Paeds · preventive-and-community-paediatrics
Adolescent preventive health care
Also known as Adolescent well visit · Adolescent health supervision · HEADSS assessment · HEEADSSS · Youth preventive care · Adolescent psychosocial screening
A fellowship approach to adolescent preventive care: time alone, conditional confidentiality, HEADSS/HEEADSSS psychosocial assessment, integrated screening, anticipatory guidance, immunisation review, red-flag safety action, follow-up and transition across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old arrives “for a check-up.” The parent answers every question. You never ask about mood, vaping or partners. Growth looks fine. You stamp “well.” Two months later the same adolescent is in ED after a deliberate overdose. The missed work was not a rare syndrome. It was a preventive visit without youth-centred process. [16] [18]
Adolescent preventive health care is longitudinal, developmentally staged care that protects current safety and future health. It includes psychosocial assessment, confidential counselling, physical screening, immunisation, anticipatory guidance and planned transition toward adult care. Frameworks such as GAPS and Bright Futures operationalise that idea; local tools (for example Greig Health Record updates in Canada) adapt content by jurisdiction. The exam skill is the process, not brand loyalty to one checklist. [4] [16]
HEADSS is a structured psychosocial interview framework. Cohen and colleagues described it for high-risk youth: Home, Education, Activities, Drugs, Sexuality, Suicide/depression (with safety woven through). Many services use HEEADSSS, which expands Eating and makes Safety/Spirituality/strengths more explicit. Treat the letters as a memory scaffold for skilled conversation, not a robotic script. [1] [19]
Core sequence of an adolescent preventive visit
Shared start
Greet both parties. Set a joint agenda. Explain the plan for private time.
Conditional confidentiality
Promise privacy with clear limits: serious harm, abuse and other legal duties.
HEADSS/HEEADSSS
Work domains with open then focused questions. Follow positive leads.
Exam and preventive tasks
Growth, BP, puberty-aware exam, vision/hearing/oral prompts, immunisations.
Screens and plan
Add validated tools if indicated. Co-create a plan the young person can use.
Classification
Start with the person in front of you, then classify stage, visit type and risk intensity. [16]
Developmental stage
| Stage | Rough age band | What changes in the visit |
|---|---|---|
| Early adolescence | ~10–13 years | Concrete language; parent still central; body changes and school stress rise |
| Middle adolescence | ~14–16 years | Peer influence peaks; risk behaviours more common; confidentiality becomes essential |
| Late adolescence / transition | ~17–21+ years | Autonomy and adult-care readiness; work, driving, relationships, transfer planning |
Age bands are guides, not law. Chronologic age can lag or lead developmental capacity. [16] [7]
Visit and assessment types
- Dedicated preventive visit: full structure, immunisation and anticipatory guidance. [4] [5]
