Paeds · preventive-and-community-paediatrics
Developmental and behavioural screening
Also known as Developmental screening programme · Behavioural screening in children · ASQ developmental screen · M-CHAT autism screening · Early childhood mental health screening
Fellowship guide to developmental and behavioural screening in preventive paediatrics: key-age general screens, autism-specific two-stage pathways, early emotional-behavioural screening, interpretation, closed-loop referral, equity and exam defence — cross-linked to surveillance technique without cloning it.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent hands you a completed questionnaire at the 18-month visit. The nurse has scored the autism screen. The toddler is climbing the examination table. Your job is not to file the paper. Your job is to run a developmental and behavioural screening programme inside preventive care: the right tool, at the right age, with the right interpretation, referral and follow-up. [1] [8]
Developmental screening is the periodic use of a standardised instrument with known performance characteristics to identify children who need further evaluation. It sits between continuous surveillance (asking, watching, documenting every visit) and evaluation (the diagnostic assessment that can name a condition and open services). Lipkin’s AAP report is the modern programme anchor for this nested model. [1] [7]
This page owns screening systems in preventive and community paediatrics. Bedside milestone technique, evidence-informed milestone content and observation craft live on the linked page Developmental surveillance and milestone assessment. Cross-link it. Do not hide a second surveillance chapter here. [1] [3]
Behavioural screening in early childhood means structured attention to emotional, relational and behavioural risk — not only motor and language scores. More than 10% of young children experience clinically significant mental health problems. The medical home is often the first and only reliable contact. [5]
Programme spine in one visit
Is the child well and safe?
If no, convert. Screening paperwork can wait.
Surveillance always
Elicit concern and observe — see the D01 surveillance page for technique.
Right tool class
General developmental, autism-specific, and/or behavioural as age and concern dictate.
Score and interpret
Pass, borderline/monitor, or refer — with clinical judgement over a lonely number.
Act and close the loop
Refer, interim supports, owner, date, safety-net.
Classification
Classify three things before you open a form: the job, the tool class, and the result band. [1]
Three nested jobs
| Job | What it is | When | Output |
|---|---|---|---|
