Paeds · preventive-and-community-paediatrics
Catch-up immunisation and uncertain vaccination history
Also known as Catch-up vaccination · Delayed immunisation schedule · Incomplete vaccination history · Undocumented vaccine history · Invalid vaccine doses
Fellowship approach to reconstructing vaccination history, classifying valid versus invalid doses, building age-banded catch-up plans, using serology selectively, and documenting registers across ANZ, UK, US and Canadian practice.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A child who is late is not “behind a birthday list.” They are under-protected against specific diseases until those antigen gaps close. That is the clinical problem this page solves. [2] [8]
R.E.C.O.R.D. catch-up
Overview & Definition
Parents often arrive with a half-filled book, a photo of a foreign card, or the sentence “I think they had everything.” Your job is to turn that mess into a safe, written plan. Catch-up immunisation means giving the vaccines still needed for the child’s current age after you account for valid past doses. It is not restarting every series from zero when good doses already exist. [1] [2]
Uncertain vaccination history means you cannot verify dates, products, or doses for one or more antigens. Verbal history alone is weak evidence for most antigens. National registers, clinic records, and parent-held cards with dates are stronger. When uncertainty remains after a proper search, the usual default is to vaccinate, not to wait for perfect paperwork. [1] [4]
This page owns history reconstruction, dose validity, multi-visit planning, selective serology, and regional operational differences. Cross-link national schedule comparison, contraindications and adverse events, and vaccine hesitancy topics rather than hiding those full chapters here. [1]
Classification
Classify two things separately: the quality of the history, and the validity of each dose. History quality runs from registry-verified, to written parent-held record, to verbal only, to no history. Dose validity asks whether each administration met minimum age, minimum interval, and age-appropriate product rules. [1] [3]
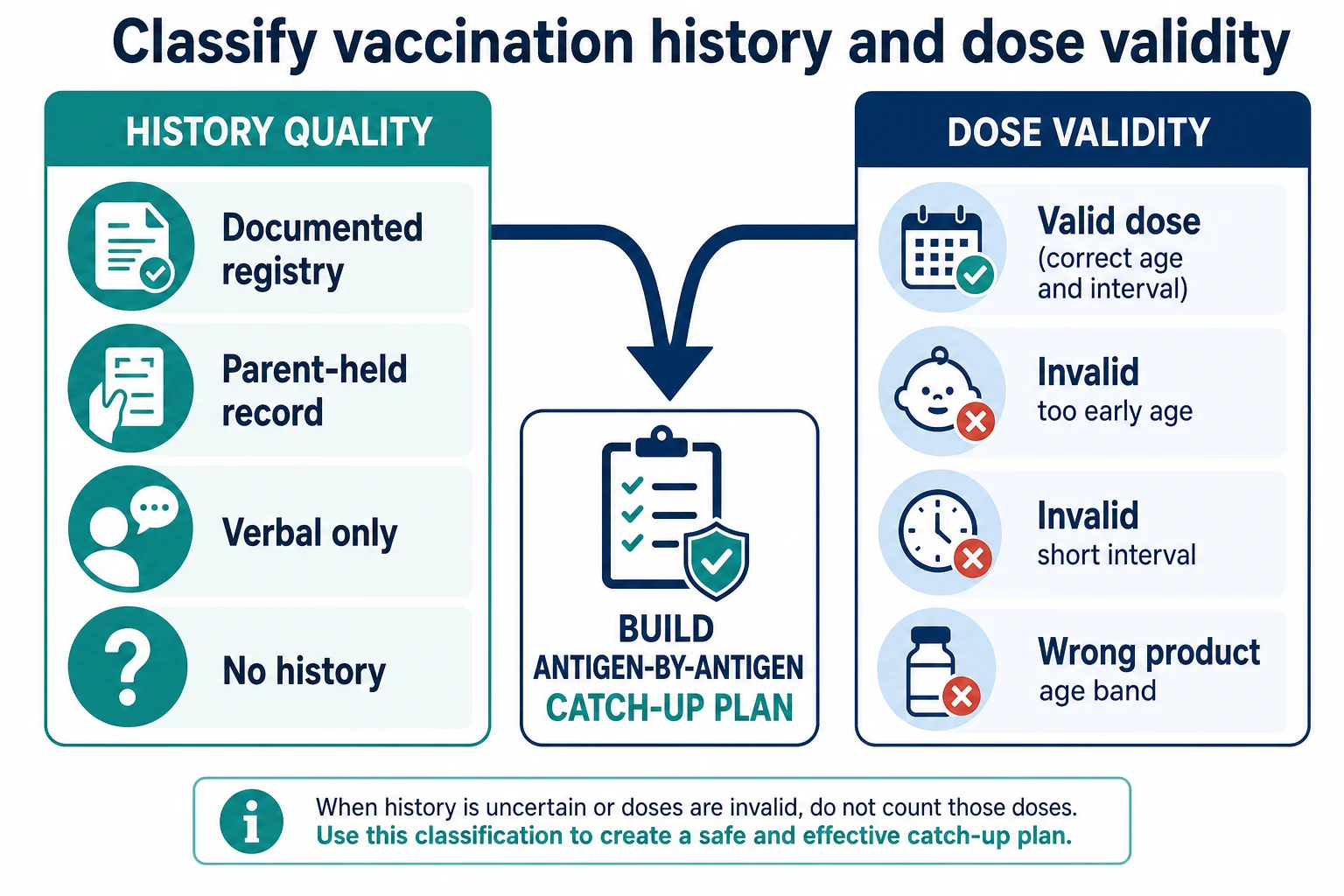
Also classify the reason for incompleteness. Access barriers, mobility, migration, medical delay, and hesitancy need different counselling and follow-up, even when the antigen gap looks the same on paper. [4] [5] [8]
Epidemiology & Risk Factors
Catch-up work concentrates in children who miss well-child visits, move between services, migrate or seek asylum, enter out-of-home care, or live with transport and language barriers. Coverage reports still show residual gaps even in high-income systems, so opportunistic review at every encounter matters. [7] [8]
