Paeds · preventive-and-community-paediatrics
Air pollution, tobacco smoke and vaping exposure
Also known as Second-hand smoke · Environmental tobacco smoke · Third-hand smoke · E-cigarette exposure children · Youth vaping · Household air pollution · PM2.5 child health · Smoke-free home counselling
Fellowship-level approach to childhood air pollution, tobacco smoke and vaping exposure: ambient and household pollutants, second- and third-hand smoke, youth e-cigarettes, mechanisms, counselling, acute EVALI-type presentations, and regional practice differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Children grow lungs, brains and immune systems in the same air adults choose to pollute. The clinical problem is not one toxin but a stack of inhalable insults: outdoor fine particles and gases, indoor combustion from cooking and heating, tobacco smoke in all its residual forms, and nicotine aerosols from electronic products. Your job in preventive paediatrics is to make that stack visible, reduce it, and treat the diseases it drives. [1] [5] [10]
Air pollution here means ambient outdoor pollutants (especially PM2.5, ozone, nitrogen dioxide) and household air pollution from solid fuels and inefficient combustion. Tobacco smoke exposure includes active smoking in pregnancy or adolescence, second-hand smoke (environmental tobacco smoke inhaled by non-smokers) and third-hand smoke (residues on surfaces, dust and fabrics that re-emit or are mouthed). Vaping exposure covers electronic nicotine delivery systems (ENDS) used by adolescents or by caregivers around children, including dual use with combustible tobacco. [1] [6] [12]
Classification
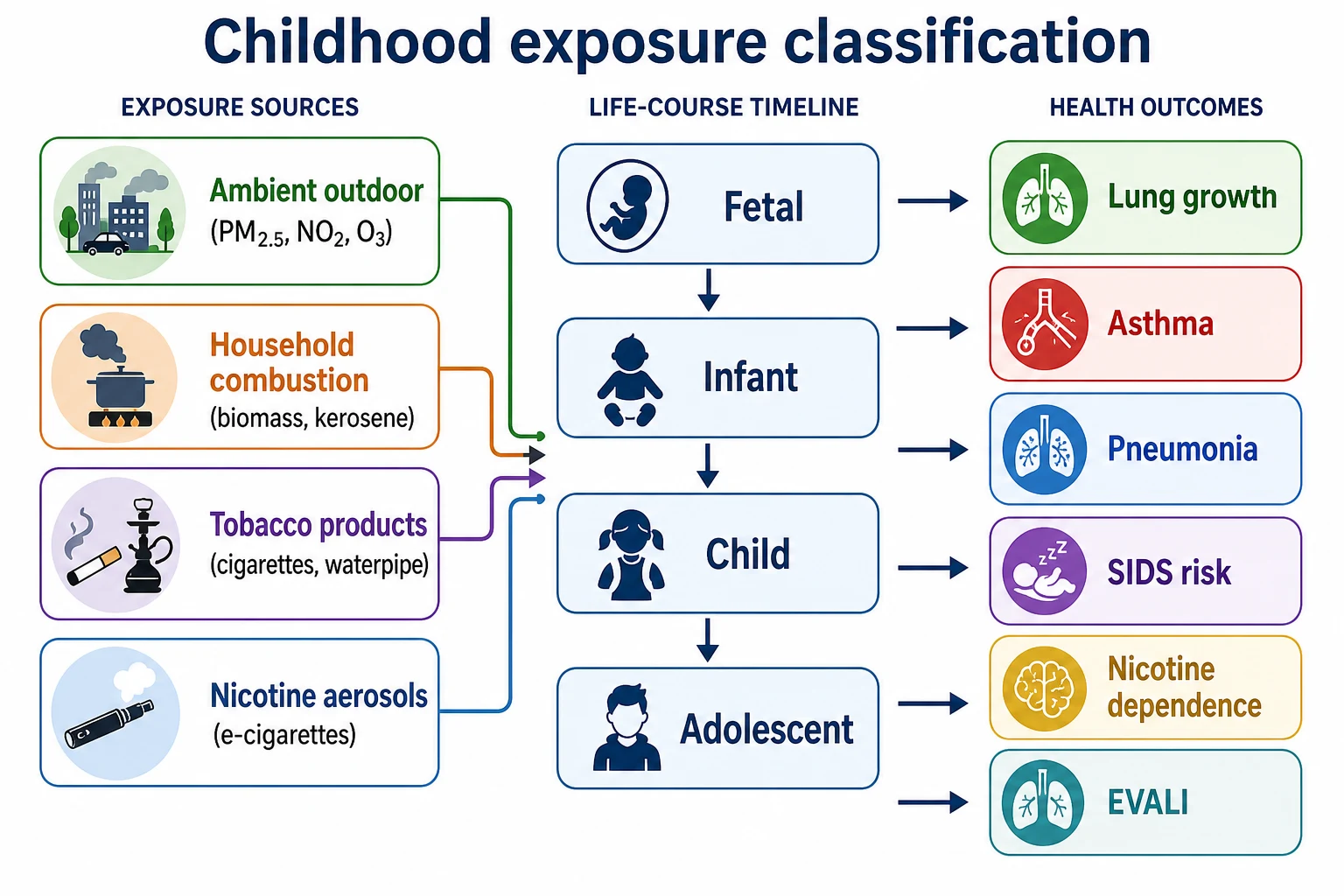
Organise every case on four axes: what is in the air, who generates it, where the child breathes it, and when in the life course exposure occurs. Those axes drive counselling scripts and urgency. [1] [5]
| Domain | Examples | Paediatric angle |
|---|---|---|
| Ambient outdoor | PM2.5, PM10, O3, NO2, SO2, wildfire smoke | Asthma days, exercise advice, equity by traffic corridor |
| Household combustion | Biomass, coal, dung, kerosene, poorly vented heaters | Global pneumonia risk; migrant and rural kitchens |