| Surveillance | Continuous skilled process: concerns, observation, milestones, domains | Every health encounter | Domain notes and red-flag action |
| Screening | Standardised tool with known performance | Key ages or on concern | Pass / borderline / refer |
| Evaluation | Diagnostic and multidisciplinary assessment | Fail screen or strong clinical worry | Diagnosis plan and services |
Surveillance technique detail is owned by the D01 page. This leaf uses that process as the always-on base layer under formal screens. [1] [3]
Tool classes
General developmental screens (for example ASQ-type parent questionnaires used by many services) look across domains such as communication, gross motor, fine motor, problem-solving and personal-social skills. They are not autism-specific. [1] [4]
Autism-specific screens target social communication risk. M-CHAT-R/F is a two-stage parent questionnaire validated at 18- and 24-month well-child visits. Stage two is a structured follow-up interview, not optional chit-chat. [2]
Behavioural and emotional screens identify early mental health and relationship risk. They sit beside developmental tools rather than replacing them. Gleason’s AAP clinical report places the paediatrician as medical-home leader for early emotional and behavioural problems. [5]
Result bands
Most programmes map results into pass, borderline/monitor, and fail/refer. Exact cut-offs live in the tool manual your service uses. Do not invent proprietary tables in a viva. State the principle, name the tool version, and act on clinical concern even when a family declines the form. [1] [4]
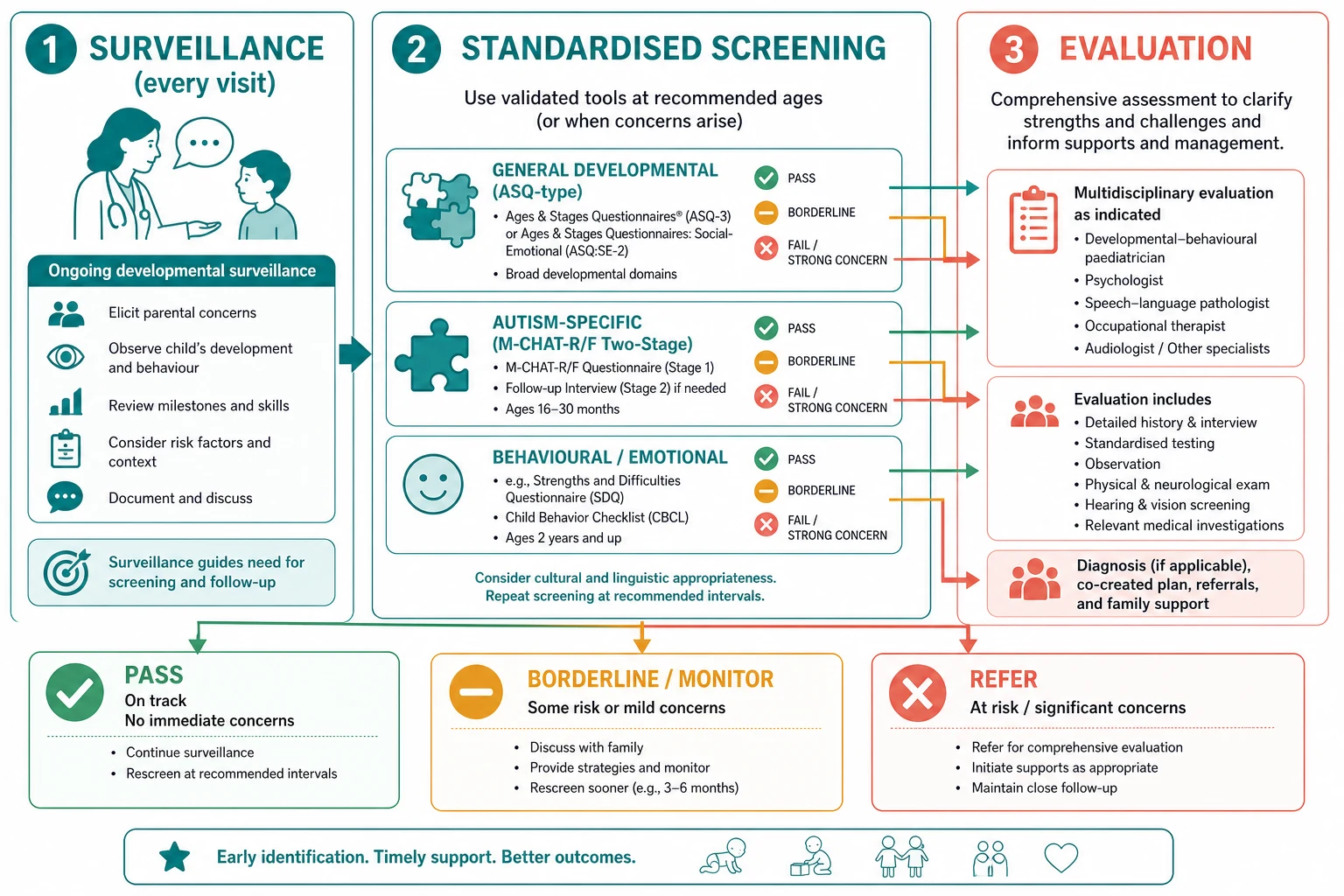
Read the figure like this: if you only do surveillance, you miss systematic detection. If you only file screens, you miss observation and caregiver concern. The programme needs both. [1]
Universal versus selective
Key-age general and autism screens are intended as universal in the medical-home model Lipkin describes. Some additional behavioural or laboratory actions are risk-based. Exams love this distinction. Do not invent a universal blood panel because a language domain was borderline. [1] [8]
Epidemiology & Risk Factors
Missed screening is patterned, not random. Families facing poverty, transport barriers, language discordance, racism in care systems or fragmented access complete fewer screens and fewer follow-ups. That is a clinical equity problem. Practice redesign — pre-visit tools, team-based delivery, standing workflows — improves preventive content for low-income panels. [15] [11]
Medical-home attributes and developmental monitoring/screening associate with earlier autism identification pathways in population analyses. Continuity beats episodic “form when we remember.” [6] [16]
