Paeds · preventive-and-community-paediatrics
Cardiovascular risk screening in childhood
Also known as Paediatric cardiovascular risk screening · Childhood blood pressure screening · Paediatric lipid screening · Familial hypercholesterolemia screening children · Cardiometabolic risk screening childhood
Fellowship approach to childhood cardiovascular risk screening: blood pressure technique and staging, lipid screening including the universal-versus-selective debate, obesity-related risk, familial hypercholesterolemia clues, staged work-up, lifestyle first-line care, referral triggers and regional guideline differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
C.U.F.F. S.A.F.E. screen
Overview & Definition
A school-age child sits for a “routine BP.” The number looks high. The trap is either panicking into adult hypertension labels or ignoring a real signal. Cardiovascular risk screening in childhood means structured detection of risk factors that begin damaging arteries early: elevated blood pressure, dyslipidaemia (including familial hypercholesterolemia), excess adiposity, diabetes risk, smoke or vape exposure, inactivity and adverse family history. [1] [3] [4]
Screening is not the same as diagnosing lifelong disease from one visit. You measure, interpret with paediatric rules, confirm abnormalities, then stage lifestyle care or work-up. High-risk paediatric groups (for example diabetes, CKD, repaired complex heart disease, transplant) need tighter surveillance than average-risk well children. [4]
This page owns screening logic and first-line action. Cross-link dedicated hypertension pharmacology, lipid clinic protocols and obesity intensive treatment leaves rather than hiding full drug monographs here when doses are jurisdiction-specific. [1] [5]
