Paeds · preventive-and-community-paediatrics
Environmental health and children's exposure risks
Also known as Paediatric environmental health · Children's environmental exposures · Environmental toxicology in children · Chemical exposures in childhood · Environmental history taking · PEHSU referral · Built environment child health
Fellowship-level hub on paediatric environmental health: why children are uniquely vulnerable, structured environmental history, major exposure domains, primary prevention, targeted testing, PEHSU and public-health pathways, and regional practice differences — without duplicating leaf detail on lead, air pollution or climate heat.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Paediatric environmental health studies how the physical and chemical world shapes child health — from the house dust a toddler crawls through to the chemicals in food packaging, well water, farm spray drift and the street outside school. A hazard is the agent that can harm. Exposure is contact with that agent. Dose is how much reaches the child. Susceptibility is how vulnerable the child is at that age and stage. Harm needs exposure plus susceptibility; removing either protects the child. [2] [3]
Most modern paediatric environmental disease is chronic and silent. Families rarely present saying “we have an exposure.” They present with asthma flares in a damp flat, developmental concerns after a renovation, or a well-looking toddler who lives near agricultural spraying. Acute high-dose poisonings still happen — pesticide ingestion, elemental mercury spills, contaminated products — but the everyday work is prevention and history. [1] [7] [9]
How to use this hub. Detailed lead management, tobacco/vaping/air pollution and climate heat have their own leaves. Here you learn the shared framework: vulnerability, history structure, major domains, when to test, when to escalate, and how to counsel without false reassurance or caregiver blame. [13] [14]
Classification