- Opportunistic preventive add-on: acute visit where you still create brief private time and sample high-yield HEADSS domains. [19]
- Universal psychosocial inquiry: HEADSS-style interview for all. [1]
- Selective validated screening: PHQ-based depression tools, anxiety screens, CRAFFT and similar when indicated by age, policy or clinical risk. [9] [2]
- Diagnostic assessment: specialist-level evaluation after a positive screen or high-risk history—not the same as a brief screen. [11]
Confidentiality classification
Conditional confidentiality means: what you say stays between us, unless I become worried you are not safe, someone else is being hurt, or the law requires me to act. That is the clinically honest frame. Absolute secrecy you cannot keep is a trust injury waiting to happen. [13] [14] [3]
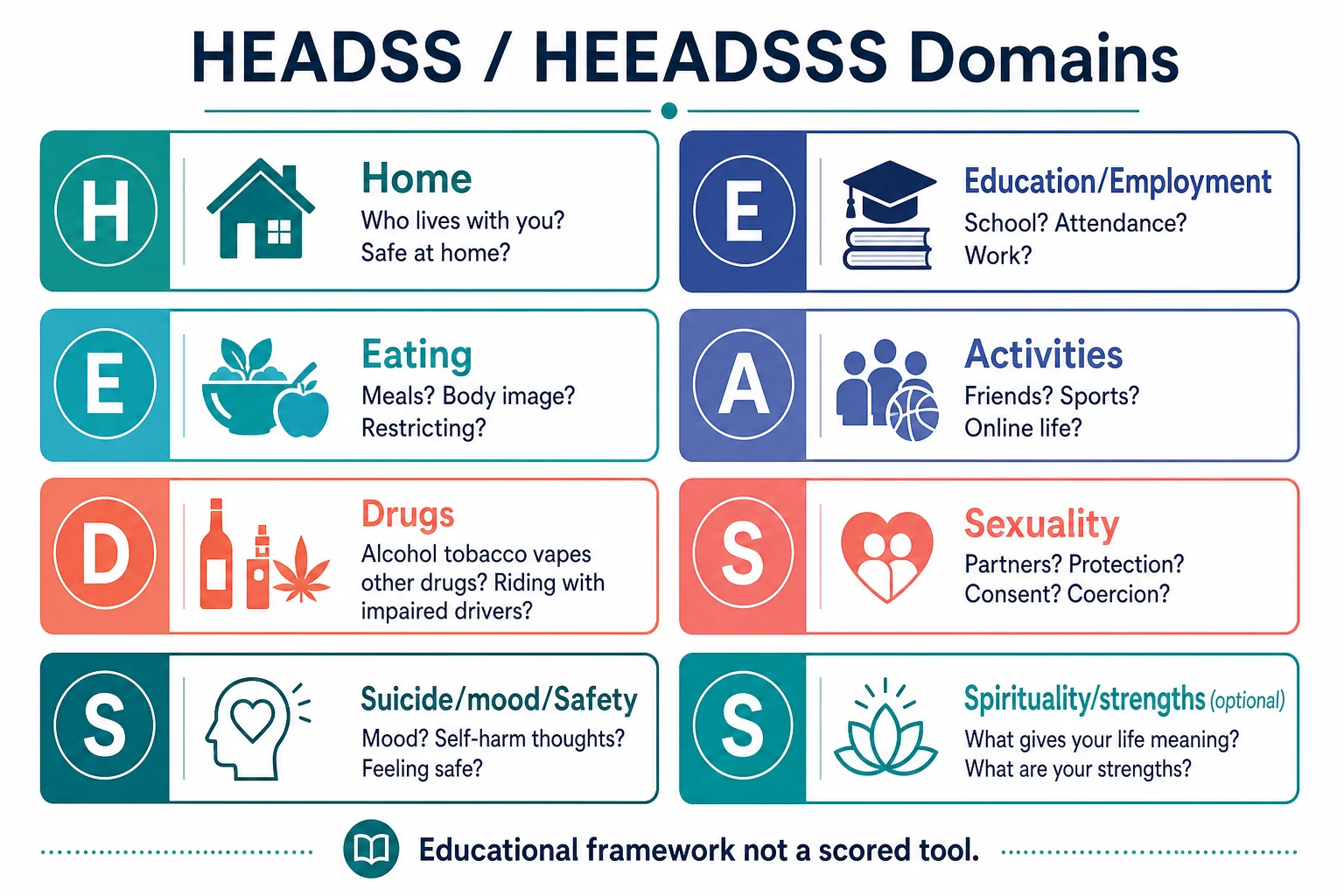
Read the figure like this: if you only ask about school and sport, you have not done HEADSS. Empty domains are unfinished clinical work. [1]
HEADSS core
Classic scaffold
- Home
- Education
- Activities
- Drugs
- Sexuality
- Suicide/depression/safety
HEEADSSS expansion
Common service form
- Adds Eating explicitly
- Safety more visible
- Spirituality/strengths in some versions
- Still an interview framework
Validated screens
Adjuncts
- Mood/anxiety instruments
- CRAFFT for substance risk
- Do not replace conversation
- Positive screen needs same-visit safety thinking
Epidemiology & Risk Factors
Adolescent health burden is dominated by injury, mental health, substance use, sexual health outcomes and rising cardiometabolic risk, not classic paediatric infectious disease alone. Preventive primary care is one place those risks can be found early. [16] [18] [21]
Preventive-visit receipt is incomplete in many systems. Policy changes that expand coverage can increase adolescent preventive care delivery, but access does not guarantee confidential process quality. [5] Attendance often falls from mid-adolescence into young adulthood; some groups disengage earlier. Engagement itself is a preventive outcome. [24]
Risk amplifiers: Poverty, racism, housing instability, rural isolation and digital exclusion; LGBTQ+ minority stress, bullying and family rejection; out-of-home care and youth justice with fragmented records; chronic disease or disability with diagnostic overshadowing; parent discomfort with confidentiality, or clinic systems that cannot protect private notes and bills; missed private time with the clinician. [16] [18] [13] [7] [23] [15] [6] [3]
Alcohol use disorder often has paediatric-onset pathways; early detection and brief intervention matter. [21] Depression and suicide-risk screening recommendations exist because untreated mood disorders are common and consequential in this age band. [9] [11]
Pathophysiology
You do not need a neuroscience lecture to counsel well. You do need a usable model. [16]
Brain development in adolescence pairs high reward sensitivity with still-maturing cognitive control. That mix supports learning and identity—and also experimentation under peer and affective pressure. Counselling that only lectures “just say no” ignores the biology of context. [16] [21]
