Paeds · preventive-and-community-paediatrics
Childcare attendance, exclusion and infection prevention
Also known as Daycare exclusion · ECEC infection control · Child care attendance policies · Return to childcare after illness · Nursery infection prevention · Out-of-home childcare infection
Fellowship-level approach to infection risk in group childcare, evidence-based exclusion and return-to-care decisions, centre infection prevention, outbreak response, special populations, and regional operational guidance differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent phones because the centre sent the toddler home with diarrhoea. Another family asks why their child has had six colds since starting care. A director emails asking whether a child with hand-foot-mouth can return tomorrow. These are core general-paediatrics tasks, not admin side work. [1] [2]
Out-of-home childcare (early childhood education and care, family day care, preschool, nursery) places many young children in prolonged close contact. That setting multiplies ordinary childhood infections. Your job is threefold: keep the seriously unwell child safe, limit unnecessary transmission, and avoid over-exclusion that harms learning, equity and parental employment. [1] [7]
Exclusion means the child stays away from the centre for a defined reason. Return-to-care means the clinical and public-health criteria for re-entry are met. Outbreak means more cases of a linked illness than expected in that setting — thresholds and definitions are public-health decisions. [9] [12]
Classification
Think in three practical buckets when a centre or parent asks “can they come?”. [11]
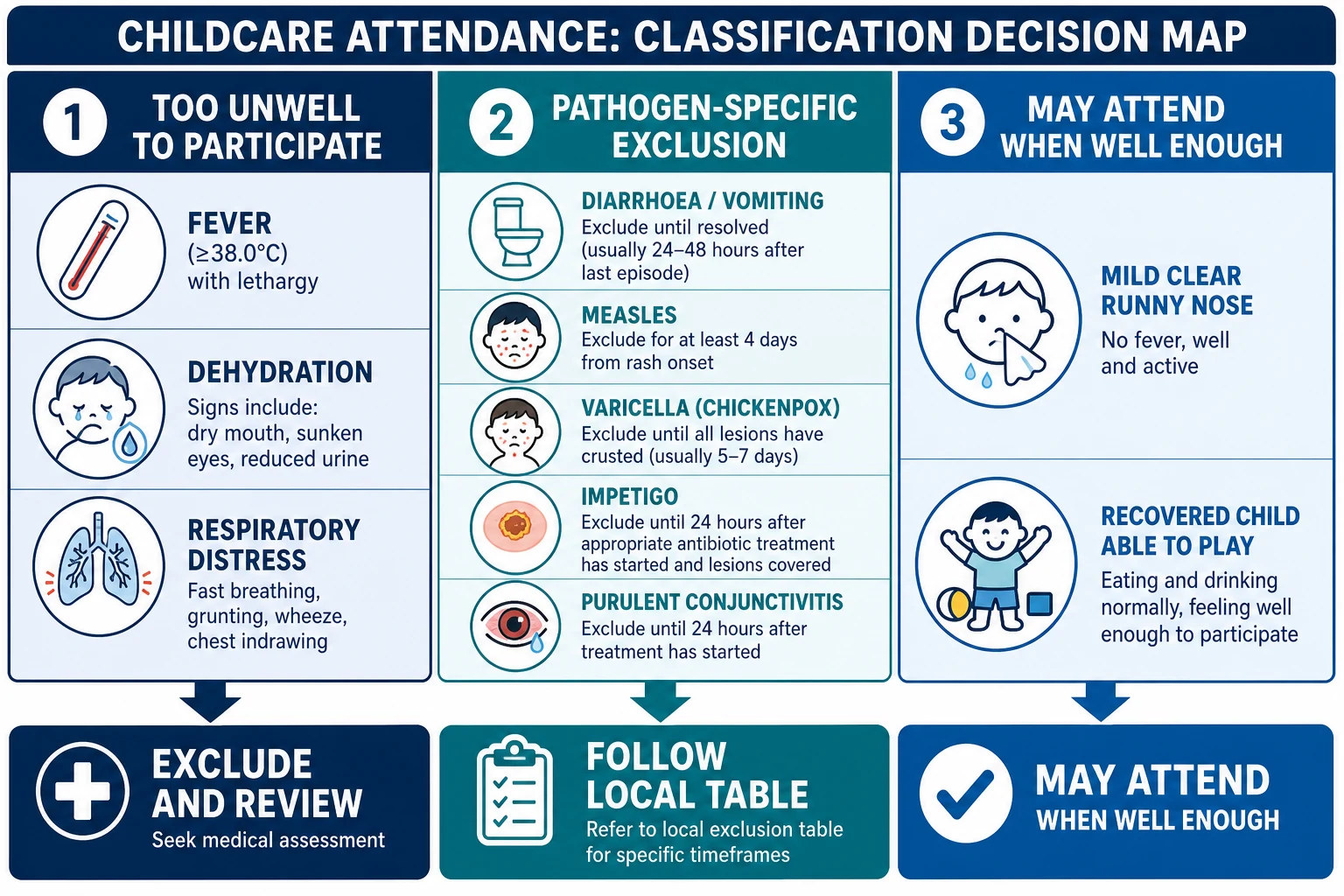
Attendance classes you must not blur
- Lethargy, poor intake, dehydration risk, respiratory distress, uncontrolled fever behaviour
- Exclude and medically assess
- Pathogen label is secondary until stable
- Diarrhoea/vomiting windows, measles, varicella, pertussis, impetigo, purulent conjunctivitis as per local table
- Infectious period may outlast feeling a bit better
- Public health may override centre custom
- Mild clear rhinorrhoea, recovered child who can play and feed
- Colonisation without disease when guidance allows
- Do not invent extra days of exclusion