Immigrant, refugee, and internationally adopted children often carry foreign schedules, different product names, or no documents at all. They need structured catch-up as part of the broader newcomer health assessment, not a shrug that “home country vaccines were probably fine.” [4] [5] [9]
Under-immunised clusters raise outbreak risk for measles and other vaccine-preventable diseases. In those settings, delayed catch-up is not a paperwork inconvenience. It is a public-health exposure. [2] [8]
Pathophysiology
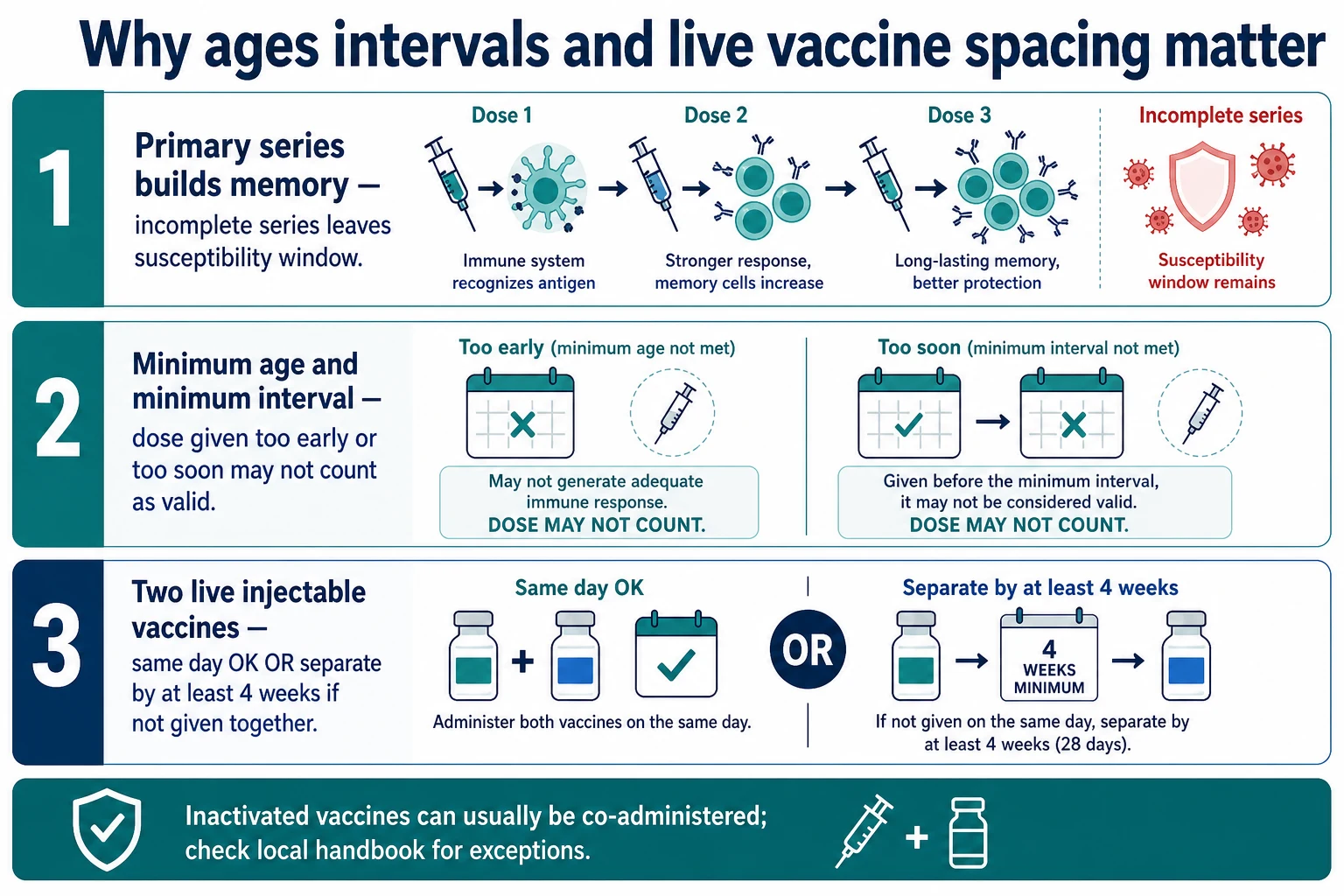
Primary series build immune memory step by step. An incomplete series leaves a susceptibility window that widens during school, travel, or community outbreaks. That is why you close gaps early rather than waiting for the next birthday visit. [1] [2]
Minimum ages and minimum intervals exist because the immune system needs time and developmental readiness for a reliable response. A dose given too early in life, or too soon after a previous dose of the same antigen, may not count as a valid series dose. Invalid doses create false security if you treat them as complete. [1] [3]
Live injectable vaccines can interfere with each other if they are separated by a short interval. Give them on the same day, or separate them by at least four weeks when they are not given together. Inactivated vaccines can usually be co-administered or spaced freely, with handbook exceptions checked locally. [1]
Serology can help for selected antigens such as hepatitis B in defined scenarios, but antibody levels fall over time and assays are imperfect. Negative serology does not always mean “never vaccinated,” and positive serology is not available or validated for every antigen you need to catch up. [6]
Clinical Presentation
The classic visit is quiet: a new school form, a refugee health check, a toddler who “missed a few needles,” or an adolescent without HPV, meningococcal, or tetanus-diphtheria-pertussis boosters. Sometimes the presentation is urgent — an under-immunised child exposed to measles — and the pathway is post-exposure prophylaxis, not a leisurely multi-visit calendar. [2] [4]
Listen for phrases that signal uncertainty: “the book was lost in the move,” “they had injections overseas,” “the clinic said they were up to date,” or “we stopped after a fever.” Each phrase points you to records first, then a safety screen, then a plan. [4] [5]
Differential Diagnosis
Separate true never-vaccinated status from partial vaccination with missing documents, and from full vaccination that was never reported. Separate medical delay (true contraindication or precaution) from access delay and from hesitancy. Those three look alike on a blank page and need different next steps. [1] [4]