Puberty changes body composition, sleep timing, sexual capacity and social status. Body-image threat rises. Cardiometabolic trajectories begin to diverge. Preventive care must notice blood pressure, BMI trend, menstrual or genital health and activity, not only sore throats. [16] [22]
Sleep debt from delayed circadian phase plus late-night device use worsens mood, attention, metabolic risk and injury risk. Ask about sleep as a vital preventive sign. [16]
Confidentiality failure is a mechanism of harm. If the young person expects parents to hear everything, sexual activity, substance use and suicidality stay hidden. Trust enables data. Data enables prevention. [3] [13] [14]
Trauma and adversity sensitise stress systems and can present as risk behaviour, somatic symptoms or school collapse. Trauma-informed pacing is part of preventive skill. [18]
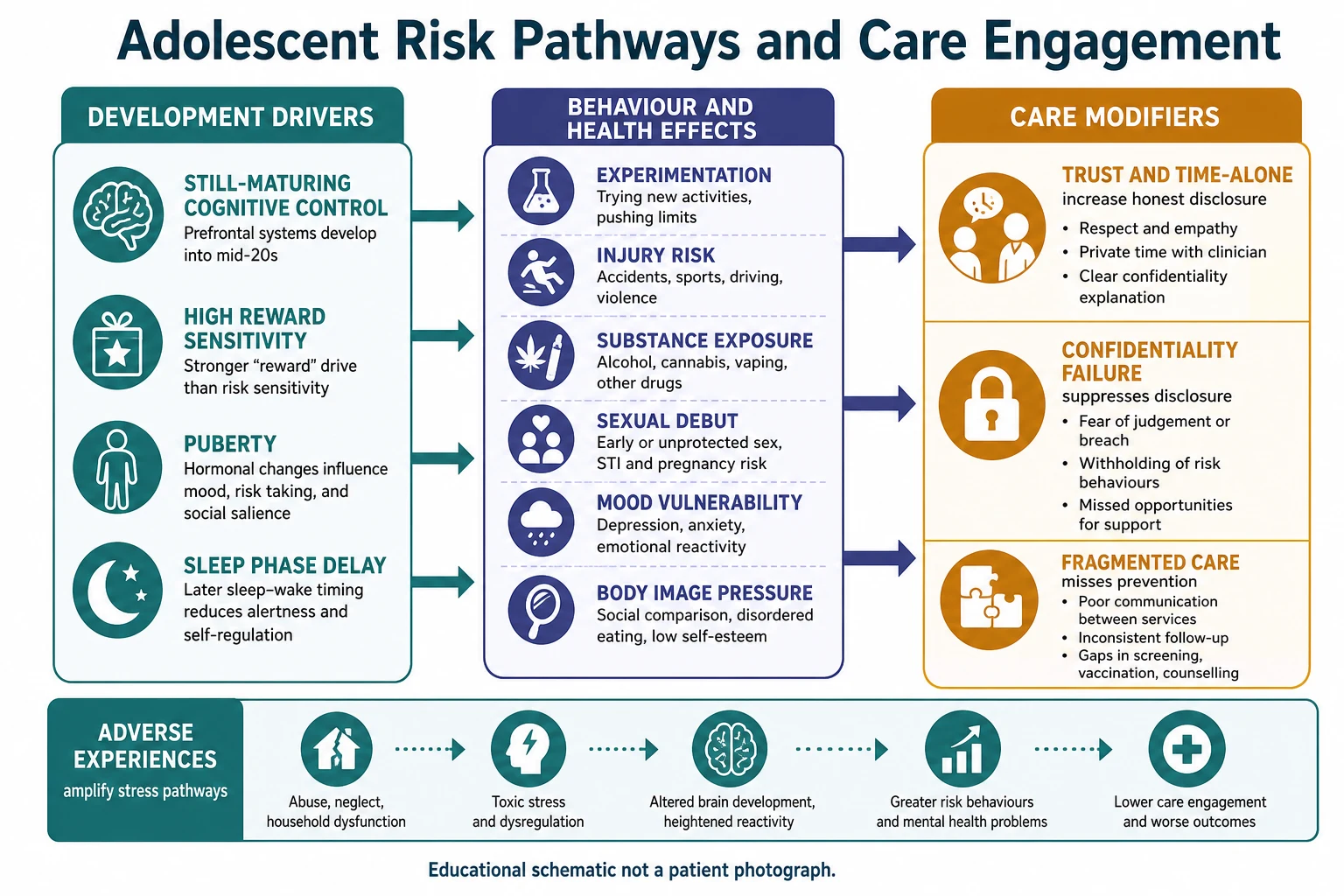
Read the figure like this: a “normal exam” does not cancel high psychosocial risk. The history is the pathophysiology of prevention. [1] [16]
Clinical Presentation
A good preventive visit looks calm. The important presentations are often quiet. [16]
Organised preventive visit: joint agenda, private time secured, HEADSS completed, growth and BP recorded, immunisations reviewed, plan shared in plain language. [4] [17]
High-risk patterns that hide inside “well” visits: parent answers every question; recurrent somatic symptoms with school decline; sleep reversal and withdrawal labelled as “attitude”; weight-loss pride or rigid food rules; “social” vaping and impaired-driving exposure; confidential STI requests; older teens with chronic disease and no adult clinic named. [6] [18] [9] [16] [2] [21] [13] [7] [24]
Hospital and ED settings often miss HEADSS even when risk is high. That missed opportunity is itself a presentation of system failure. [19]
Differential Diagnosis
In prevention, the differential is less “which rash” and more “which driver of risk or distress.” [18]
| What it looks like | Safer framing questions | Do not miss |
|---|---|---|
| Moodiness | Duration, function, anhedonia, sleep, suicide thoughts | Major depression, bipolar risk, abuse |
| School refusal | Anxiety, bullying, learning difficulty, depression, family conflict | Safeguarding, untreated anxiety disorder |
| Weight concern | Restriction, binge-purge, body image, sports pressure | Medical instability, eating disorder |
| Substance “experimenting” | Frequency, blackouts, CRAFFT items, driving risk | Hazardous use, use disorder, trauma self-medication |
| Fatigue | Sleep, mood, anaemia risk, mono, chronic disease | Depression, sleep debt, organic disease |
| Sexual activity request | Consent, coercion, contraception, STI, pregnancy intention | Assault, trafficking, untreated STI |
| Conflict with parents | Autonomy struggle versus coercive control or violence | Maltreatment, intimate partner violence |
Separate normative exploration from impairment and danger. Function at home, school and with peers is your discriminator. [18]
Clinical & Bedside Assessment
1. Open and set the frame