| Combustible tobacco | Cigarettes, cigars, waterpipe | SHS + third-hand; prenatal toxicity |
| Nicotine aerosols | E-cigarettes, pods, mods, heated tobacco | Youth initiation, dual use, EVALI cluster products |
Life-course timing. Fetal exposure (maternal smoking or nicotine) affects growth and airway development. Infancy concentrates SIDS and infection risk. School age shows asthma and otitis burden. Adolescence adds active use and dependence. Prevention messages change with age even when the toxicology overlaps. [3] [14]
Epidemiology & Risk Factors
Ambient fine particulate matter contributes substantially to global disease burden; integrated exposure–response models underpin estimates used in burden-of-disease work. Children with asthma are particularly sensitive to pollutant peaks. Household solid-fuel smoke remains a major driver of childhood pneumonia in low- and middle-income settings. [5] [9] [10]
Second-hand smoke exposure fell in many high-income countries after indoor bans, yet residual exposure persists in private homes and cars, multiunit housing and disadvantaged communities. Parental smoking and e-cigarette use inside homes and vehicles remain common enough that every well-child visit should ask. [1] [11]
Youth tobacco product surveillance in the United States (National Youth Tobacco Survey) continues to show e-cigarettes as a dominant product among middle- and high-school students who use tobacco products, with dual use still clinically important. Local prevalence differs by country and year — quote the latest local survey in viva, not a memorised global percentage. [13] [1]
High-yield risk clusters: parental combustible or e-cigarette use; smoking in the car; multiunit seepage; winter heating with dirty fuels; traffic or industrial corridors; wildfire seasons; asthma or BPD; prematurity; adolescence with peer and social-media marketing pressure. [1] [5] [11]
Pathophysiology
Children inhale more air per kilogram than adults, spend more time near floors and outdoor play spaces, and have airways still branching and growing. Particulate matter and oxidant gases drive airway inflammation, oxidative stress and impaired host defence, which links ambient and household pollution to wheeze, asthma exacerbations and lower respiratory infection. [5] [9] [10]