Children in foster or kinship care often arrive with incomplete records. Catch-up screening is part of medical-home assignment, not a courtesy when “things settle.” [13]
Children with medical complexity are at risk of diagnostic overshadowing: every lag is blamed on the known diagnosis and new treatable needs are missed. [12]
Early emotional-behavioural problems are common enough that ignoring them is not “staying in lane.” More than 10% of young children have clinically significant mental health problems, with impairment and persistence comparable to older children. Access to psychotherapeutic care is limited; rigorous support for early psychopharmacology is narrow. Your screening and referral role therefore matters. [5]
Pathophysiology
Why does a questionnaire at 18 months matter at school entry? Early childhood is a high-plasticity window. Skills scaffold on earlier skills. If hearing is impaired, language maps form on a weak signal. If social-communication differences go unrecognised, intervention time is lost. If severe unbuffered stress keeps stress systems activated, behaviour and learning change — Garner’s toxic-stress framing without fatalism. [1] [10]
False reassurance is a mechanism of harm. A single pass screen, especially without surveillance, can silence a parent who was right. Open-loop failure is another mechanism: the screen was correct, the referral was written, and nobody chased the appointment. The biology of the child did not change; the system failed. [1] [14]
False positives also have a mechanism: family distress, over-medicalisation, and strained trust if you present a screen as a diagnosis. Good counselling converts uncertainty into a clear next step. [2]
Language-discordant administration degrades validity. A tool completed without professional interpreting is not the same instrument that was validated. [11]
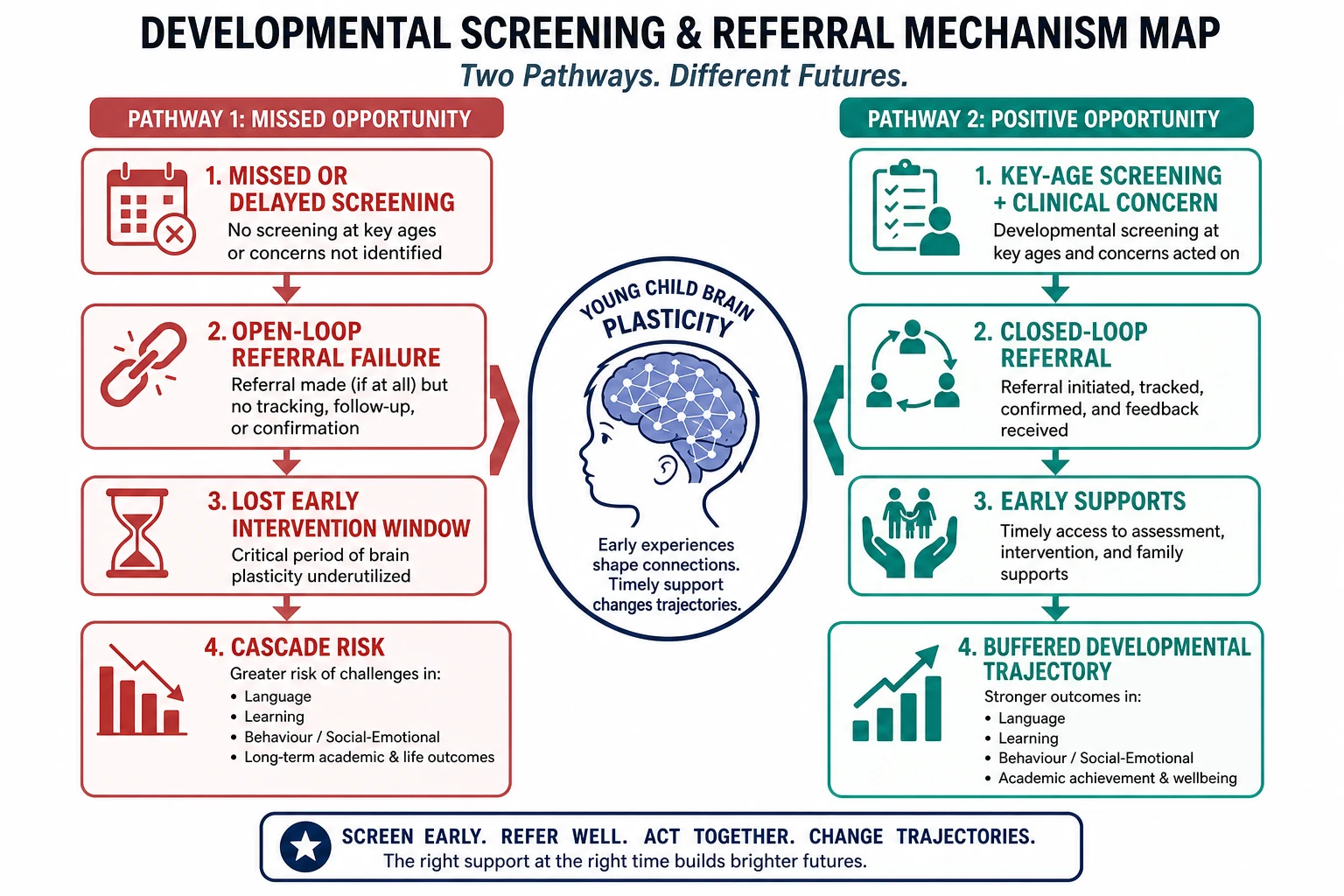
Read the figure like this: your job is not to promise a perfect life course. Your job is to remove remediable delays in detection and service access. [1] [10]
Clinical Presentation
Screening findings present as paper, as parent words, and as what you see on the floor. [1]
Common entry tickets
- “We filled the blue form for clinic.”
- “Speech is behind cousins.”
- “He does not look when we call his name.”
- “She was saying words and stopped.”
- “Behaviour is impossible at childcare.”
- “New foster placement — no records.”
What a positive general screen looks like
A parent-report tool at 9, 18 or 30 months lands in a refer band for one or more domains. The child may still “look cute” in a short visit. Domain scores plus observation decide urgency, not charm. [1] [4]
What a positive autism pathway looks like