Introduce yourself to the young person first, then the parent. Ask both what they hope to cover. Explain that you will spend time with everyone, then private time with the young person, then bring the plan together. [6] [16]
2. Confidentiality script you can say aloud
“What we talk about privately stays private, unless I become worried that you are not safe, that someone else is being hurt, or the law says I must act. If that happens, I will tell you what I need to do and we will plan it together as much as possible.” Then check understanding. [13] [14] [3]
3. Create time alone
Ask the parent to step out. If resistance appears, normalise: this is standard adolescent care, like teaching self-management. Parent perspectives research shows many will accept private time when the purpose is explained. [6] [23]
4. Work HEADSS/HEEADSSS
Use open questions, then focus. Example anchors: Home — Who lives with you? How do people get on? Do you feel safe there? Education/Employment — School or work? Attendance? Supports? Bullying? Eating — Meals? Body image? Restricting, bingeing, purging, diet pills? Activities — Friends? Sport? Online life? Who knows the real you? Drugs — Alcohol, vapes, cannabis, other drugs? Riding with someone impaired? Sexuality — Partners? Practices? Protection? Consent? Pressure? Suicide/mood/Safety — Mood? Self-harm thoughts or plans? Feeling unsafe anywhere? Strengths — What keeps you going? Who helps? [1]
5. Physical preventive exam elements
Measure height, weight, BMI trajectory and blood pressure with age-appropriate norms. Note puberty stage as relevant, skin for injury or self-harm marks, and oral health prompts. Chaperone sensitive exams. Match genital examination to indication, not habit. [16]
6. Sexual history without shame
Ask permission. Use inclusive language. Cover partners, practices, protection, pregnancy intention, pleasure is optional—coercion is not optional to ask. [13]
7. When mood is low, assess suicide risk now
Ideation, plan, intent, prior attempts, access to means, protective factors, ability to keep safe until follow-up. A positive depression screen without suicide assessment is incomplete. [9] [11]
8. Document with care
Record enough for safety and continuity. Protect sensitive details according to local medical-record and portal rules. Billing and after-visit summaries can leak content if systems are naive. [15] [12] [14]
Investigations
Most well adolescents need few routine labs. Investigation is selective and history-led. [16]
Often useful adjuncts: validated depression instruments (for example PHQ-A/PHQ-9 modified in many services) where recommended; anxiety screening tools aligned with USPSTF-style recommendations and local pathways; CRAFFT for substance-use risk in clinic populations; pregnancy testing when clinically indicated; STI testing matched to sites and practices disclosed; targeted cardiometabolic labs when risk factors and local guidance support them. [9] [11] [10] [2] [13] [16]
Electronic psychosocial tools (digital HEEADSSS-style devices, YouthCHAT and similar) can improve completion and documentation in some settings. They support, not replace, clinical judgement and safety action. [20]
