Paeds · preventive-and-community-paediatrics
Climate change, heat and child health
Also known as Heat illness children · Heat stroke paediatrics · Climate change child health · Exertional heat stroke · Heat wave paediatric morbidity · Paediatric thermoregulation heat
Fellowship-level approach to climate-driven heat risk in children: thermoregulation, heat-illness spectrum, cool-first resuscitation, sports and school prevention, equity, and multi-board anticipatory guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A coach calls from the sideline: a 15-year-old collapsed in the first week of preseason training. The air is humid. The child is confused. That is not “just dehydration.” That is heat stroke until you prove otherwise, and the clock is running on brain and organ injury. [6] [7]
Climate change raises the frequency and intensity of heat extremes and stacks other child-health threats on top — worse air quality days, wildfire smoke, shifting infections, food and housing stress, and disaster displacement. The American Academy of Pediatrics (AAP) frames this as a paediatric emergency across the life course, from fetal life through adolescence. [1] [2] [3] [4]
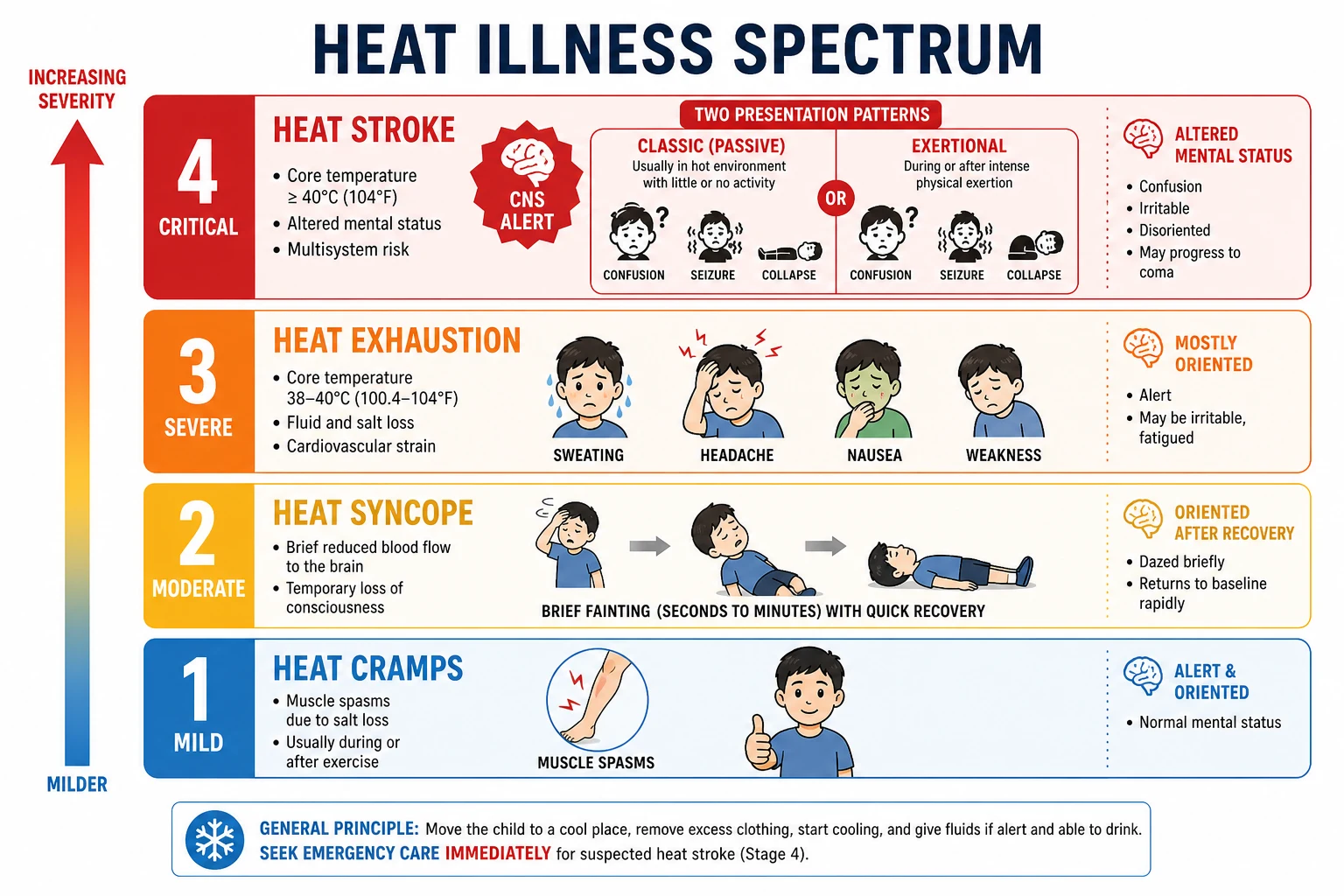
Heat illness is the clinical spectrum of body-temperature stress: cramps, heat syncope, heat exhaustion and heat stroke. Heat stroke is the emergency end: hyperthermia plus central nervous system dysfunction after heat exposure or exertion. You treat the syndrome, not a single thermometer reading in isolation. [6]
This page teaches the bedside ladder, the cool-first algorithm, and the preventive and advocacy work that keeps the next child off that ladder. [5] [13]
Classification
Separate climate pathways, heat-illness severity, and classic versus exertional heat stroke. Mixing them confuses exams and teams. [1] [6]
Climate-related child-health pathways (AAP framing) include extreme heat, air pollution and aeroallergens, vector- and water-borne disease shifts, food insecurity, mental health after disasters, and inequitable housing or displacement. Heat is the sharp clinical edge of that wider map. [1] [3] [13]
| Category | What you see | Urgency |
|---|---|---|