Also separate colonisation from infection. A child may carry organisms without being the reason for an outbreak policy. Staff and public health decide cohorting and screening — clinicians should not invent surveillance cultures for routine daycare letters. [2]
Epidemiology & Risk Factors
Group care raises the rate of respiratory and gastrointestinal infections, especially in the first years of regular attendance. Longitudinal work shows frequent illness in day care, with the burden most obvious early and often attenuating as children age and acquire immunity. Birth-cohort data link day care with more respiratory and GI infections in early life. [7] [8]
Risk amplifiers include large group size, mixed ages, shared toys and food, incomplete hand hygiene after nappy changes, incomplete immunisation, winter respiratory season, and staff working while infectious. Protective factors include staff and child immunisation, structured hand-hygiene and cleaning programmes, adequate nappy-change hygiene, ventilation and outdoor time, written illness policies, and smaller consistent groups. [1] [2] [6]
Inequity matters. Families with no paid leave, single parents, and out-of-home care placements face harsher consequences from every exclusion day. Over-exclusion of mild illness is not a neutral public-health win. [1]
Pathophysiology
Childcare is a transmission ecology, not a mystery. Young children cough into each other’s faces, put shared toys in their mouths, and need frequent nappy changes. Those facts explain the epidemiology. [2]
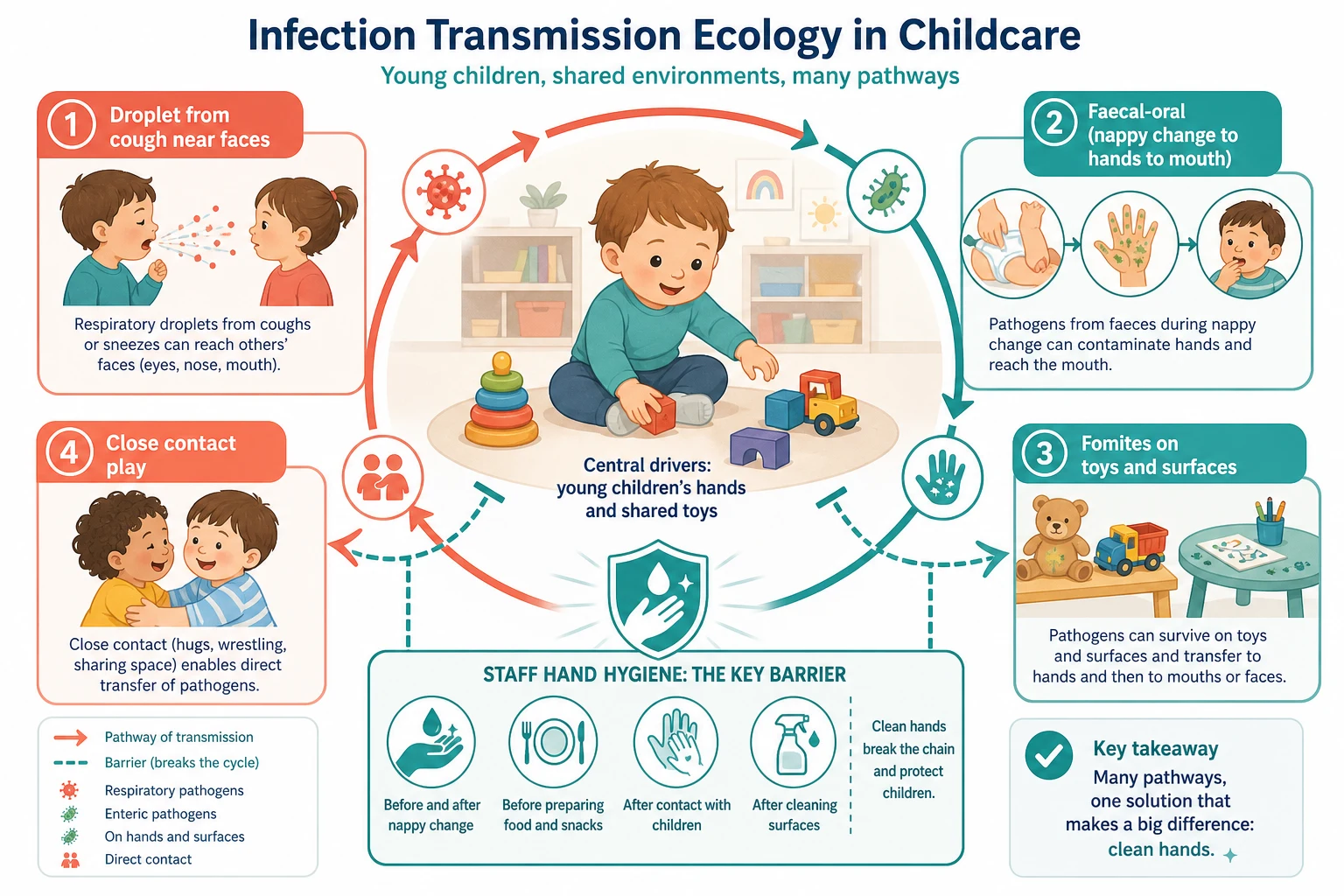
Faecal–oral spread drives many diarrhoeal outbreaks. Norovirus and other enteric pathogens spread efficiently in centres; household secondary cases are common after a childcare index case. Viral shedding can continue after symptoms settle, which is why cleaning and hand hygiene still matter after return. [9] [10] [18]
Respiratory viruses spread by droplets, aerosols and contaminated hands. Skin and eye pathogens (impetigo, conjunctivitis) spread by contact. Blood/body fluid risks are lower day-to-day but still drive standard precautions for staff. [2]
CMV and parvovirus B19 deserve special mention for pregnant contacts. Toddlers can shed CMV in urine and saliva for prolonged periods. That is a staff hygiene and occupational-health issue — not a reason to exclude every asymptomatic toddler who might shed CMV. [14] [15] [16]