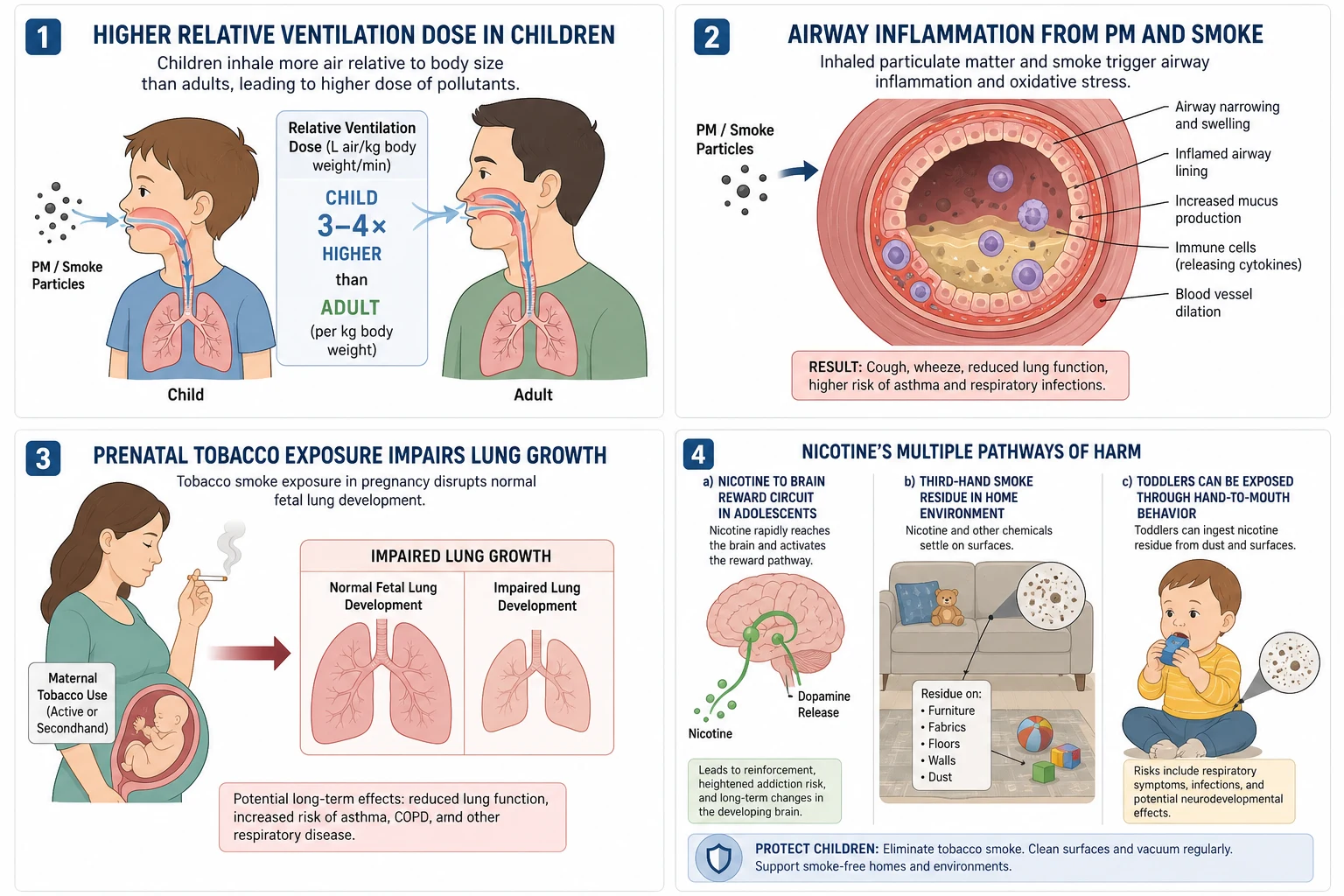
Tobacco smoke delivers thousands of combustion products. Prenatal exposure contributes to fetal hypoxia pathways, growth restriction risk and altered airway development; postnatal exposure maintains inflammation and infection susceptibility. Reviews link environmental tobacco smoke to poorer postnatal lung function trajectories and asthma risk. [3] [14]
Nicotine is not a benign flavour carrier. It is a developmental neurotoxin for reward pathways and a highly dependence-forming alkaloid. E-cigarette aerosols can contain nicotine at high effective doses, plus carbonyls, metals and flavourant toxicants. Clinician-facing reviews summarise cardiopulmonary concerns beyond simple “water vapour” marketing claims. [6] [7]
Third-hand smoke leaves nicotine and tobacco-specific compounds on surfaces and in dust. Infants and toddlers who mouth objects and crawl receive dermal and oral doses even when no one is actively smoking in the room. Residues are hard to remove with casual airing. [12]
EVALI (e-cigarette or vaping product use–associated lung injury) is an acute toxic lung injury syndrome linked in outbreak investigation to certain product practices (notably vitamin E acetate in some illicit THC cartridges in the classic US cluster), though product chemistry evolves. It is a diagnosis of exclusion that can present with respiratory and gastrointestinal symptoms. [8]
Clinical Presentation
Most exposure is silent until you ask. The history often outruns the examination. Families may say they “never smoke around the baby” while using the car as an ashtray or vaping in shared rooms. [1] [11]
When disease appears, patterns examiners expect include: [3] [4] [5]
- Recurrent wheeze or poorly controlled asthma with indoor smoke or high pollution days
- Frequent otitis media and chronic cough in SHS-exposed young children
- Lower respiratory infections, especially where household solid-fuel smoke is intense
- Adolescent daily vaping with craving, cough, chest tightness or declining sport performance