Low-value patterns: automatic full blood panels every year for asymptomatic low-risk youth; repeating STI panels without indication; using a screen score as a diagnosis. [16] [11]
Management — Resuscitation
Prevention visits can become emergency care in one sentence of disclosure. [18]
- Stabilise physiology if needed: ABCDE, glucose, intoxication, severe restriction complications.
- Secure immediate safety for suicidality: do not leave high-risk youth alone; remove means if present in clinic; escalate to ED/crisis teams per local pathway. [9]
- Break confidentiality ethically when thresholds are crossed: tell the young person what you must share and why; involve parent/carer or authorities as required. [13] [14]
- Safeguarding pathway for abuse, assault or coercive control—parallel to medical care. [13]
- Do not negotiate away urgent transfer because the visit was booked as “well adolescent.”
Document decisions, who was informed, and the safety plan. [14]
Management — Definitive & Stepwise
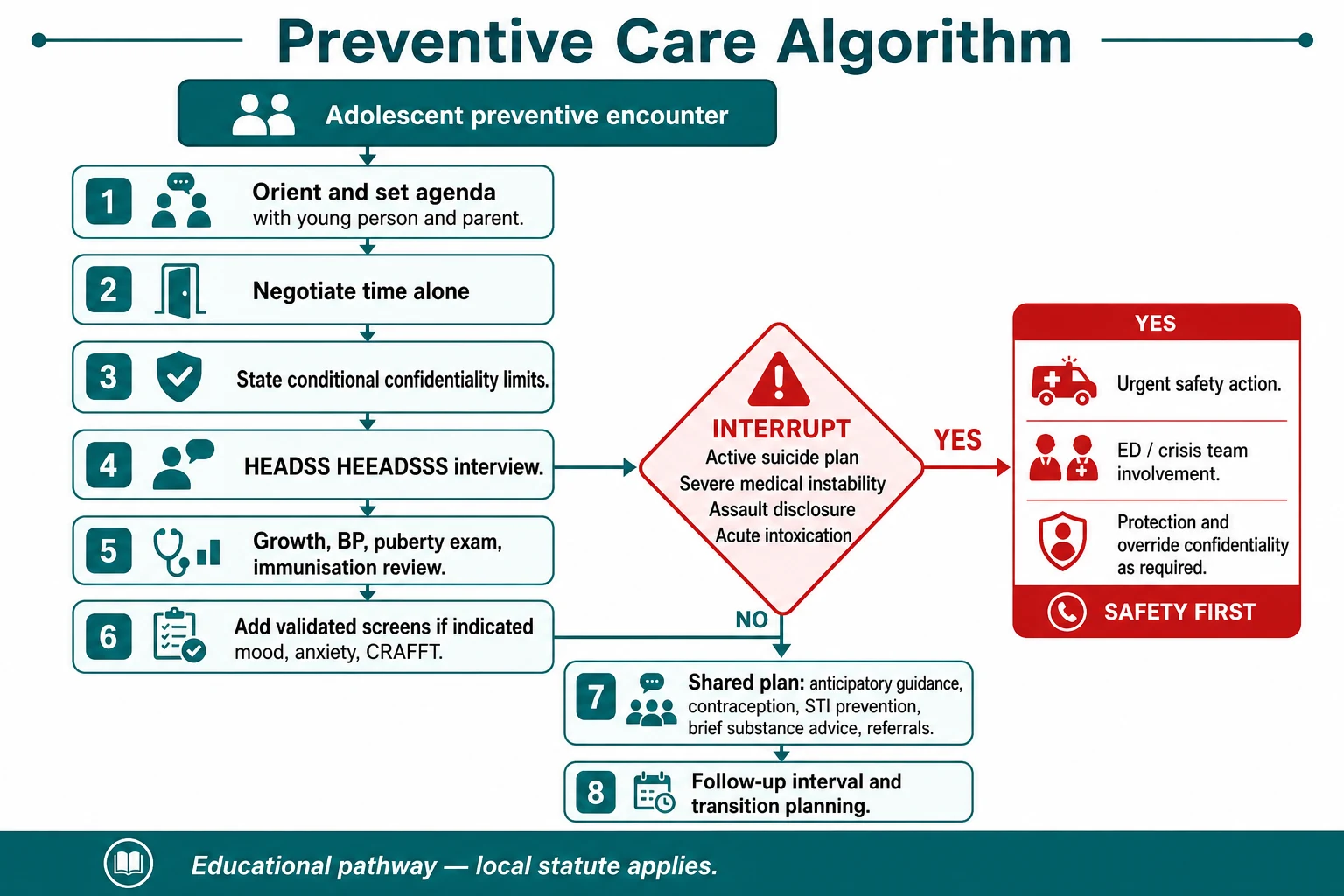
Read the figure like this: the red diamond is not optional decoration. Positive suicide risk or assault disclosure exits the routine path. [9]
Stepwise routine pathway
- Orient and agenda-set with both parties. [16]
- Negotiate time alone and state conditional confidentiality. [3] [6]
- Complete HEADSS/HEEADSSS and follow positives. [1]
- Exam + immunisation review + catch-up planning. Do not leave vaccines for “next time” without a reason. [16]
- Add validated screens when age, symptoms or policy indicate. [9] [10] [2]
- Brief interventions: motivational, non-judgemental advice for substance use; computer-facilitated screening plus brief counselling has trial support as a care model in paediatric primary care. [8] [21]
- Sexual and reproductive health: condoms, contraception options, HPV discussion, STI prevention, consent education. Use local prescribing protocols for product-specific detail. [13]
- Lifestyle guidance with numbers where sourced: support physical activity and limit sedentary time in line with WHO guidance for 5–17-year-olds; personalise to disability and context. [22]
- Weight conversations without stigma: focus on health behaviours; screen for disordered eating rather than praise rapid loss. [16]
- Media and online life: ask what platforms they use; counsel on sleep, bullying, exploitation and privacy. Primary-care social-media counselling interventions are an emerging evidence area. [17]
- Shared plan: what the young person will do, what you will do, when to return, how to get help after hours.
- Transition tasks from middle adolescence: name conditions/medicines, build a portable summary, identify future adult care. Transition is a process inside the medical home, not a birthday letter. [7]
Follow-up intensity
- Low-risk, complete visit: routine interval per local schedule.
- New mild-moderate mental-health or substance concerns: early review (days to a few weeks), not six months by default. [18]
- High risk: same-day or next-day pathway as above. [9]
Specific Subtypes & Scenarios