| Heat cramps | Painful muscle spasms after sweat loss | Rest, cool environment, oral sodium-containing fluids if alert |
| Heat syncope | Brief faint after standing or stopping hard work in heat | Lie flat, cool, reassess for injury and cardiac red flags |
| Heat exhaustion | Heavy sweat, headache, nausea, weakness; mentation mostly preserved | Remove from heat, cool, hydrate; escalate if any CNS change |
| Heat stroke | Hyperthermia + altered mental status, seizure, combativeness or coma | Emergency cooling + resuscitation |
Classic (passive) heat stroke hits infants, disabled children and people trapped in hot rooms or cars without heavy exercise. Exertional heat stroke hits athletes and outdoor workers who generate huge heat loads; skin may still be wet with sweat. Sweating does not rule out heat stroke. [6] [7]
Environmental metrics such as heat index and wet-bulb globe temperature (WBGT) help sports and school policies set work-to-rest ratios. You do not need to calculate WBGT on every ED shift, but you should know that humidity blocks evaporative cooling and that policy uses environmental thresholds. [5]
Epidemiology & Risk Factors
Ambient heat and heat waves are linked with higher paediatric emergency and acute-care use, including respiratory, infectious and heat-specific presentations. Systematic and scoping reviews of ambient temperature and extreme heat show consistent morbidity signals in children, with vulnerability concentrated at younger ages and in high-exposure settings. [8] [9] [11] [16]
Who is at highest risk? [5] [10] [12]
- Infants and young children who cannot move to shade, undress or ask for water.
- Adolescent athletes in preseason, especially American football, rugby, endurance running and multi-session days.
- Obesity, cardiac disease, cystic fibrosis, poorly controlled diabetes, epilepsy and acute febrile illness.
- Medications that impair sweating or raise heat production (for example anticholinergics, some stimulants — review the child’s list).
- Neurodevelopmental disability, limited communication, or fixed outdoor programmes.
- Housing without cooling, urban heat islands, remote travel, outdoor work for older teens.
- Families with low income, language barriers, or recent migration into a hotter climate.