- Acute EVALI-type illness: dyspnoea, hypoxaemia, GI symptoms, bilateral infiltrates after recent product use
- Sleep disruption and behavioural irritability that families misattribute solely to “personality”
Prenatal tobacco and heavy postnatal exposure remain classic risk factors in SIDS counselling frameworks — integrate smoke-free messaging with safe-sleep teaching without replacing either. [3]
Differential Diagnosis
| Presentation | Exposure-favouring clues | Key alternatives |
|---|---|---|
| Wheeze / “viral asthma” | Indoor smoke, traffic peaks, seasonal pollution | Isolated viral bronchiolitis, atopy alone, foreign body |
| Chronic cough | SHS, biomass kitchen, damp mould co-exposure | Post-nasal drip, pertussis, aspiration, CF/PCD |
| Recurrent LRTI | Solid-fuel smoke, crowding, SHS | Immunodeficiency, aspiration, anatomic airway disease |
| Adolescent dyspnoea | Recent vaping, dual use, modified cartridges | Infection, PE rare, anxiety, primary asthma |
| Failure to thrive / small for dates | Maternal smoking/nicotine | Placental insufficiency of other cause, nutrition |
Do not force every cough into an “air pollution” label. Use exposure history to explain risk and modify triggers while completing a proper respiratory differential. [5]
Clinical & Bedside Assessment
Open without shame: “Many families are cutting down on smoking or vaping — can we talk about what smoke or vapour your child is around at home or in the car?” Blame ends disclosure. [1]
Five-minute air and nicotine exposure assessment
Products and people
Who smokes or vapes? Cigarettes, waterpipe, e-cigarettes, dual use, cannabis co-use if relevant.
Places
Inside home, balcony doorway drift, multiunit seepage, car, workplaces bringing residue home.
Pregnancy and early life
Maternal use, partners, indoor solid fuels for cooking or heating.
Child disease load
Asthma control, otitis, LRTI frequency, sleep, sport tolerance.
Adolescent confidential screen
Own use, flavours, nicotine strength, dependence, supply source, dual use.
Plan and teach-back
Agree smoke-free/vape-free home and car steps; link cessation; write one next action.