Early adolescent with parent fused to the chair. Normalise private time early. Use shorter questions. Offer the parent a parallel agenda (school, vaccines, home safety). [6]
ED or ward opportunistic HEADSS. Risk is often higher here. Even a focused safety, mood, substance and home screen can change disposition. Missed HEADSS in hospitalised adolescents is documented. [19]
School-based health. Access improves; dual relationships and parent notification rules need local clarity. Link back to the medical home. [16]
LGBTQ+ and gender-diverse youth. Affirm identity, assess minority stress, tailor sexual health to anatomy and practices, watch for family rejection and bullying. [13] [18]
Disability and neurodiversity. Easy-read materials, longer slots, capacity assessment, sensory adjustments. Carers help—but private time may still be possible with support. Avoid overshadowing mental health. [7]
Out-of-home care / youth justice. Assume incomplete immunisations and trauma exposure. Clarify legal consent. Reconstruct history actively. [16]
Chronic disease clinics. Disease metrics are not a full preventive visit. Still do HEADSS, sexual health and transition. [7]
Rural and telehealth. Dual relationships threaten confidentiality. Create private audio space deliberately; if a parent is in the room off-camera, ask. [13]
Migrant and refugee youth. Interpreter is mandatory when needed; family interpreters are not equivalent for confidential content. Trauma-informed pacing and catch-up prevention matter. [16]
Complications & Pitfalls
- Skipping time alone “because they seem fine.” [3] [6]
- Promising absolute secrecy you will break. [13]
- Checklist completion without rapport or follow-through. [4]
- Parent present for sexual and substance history. [13]
- Portal, insurance or billing letters disclosing contraception or mental-health visits. [15] [12]
- Positive mood screen filed without suicide assessment. [9]
- CRAFFT positive treated as moral failure instead of brief intervention and follow-up. [2] [8]
- Weight lectures that trigger or miss eating disorders. [16]
- Ignoring immunisation opportunities. [16]
- Transition deferred until the week before the 18th birthday. [7] [24]
Prognosis & Disposition
Prognosis in this topic means trajectory of risk and engagement, not a tumour stage. [16]
Routine disposition: complete low-risk visit, clear safety, vaccines planned, adolescent can re-access care. Early review disposition: new mood or substance concerns, unstable housing, recent relationship violence without current emergency, incomplete assessment needing return with trust built. Urgent disposition: active suicide risk, assault, medical instability, severe restriction, acute intoxication with danger—ED/crisis/safeguarding as indicated. [16] [18] [9] [13]
Safety-net explicitly: who to call tonight, when to come back sooner, how confidentiality will work with parents after an override. Close loops after psychology, sexual-health or social-work referral. [14] [7]
Engagement from mid-adolescence into young adulthood is fragile; disposition should name the next visit and the adult-care direction. [24] [7]
Special Populations