Also separate invalid early doses from valid doses given under a different national schedule with unfamiliar product names. A foreign combination vaccine may still count for its antigens if age and intervals were valid. Do not discard a whole overseas history because the brand is unfamiliar. [1] [5]
Clinical & Bedside Assessment
Start with open questions. Which country and clinic gave vaccines? Are there dates, stamps, or product names? Any severe allergic reaction, encephalopathy after pertussis-containing vaccine, or current immunosuppression? Any pregnancy risk in an adolescent before live vaccines? Then search the national register and local records before you invent a plan from memory. [1] [7]
Examine only what changes safety today: acute severe illness, unstable chronic disease, signs of immunosuppression when relevant. Mild afebrile colds usually do not block inactivated vaccines. Document the source of every counted dose. If another clinician will give the injections, hand over the antigen list and the next valid dates clearly. [1]
Use professional interpreters for language-discordant families. Catch-up counselling fails when the family cannot name past reactions or understand return dates. [4] [9]
Investigations
Registry lookup is the first investigation. In Australia, the Australian Immunisation Register supports practice-level catch-up and coverage improvement when used actively. Similar immunisation information systems serve UK, US, and Canadian services. [7] [8]
Serology is selective, not default. Hepatitis B surface antibody testing can guide management in incomplete series or special risk groups according to local hepatitis B guidance. Routine multi-pathogen serology panels for every uncertain history delay care and rarely replace vaccination for measles-containing and many other antigens. Prefer vaccinate-now when records are missing and there is no contraindication. [1] [6]
Pregnancy testing before live vaccines in adolescents follows local protocol and clinical context. Do not invent a universal lab panel for every catch-up visit. [1]
Management — Resuscitation
Most catch-up is outpatient preventive care. The emergency exception is exposure. An under-immunised child exposed to measles, varicella, or hepatitis B may need immunoglobulin, vaccine within a time window, or both, according to public-health advice. That pathway outranks a routine multi-visit schedule. [2] [6]
