Paeds · preventive-and-community-paediatrics
Community needs assessment and child-health advocacy
Also known as Child health advocacy · Community paediatrics needs assessment · Paediatric health advocate role · Community pediatrics advocacy · Population advocacy for children
Fellowship guide to community needs assessment and child-health advocacy: define the community, gather mixed data, map assets, prioritise with partners, act at patient-to-policy levels, evaluate equity outcomes, and keep acute social crises on the resuscitation pathway.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
A.D.V.O.C.A.T.E. cycle
Overview & Definition
A parent asks for “a letter for housing.” A resident wants “a community project.” A school reports rising absences. A journalist wants a quote after a toddler drowning cluster. These are not soft extras. They are the everyday face of community needs assessment and child-health advocacy. [1] [17]
Community needs assessment is the disciplined way you learn what a defined population needs and what it already has. You combine epidemiology, service data and community voice before you invent a programme. Child-health advocacy is the work of using your expertise and influence to improve those conditions — for one child, for your clinic population, with a community coalition, or in policy and media. [1] [2]
Earnest and colleagues framed physician advocacy as action beyond the individual patient to promote social, economic, educational and political changes that secure better health. That definition keeps advocacy clinical, not purely political hobby. [1]
This page owns the method and the skill set. Dedicated leaves cover deep housing and food insecurity care, Indigenous and Māori culturally safe care, pure population epidemiology methods, rural inequity, and global child health. Cross-link those rather than hiding second chapters here. [19] [21] [22]
Classification
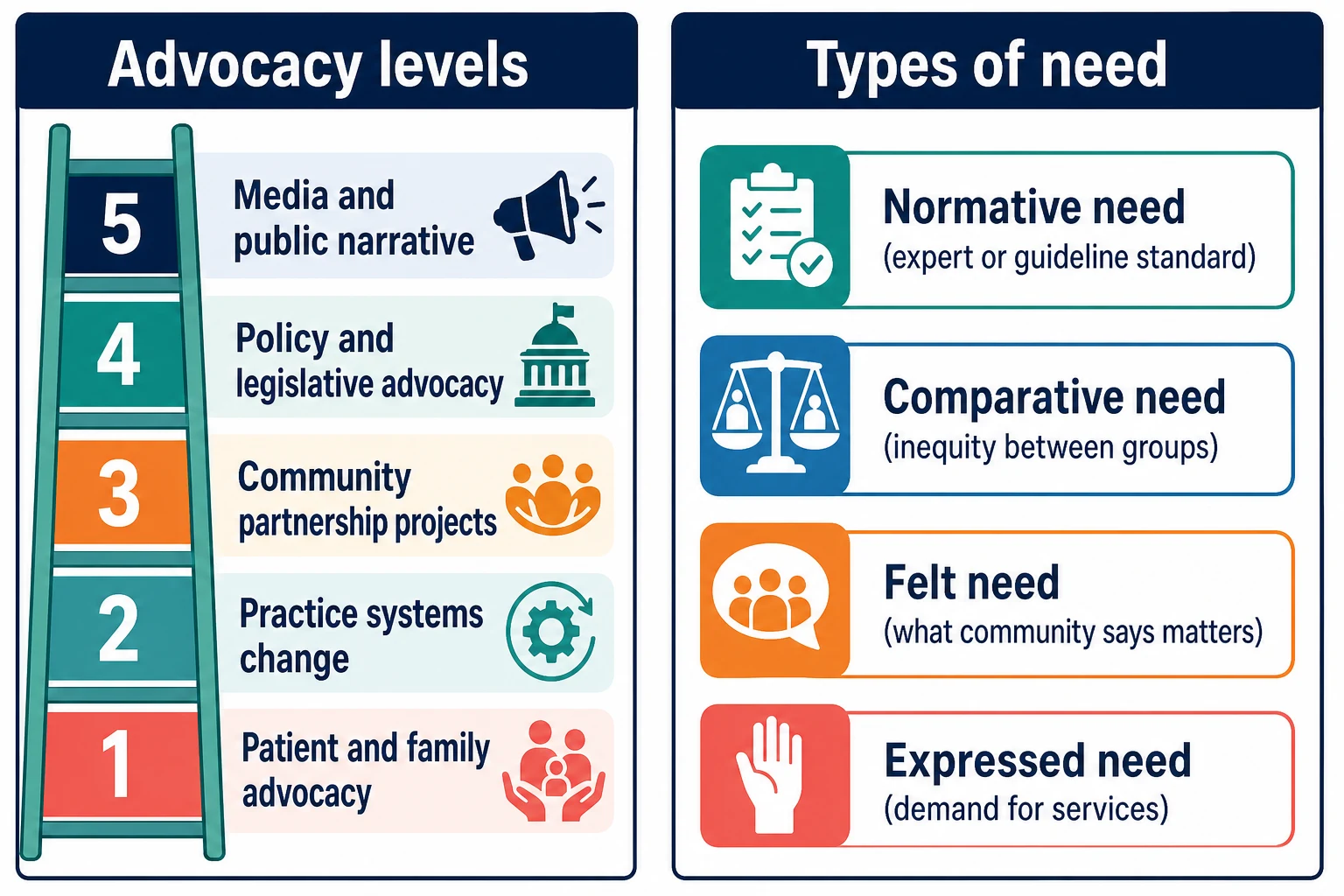
Sort the work two ways: level of advocacy and type of need. [1] [2]
- Patient and family — letters, forms, care navigation, school plans, disability supports, legal aid referral.