Equity is not an optional paragraph. Climate harm lands hardest on children already facing disadvantage, including many Indigenous and remote communities and those in poorly cooled rental housing. [12] [3]
Pathophysiology
Children are not small adults with the same heat budget. Relative to body mass they often have a larger surface area, which can increase heat gain from a hot environment. Sweating and cardiac output responses are still developing. Young children depend on adults for fluids, clothing and escape from heat. [10]
Heat balance is simple on paper: heat production (basal metabolism + exercise) minus heat loss (radiation, convection, conduction, evaporation). When air is hotter than skin, radiation and convection can reverse and add heat. High humidity blocks sweat evaporation — the main cooling route during exercise. Core temperature then climbs. [6] [10]
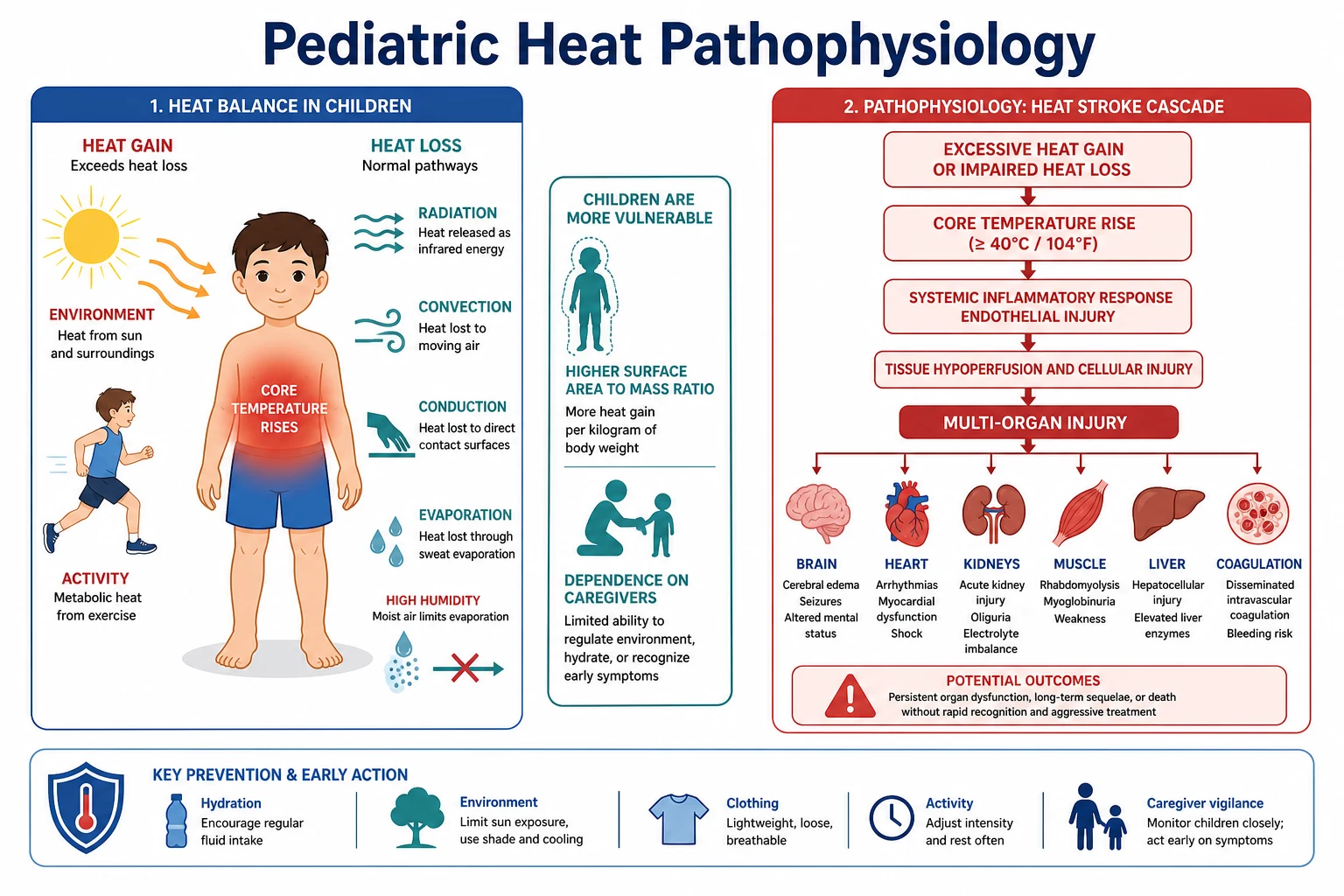
In heat stroke, high core temperature and a systemic inflammatory response damage brain, heart, liver, kidney, muscle and clotting. Rhabdomyolysis, acute kidney injury, disseminated intravascular coagulation and arrhythmia can follow. Time spent critically hot drives outcome — which is why field cooling exists. [6] [7]
Children with congenital or acquired heart disease face a dangerous convergence: limited cardiac reserve, medications, and heat stress on top of exercise. Modify plans early rather than waiting for collapse. [15]
Perinatal heat stress is part of the same climate story: maternal heat exposure links to adverse pregnancy and neonatal outcomes in emerging evidence syntheses. Counsel pregnant adolescents and new parents on cooling access and hydration during heat waves. [14]
Clinical Presentation
Prevention visits dominate volume. Families ask about sports camp, school sports days, or a heat-wave warning. Give a concrete plan: fluids, shade, clothing, activity cuts, medication review, and vehicle safety. [5] [3]
Heat exhaustion looks like a “wiped-out” child after outdoor play: pale or flushed, sweaty, nauseated, headache, thirsty, tired, sometimes dizzy. Mentation is mostly intact. They improve with rest in a cool place and oral fluids if they can drink. [5]
Heat stroke looks like an emergency: confusion, aggression, seizure, ataxia, or unresponsiveness. Temperature is typically very high when measured with a reliable core method, but do not delay cooling while hunting a perfect reading if the clinical picture is clear. Skin may be hot and dry or still sweaty in exertional cases. [6] [7]
- Infant: hot car, overbundling, poorly ventilated room during a heat wave. [8]