Examine growth, work of breathing, oxygen saturation, chest findings and ear status. Smell of smoke on clothing is a soft clue only — never a confrontation tool. For adolescents, use confidential time; parents need the public-health message, but dependence treatment needs a private alliance. [1] [7]
Investigations
Exposure is primarily a history diagnosis. Objective biomarkers such as cotinine can support advocacy, research or contested custody contexts, but most preventive visits do not need them to act. [1] [3]
When investigations help: [5] [8]
- Spirometry or peak-flow trends in school-age asthma when pollution or smoke is a suspected trigger
- Chest radiograph and infection workup for severe LRTI or possible EVALI
- Specialist respiratory pathways for hypoxaemic vaping-associated illness (exclude infection; consider advanced imaging as guided)
Do not order commercial “toxin panels” or “lung detox” tests. Air quality indices guide outdoor activity advice; they do not diagnose an individual child. [5]
Management — Resuscitation
Treat the physiology first. Severe asthma, bronchiolitis with hypoxia, or suspected EVALI follows standard paediatric emergency pathways: oxygen, inhaled therapy as indicated, fluids carefully, early senior help. Remove the child from ongoing indoor aerosol while you resuscitate. [5] [8]
Suspected EVALI needs supportive care, exclusion of infection, and early respiratory/critical-care involvement. Corticosteroid use is individualised with specialist advice — do not claim a single universal steroid recipe in the viva without naming that caveat. Stop the implicated product. [8]
Infant life-threatening events in heavy smoke environments require medical stabilisation plus an immediate safety plan for air quality and safe sleep. [3]
Management — Definitive & Stepwise
Most of your impact is preventive and conversational, not pharmacologic. [1]
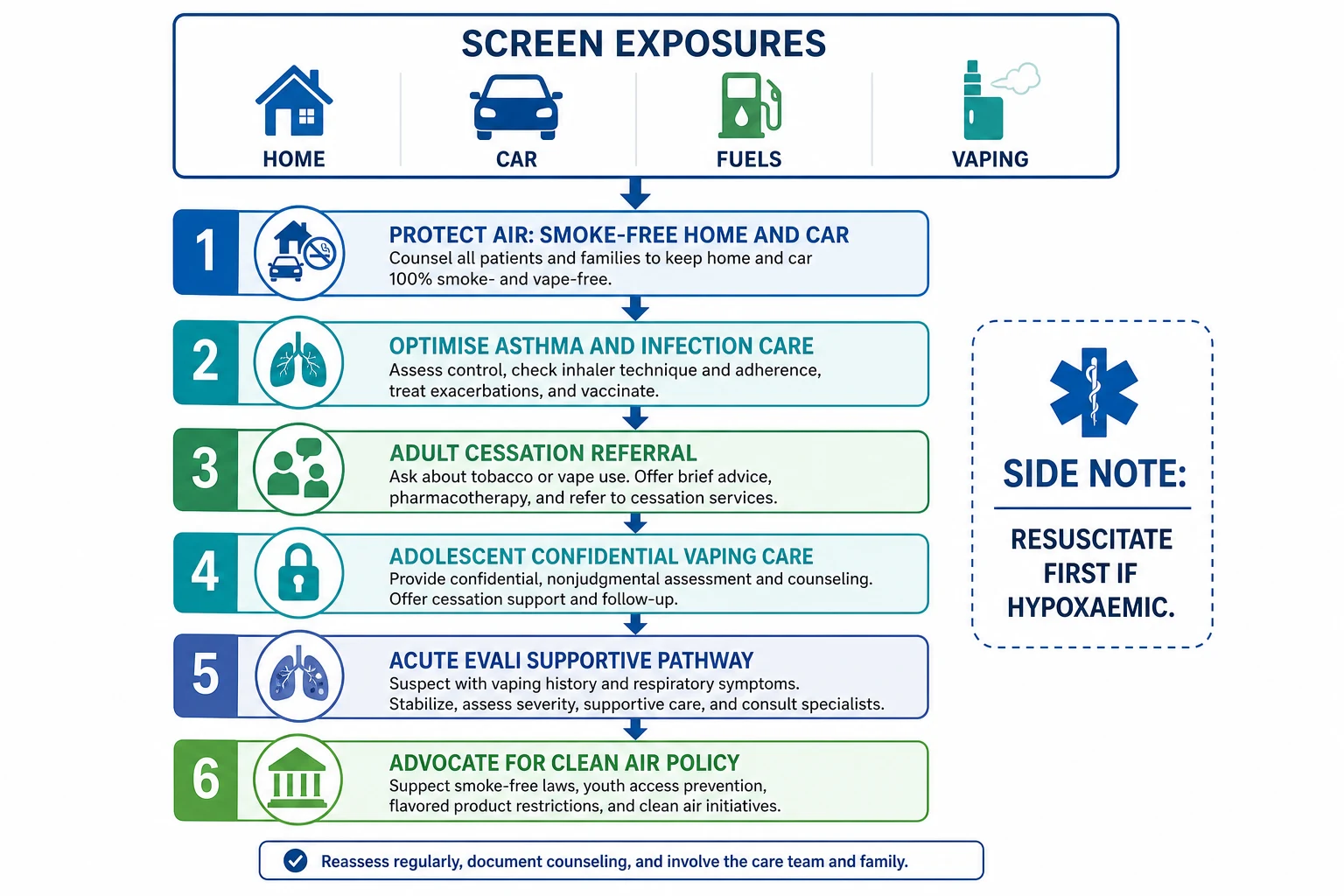
1. Primary prevention. Support pregnancy tobacco and nicotine cessation. Keep all homes and cars smoke-free and vape-free. Promote clean household energy where solid fuels dominate. Reduce outdoor exertion on high-pollution or wildfire days for children with asthma. [1] [5] [9]
2. Brief intervention for caregivers. Ask, advise, assist, arrange. Offer local quitline, primary-care cessation and nicotine replacement pathways for adults. Focus on the child’s health without humiliating the parent. Smoking outside with residual third-hand contamination still needs honest discussion. [1] [11] [12]
3. Disease control. Escalate asthma preventer therapy when exposure is hard to eliminate immediately, while still working on air quality. Treat infections on merit. Written action plans should name smoke and pollution as triggers. [4] [5]
4. Adolescent vaping care. Confidential counselling, dependence assessment, behavioural support, and school liaison when helpful. Pharmacotherapy for nicotine dependence in adolescents is evolving and jurisdiction-specific — state principles and involve experienced clinicians rather than inventing adult doses for children. Address dual use explicitly. [1] [6] [7]
5. Environmental adjuncts. HEPA filtration can reduce indoor particles as an adjunct, not a licence to smoke indoors. Ventilation helps cooking emissions; it does not make indoor smoking safe. [5]
6. Advocacy. Smoke-free multiunit housing, taxation and marketing limits on youth-appealing products, school policies, and clean cooking transitions are part of paediatric professionalism, not optional politics. [1] [2]