- Practice systems — social-determinant screening workflows, interpreter access, after-hours pathways, clinic–school linkage.
- Community partnership — projects with schools, councils, NGOs, primary-care networks.
- Policy and legislative — submissions, testimony, guideline or funding reform.
- Media and public narrative — accurate framing of child-health problems without sensational harm. [1] [2] [17]
Types of need (planning language). Normative need is the gap from a standard (guideline coverage, vaccine schedule). Comparative need is inequity between groups. Felt need is what families say matters. Expressed need is demand that shows up as waitlists or ED use. All four can disagree; good assessment holds the tension instead of picking the convenient one. [8] [17]
Partnership stance. Hubinette and colleagues emphasise advocacy with communities, not only for them. “For” without “with” risks professional capture and failed interventions. [3] [4]
Epidemiology & Risk Factors
Unmet social needs concentrate where power and resources are thin: socioeconomic disadvantage, Indigenous communities, migrant and refugee families, out-of-home care, youth justice and rural or remote catchments. Food insecurity and housing instability are common clinic signals of wider community failure. [19] [21] [22]
Paediatrician involvement in community child health has been tracked for decades. Surveys show variable participation and a training effect: structured community and advocacy education is associated with later community engagement strategies. CPTI follow-up and related studies support investment in residency-level community pediatrics. [10] [14] [15] [16]
US residency programmes teach community pediatrics and advocacy unevenly, and evaluation methods vary. CATCH-style community projects can shape career community involvement. Disparity-focused tracks that combine global health with local advocacy are one design response. [11] [12] [13]
System barriers matter as much as individual motivation: time, funding, mentorship, psychological safety, and institutional permission shape whether advocacy is possible. [6] [18]
Pathophysiology
Think of mechanisms that turn a postcode into a clinic problem. [20]
Toxic stress pathway. Early adversity and chronic threat, without buffering relationships, dysregulate stress physiology and shape lifelong health risk. The paediatrician’s role includes prevention, screening and systems response, not only individual counselling. [20]
Service-gap cascade. A treatable problem becomes chronic harm when transport, language access, waitlists, school exclusion or housing churn block care. Fragmented information between clinic, school and community services amplifies delay. [17] [22]
Power and voice. When professionals define “the need” without community partnership, projects miss felt priorities, waste trust and can stigmatise families. Advocacy that blames parents for structural poverty is a pathogenic narrative. [3] [4]
Inequity amplification. Children already facing adversity absorb the largest share of policy failure. Small access gains for privileged groups can widen gaps if equity is not measured. [13] [17]

Clinical Presentation
You will meet this topic in ordinary rooms. [17] [19]
Clinic signals of community problems. Repeated no-shows with transport barriers. “We ran out of food before payday.” Multiple address changes. A cluster of school absences in one estate. Several children with the same environmental exposure. One letter request that is really systems advocacy. [21] [22]
Project invitations. A service asks for “a resident community project.” A council wants a paediatric opinion on playgrounds or air quality. An NGO invites partnership on early years support. These need a needs-assessment frame, not a logo on a flyer. [8] [11]
Public-facing requests. Media after a child injury cluster. Policy consultation on poverty, early childhood or immunisation access. Testimony that must stay evidence-true. [1] [18]
Learner presentation. A trainee who wants to “do advocacy” without defining the community, partners or evaluation plan. Teaching starts with structure, not enthusiasm alone. [7] [9]
Differential Diagnosis
Name what problem you actually have. [2] [8]
| You notice | Prefer this framing | Not only this trap |
|---|---|---|