- Toddler/preschool: all-day outdoor event without shade or drinks. [5]
- School-age: sports carnival at midday. [5]
- Adolescent: two-a-day practices, weight-cutting myths, or stimulant misuse plus heat. [5]
Co-travel problems are common: sunburn, asthma flares on hot smoky days, and gastroenteritis that tips a child into heat-related dehydration. [11] [13]
Differential Diagnosis
Collapse in heat is not always heat stroke. Run the short list while you cool if heat stroke remains likely. [6]
- Sepsis or meningitis — fever and altered mental status without a clear heat story, or sick contacts and rash.
- Head injury from the fall itself.
- Hypoglycaemia — check glucose early in every collapsed child.
- Hyponatraemia from large volumes of free water without sodium during endurance events (can coexist with heat stress).
- Cardiac syncope or arrhythmia, especially with exertional onset and known heart disease. [15]
- Toxic ingestion, seizure disorder, anaphylaxis.
- Malignant hyperthermia or neuroleptic malignant syndrome when history fits drugs or anaesthesia — rare but exam-favourite mimics.
The practical discriminator for heat illness severity is CNS function. Normal mentation with fatigue and sweat points to exhaustion; clear CNS failure points to stroke-level care. [6]
Clinical & Bedside Assessment
Start with scene safety and remove the child from the heat source. Strip excess clothing and gear. Do a rapid ABCDE with a focused neuro check. [7]
History that changes management [5] [7]
- How long outdoors or in a car? Activity intensity?
- Fluids: what, how much, any salt-containing drinks?
- First days of heat season (poor acclimatisation)?
- Chronic disease, cardiac history, disability?
- Medicines and recent illness?
- Witnessed seizure, head strike, or chest pain?
Exam priorities: mental status, airway protection, work of breathing, perfusion, glucose, skin findings, muscle tenderness, trauma from collapse. Measure temperature with the best available method; rectal/core is preferred when feasible for heat stroke monitoring. [6] [7]
For preventive visits, audit the real plan: school policy, coach education, shade, water access, and whether anyone would start immersion cooling on site. [5]
Five-minute heat assessment
Threat and removal
Get out of sun/car/kit; strip excess clothing.
CNS and ABC
Confusion, seizure, airway, breathing, circulation, glucose.
Heat story
Exertion vs passive heat, humidity, duration, fluids.
Risk filters
Age, cardiac disease, obesity, disability, drugs.
Cooling decision
If heat stroke likely, start aggressive cooling now.
Prevention close
If well visit, leave a written heat-day plan.