Classification
By risk domain. Blood pressure. Lipids (LDL-focused for atherosclerosis risk). Adiposity/BMI. Glycaemic risk. Tobacco/vape exposure. Physical activity and diet pattern. Family history of premature atherosclerotic cardiovascular disease (ASCVD) or known FH. [3] [4]
By strategy. Universal age-based testing versus selective testing triggered by obesity, diabetes risk, kidney disease, drugs, or family history. Lipid policy is the classic controversy: AAP-linked childhood lipid guidance has supported broader screening, while USPSTF 2023 again found insufficient evidence for routine screening of asymptomatic youth. [2] [3] [7]
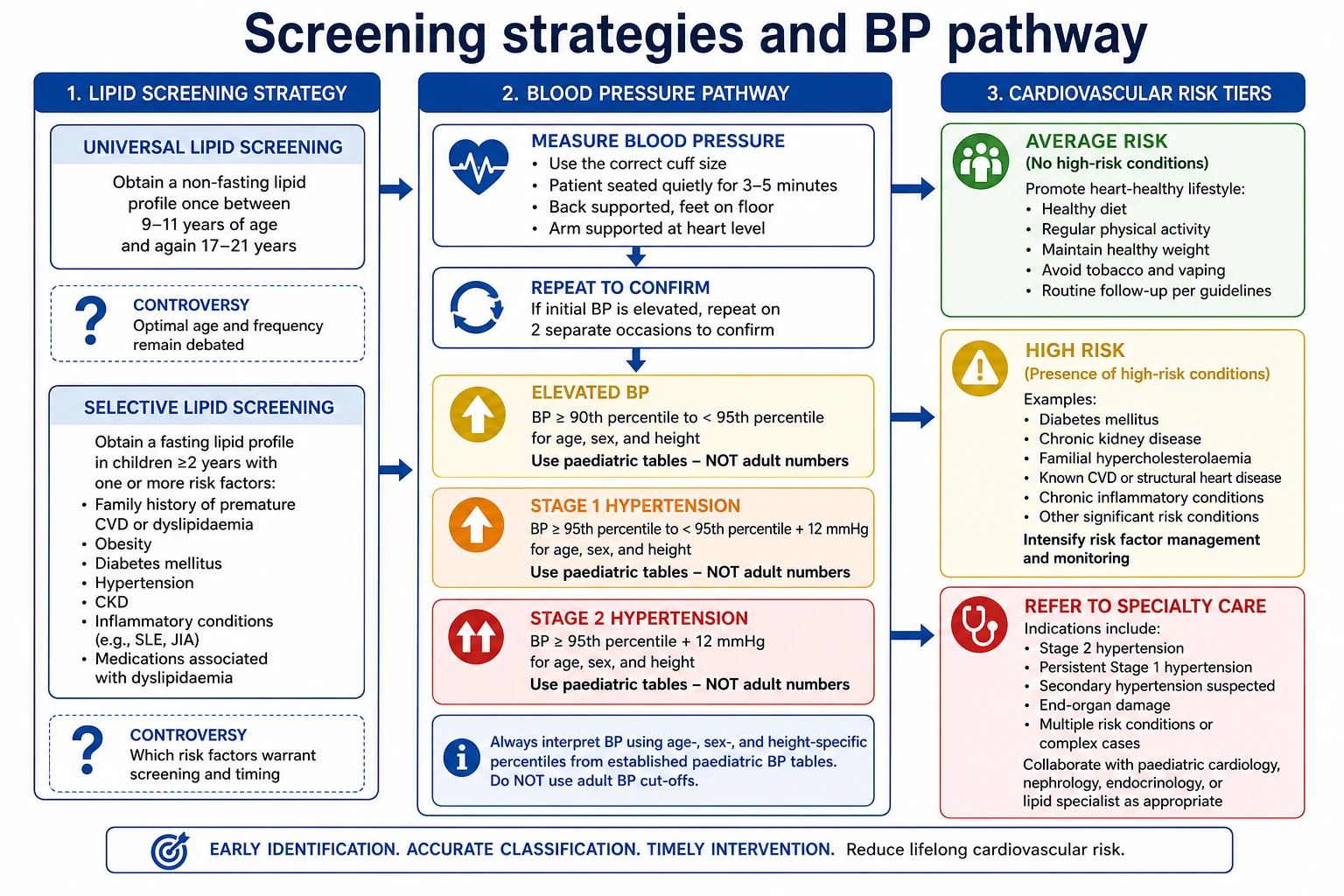
By BP category (framework). Flynn and colleagues’ 2017 AAP clinical practice guideline redefined paediatric BP tables (normal-weight reference) and staging language (normal, elevated, stage 1, stage 2) with age-based simplified thresholds for adolescents at the upper end. Use the guideline tables rather than inventing numbers in a viva if you cannot recall exact percentiles. [1] [8]
By disposition after screen. Normal — lifestyle reinforcement and routine recall. Abnormal unconfirmed — repeat. Confirmed mild — lifestyle and scheduled follow-up. Confirmed severe, symptomatic, or secondary features — work-up and specialty referral. [1] [4]
Epidemiology & Risk Factors
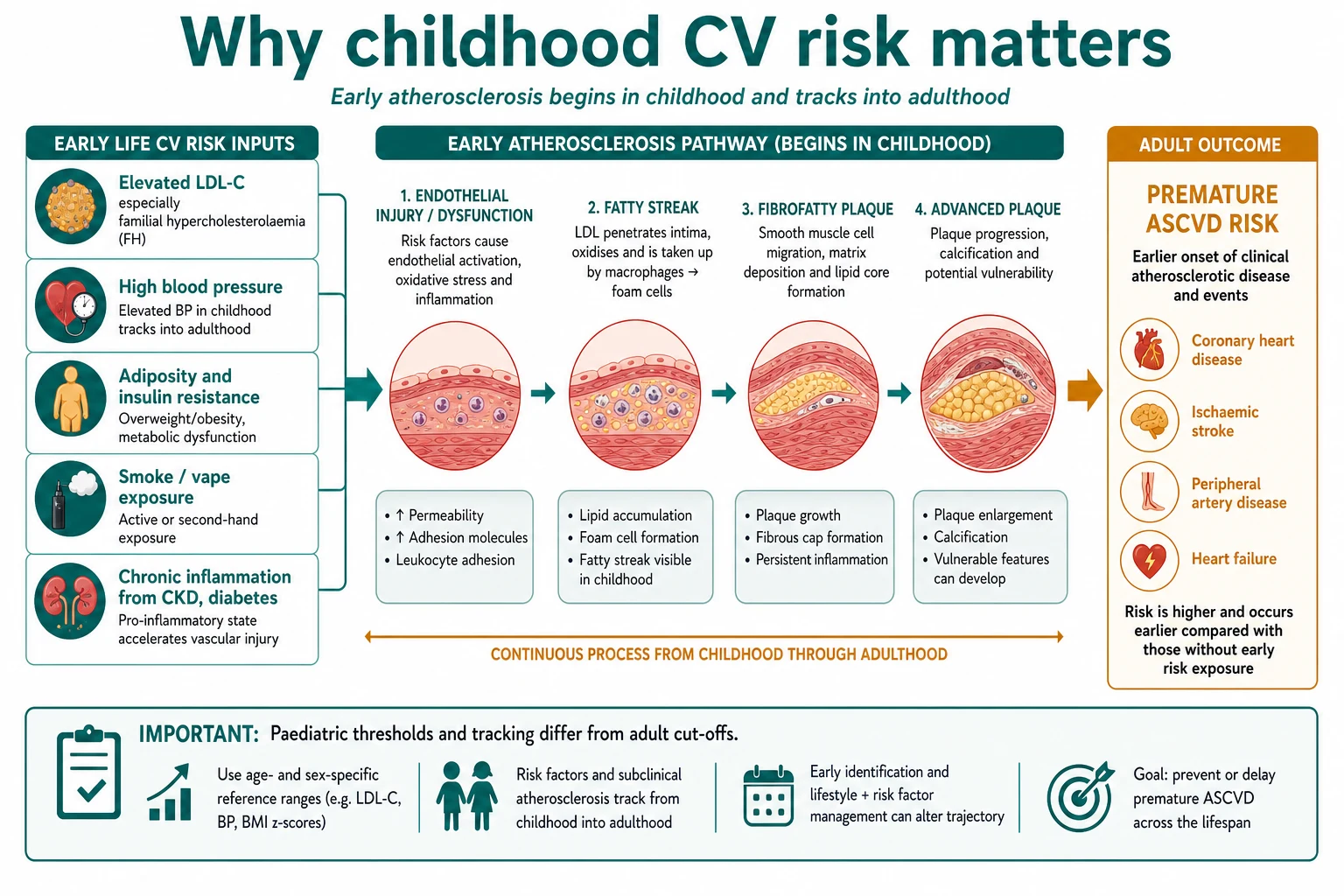