| One family in crisis | Patient-level advocacy + safety plan | “We need a whole campaign first” |
| Same barrier across many families | Practice or community pattern | Isolated parenting failure |
| Community says X; data say Y | Hold both; explore measurement bias | Discard lived experience |
| Waitlist demand rises | Expressed need ± access failure | Assume more of the same service is the only answer |
| Trainee wants a project | Needs assessment + partner first | Instant programme branded to the hospital |
| Injury or infection cluster | Public-health emergency pathway | Slow committee without notification |
Safeguarding versus structural inequity. Both can coexist. Maltreatment concern still needs mandatory reporting pathways. Structural poverty still needs systems advocacy. Do not use one to erase the other. [20] [22]
Clinical & Bedside Assessment
Start with the child in front of you. Screen social needs with dignity. Ask about food, housing, safety, school and money stress in plain language. Offer help, not interrogation. Document facts needed for care and consent for any external advocacy letter. [19] [21] [22]
Define the community. Geography, school cluster, cultural identity group, service catchment or clinic panel — name it. A vague “the community” cannot be assessed. [8]
Map stakeholders. Families and young people first. Then schools, primary care, public health, local government, cultural leaders, NGOs and existing coalitions. Who already holds trust? Who holds data? Who holds power to change a rule? [2] [3]
Asset map before deficit dump. Skills, places, programmes, informal networks and cultural strengths prevent reinventing what already works. [8] [11]
Ethics at the bedside of community work. Consent for stories. Cultural safety. Avoid extractive surveys. Protect children used as “case examples” in media. [3] [6]
Investigations
Treat “investigation” as mixed methods, not only blood tests. [8] [17]
Quantitative sources. Local epidemiology and deprivation indices. Immunisation coverage. ED and admission patterns for ambulatory-sensitive conditions. School absence data. Clinic social-need screen results. Housing or food-bank utilisation where available. [17] [19]
Qualitative sources. Focus groups, key-informant interviews, community forums, youth voice sessions, and partner mapping meetings. Stories explain why numbers look the way they do. [2] [8]
Required versus optional versus harmful. [8]
- Required when acting at scale: a defined population, at least one community voice source, and baseline metrics you can re-measure.
- Optional: formal survey research if simpler partner data already answer the question.
- Harmful delays: waiting for perfect data while a child is hungry, homeless or unsafe; or endless assessment that never reaches action. [8] [21] [22]
Evaluation metrics. Process (who engaged, what delivered), outcome (access, health, education), and equity (did the gap narrow for the groups most affected?). [9] [10]
Management — Resuscitation
Some “community issues” are emergencies for a child today. [20] [22]
Act now for the individual. Food crisis: same-day food access pathway and follow-up. Housing crisis: social work/housing service linkage and safety planning. Suspected maltreatment: mandatory reporting and protection pathway per local law. Acute environmental hazard or outbreak: notify public health and protect exposed children. [19] [21] [22]
Do not park crisis in a project log. A needs-assessment cycle can run in parallel for the population pattern, but the child in front of you still needs a plan before the next night. [8] [22]
Cluster emergencies. Multiple children with the same injury mechanism, toxin exposure or vaccine-preventable disease may need public-health activation, not only clinic QI. [17]
Management — Definitive & Stepwise
Use a repeatable cycle. The AAP Community Pediatrics Training Initiative project-planning approach is a practical scaffold for learners and services. [8]
- Define the community and the question.
- Engage partners early — especially family and youth voice.
- Collect mixed data (numbers + stories).
- Map assets and gaps.
- Prioritise with transparent criteria (severity, equity, feasibility, community priority, political window).
- Plan and act with roles, timeline and risk management.
- Evaluate process, outcome and equity.