Investigations
Do not delay cooling for blood tests or CT when heat stroke is the working diagnosis. [6] [7]
Once cooling is under way, typical hospital workup includes bedside glucose, electrolytes, renal function, creatine kinase, liver enzymes, coagulation, blood gas, and ECG as indicated. Image for trauma or alternative diagnoses when the story is incomplete. Mild heat exhaustion that resolves quickly often needs no labs. Prevention counselling needs none. [6]
Document peak temperature if known, cooling method, and time course — that record matters for sports clearance and for learning system failures. [7]
Management — Resuscitation
Heat stroke is a time-critical cooling emergency. The organ that fails first is often the brain you are watching. [6]
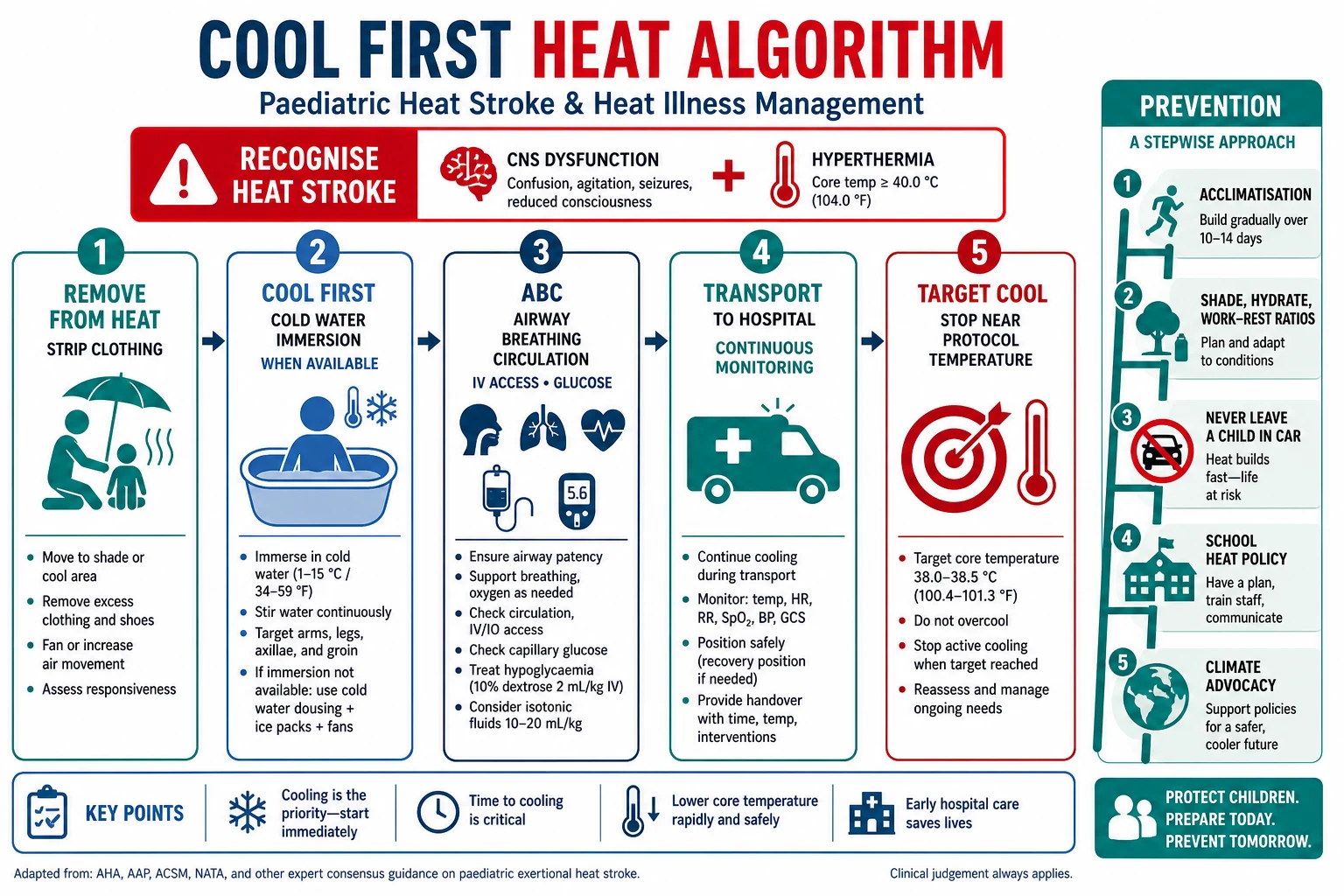
- Recognise heat stroke (heat exposure/exertion + CNS dysfunction).
- Call for help; remove from heat; strip clothing and equipment.
- Cool first. For exertional heat stroke, cold-water immersion (whole-body when feasible) is the preferred prehospital method when a tub or equivalent is available. If immersion is impossible, use continuous cold-water dousing, ice towels rotated rapidly, and ice packs over large vessels while arranging transfer — do not substitute weak fanning alone for true heat stroke.