Childhood BP and lipid elevations can track into adulthood. Obesity prevalence multiplies the chance you will find elevated BP, abnormal lipids and insulin resistance in the same clinic. [5] Familial hypercholesterolemia is under-detected when family history is unknown and lipids are never measured; missing it wastes years of prevention. [3] [6]
Equity matters. Families with transport barriers, language discordance or fragmented care miss repeated BP checks and lab follow-up. Medical complexity can overshadow routine risk screening. [9] [11] Caregiver concern still matters when a child seems unwell at a “BP review” — escalate acute assessment if the child looks sick. [10]
Pathophysiology
Atherosclerosis begins with endothelial injury and lipid retention in the arterial intima. High LDL cholesterol, especially lifelong elevation in FH, accelerates fatty streaks that can become plaque decades later. Elevated BP adds mechanical stress. Adiposity and insulin resistance promote a proinflammatory, prothrombotic milieu. Smoke and vape aerosols add further vascular injury. [3] [4]
Blood pressure in clinic is the product of cardiac output and systemic vascular resistance, filtered through measurement error. A cuff that is too small falsely raises readings. Anxiety raises readings (white-coat effect). That is why confirmation and ambulatory strategies appear in paediatric HTN pathways. [1] [8]
Paediatric percentile tables exist because normal BP rises with age and height. Adult cut-offs misclassify young children. [1]
Clinical Presentation
Most screened children are asymptomatic. You may meet: [1] [3]
- An incidental high office BP at a well visit.
- A child with obesity, acanthosis and a family of early heart disease.
- A teenager who vapes and has a parent with MI at 42.
- Rarely, xanthomas or extremely high LDL pointing to FH.