Clinical Presentation
Most presentations are ordinary: clear or coloured rhinorrhoea, cough, fever, loose stools, vomiting, red eye, mouth ulcers with hand/foot spots, honey-crusted sores, or head lice. The centre’s presentation is often a letter, a phone call, or a parent under work pressure. [2] [7]
Ask what the centre actually said. Policies vary. Some letters over-exclude. Some under-exclude during gastroenteritis clusters. Translate the letter into a clinical assessment: Is the child well enough to play, feed and be cared for safely? What syndrome is this? Is there an outbreak notice? [11] [12]
Red-flag presentations are not “daycare problems”. Petechiae or purpura, stiff neck, continuous vomiting with lethargy, severe work of breathing, seizures, or a child who cannot be roused need emergency care. Do not spend the first ten minutes negotiating return dates. [2]
Staff may present with repeated exposures or pregnancy concerns after a parvovirus or CMV discussion at work. Treat those as occupational and obstetric-risk conversations with accurate hygiene advice. [15] [16]
Differential Diagnosis
Start with the cannot-miss list, then the common list. [2]
| Pattern | More likely mild centre illness | Do not miss |
|---|---|---|
| Fever + coryza | Viral URTI | Sepsis, pneumonia, UTI in infants, influenza with complications |
| Vomiting/diarrhoea | Viral AGE | Surgical abdomen, severe dehydration, foodborne outbreak needing public health |
| Red eye | Viral/allergic conjunctivitis | Periorbital cellulitis, gonococcal/chlamydial in neonates, severe pain/photophobia |
| Rash | Viral exanthem, HFMD, mild eczema flare | Meningococcal disease, measles, varicella in high-risk contact, eczema herpeticum |
| Skin sores | Impetigo | Staph scalded skin, necrotising infection, scabies clusters |
Vaccine-preventable diseases (measles, pertussis, varicella, influenza) change the whole response: notification, contact tracing, and exclusion of unprotected contacts. A “viral rash” in an under-immunised cohort is not a routine HFMD conversation until measles is off the table. [11] [12]
Clinical & Bedside Assessment
Use a short structured script. [11]
Five-minute childcare illness assessment
Severity first
Appearance, work of breathing, hydration, alertness, fever behaviour, ability to drink and play.