- Protect airway if consciousness is reduced; give oxygen as needed; treat seizures with standard paediatric algorithms.
- IV access; correct hypoglycaemia; use isotonic fluids for hypovolaemia guided by perfusion — avoid reckless free-water overload.
- Continuous monitoring; stop aggressive cooling near local target (commonly discussed near ~38.5–39 °C in sports-medicine protocols — follow your service protocol to avoid overshoot). [7]
- Transport to a facility that can manage multi-organ complications; continue cooling en route if still critically hot.
Classic infant heat stroke uses the same principle — remove heat and cool aggressively — while preparing for airway support and ICU-level care. [6]
Management — Definitive & Stepwise
After heat exhaustion: cool environment, oral rehydration if alert, observation until normal, written safety-net for relapse, and a plan that cuts the next day’s heat load. [5]
After heat stroke: hospital monitoring for organ injury; ICU when CNS, renal, hepatic, clotting or cardiac complications persist. Return-to-play needs medical clearance, a period free of symptoms, and a graded programme — not the next game. [5] [7]
Prevention ladder (clinic language) [5] [3]
- Hydration culture: scheduled drinks; free water access at sport and school; caution against “no water until the end.”
- Acclimatisation: progressive heat exposure over about 10–14 days at the start of a hot season for sports.
- Modify work and rest with heat and humidity; cancel or move events when conditions are extreme per local policy.
- Clothing and shade: light breathable kit, shade structures, indoor alternatives.
- Never leave a child in a vehicle — even briefly. Teach every caregiver.
- Chronic disease action plans and medication review before summer.
- Home cooling access: fans, cool rooms, community cooling centres, welfare checks for vulnerable households.
- Climate health counselling: smoke days, disaster readiness, and advocacy for school and city cooling policy. [1] [12]
Heat exhaustion versus heat stroke — what you do
- Mentation mostly preserved
- Remove heat, rest, oral fluids if safe
- Escalate if any CNS change
- CNS dysfunction present
- Cold-water immersion when possible
- ABC + hospital/ICU pathway
- Acclimatise and hydrate
- School/sport policy
- Vehicle and equity check
Specific Subtypes & Scenarios
Hot car / passive infant: treat as classic heat stroke pathway; safeguarding and caregiver education after stabilisation; ask about sleep practices and supervision without delaying care. [8]
Preseason football or rugby: highest classic exam scenario for exertional heat stroke; immersion plan must exist before the season. [5] [7]
Cardiac disease: lower threshold to cancel outdoor exertion on extreme days; coordinate with cardiology exercise advice. [15]
Disability and residential care: fixed outdoor schedules, communication barriers, and polypharmacy need written heat protocols. [12]
Rural/remote carnival: no immersion tub? Pre-plan tarpaulins, ice, water supply and retrieval; cool during transport. [7]
Heat wave ED surge: expect dehydration, asthma, heat illness and stressed caregivers; stream pathways and public messaging. [11] [16]
Smoke plus heat: dual exposure worsens respiratory illness; indoor clean-air and cooling plans together. [13]
Complications & Pitfalls
- Delaying cooling for imaging.
- Assuming “still sweating = not heat stroke.”
- Missing hyponatraemia in the endurance athlete who drank only water.
- Early return to full heat load after illness.
- Shaming families without air-conditioning instead of linking practical supports.
- Treating only the acute episode and never writing a prevention plan.
- Ignoring climate equity and school policy as “not medical.” [6] [7] [12]
Prognosis & Disposition
Outcome after heat stroke tracks duration and severity of hyperthermia and multi-organ injury. Early effective cooling improves the chance of full recovery; delayed cooling raises death and disability risk. [6] [7]
- Mild heat exhaustion, normal mentation, good intake, reliable caregivers → home with written plan.
- Any residual CNS abnormality, organ lab abnormalities, or uncertain diagnosis → admit; PICU if unstable.
- Sports clearance only after medical review and graded return.