- Clues to secondary hypertension: poor femoral pulses, abdominal bruit, oedema, growth failure, known kidney disease, endocrine signs. [1] [3] [4]
Differential Diagnosis
High office BP. True hypertension (primary or secondary) versus white-coat elevation versus wrong cuff versus pain/anxiety versus recent stimulant. [1]
High LDL. FH versus polygenic hypercholesterolemia versus secondary causes (hypothyroidism, nephrotic syndrome, cholestasis, some drugs) versus non-fasting artefact depending on which particles you interpret. [3] [6]
Clustered risk. Obesity-related cardiometabolic pattern versus monogenic disease versus medication effects (for example some antipsychotics). [5]
Clinical & Bedside Assessment
History. Perinatal course, kidney or heart disease, medications (including stimulants, steroids, oral contraceptives in adolescents), sleep-disordered breathing symptoms, diet pattern, activity minutes, smoke/vape exposure, and three-generation family history of premature ASCVD, high cholesterol, sudden death or known FH. [1] [3]
Blood pressure technique. Child seated, feet on floor, arm supported, correct cuff bladder size, quiet rest when feasible. Repeat abnormal readings in the same visit. Compare limbs and feel femorals when secondary causes are plausible. Plot against paediatric tables/guideline staging — not adult shortcuts — unless the adolescent simplified thresholds in the 2017 CPG apply. [1] [8]
Growth. Height, weight, BMI-for-age. Excess weight changes pretest probability of elevated BP and lipids and guides lifestyle intensity. [5]
Exam. Heart sounds, pulses, radiofemoral delay, thyroid, abdomen, oedema, rare lipid deposits, acanthosis. [1] [4]
Document numbers, cuff size, limb, and posture so the next clinician can interpret the trend. Structured handover reduces lost abnormal results. [12]
Investigations
After elevated BP. Confirm with repeated visits as the guideline pathway requires. Consider ambulatory BP monitoring when available for white-coat questions. Evaluation for secondary causes is not automatic for every mild elevation; it is driven by age, stage, persistence and clinical clues. [1]
Lipids. Follow local policy. If testing, know whether your lab panel is fasting or non-fasting and how your service interprets results. Confirm marked abnormalities before lifelong labels. Seek secondary causes when indicated. [2] [3] [6]
High-risk conditions. Children with diabetes, CKD, Kawasaki with persistent aneurysms, severe obesity with comorbidities, or other AHA high-risk categories need condition-specific intensification rather than average-risk schedules alone. [4]
Avoid. Adult coronary calcium scoring as a routine paediatric screen. Random genetic panels without lipid clinic context. Lab shotgun panels for a single mildly high BP with clear white-coat features. [1] [4]
Management — Resuscitation
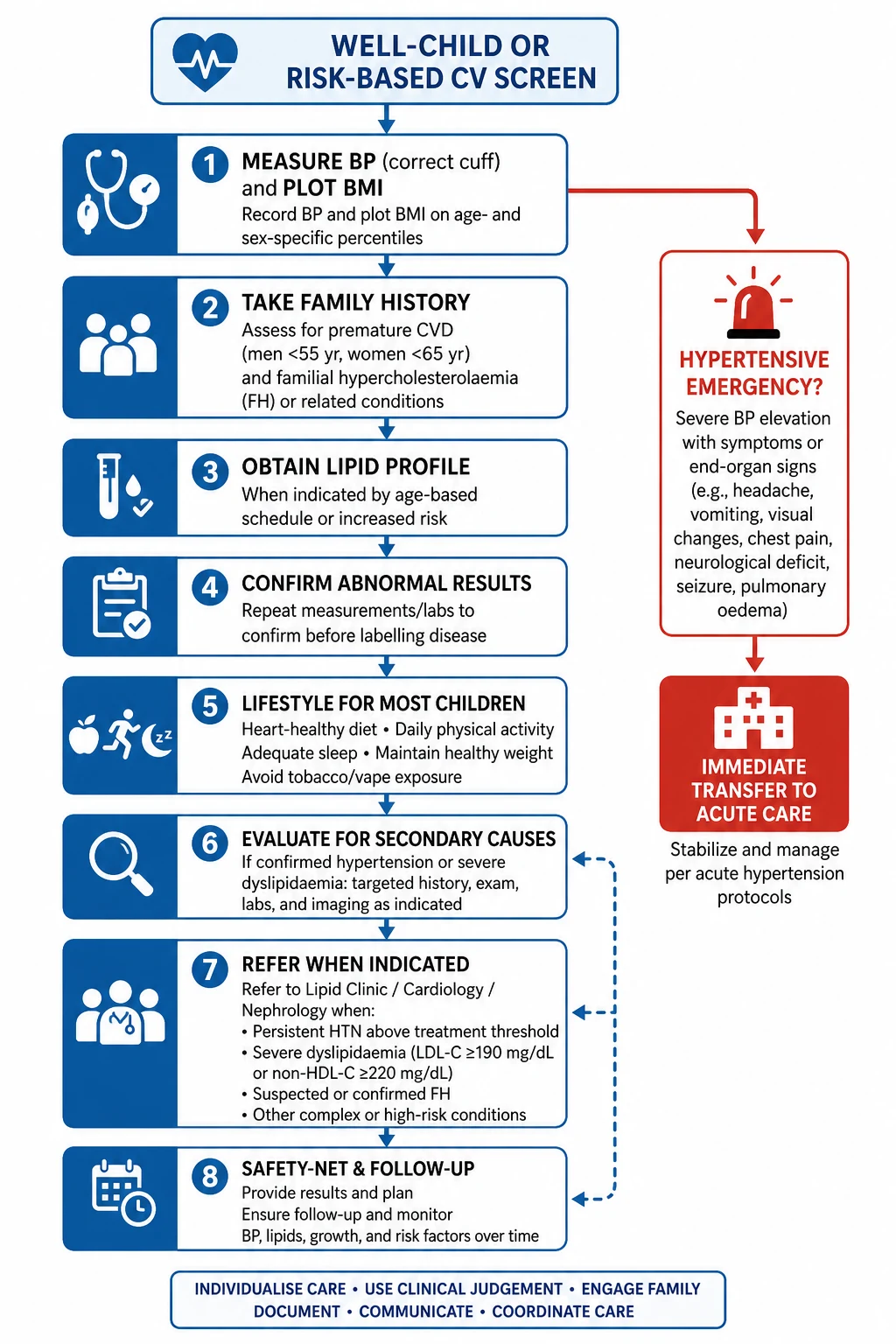
Hypertensive emergency features (encephalopathy, acute heart failure, severe acute kidney injury) are acute care problems. Stabilise ABCDE, use local hypertensive emergency pathways, and do not treat this as a lifestyle counselling visit. [1] [10]
A single high reading in a well child is not an emergency drug start. Confirm, assess symptoms, and follow staged outpatient rules unless the child is unwell. [1]
Management — Definitive & Stepwise
- Measure correctly — cuff, position, repeat. Plot BMI. [1] [5]