Syndrome
Respiratory, GI, eye, rash, skin, lice, mouth/HFMD — name the pattern in plain language.
Participation test
Could staff provide care without one-to-one nursing? Can the child join usual activities?
Context
Centre outbreak notice, immunisation status, high-risk household contacts, pregnant staff concerns.
Local rule
Map to NHMRC / UKHSA / CFOC-state table; do not invent days. Document advice and safety-net.
Examine when the story suggests more than a mild viral illness, when you will write a medical certificate, or when red flags appear. For pure policy questions about a well child who already recovered at home, you still need enough history to avoid rubber-stamping unsafe return. [12]
Assess family capacity. “Stay home until 48 hours after the last vomit” is only workable if someone can provide care. Offer practical planning without blaming poverty or work constraints. [1]
Investigations
Most mild childcare-associated illness needs no test. History and examination decide exclusion and home care. Ordering a multiplex panel so a parent can “prove” a virus to a centre is not good practice. [2]
Investigate when the child is severely unwell or hospitalised; a vaccine-preventable disease is suspected; public health requests testing in an outbreak; atypical features suggest a non-viral diagnosis; or results will change treatment or exclusion in a defined way (for example influenza in a high-risk child where antivirals are considered under local rules). [9] [10] [12]
Stool studies, respiratory PCR/antigen, rapid strep testing, and serology for specific exposures are tools — not default daycare paperwork. For pregnant staff worried about CMV or parvovirus, occupational health and obstetric pathways guide adult testing; do not turn every toddler into a surveillance subject. [14] [15]
Management — Resuscitation
If the child is critically unwell, ignore the exclusion debate. Open the airway, support breathing and circulation, check glucose, treat shock, and use local paediatric emergency pathways. Notify seniors early. [2]
For suspected meningococcal disease, measles, or other high-consequence notifiable infections, treat the patient and notify public health without waiting for perfect laboratory confirmation when clinical suspicion is high. Protect exposed high-risk contacts as directed by public health. [11] [12]
Centre paperwork never delays oxygen, fluids or antibiotics when indicated. [2]
Management — Definitive & Stepwise
Prevention and clear return rules are the definitive work for almost every consultation on this topic. [1] [6]
Step 1 — Daily infection prevention (every centre, every day)
Hand hygiene after toileting and nappy change, and before food handling, is the intervention with the strongest practical evidence base in childcare trials and broader diarrhoea-prevention reviews. Surface cleaning of mouthed toys, safe food handling, respiratory etiquette, and up-to-date immunisation for children and staff complete the package. [3] [4] [5] [6] [13]
Randomised and open-trial work in childcare settings has shown that structured infection-control programmes can reduce diarrhoeal episodes and influence respiratory illness patterns. Results vary by adherence, but the direction of effect supports programme quality over fatalism. [4] [5] [6]
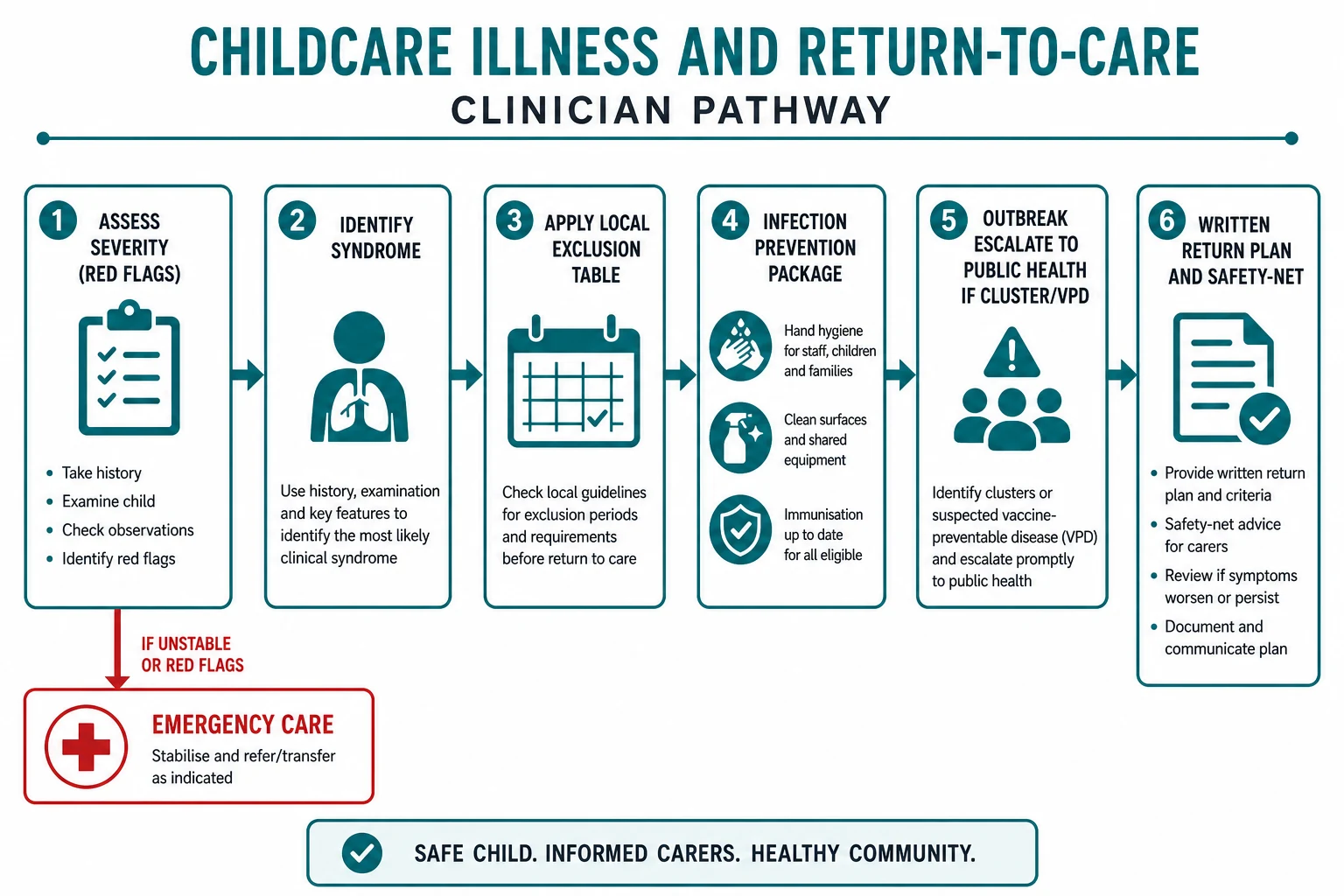
Step 2 — Severity and participation rule
If the child cannot join usual activities, is in pain, needs frequent one-to-one care, or has uncontrolled symptoms, they stay home — even if a pathogen table would allow return for a well child with the same label. [11]