Every vaccination session still needs anaphylaxis readiness: trained staff, adrenaline, and observation per local policy. True anaphylaxis to a vaccine component is a stop sign until specialist review. [1]
Management — Definitive & Stepwise
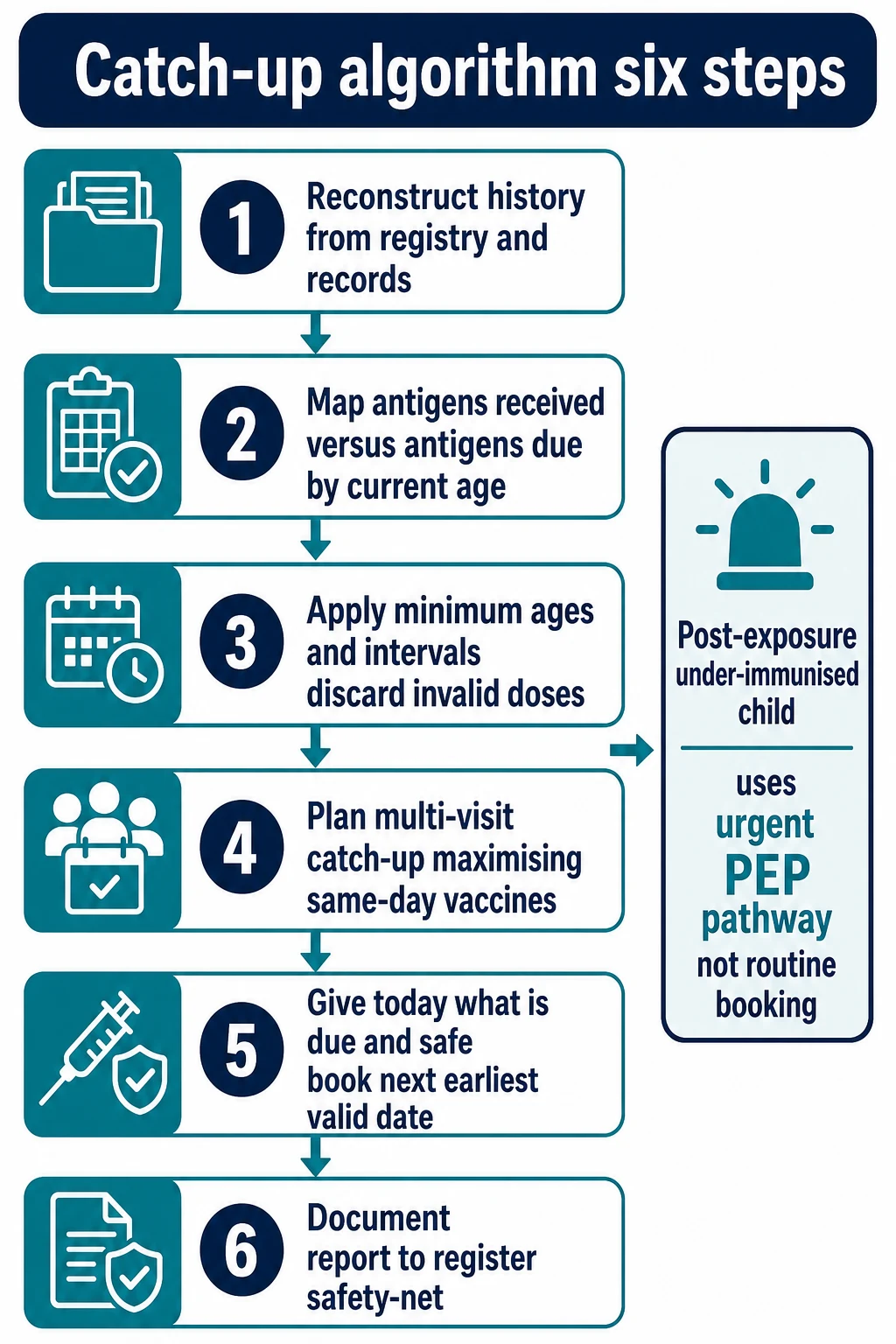
- Reconstruct history. Registry, clinic notes, parent-held records, translated overseas cards.
- Map antigens. List what is already valid for the child’s current age against the current national schedule.
- Apply validity rules. Discard doses given before minimum age or before minimum interval. Do not restart a series that already has valid doses. [1] [3]
- Plan visits. Maximise same-day vaccines. Use combination products when age-appropriate to cut visits. Separate live injectables by ≥4 weeks if not given together. [1]
- Give today. Administer every due, safe vaccine at this encounter unless a true contraindication or precaution blocks it. Book the next earliest valid date before the family leaves.
- Document and report. Write the plan, report doses to the national register, and safety-net missed appointments. [7]
Product age bands matter. Young children need higher-dose diphtheria and pertussis components in DTaP-containing vaccines; older children and adolescents use Tdap formulations per local handbook. Getting the age band wrong is a classic invalid-dose error. [10]
Specific Subtypes & Scenarios
Infant with delayed primary series. Start now. Use minimum intervals from the handbook. Do not wait until the next well-child birthday. Watch age limits for vaccines such as rotavirus, which have maximum starting and finishing ages that vary by product and country. [1] [2]
Toddler with a foreign schedule. Translate antigen content, not brand marketing names. Count valid doses, then fill NIP/ACIP/Green Book/NACI gaps. [4] [5]
School-age child missing second MMR. Close measles protection promptly, especially before school entry or travel. Same-day inactivated vaccines can ride along. [1] [2]
Adolescent catch-up. HPV, meningococcal, Tdap, and any missed childhood antigens. Use school and sports form moments as opportunistic catch-up visits. [2] [10]
No documents at all. After registry search and safety screen, give age-appropriate catch-up rather than indefinite delay for serology. Extra doses of many vaccines are preferable to leaving a child unprotected. [1] [4]
Incomplete hepatitis B series. Continue the series; do not automatically restart. Use serology in the special situations your handbook defines, such as infants of mothers with hepatitis B or immunocompromised hosts. [6]
Immunocompromised child. Prefer inactivated vaccines when live vaccines are contraindicated. Protect household contacts. Coordinate with the treating specialist before live products. [1]