On M-CHAT-R/F, an initial total score of 3 or more triggers the structured Follow-Up Interview. If the score remains 2 or more after follow-up, the child is high risk: about 47.5% later received an ASD diagnosis and about 94.6% had any developmental delay or concern in the validation cohort. That is enough to refer and support — not enough to label ASD in the waiting room. [2]
Behavioural presentations
Aggression, extreme tantrums, sleep collapse, withdrawn play, or caregiver fear of the child’s behaviour can be the presentation of early mental health need, sleep debt, hearing loss, trauma, developmental disorder, or several at once. Screen and assess; do not start with punishment advice. [5] [10]
When “screening visit” is the wrong label
Regression, encephalopathy, seizures, severe neglect, or an unwell child are not questionnaire days. Convert. [1]
Differential Diagnosis
In screening clinics the differential is often what system is this pattern pointing to? [1]
| Pattern | Prefer first | Also consider | Do not assume |
|---|---|---|---|
| Isolated language lag on screen | Hearing loss, language disorder pathway | Bilingual tempo with true concern still needs follow-up | “They will catch up” with no plan |
| Multi-domain fail | Global developmental delay evaluation | Medical illness, severe psychosocial deprivation | Single-domain speech therapy only |
| Social communication + restricted patterns | Autism evaluation pathway | Hearing loss, global delay, trauma-related withdrawal | Instant ASD label from M-CHAT alone |
| Behavioural crisis with normal motor scores | Sleep, hearing, trauma, early mental health, learning | Primary “naughty child” framing | Medication as first clinic move |
| Pass screen + strong caregiver concern | True emerging disorder, hearing, intermittent skills | Parental anxiety alone | End of pathway because the form passed |
| Known complex disease + new stall | New treatable developmental need | Expected baseline for the diagnosis | Overshadowing without fresh look |
Clinical & Bedside Assessment
Embed screening in the visit
Confirm the child is well enough for preventive care. Ask the family agenda first. Then run surveillance (see the D01 page) and the age-appropriate standardised tools your service uses. Screening should not erase listening. [1] [8]
Choose and administer tools
Use the validated instruments your clinic stocks and is trained to score. Common general tools include ASQ-type questionnaires; autism-specific pathways often use M-CHAT-R/F at toddler ages. Behavioural tools vary by region and age — name your local instrument rather than inventing one. [1] [2] [4]
Offer professional interpreters before tool completion when language discordance exists. Check literacy. A caregiver who cannot read the items is not “non-compliant.” [11]
M-CHAT-R/F pathway at the bedside
- Parent completes M-CHAT-R.