Step 3 — Syndrome-linked exclusion principles
Exact day counts are jurisdiction-specific. Teach principles, then open the local table (NHMRC Staying Healthy in Australia; UKHSA education/childcare guidance in the UK; CFOC plus state/local health rules in the US). [11] [12]
Common principle patterns (confirm locally before quoting a number in a letter): exclude while diarrhoea/vomiting are present and follow the local symptom-free interval (often framed as about 24–48 hours); exclude while febrile and unwell; return with HFMD or mild viral rash when well enough to participate if no local restriction; follow local wording for purulent conjunctivitis and impetigo; exclude varicella until lesions crust (classic principle); use pathogen-specific windows and public-health direction for measles/pertussis; treat head lice per current local education-setting advice rather than old myths. [9] [11] [12]
Step 4 — Outbreak response
When a centre reports a cluster (classic example: norovirus-like illness), support a public-health style response: case definition, line list, enhanced cleaning, hand hygiene reinforcement, cohorting if advised, temporary broader exclusion if directed, and clear family communication. Australian childcare norovirus investigations show household spread after centre exposure — counsel families about home hygiene too. [9] [10]
Step 5 — Certificates and communication
Write what is true: diagnosis impression, date last symptomatic, advice given, and the local criterion used. Do not invent negative tests. Do not prescribe antibiotics solely to “clear” a child for daycare when bacterial treatment is not indicated. [2]
Step 6 — Immunisation as structural prevention
High coverage reduces the chance that a centre introduction of measles, varicella, pertussis, influenza or other VPDs becomes a large outbreak. Catch-up incomplete schedules when you see care-entry forms. [1]
COVID-era strategies such as test-to-stay were studied in daycare contexts; they are pathogen- and policy-era specific, not a universal template for all illnesses. [17]
Specific Subtypes & Scenarios
Toddler with “constant colds” after starting care. Explain expected early excess infections, red flags for when to review, hand hygiene at home, smoke-free care, and immunisation. Do not start an immune work-up for ordinary first-year daycare frequency alone. [7] [8]
Norovirus/AGE outbreak. Symptom-based exclusion, strict hand hygiene, environmental cleaning, public-health notification when thresholds met, and household secondary-case counselling. [9] [10]
HFMD. Focus on hydration, pain control, participation, and avoiding unnecessary prolonged exclusion beyond local guidance. [11] [12]
Suspected measles or pertussis in a centre. Isolate from the waiting room strategy in clinic, urgent public health, immunisation review of contacts, and post-exposure pathways for eligible people. [11] [12]
Impetigo. Treat appropriately, cover lesions when advised, and use the local return rule — not indefinite exclusion. [11] [12]
Incomplete immunisation during a VPD outbreak. Align with public-health exclusion of susceptible contacts; offer catch-up urgently. [1]
Immunocompromised classmate. Individualise with oncology/immunology and public health; a “mild” varicella exposure is not mild for them. [1] [11]
Pregnant educator. Emphasise hand hygiene after nappy care and saliva contact; discuss CMV/parvovirus occupational risk honestly; involve occupational health. Do not exclude healthy CMV-excreting toddlers as policy. [14] [15] [16]
Rural centre. Telehealth can triage mild illness; still use local public-health contacts for outbreaks; written plain-language plans help when the GP is hours away. [1] [9]