What each intervention actually achieves
- Cuts the dominant private SHS source
- Reduces third-hand loading over time
- Protects siblings and visitors
- Reduces exacerbation risk while exposure falls
- Does not neutralise ongoing smoke
- Needs a written trigger plan
- Targets dependence and dual use
- Needs confidentiality and follow-up
- Not solved by one scare lecture
Specific Subtypes & Scenarios
Well-child visit, smoking parent. Normalise the question. Agree a smoke-free home and car as the first win even if adult cessation will take time. Offer cessation referral every visit. [1] [11]
School-age asthma with winter flares. Map indoor smoke, unflued heaters and outdoor pollution. Step up controller therapy and write pollution/smoke into the action plan. [4] [5]
Adolescent exclusive vaping. Confidential history of device type, nicotine concentration, frequency, withdrawal and supply. Counsel addiction risk and cardiopulmonary uncertainty; plan follow-up. Screen for combustible dual use. [6] [7] [13]
Suspected EVALI. Acute respiratory ± GI illness after vaping: oxygen, exclude infection, imaging as indicated, specialist care, stop product, report per local public-health pathways. [8]
Household biomass and recurrent pneumonia. Treat the infection, then counsel clean fuels, improved stoves and ventilation as feasible, and link social supports. This is global child-health core knowledge, not only “overseas medicine.” [9]
Wildfire or extreme PM days. Temporary outdoor activity limits for high-risk children, indoor particle reduction, medication readiness for asthma. [5]
Prenatal nicotine use. Partner with maternity services; emphasise fetal growth and future lung health; offer intensive cessation support. [3] [14]
Complications & Pitfalls
Medical complications span SIDS risk pathways, recurrent otitis, impaired lung growth, asthma morbidity, pneumonia risk with household pollution, nicotine dependence, and rare but severe acute lung injury from certain vaping products. Equity compounds each of these. [3] [4] [9]
Prognosis & Disposition
Reducing exposure improves asthma control and lowers infection-related morbidity; some structural effects of early-life smoke on lung growth may persist, which is why prevention starts before birth. Nicotine dependence is chronic and needs longitudinal care, not a single clinic pep talk. [3] [4] [14]
Disposition follows disease severity: most counselling is outpatient; severe asthma or EVALI-type illness may need ward or intensive care. Never discharge a hypoxaemic adolescent back to continued product use without a clear stop plan and follow-up. [5] [8]
Special Populations
Fetus and neonate. Growth restriction risk, altered lung development, and SIDS-associated pathways make pregnancy and the first months high-yield for smoke-free counselling. [3]
Infants and toddlers. Highest relative dose, mouthing of third-hand residues, bronchiolitis and otitis burden. [3] [12]
Chronic lung or cardiac disease. Lower threshold for harm from pollution peaks and indoor smoke; individualise outdoor activity advice. [5]
Adolescents. Initiation, flavoured products, social networks, dual use and dependence. Confidentiality rules still apply within local safeguarding limits. [1] [7] [13]
Indigenous, migrant, refugee and socioeconomically disadvantaged families. Higher exposure clustering and fewer housing choices. Offer practical steps, interpreters and non-blaming partnership; advocate for structural fixes. [1] [9]
Evidence, Guidelines & Regional Differences