- Total score ≥3 (or local protocol-critical item rules if your service uses them) → complete the Follow-Up Interview.
- After follow-up, score ≥2 → high risk → refer for autism/developmental evaluation and early intervention supports.
- Explain uncertainty and next steps with teach-back.
- Document scores, interview completion, and referral owner. [2]
Do not skip follow-up to “save time.” That is how false positives multiply and true pathways get messy. [2]
Observation still counts
Watch response to name, joint attention, gesture, play quality, motor patterns and how the child uses the caregiver. Observation plus tool is stronger than either alone. Detailed milestone craft remains on the surveillance page. [1] [3]
Document like a system
Record tool name and version, date, domain or total bands, language of administration, interpreter use, clinical concern level, action, owner and review date. Handover fails when only “ASQ done” appears. [14]
Investigations
Screens guide people and pathways. They rarely replace sensory checks when communication is the problem. [1]
Hearing and vision. Any significant language or social-communication concern needs a hearing pathway if not already closed. Vision concerns need age-appropriate assessment routes. Do not wait for a specialist developmental diagnosis before fixing a sensory barrier. [1]
Medical testing. Targeted tests belong with evaluation teams unless red flags demand urgent neurology or metabolic review. Avoid shotgun genetics from one missed fine-motor item. [1]
Tool performance examples you may quote. In Schonhaut’s term and preterm cohort, ASQ showed about 75% sensitivity and 81% specificity against a developmental reference standard — useful as an example of “good enough for screening, not diagnosis,” not as a universal constant for every age and translation. [4]
M-CHAT-R/F predictive values after two-stage positive screening are cited above from Robins 2014. Quote them as validation-cohort figures, not personal folklore. [2]
Low-value moves. Repeating a failed screen next week instead of referring when concern is clear. Ordering broad panels because a parent is anxious and you want to look busy. Filing a positive screen without a named referral. [1] [14]
Management — Resuscitation
Most screening is outpatient prevention. Exceptions demand conversion: [1]
- Regression with encephalopathy, seizures or collapse — emergency paediatric pathway first.
- Active safeguarding or severe neglect — safety and statutory pathways supersede form completion.
- Caregiver acute mental health crisis discovered during psychosocial items — urgent adult mental-health/safety route while protecting the child.
- Child too unwell for a preventive slot — ABCDE assessment; book screening catch-up later.