Complications & Pitfalls
Complications of poor practice include preventable outbreaks, delayed care for the seriously unwell child, unnecessary antibiotic resistance pressure, and loss of childcare places for families already under strain. [1] [4]
Prognosis & Disposition
Most childcare-associated illnesses are self-limited. Many children experience a high frequency of viral infections in the first period of regular group care, then fewer disruptive episodes as they grow. [7] [8]
Disposition: home until severity and local exclusion criteria clear, with clear safety-net advice; primary care review if symptoms persist, worsen, or the diagnosis is uncertain; ED/urgent care for red flags; public health pathway for outbreaks and notifiable diseases. [9] [12]
Give a written or explicitly stated return plan: what must stop (vomiting, free stools, fever), what “well enough to participate” looks like, and when to come back earlier. [11] [12]
Special Populations
Young infants have fewer vaccines completed and less physiological reserve — lower threshold for medical review. [2]
Immunocompromised children need personalised exposure plans; centres should know whom to call without breaching privacy beyond need-to-know. [1]
Medical complexity / technology dependence may need care plans that address suction, feeds and aerosol-generating procedures in the centre, plus clearer exclusion when baseline is fragile. [1]
Indigenous and socioeconomically disadvantaged families may have fewer leave options and higher baseline infection burden — advocate for fair policies and support, not blame. [1]
Migrant and refugee families may face language barriers and incomplete immunisation records — use interpreters and catch-up pathways. [1]
Out-of-home care multiplies carers and transport logistics; put return rules in writing for every carer. [1]
Disability / neurodiversity can make hygiene independence and participation assessments nuanced — exclude for true infectious risk and care needs, not for difference itself. [1]
Pregnant staff and household members need CMV/parvovirus hygiene counselling and occupational pathways. [14] [15] [16]
Evidence, Guidelines & Regional Differences
Trials and epidemiology. Black’s classic day-care handwashing work and later childcare infection-control trials (Roberts diarrhoea and respiratory RCTs; Uhari open RCT) support structured hygiene programmes. Wald’s follow-up and Zutavern’s cohort data describe the real infection burden of day care. [3] [4] [5] [6] [7] [8]
Exclusion evidence base. Richardson and Czumbel synthesise incubation and infectiousness data that underpin school and childcare exclusion tables — useful when defending why tables exist, not a licence to invent days. [11] [12]
Outbreak literature. Mattison’s US childcare/school AGE outbreak analysis and Australian norovirus childcare investigations show how quickly enteric pathogens move through centres and homes. [9] [10]
Regional operational sources (use the current local edition in practice): Australia/NZ NHMRC Staying Healthy plus state public health; UK UKHSA education/childcare health-protection guidance; US AAP quality childcare policy plus CFOC and state rules; Canada provincial exclusion schedules. Always quote the current local table. [1] [11] [12]
| Region | Operational anchor | Clinician habit |
|---|---|---|
| Australia / NZ | NHMRC Staying Healthy (ECEC) + state/territory public health | Quote table + notify as required |
| United Kingdom | UKHSA health protection in education/childcare settings | Align certificates with UKHSA periods |