Complications & Pitfalls
Restarting a whole series when valid doses exist wastes visits and trust. Counting invalid early doses creates false completion. Spacing live injectables at two weeks instead of same-day or ≥4 weeks is a classic error. Waiting months for “perfect serology” leaves susceptibility open. Losing the family after “come back sometime” is a system failure — book the next date today. Using Tdap in a toddler who needs DTaP-containing vaccine is a product-band mistake. Forgetting register reporting breaks the next clinician’s history. [1] [3] [7] [10]
Prognosis & Disposition
Timely catch-up closes personal and community susceptibility windows. Disposition is a written multi-visit plan with exact return dates, not a vague promise. Provide school or childcare certificates when complete. Teach caregivers which mild reactions are expected and which need urgent review. [2] [8]
Special Populations
Migrant, refugee, asylum-seeking, and internationally adopted children need catch-up as core care, with interpreters and trauma-aware communication. [4] [5] [9] Indigenous children and remote communities need opportunistic vaccination and culturally safe services. Children in out-of-home care often have fragmented records — assume gaps until proven otherwise. Adolescents need confidential sexual-health-aware counselling before live vaccines when pregnancy is possible. Children with medical complexity need care coordination so “specialist clinics” do not become an excuse for perpetual delay of routine antigens. [4] [8]
Evidence, Guidelines & Regional Differences
ACIP general recommendations define timing, spacing, simultaneous administration, and the approach to uncertain history. [1] The current ACIP child and adolescent schedule is the US operational calendar against which catch-up tables are built. [2] Invalid-dose studies show how often early or short-interval doses fail validity rules in real programmes. [3] Immigrant and refugee frameworks stress structured catch-up rather than assumption of immunity. [4] [5] [9] Australian register tools and coverage reports show how systems close residual gaps. [7] [8] Hepatitis B and diphtheria-tetanus-pertussis product guidance illustrate antigen-specific catch-up detail you must pull from the live handbook, not from memory. [6] [10]
Use the Australian Immunisation Handbook catch-up tables and the Australian Immunisation Register. In Aotearoa New Zealand, use the national immunisation schedule and NIR processes. State antigen due lists from the live handbook for the child’s age; do not invent cells. [7] [8]
