chronic conditions in inpatient hospital settings in the United States. Pediatrics, 2010.PMID 20855394
- [10]Shaw KL, Brook L, Cuddeford L, Darnill M, Doalfe J, Ersser S, Goodhand S, Halls S, Hicken S, Kelly P, et al The Spectrum of Children's Palliative Care Needs: a classification framework for children with life-limiting or life-threatening conditions. BMJ Support Palliat Care, 2015.PMID 24644200
- [11]Bluebond-Langner M, Beecham E, Candy B, Langner R, Jones L Preferred place of death for children and young people with life-limiting and life-threatening conditions: a systematic review of the literature and recommendations for future inquiry and policy. Palliat Med, 2013.PMID 23612958