| United States | AAP quality childcare policy + CFOC standards + state health dept | State rules can differ — check |
| Canada | Provincial public health exclusion schedules | Provincial table wins |
Controversies. How aggressively to exclude mild respiratory illness; role of routine viral testing; COVID-era test-to-stay models; and balancing equity against transmission control. Evidence supports hygiene programmes more strongly than maximalist exclusion of every runny nose. [5] [13] [17]
Exam Pearls
Viva stem pattern: “Centre says the child needs a clearance letter after diarrhoea — what do you do?” Answer: assess severity and hydration, confirm last symptom time, open local table, give hygiene advice, document, safety-net. OSCE pattern: angry parent who must work tomorrow — partner, explain transmission, problem-solve care, do not invent a false clearance. [10] [12]
References
- [1]Donoghue EA Quality Early Education and Child Care From Birth to Kindergarten. Pediatrics, 2017.PMID 28771418
- [2]Nesti MM Infectious diseases and daycare and preschool education. Jornal de pediatria, 2007.PMID 17632670
- [3]Black RE Handwashing to prevent diarrhea in day-care centers. American journal of epidemiology, 1981.PMID 7211827
- [4]Roberts L Effect of infection control measures on the frequency of diarrheal episodes in child care: a randomized, controlled trial. Pediatrics, 2000.PMID 10742314
- [5]Roberts L Effect of infection control measures on the frequency of upper respiratory infection in child care: a randomized, controlled trial. Pediatrics, 2000.PMID 10742313
- [6]Uhari M An open randomized controlled trial of infection prevention in child day-care centers. The Pediatric infectious disease journal, 1999.PMID 10462334
- [7]Wald ER Frequency and severity of infections in day care: three-year follow-up. The Journal of pediatrics, 1991.PMID 2007922
- [8]Zutavern A Day care in relation to respiratory-tract and gastrointestinal infections in a German birth cohort study. Acta paediatrica (Oslo, Norway : 1992), 2007.PMID 17666100
- [9]Mattison CP Childcare and School Acute Gastroenteritis Outbreaks: 2009-2020. Pediatrics, 2022.PMID 36278284
- [10]Schulz C Outbreak investigation of norovirus gastroenteritis in a childcare facility in Central Queensland, Australia: a household level case series analysis. Communicable diseases intelligence (2018), 2024.PMID 39165020
- [11]Richardson M Evidence base of incubation periods, periods of infectiousness and exclusion policies for the control of communicable diseases in schools and preschools. The Pediatric infectious disease journal, 2001.PMID 11332662
- [12]Czumbel I Management and control of communicable diseases in schools and other child care settings: systematic review on the incubation period and period of infectiousness. BMC infectious diseases, 2018.PMID 29716545
- [13]Ejemot-Nwadiaro RI Hand-washing promotion for preventing diarrhoea. The Cochrane database of systematic reviews, 2021.PMID 33539552
- [14]Dobbins JG The risks and benefits of cytomegalovirus transmission in child day care. Pediatrics, 1994.PMID 7971042
- [15]Pass RF Day-care centers and the spread of cytomegalovirus and parvovirus B19. Pediatric annals, 1991.PMID 1658718
- [16]Pass RF Increased rate of cytomegalovirus infection among day care center workers. The Pediatric infectious disease journal, 1990.PMID 1973533
- [17]Dewald F SARS-CoV-2 Test-to-Stay in Daycare. Pediatrics, 2024.PMID 38596855
- [18]Steimle LN Cost-effectiveness of pediatric norovirus vaccination in daycare settings. Vaccine, 2021.PMID 33741192