Indigenous adolescents. Cultural safety, community connection, racism as a health exposure, and local service pathways matter as much as the HEADSS letters. [16]
Gender and sexual diversity. Confidentiality, chosen name/pronouns, tailored sexual health, and vigilance for bullying and family rejection. [13]
Socioeconomic disadvantage. Ask about food, transport and device access before blaming “non-adherence.” [16]
Athletes. Screen relative energy deficiency risk, performance pressure and injury; do not equate thinness with health. [16]
Complex chronic conditions. Integrate specialty goals with whole-person prevention and transition. [7]
Evidence, Guidelines & Regional Differences
HEADSS remains the foundational published psychosocial instrument for structured youth risk interview in the classic literature. Services expand letters (HEEADSSS) without abandoning the core idea. [1]
GAPS showed that structured preventive guidelines can be implemented in practice and can surface mental-health needs; process fidelity still varies. [4]
Confidentiality science and policy: Ford’s work on confidentiality assurances; Miller on time alone; AAP 2024 policy and technical report; open-notes/Cures Act tensions for adolescent portals. [3] [6] [13] [14] [12] [15] Parent views on confidentiality in preventive services continue to shape feasibility. [23]
Screening recommendations (US reference point): USPSTF 2022 statements support screening for depression and suicide risk and for anxiety in children and adolescents within specified age bands and with adequate systems for follow-up—read the grade and ages from the source when quoting precisely. Evidence reviews underpin those statements. [9] [10] [11] NICE and other national pathways guide UK management after identification. Local ANZ youth-health frameworks emphasise youth-friendly confidential care. [16]
Substance use: CRAFFT validation in clinic samples; paediatric-onset framing of alcohol use disorder; pilot RCT support for computer-facilitated screening and brief counselling models. [2] [21] [8]
Activity: WHO 2020 evidence summary informs physical activity and sedentary behaviour counselling for 5–17 years. [22]
Transition: White et al. medical-home transition policy is a core late-adolescent preventive standard. [7]
Regional differences to name, not invent: consent ages, minor treatment statutes, mandatory reporting triggers, portal defaults, school-based clinic rules and immunisation schedules differ across ANZ, UK, US and Canada. State the principle and check local law. Canada’s Greig Health Record updates illustrate national preventive-tool refresh cycles. [13] [16]
ANZ: youth-friendly care, HEADSS/HEEADSSS culture in many hospitals, RCH-linked adolescent resources, local consent/reporting statutes.
UK: NICE pathways for depression identification/management; Gillick/Fraser capacity concepts in sexual health counselling contexts—apply with current local legal teaching.
US: Bright Futures periodicity, AAP confidentiality policy, USPSTF screening statements, open-notes implementation challenges.
Canada: Greig Health Record and CPS-aligned preventive tools; provincial consent variation.