Say the conversion out loud: “We are pausing the routine checks because safety comes first.” That is clinical leadership, not rudeness. [8]
Management — Definitive & Stepwise
- Build the clinic algorithm. Surveillance every visit. Standardised general developmental screening at key ages (Lipkin: 9, 18, 30 months). Autism-specific screening at toddler ages (validation model: 18 and 24 months). Behavioural/emotional screening per local early-childhood pathway. [1] [2] [5]
- Stock and train. Use validated tools your team can score correctly. Keep manuals accessible. Do not invent cut-offs in the corridor. [4]
- Administer with equity. Interpreters, literacy support, pre-visit completion when redesign allows. [11] [15]
- Interpret with judgement. Pass → continue surveillance and next key age. Borderline → structured early recheck plus interim strategies. Fail or strong concern → refer even if a tool is incomplete or “pass.” [1]
- Complete autism two-stage pathway when using M-CHAT-R/F; never treat stage one alone as final. [2]
- Refer early to developmental-behavioural paediatrics, speech/physio/OT, psychology, early intervention and education supports as indicated. Care coordination is part of the medical home. [14] [16]
- Counsel clearly. “This screen finds children who need a closer look. It does not give a final diagnosis.” Use teach-back. Share interim play, language and safety strategies. [1] [2]
- Close the loop. Track referral status. Chase no-shows. Document owners and dates. Measure completion and equity gaps as quality work. [6] [14]
- Safety-net. What to watch for (regression, lost skills, new safety risk). When to return sooner. How to contact the clinic if the referral stalls. [1]
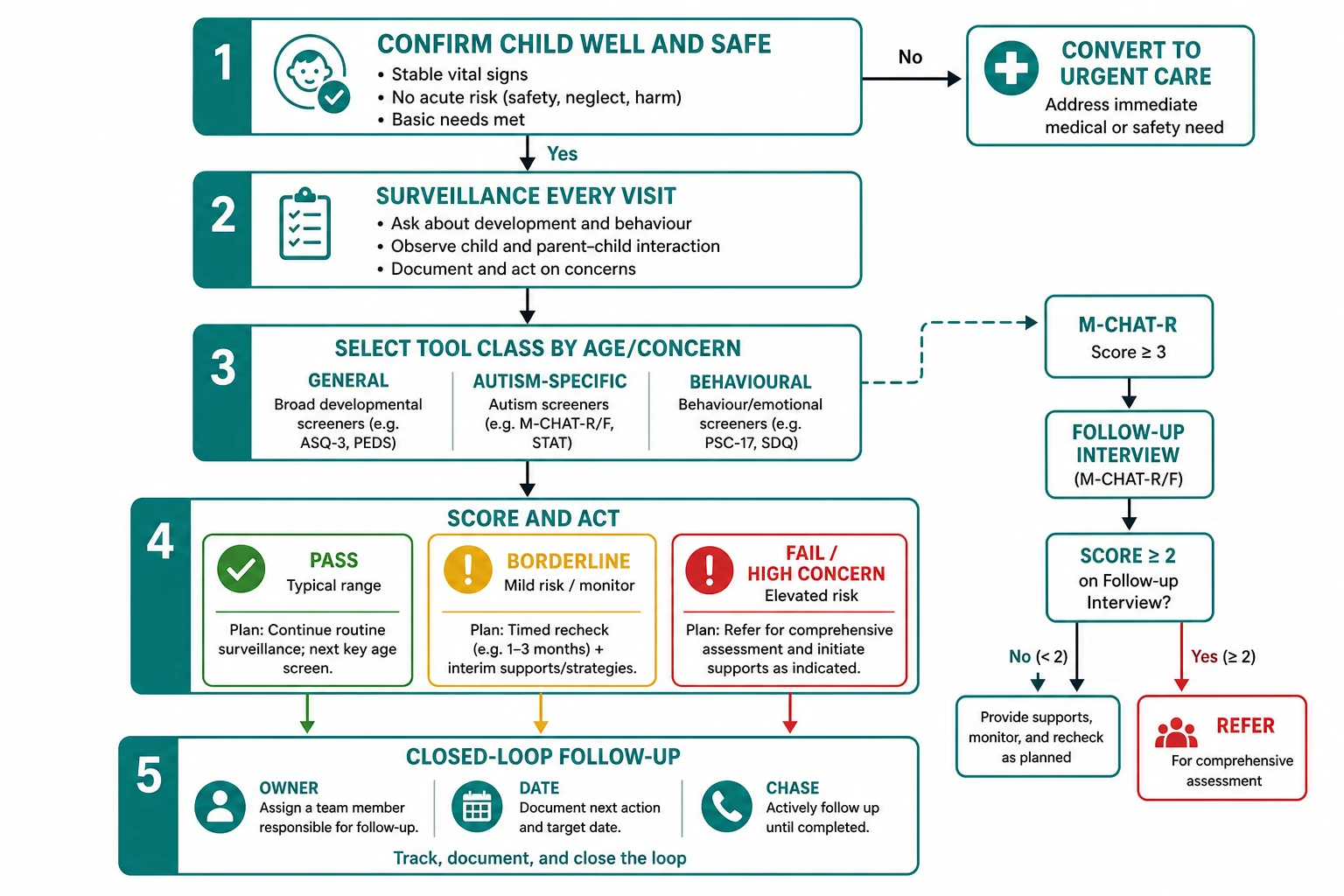
Read the figure like this: the algorithm fails at the weakest arrow. Most real-world failures are open loops, not missing forms. [14]
Specific Subtypes & Scenarios
Nine-month general screen. Motor and early communication domains matter. Act on fails; do not wait for the first birthday “because vaccines are the focus.” [1] [8]