Organise every environmental problem on three axes: what medium carries the hazard, how it enters the child, and whether the problem is acute high-dose or chronic low-level. Those axes decide urgency, which test (if any) to order, and who else must act. [2] [3]
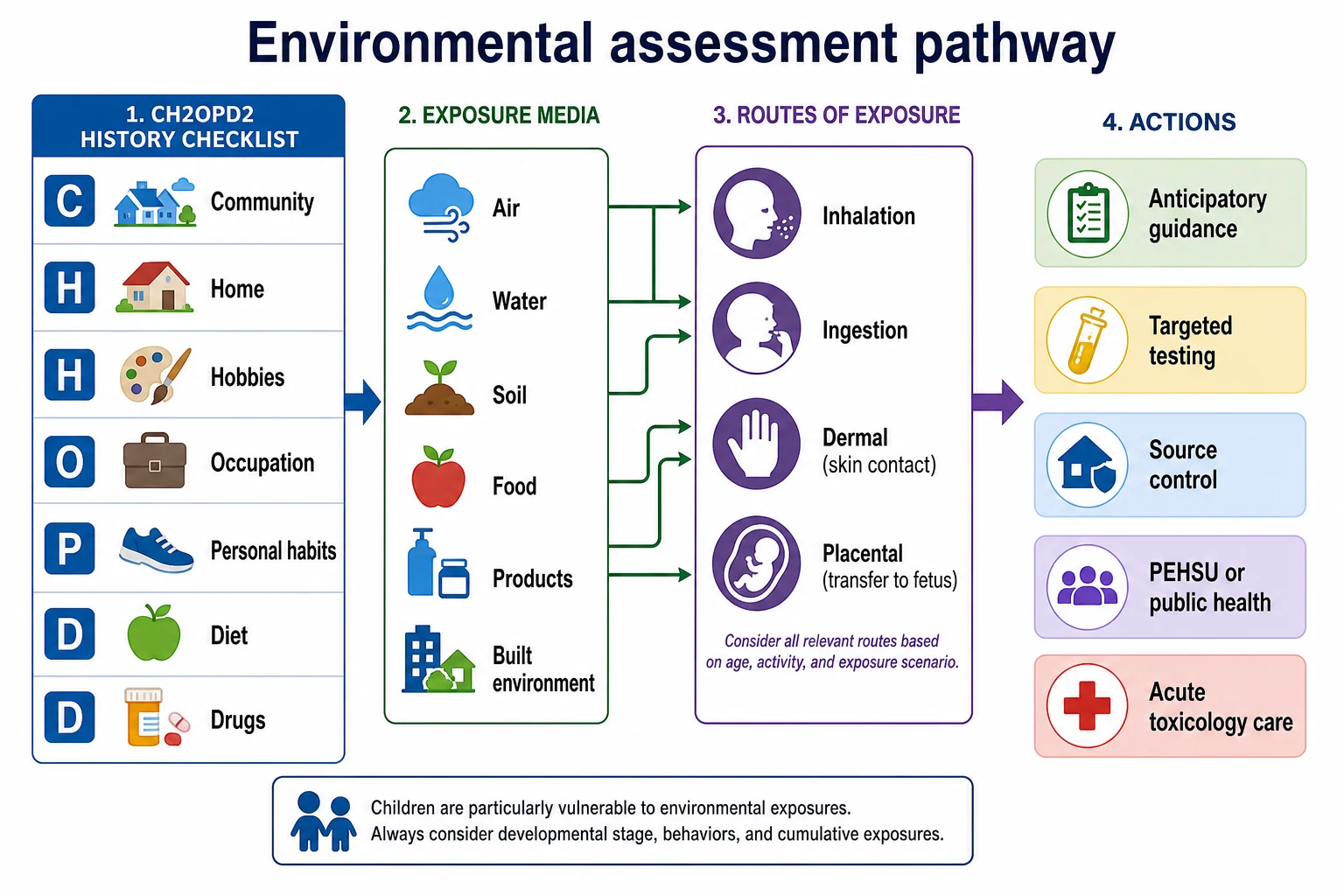
By medium (where the agent lives): air (indoor and outdoor), water, soil and dust, food, consumer products and cosmetics, and the built environment (housing quality, traffic, parks, schools). [4] [5]
By route (how it enters): inhalation, ingestion (including hand-to-mouth dust), dermal absorption, placental transfer, and breast-milk transfer for some agents. [2] [7]
By tempo: acute high-dose, subacute household, chronic low-level, and community/cluster patterns drive different first moves. [1] [11]
| Pattern | What you see | First move |
|---|---|---|
| Acute high-dose | Rapid systemic or organ toxicity after a clear event | Remove exposure, ABCDE, poison centre |
| Subacute household | New renovation, spill, product, well change | Stop the source, assess household, targeted tests |
| Chronic low-level | Silent developmental, respiratory or learning effects | Prevention, risk reduction, surveillance |
| Community/cluster | Several children with shared place or product | Public health investigation |
Do not invent a single “safe versus toxic” blood number that applies to all chemicals. Lead has its own reference-value language; other agents use different markers or no routine biomarker at all. [13]
Epidemiology & Risk Factors
Environmental risk is not randomly distributed. Younger children, families in poor-quality housing, communities near industry or intensive agriculture, and groups facing structural inequity carry more of the burden. After petrol and many product reforms, residual hazards still cluster where housing stock is old, regulation is weaker, or private wells replace treated municipal water. [3] [4] [5]
High-yield risk settings to ask about every time: [1] [4] [5]
- Older or damp housing, recent renovation, peeling paint, visible mould