Exam Pearls
- Open every viva with time alone + conditional confidentiality limits. [13] [3]
- Recite HEADSS letters with one question each; state your local HEEADSSS expansion. [1]
- CRAFFT screens; it does not diagnose. Positive → brief advice + further assessment. [2]
- Positive mood screen → same-visit suicide assessment. [9]
- Portal/billing leaks are modern exam traps. [15] [12]
- Opportunistic HEADSS in ED/ward is fair game. [19]
- Transition is preventive care from mid-teens, not a birthday event. [7]
- Parent alliance and adolescent autonomy are both goals—frame both. [23] [6]
- “Normal exam” never cancels unfinished psychosocial domains. [1] [16]
- Do not invent universal legal ages; name the principle and local statute. [13]
PREVENT visit anchors
References
- [1]Cohen E HEADSS, a psychosocial risk assessment instrument: implications for designing effective intervention programs for runaway youth. Journal of adolescent health : official publication of the Society for Adolescent Medicine, 1991.PMID 1772892
- [2]Knight JR Validity of the CRAFFT substance abuse screening test among adolescent clinic patients. Archives of pediatrics & adolescent medicine, 2002.PMID 12038895
- [3]Ford CA Delivery of confidentiality assurances to adolescents by primary care physicians. Archives of pediatrics & adolescent medicine, 1997.PMID 9158445
- [4]Gadomski A Guidelines for Adolescent Preventive Services: the GAPS in practice. Archives of pediatrics & adolescent medicine, 2003.PMID 12742877
- [5]Adams SH Association Between Adolescent Preventive Care and the Role of the Affordable Care Act. JAMA pediatrics, 2018.PMID 29114725
- [6]Miller VA Adolescents Spending Time Alone With Pediatricians During Routine Visits: Perspectives of Parents in a Primary Care Clinic. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2018.PMID 29887486
- [7]White PH Supporting the Health Care Transition From Adolescence to Adulthood in the Medical Home. Pediatrics, 2018.PMID 30348754
- [8]Knight JR Effect of Computer-Based Substance Use Screening and Brief Behavioral Counseling vs Usual Care for Youths in Pediatric Primary Care: A Pilot Randomized Clinical Trial. JAMA network open, 2019.PMID 31225897
- [9]US Preventive Services Task Force Screening for Depression and Suicide Risk in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA, 2022.PMID 36219440
- [10]US Preventive Services Task Force Screening for Anxiety in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA, 2022.PMID 36219403
- [11]Viswanathan M Screening for Depression and Suicide Risk in Children and Adolescents: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA, 2022.PMID 36219399
- [12]English A Adolescent Consent and Confidentiality: Complexities in Context of the 21st Century Cures Act. Pediatrics, 2022.PMID 35531643
- [13]Chung RJ Confidentiality in the Care of Adolescents: Policy Statement. Pediatrics, 2024.PMID 38646690
- [14]Chung RJ Confidentiality in the Care of Adolescents: Technical Report. Pediatrics, 2024.PMID 38646698
- [15]Pasternak RH 21st Century Cures Act ONC Rule: Implications for Adolescent Care and Confidentiality Protections. Pediatrics, 2023.PMID 37010402
- [16]Klein JD Opportunities to Improve Adolescent Health and Wellbeing Through Medical Education and Delivery of Quality Preventive Care. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2022.PMID 36122998
- [17]Jenssen BP Accelerating Innovation in Primary Care to Support Adolescent Health Discussions. Pediatrics, 2024.PMID 38836314
- [18]McGorry PD The Lancet Psychiatry Commission on youth mental health. The lancet. Psychiatry, 2024.PMID 39147461
- [19]Addison J HEADSS Up! Missed Opportunity for Psychosocial Screening in Hospitalized Adolescents. Hospital pediatrics, 2021.PMID 33789962
- [20]Ho J Digital psychosocial assessment: An efficient and effective screening tool. Journal of paediatrics and child health, 2020.PMID 31883286
- [21]Hadland SE Alcohol Use Disorder: A Pediatric-Onset Condition Needing Early Detection and Intervention. Pediatrics, 2019.PMID 30783023
- [22]Chaput JP 2020 WHO guidelines on physical activity and sedentary behaviour for children and adolescents aged 5-17 years: summary of the evidence. The international journal of behavioral nutrition and physical activity, 2020.PMID 33239009
- [23]McKay EA Parents' Perspectives on Confidentiality in Clinical Preventive Services for Adolescents. The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2025.PMID 40580168
- [24]Akande M Well-Visit Attendance From Mid-Adolescence to Young Adulthood: Who Remains Engaged? The Journal of adolescent health : official publication of the Society for Adolescent Medicine, 2026.PMID 41416974