Core anchors include the AAP 2023 policy and technical report on protecting children and adolescents from tobacco and nicotine, DiFranza’s synthesis of prenatal and postnatal environmental tobacco smoke harms, meta-analytic evidence that SHS worsens paediatric asthma morbidity, clinician reviews of e-cigarette cardiopulmonary effects, EVALI reviews, household solid-fuel pneumonia meta-analysis, and PM2.5 burden modelling. [1] [2] [3] [4] [6] [8] [9] [10]
Australia and Aotearoa New Zealand combine strong outdoor smoke-free public norms with ongoing private-home exposure and a youth vaping challenge. Use local quit services, school frameworks and product regulations; clinical principles match AAP toxicology even when product law differs. Household solid-fuel issues matter for some rural and migrant households. [1] [5]
Controversies to handle cleanly. E-cigarettes may help some adults quit combustibles while simultaneously addicting nicotine-naive youth — paediatric duty of care prioritises youth protection. Outdoor air standards and clean-cooking implementation are political as well as medical; your viva answer is still the child’s lungs. [1] [6] [10]
Exam Pearls
CLEARAIR
If you remember only one chain: contaminated air → higher childhood dose → inflamed growing lungs and nicotine-exposed brains → preventable morbidity. Your job is to clean the air and interrupt nicotine uptake. That is the fellowship answer. [1] [3] [10]
References
- [1]Jenssen BP Protecting Children and Adolescents From Tobacco and Nicotine. Pediatrics, 2023.PMID 37066668
- [2]Jenssen BP Protecting Children and Adolescents From Tobacco and Nicotine. Pediatrics, 2023.PMID 37066685
- [3]DiFranza JR Prenatal and postnatal environmental tobacco smoke exposure and children's health. Pediatrics, 2004.PMID 15060193
- [4]Wang Z Effects of secondhand smoke exposure on asthma morbidity and health care utilization in children: a systematic review and meta-analysis. Annals of allergy, asthma & immunology, 2015.PMID 26411971
- [5]Tiotiu AI Impact of Air Pollution on Asthma Outcomes. International journal of environmental research and public health, 2020.PMID 32867076
- [6]Neczypor EW E-Cigarettes and Cardiopulmonary Health: Review for Clinicians. Circulation, 2022.PMID 35041473
- [7]Livingston JA Physical and mental health outcomes associated with adolescent E-cigarette use. Journal of pediatric nursing, 2022.PMID 35121206
- [8]Belok SH E-cigarette, or vaping, product use-associated lung injury: a review. Pneumonia (Nathan Qld.), 2020.PMID 33110741
- [9]Chen T Indoor air pollution from solid fuel on children pneumonia in low- and middle-income countries: a systematic review and meta-analysis. Environmental science and pollution research international, 2022.PMID 35066845
- [10]Burnett RT An integrated risk function for estimating the global burden of disease attributable to ambient fine particulate matter exposure. Environmental health perspectives, 2014.PMID 24518036
- [11]Drehmer JE Parental Smoking and E-cigarette Use in Homes and Cars. Pediatrics, 2019.PMID 30858346
- [12]Vanzi V Thirdhand Smoke and Neonatal/Pediatric Health: A Scoping Review on Nursing Implications. Healthcare (Basel, Switzerland), 2025.PMID 41464358
- [13]Jamal A Tobacco Product Use Among Middle and High School Students - National Youth Tobacco Survey, United States, 2024. MMWR. Morbidity and mortality weekly report, 2024.PMID 39418216
- [14]Wang L Detrimental effects of tobacco smoke exposure during development on postnatal lung function and asthma. Birth defects research. Part C, Embryo today : reviews, 2008.PMID 18383132