Eighteen- and twenty-four-month autism pathway. Run general developmental screening as indicated and autism-specific two-stage screening. High concern or positive follow-up means referral now. [1] [2]
Thirty-month general screen. Catches children who were “borderline talkers” at 18 months. School-readiness risk starts here for many families. [1]
Pass screen, worried parent. Believe the signal. Recheck early or refer. Caregiver concern is clinical data. [1]
Ex-preterm infant. Intensified surveillance and screening; use corrected age only as your local developmental follow-up protocol advises, and do not skip tools because neonatal history “explains everything.” [1] [4]
Language-discordant family. Interpreter-mediated administration and counselling. Invalid tool completion is not a pass. [11]
Foster or kinship care. Assume missing screens until proven otherwise. Catch up and assign a medical home. [13]
Medical complexity. Ask what is new for this child. Avoid overshadowing. [12]
Preschool behavioural storm. Screen development and hearing/vision context; assess sleep, trauma and caregiver mental health; refer for early childhood mental-health supports; do not leap to medication as the medical-home first move when evidence for early psychopharmacology is limited. [5]
Rural long waitlists. Refer anyway, start interim allied-health and early-intervention supports available locally, and safety-net aggressively. Waitlists do not justify silence. [14]
Complications & Pitfalls
- Wait-and-see after a clear fail or strong concern.
- Screen-as-diagnosis language to families.
- Skipping M-CHAT follow-up after a positive initial score.
- Unvalidated checklists or outdated average-age milestone lists used as screens.
- No interpreter for tool completion.
- Open-loop referrals with no chase plan.
- Shotgun testing from a single mild lag.
- Behaviour label first, sensory and developmental causes second.
- Documenting a screen that never happened.