- Public-health layer: heat alerts, event cancellation, cooling centres. [5] [8]
Special Populations
Infants need caregiver-dependent prevention. Adolescents need autonomy-respecting counselling that still bans dangerous heat practices. Indigenous and remote families need culturally safe, practical cooling and transport plans. Migrant families new to extreme heat need explicit education. Out-of-home care needs multi-caregiver consistency. Cardiac and technology-dependent children need individualised plans. [12] [15] [3]
Evidence, Guidelines & Regional Differences
- AAP 2015 policy and technical report on global climate change and children’s health. [1] [2]
- AAP 2024 policy and technical update building a healthy climate future for children. [3] [4]
- AAP 2011 climatic heat stress policy for exercising children and adolescents (acclimatisation, hydration, event modification). [5]
- Bouchama NEJM heat stroke review for pathophysiology and cooling principles. [6]
- Prehospital exertional heat stroke roundtable emphasising cold-water immersion and cool-first care. [7]
- Ambient temperature and heat-wave paediatric morbidity reviews; extreme-heat acute-care utilisation studies. [8] [9] [11] [16]
- Thermoregulation and perinatal heat syntheses; equity and education papers. [10] [14] [12] [13]
Regional practice notes [3] [5]
- ANZ: Sports Medicine Australia and school extreme-heat policies; high ambient UV often coexists with heat — pair with sun protection counselling without merging the topics. [5]
- UK: UKHSA heat-health alerts and adverse weather plans drive school and community response. [3]
- US: AAP climate and sports policies; NATA/NFHS-style preseason heat safety and immersion culture in many athletic programmes. [5] [7]
- Canada: provincial heat warnings and public-health messaging; adapt counselling to local alert systems. [3]
Exact cancellation thresholds differ by sport governing body — quote the local policy in OSCE stations rather than inventing a universal number. [5]
Exam Pearls
- Heat stroke = heat stress + CNS dysfunction → cool immediately. [6]
- Exertional heat stroke victims may still sweat. [6]
- Cold-water immersion is preferred field cooling when available. [7]
- Acclimatise sports over roughly 10–14 days; modify for humidity. [5]
- Never leave a child in a parked car. [8]
- Children have developmental thermoregulatory limits and caregiver dependence. [10]
- Climate change is a paediatric equity issue with clinical and advocacy roles. [1] [3] [12]
- Check glucose in every collapsed child; do not miss mimics. [6]
References
- [1]Council on Environmental Health Global Climate Change and Children's Health Pediatrics, 2015.PMID 26504130
- [2]Ahdoot S Global Climate Change and Children's Health Pediatrics, 2015.PMID 26504134
- [3]Ahdoot S Climate Change and Children's Health: Building a Healthy Future for Every Child Pediatrics, 2024.PMID 38374808
- [4]Ahdoot S Climate Change and Children's Health: Building a Healthy Future for Every Child Pediatrics, 2024.PMID 38374809
- [5]Council on Sports Medicine and Fitness and Council on School Health Policy statement—Climatic heat stress and exercising children and adolescents Pediatrics, 2011.PMID 21824876
- [6]Bouchama A Heat stroke N Engl J Med, 2002.PMID 12075060
- [7]Miller KC Roundtable on Preseason Heat Safety in Secondary School Athletics: Prehospital Care of Patients With Exertional Heat Stroke J Athl Train, 2021.PMID 33290540
- [8]Xu Z The impact of heat waves on children's health: a systematic review Int J Biometeorol, 2014.PMID 23525899
- [9]Xu Z Impact of ambient temperature on children's health: a systematic review Environ Res, 2012.PMID 22831555
- [10]Smith CJ Pediatric Thermoregulation: Considerations in the Face of Global Climate Change Nutrients, 2019.PMID 31454933
- [11]Uibel D Association of ambient extreme heat with pediatric morbidity: a scoping review Int J Biometeorol, 2022.PMID 35751701
- [12]Budolfson KC Climate Change and Child Health Equity Pediatr Clin North Am, 2023.PMID 37422317
- [13]Henning A Impact of the Climate Crisis on Childhood Health Pediatr Rev, 2025.PMID 41320106
- [14]Principi N The Influence of Heat on Pediatric and Perinatal Health: Risks, Evidence, and Future Directions J Clin Med, 2025.PMID 40004654
- [15]Souilla L Children With Cardiac Disease and Heat Exposure: Catastrophic Converging Consequences? Pediatr Exerc Sci, 2024.PMID 38171350
- [16]Ndovu A Spatial Variation in the Association between Extreme Heat Events and Warm Season Pediatric Acute Care Utilization: A Small-Area Assessment Environ Health Perspect, 2025.PMID 39883533