Use the UKHSA Green Book schedule and incomplete-immunisation algorithms. School-aged catch-up programmes and GP systems differ from NIP branding but share the same validity logic: count valid doses, then complete. [1]
Use ACIP child/adolescent schedules and catch-up tables in the US, and NACI/Canadian Immunization Guide tables in Canada. State and provincial programmes vary for school entry rules — name the local requirement when counselling families. [2] [9]
Exam Pearls
- Never restart a valid series; continue from documented valid doses. [1]
- Invalid if given before minimum age or before minimum interval. [1] [3]
- Two or more inactivated vaccines: same day or any interval, with handbook exceptions. [1]
- Two live injectable vaccines: same day or ≥4 weeks apart. [1]
- Uncertain history after record search: usually vaccinate, do not assume immunity. [1] [4]
- Combination vaccines reduce visit burden when age-appropriate. [2]
- DTaP versus Tdap is an age-band decision, not a synonym. [10]
- Report every dose to the national register. [7]
- Post-exposure under-immunised child is urgent public-health care. [2]
References
- [1]Kroger AT General recommendations on immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports, 2006.PMID 17136024
- [2]Issa AN Advisory Committee on Immunization Practices Recommended Immunization Schedule for Children and Adolescents Aged 18 Years or Younger - United States, 2025. MMWR. Morbidity and mortality weekly report, 2025.PMID 39819853
- [3]Stokley S Evaluation of invalid vaccine doses. American journal of preventive medicine, 2004.PMID 14700710
- [4]Abu-Shamsieh A Pediatric Care for Immigrant, Refugee, and Internationally Adopted Children. Pediatric clinics of North America, 2022.PMID 34794672
- [5]Dvergsdal ET Low Childhood Vaccination Coverage among Ukrainian Refugees in Norway. A Nationwide, Register-Based Cohort Study, 2022-2023. Journal of immigrant and minority health, 2025.PMID 40668470
- [6]Schillie S Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports, 2018.PMID 29939980
- [7]Nyinawingeri A Using the Australian Immunisation Register to support general practices to improve childhood vaccination rates. Australian journal of general practice, 2024.PMID 38437660
- [8]Hull B Annual Immunisation Coverage Report 2023. Communicable diseases intelligence (2018), 2026.PMID 41730159
- [9]Crockett M New faces from faraway places: Immigrant child health in Canada. Paediatrics & child health, 2005.PMID 19668632
- [10]Liang JL Prevention of Pertussis, Tetanus, and Diphtheria with Vaccines in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR. Recommendations and reports : Morbidity and mortality weekly report. Recommendations and reports, 2018.PMID 29702631