- Take family and risk history including premature ASCVD and FH clues. [3]
- Apply lipid policy deliberately — universal where your service uses it, selective where it does not — and still test when risk is high. [2] [3] [7]
- Confirm abnormal results before chronic disease labelling. [1] [6]
- Lifestyle first-line for most elevated BP and non-extreme dyslipidaemia: diet quality, activity, sleep, weight trajectory support without shame, smoke/vape cessation. Obesity CPG principles support structured, non-stigmatising treatment pathways. [1] [5]
- Work-up secondary causes when age, severity, or clues demand it. [1]
- Refer to paediatric nephrology/hypertension, cardiology or lipid clinic for confirmed stage needing specialist care, suspected FH, or high-risk cardiac conditions. Do not invent statin starting doses in a viva if you cannot cite the exact local protocol — state the referral threshold and monitoring principles instead. [4] [6]
- Explain with teach-back, share decisions with consent principles, and safety-net follow-up timing. [13] [14]
Specific Subtypes & Scenarios
Suspected FH. Very high LDL, family premature CVD, or known parental FH — expedite lipid clinic/genetics pathways and cascade family testing per local rules. [3] [6]
Obesity with elevated BP and lipids. Combine non-stigmatising obesity care with BP and lipid confirmation; treat the cluster, not one lab in isolation. [5]
CKD or diabetes. Use high-risk paediatric CV statements: tighter targets and earlier specialty partnership. [4]
White-coat pattern. Repeated normal out-of-office readings with correct technique; still counsel lifestyle and recheck schedules. [1]
Adolescent. Simplified BP thresholds at older ages per 2017 CPG, confidential smoke/vape history, and transition planning if chronic risk is confirmed. [1] [8]
Incomplete family history. Do not assume low risk; this is a reason some systems prefer broader lipid screening. [3] [7]
Complications & Pitfalls
Wrong cuff size. Labelling hypertension from one reading. Using adult 140/90 in a seven-year-old. Ignoring weak femorals. Missing FH because “USPSTF is inconclusive so I never test anyone.” Shaming weight. Starting multiple antihypertensives in clinic without confirmation. Losing abnormal lipid results between visits. [1] [2] [12]
Prognosis & Disposition
Childhood risk is modifiable. Early lifestyle change and treatment of FH or sustained hypertension change long-term arterial outcomes more than late adult catch-up alone. Disposition ranges from primary-care lifestyle follow-up to hypertension clinic, lipid clinic, nephrology or cardiology. Always leave a written recheck plan. [3] [4] [14]
Special Populations
Indigenous and disadvantaged families. Higher cardiometabolic burden in many populations — screen access and culturally safe counselling matter as much as lab thresholds. [5] [11]
Language discordance. Professional interpreters for risk counselling and consent to cascade testing. [11] [13]
Medical complexity. Do not let technology dependence erase BP and lipid surveillance when life expectancy and quality benefit. [9]
High-risk cardiac cohorts. Follow condition-specific AHA risk reduction statements rather than average well-child intervals alone. [4]
Evidence, Guidelines & Regional Differences