- Feedback and sustain or hand over deliberately. [2] [8] [9]
Advocacy ladder in practice. Fix the individual barrier. Change the clinic system that produced it. Build a community coalition for shared problems. Escalate to policy or media only with verified evidence and partner consent. [1] [2] [17]
Communication products. One-page briefs for decision-makers. Structured testimony: who you are, what you see, what evidence shows, what you ask for, what residual uncertainty remains. Never invent prevalence figures under pressure. [1] [18]
Training and competence. Systematic reviews show advocacy can be taught, but programmes vary. Milestone tools such as CHAMP link community work to observable competence rather than attendance alone. [7] [9] [12]

Specific Subtypes & Scenarios
Food insecurity practice pathway. Screen, normalise, link to food access, and track clinic patterns that may justify partnership with food banks or local policy work. Individual help and systems work both count. [19] [21]
Housing insecurity. Letters should state clinical facts, functional impact and urgency without fabricating diagnoses. Parallel social-work pathways and population advocacy for housing supply or tenancy protections may follow. [22]
School absence cluster. Define the school or estate, meet education partners, check health contributors (asthma, mental health, transport, bullying, undiagnosed disability), and avoid pure medicalisation of education failure. [17]
Immunisation access inequity. Map who is missing, why (access, trust, logistics), and design catch-up with community partners rather than blame campaigns alone. [17]
Resident advocacy project. Use a planning tool: community definition, partners, objectives, activities, evaluation, sustainability. Link to milestones so learning is assessable. [8] [9] [12]
Media after a child injury cluster. Lead with verified facts, prevention layers and system asks. Protect identities. Decline speculative blame. [1]
Policy consultation. Bring clinic epidemiology, community partner priorities and clear asks. Disclose uncertainty. Avoid party-political branding in professional testimony. [1] [18]
Complications & Pitfalls
- Needs assessment without community voice (professional capture). [3]
- Endless data collection with no action. [8]
- Launching a branded programme nobody asked for. [2]
- Blaming families for structural inequity. [20]
- Inventing statistics for media or grants. [1]
- Confidentiality breaches in storytelling. [6]
- Lone-hero advocacy without coalition or succession. [2] [6]
- Measuring attendance at events instead of equity outcomes. [9]
- Ignoring acute safeguarding while “advocating upstream.” [20] [22]
- Token Indigenous or migrant consultation without power-sharing (cross-link dedicated cultural-safety leaves). [3]
Prognosis & Disposition
Successful advocacy is visible in access, outcomes and narrowed inequities — not in press cuttings alone. CPTI and related training literature suggest structured exposure can influence later community engagement, though system supports still determine sustainability. [10] [15]
Disposition choices for projects. Continue and scale if equity metrics move and partners remain. Redesign if the wrong need was prioritised. Hand over if a community organisation should own the work. Stop if harm, futility or extractive dynamics appear. [2] [8]
Career disposition. General paediatric practice can include patient advocacy weekly, practice systems monthly, and selected community or policy work yearly. Not every paediatrician leads legislation; every paediatrician can refuse to treat structural barriers as invisible. [14] [17]
Special Populations
Indigenous families and communities. Advocacy must be partnership-led and culturally safe. Dedicated leaves cover Indigenous, Aboriginal and Torres Strait Islander, and Māori/Te Tiriti frameworks — do not improvise those sovereignties here. [3]
Migrant and refugee communities. Language access, trauma-informed engagement and distrust of authorities shape both needs assessment and advocacy letters. [13]
Disability and medical complexity. Systems advocacy often targets equipment funding, school support hours, transport and respite — with families as experts on daily barriers. [17]
Out-of-home care and youth justice. Information fragmentation and power imbalance demand careful consent and strong inter-agency advocacy. [22]
Rural and remote. Thin services mean coalition work with primary care, retrieval systems and telehealth; do not assume urban NGO density. [17]
Adolescents. Include youth voice in assessment and advocacy. Confidentiality rules still apply when stories become public. [3] [6]
Evidence, Guidelines & Regional Differences
Core evidence includes definitions and models of physician advocacy, partnership-framed Health Advocate teaching, CPTI project-planning and milestone tools, community pediatrics involvement surveys, CATCH influence, residency teaching patterns, and AAP public-health, food-security and housing statements. Toxic-stress science supplies the developmental rationale for upstream work. [1] [2] [3] [7] [8] [9] [10] [11] [17] [20] [21] [22]
Community child health and public-health paediatric roles vary by jurisdiction. Use local community health services, Aboriginal Community Controlled Health Services, Māori health partners, and state/territory public-health units. RACP training expects professional practice around equity and systems. Do not invent national benefit rates; name the local pathway. [17]