- Cloning D01 surveillance detail instead of linking it — wastes words and drifts both pages. [1] [2] [3] [11]
Prognosis & Disposition
Earlier access to intervention services improves functional trajectories for many children with developmental disorders. Screening only helps if it shortens time to support. [1] [6]
| Result | Disposition | Must include |
|---|---|---|
| Pass, no concern | Home with next key-age screen planned | Safety-net for new concern |
| Borderline/monitor | Timed early recheck | Interim strategies and owner |
| Fail or high concern | Referral + interim supports | Closed-loop chase plan |
| Regression/urgent flags | Acute or priority evaluation pathway | Same-day senior plan |
Disposition is not “refer and forget.” Give families something to do this week while systems move. [1] [14]
Special Populations
NICU graduates need organised developmental follow-up and screening intensity matched to risk. [1] [4]
Disability and neurodiversity. Adapt communication; screen for additional treatable needs; avoid deficit-only framing. [12]
Indigenous families. Culturally safe practice, trust, and local service pathways are part of valid screening — not optional courtesy. [15]
Migrant and refugee families. Catch-up screening, interpreter access, and trauma-informed pacing. [11] [13]
Out-of-home care. Incomplete histories are expected; accelerate medical-home screening catch-up. [13]
Socioeconomic disadvantage. Screening without social support pathways under-delivers; redesign visit flow. [15]
Maltreatment and family violence. Screening conversations may disclose risk — know your mandatory reporting and safety steps. [5] [10]
Evidence, Guidelines & Regional Differences
Lipkin and colleagues (AAP, 2020) model universal developmental surveillance every health supervision visit plus standardised screening at 9, 18 and 30 months, within a broader early-identification system that includes autism and other developmental conditions. [1]
Robins and colleagues validated M-CHAT-R/F as a two-stage screener at 18- and 24-month visits, with the score thresholds and predictive values cited above. [2]
Zubler and colleagues supply evidence-informed milestone content for surveillance tools — use via the D01 page rather than re-teaching full lists here. [3]
Schonhaut and colleagues provide an example of ASQ validity in term and preterm infants (about 75% sensitivity, 81% specificity in that study). Performance varies by age, setting and translation — treat as evidence of screening utility, not a universal constant. [4]
Gleason and colleagues define the medical-home role in early childhood emotional and behavioural problems and note limited rigorous psychopharmacology evidence in this age band. [5]
Barger and colleagues link medical-home monitoring/screening processes with earlier autism identification pathways. [6]
Bright Futures / AAP periodicity recommendations embed preventive screening tasks in the US map of well-child care. They are not global law. [8] [9]
Use jurisdictional child health books, local developmental screening programmes, and service-approved tools. Name your state/territory or DHB pathway in clinical practice. Cultural safety and interpreter access are part of valid screening. Do not import US ages as statute — use them as an evidence-informed framework and map to local schedules. [1]
The Healthy Child Programme structures universal contacts. Tool choice and referral pathways follow local integrated care and neurodevelopmental services. Defend principles (surveillance, key-age detection, early referral) and look up local operational forms. [1]
Bright Futures periodicity and AAP developmental guidance dominate exam answers. M-CHAT-R/F and ASQ-type tools are widely used. Still counsel that a screen is not a diagnosis. [1] [2] [8]
Primary-care tools such as Rourke-related records often structure visits; provincial pathways vary. Same nested model: surveillance, standardised screens, evaluation. [1]
Controversies. Universal versus selective intensity under workforce pressure; which general tool a service stocks; ethics of long neurodevelopmental waitlists; over-use of medication for early behaviour when therapy access is poor. Name the tension; do not invent false certainty. [5] [15]
Exam Pearls
References
- [1]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [2]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [3]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [4]Schonhaut L Validity of the ages and stages questionnaires in term and preterm infants. Pediatrics, 2013.PMID 23629619
- [5]Gleason MM Addressing Early Childhood Emotional and Behavioral Problems. Pediatrics, 2016.PMID 27940734
- [6]Barger B Medical Home, Developmental Monitoring/Screening, and Early Autism Identification. Journal of autism and developmental disorders, 2024.PMID 37477840
- [7]Council on Children With Disabilities Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening. Pediatrics, 2006.PMID 16818591
- [8]Committee on Practice and Ambulatory Medicine 2023 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2023.PMID 36938620
- [9]Committee on Practice and Ambulatory Medicine 2021 Recommendations for Preventive Pediatric Health Care. Pediatrics, 2021.PMID 33593848
- [10]Garner AS Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148
- [11]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [12]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [13]Szilagyi MA Health Care Issues for Children and Adolescents in Foster Care and Kinship Care. Pediatrics, 2015.PMID 26416941
- [14]Turchi RM Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [15]Coker TR Well-child care clinical practice redesign for serving low-income children. Pediatrics, 2014.PMID 24936004
- [16]Medical Home Initiatives for Children With Special Needs Project Advisory Committee The medical home. Pediatrics, 2002.PMID 12093969