Flynn 2017 is the core paediatric BP screening and management CPG used in exams worldwide as the modern US reference. [1] Blanchette reviews practical implications of that shift. [8] Daniels 2008 captures AAP lipid screening and cardiovascular health guidance that underpins much universal-screening teaching. [3] USPSTF 2023 states the evidence remains insufficient for routine lipid screening in asymptomatic children and adolescents — the key controversy to name. [2] de Ferranti 2019 details intensification for high-risk paediatric patients. [4] Hampl 2023 obesity CPG frames non-stigmatising evaluation and treatment that intersects CV risk. [5] Wiegman reviews lipid screening action and follow-up. [6] Practice surveys show real-world cholesterol screening remains inconsistent. [7]
Use local heart foundation/paediatric society BP and lipid pathways and laboratory reference practices. Many services emphasise selective lipids plus strong family history capture; confirm your hospital guideline rather than importing US universal ages unchanged. [1] [2]
NICE FH identification pathways and local hypertension references dominate. Do not invent US percentile tables as if they were NICE text — state the local tool. [2] [6]
AAP BP CPG and Bright Futures periodicity commonly drive clinic workflows; USPSTF lipid statement creates tension with broader paediatric lipid guidance. Canadian provincial tools vary — name them. [1] [2] [3]
Exam Pearls
- Correct cuff before you interpret. [1]
- Paediatric tables, not adult defaults. [1]
- Confirm before diagnose. [1]
- Name the lipid policy controversy (USPSTF insufficient vs broader paediatric screening). [2] [3]
- Family history is still a powerful trigger. [3]
- FH is treatable — missing it is the unforgivable miss. [6]
- High-risk conditions need intensified pathways. [4]
- Lifestyle first for most; specialty for extremes. [1] [5]
- Safety-net rechecks in writing. [14]
References
- [1]Flynn JT Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics, 2017.PMID 28827377
- [2]US Preventive Services Task Force Screening for Lipid Disorders in Children and Adolescents: US Preventive Services Task Force Recommendation Statement. JAMA, 2023.PMID 37462699
- [3]Daniels SR Lipid screening and cardiovascular health in childhood. Pediatrics, 2008.PMID 18596007
- [4]de Ferranti SD Cardiovascular Risk Reduction in High-Risk Pediatric Patients: A Scientific Statement From the American Heart Association. Circulation, 2019.PMID 30798614
- [5]Hampl SE Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity. Pediatrics, 2023.PMID 36622115
- [6]Wiegman A Lipid Screening, Action, and Follow-up in Children and Adolescents. Current cardiology reports, 2018.PMID 30090990
- [7]de Ferranti SD Cholesterol Screening and Treatment Practices and Preferences: A Survey of United States Pediatricians. The Journal of pediatrics, 2017.PMID 28209292
- [8]Blanchette E Implications of the 2017 AAP Clinical Practice Guidelines for Management of Hypertension in Children and Adolescents: a Review. Current hypertension reports, 2019.PMID 30953215
- [9]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [10]Mills E Association between caregiver concern for clinical deterioration and critical illness in children presenting to hospital: a prospective cohort study. The Lancet. Child & adolescent health, 2025.PMID 40451224
- [11]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [12]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [13]Katz AL Informed Consent in Decision-Making in Pediatric Practice. Pediatrics, 2016.PMID 27456510
- [14]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428