Community paediatrics and public-health nursing structures differ from US SBHC models. RCPCH Progress+ emphasises health promotion, communication and system working. Local authority and NHS interfaces shape needs assessment partners. [7]
AAP community pediatrics, CATCH and CPTI tools are prominent training resources. Residency advocacy curricula are common but heterogeneous in evaluation. Policy advocacy culture is more explicit in many programmes. [8] [11] [12] [17]
CanMEDS Health Advocate is an explicit role. Assessment of advocacy competence remains debated; examiners still expect partnership language and population thinking. Provincial public-health and social-service pathways vary. [4] [5] [6]
Controversies to handle carefully: myths of pure political neutrality; burden and ethics of universal SDOH screening; whether advocacy competence can be standardised; and how far trainees should go in public politics. Exam answers show judgment, partnership and evidence discipline. [5] [6] [18]
Exam Pearls
- Advocacy is a clinical skill set, not optional activism. [1]
- With communities, not only for them. [3]
- Define the community before the project logo. [8]
- Assets as well as deficits. [8]
- Acute food, housing or safety crisis is resuscitation. [21] [22]
- Never invent numbers for media or policy. [1]
- Measure equity outcomes, not only event attendance. [9]
- CanMEDS Health Advocate is examinable language in Canada. [5]
- Training exposure predicts later community strategies — system supports still matter. [10] [15]
- Cross-link population epidemiology for pure epi methods; this page owns advocacy method. [17]
References
- [1]Earnest MA Perspective: Physician advocacy: what is it and how do we do it? Academic medicine : journal of the Association of American Medical Colleges, 2010.PMID 20042825
- [2]Dobson S From the clinic to the community: the activities and abilities of effective health advocates. Academic medicine : journal of the Association of American Medical Colleges, 2015.PMID 25470309
- [3]Hubinette M Not just 'for' but 'with': health advocacy as a partnership process. Medical education, 2015.PMID 26152491
- [4]Hubinette MM Lessons From Rocket Science: Reframing the Concept of the Physician Health Advocate. Academic medicine : journal of the Association of American Medical Colleges, 2016.PMID 27438156
- [5]LaDonna KA Grappling with key questions about assessment of the Health Advocate role. Canadian medical education journal, 2023.PMID 36998507
- [6]Kahlke R Health advocacy among medical learners: Unpacking contextual barriers and affordances. Medical education, 2023.PMID 36490220
- [7]Scott MD Teaching Health Advocacy: A Systematic Review of Educational Interventions for Postgraduate Medical Trainees. Academic medicine : journal of the Association of American Medical Colleges, 2020.PMID 31702691
- [8]Hoffman BD The Community Pediatrics Training Initiative Project Planning Tool: A Practical Approach to Community-Based Advocacy. MedEdPORTAL : the journal of teaching and learning resources, 2017.PMID 30800831
- [9]Hoffman BD The Community Health and Advocacy Milestones Profile: A Novel Tool Linking Community Pediatrics and Advocacy Training to Assessment of Milestones-Based Competence in Pediatric Residency Training. Academic pediatrics, 2016.PMID 27002213
- [10]Minkovitz CS Five-year follow-up of Community Pediatrics Training Initiative. Pediatrics, 2014.PMID 24982098
- [11]Soares NS The influence of Community Access to Child Health (CATCH) program on community pediatrics. Pediatrics, 2014.PMID 24323996
- [12]Lichtenstein C How Do US Pediatric Residency Programs Teach and Evaluate Community Pediatrics and Advocacy Training? Academic pediatrics, 2017.PMID 28254496
- [13]Pak-Gorstein S Training Pediatricians to Address Health Disparities: An Innovative Residency Track Combining Global Health With Community Pediatrics and Advocacy. Academic medicine : journal of the Association of American Medical Colleges, 2018.PMID 29847326
- [14]Minkovitz CS Pediatricians' involvement in community child health from 2004 to 2010. Pediatrics, 2013.PMID 24249821
- [15]Solomon BS Residency training and use of strategies to promote community child health one year after graduation. Academic pediatrics, 2012.PMID 22405963
- [16]Minkovitz CS Pediatricians' involvement in community child health from 1989 to 2004. Archives of pediatrics & adolescent medicine, 2008.PMID 18606937
- [17]Kuo AA Pediatricians and Public Health: Optimizing the Health and Well-Being of the Nation's Children. Pediatrics, 2018.PMID 29358481
- [18]Federico SG United States Pediatricians' Attitudes Regarding Public Policies for Low-Income Children and Their Profession's Advocacy Priorities. Academic pediatrics, 2018.PMID 29654906
- [19]Hartline-Grafton H Food Insecurity and Health: Practices and Policies to Address Food Insecurity among Children. Academic pediatrics, 2021.PMID 32653691
- [20]Garner AS Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148
- [21]COUNCIL ON COMMUNITY PEDIATRICS Promoting Food Security for All Children. Pediatrics, 2015.PMID 26498462
- [22]Council on Community Pediatrics Providing care for children and adolescents facing homelessness and housing insecurity. Pediatrics, 2013.PMID 23713108