- Private well water or intermittent water supply
- Farm, orchard, pest-control or industrial work with take-home dust or clothing
- School or childcare near busy roads or spraying
- Imported cosmetics, traditional remedies, hobbies (soldering, ceramics, shooting ranges)
- Loud recreational noise without hearing protection
Inequity is clinical data. A family may know the flat is mouldy and still have no power to move. Your plan must include practical interim controls and advocacy pathways, not only advice to “find better housing.” [4] [9]
Pathophysiology
Children receive a higher dose of many agents per kilogram than adults. They breathe faster, drink more water per kilogram, and put hands and objects in their mouths. Skin surface area relative to body mass is larger in infants. Detoxification enzyme systems and the blood–brain barrier mature over time, so the same external concentration can mean a different internal dose and a different brain effect. [2] [7]
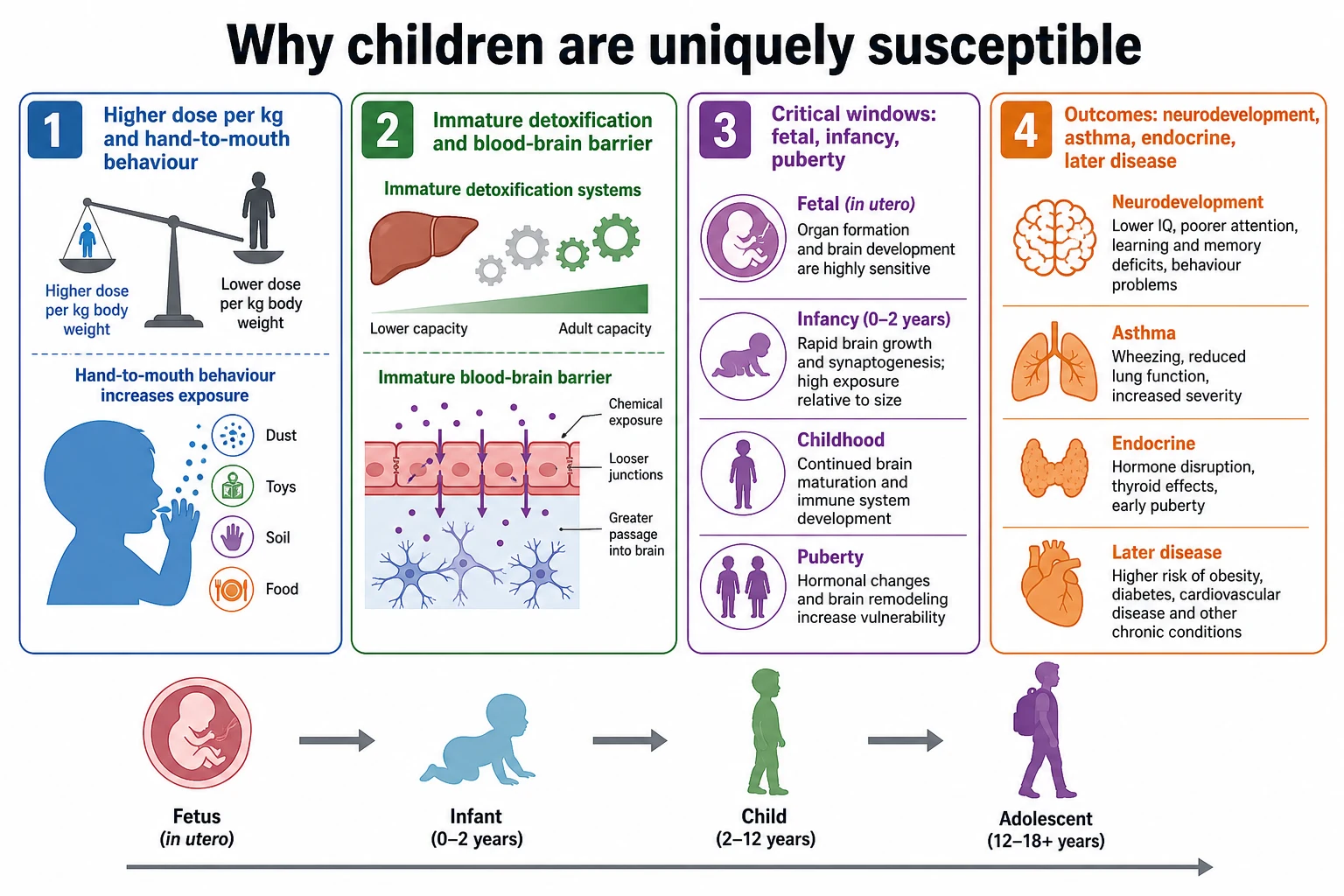
Critical windows matter more than average lifetime dose for many outcomes. A chemical present during neurogenesis, airway growth or puberty can change structure and set-points that later medicine cannot fully reset. That is why prenatal and infant exposures dominate policy debates even when adult workers tolerate higher levels. [3] [14]
Mechanistic themes examiners expect by name: [2] [7]
- Developmental neurotoxicity (e.g. lead, methylmercury, some pesticides)
- Respiratory sensitisation and irritation (dampness/mould, indoor combustion, outdoor pollutants — detail on the air leaf)
- Endocrine disruption (selected industrial chemicals and consumer product plasticisers — counsel on reduction, avoid overclaiming single-product cures)
- Mixture and cumulative risk — real children meet several agents at once; regulation often tests one chemical at a time [3]
Latency is part of the pathophysiology. Early exposure may show as school difficulty years later. That latency is why primary prevention is the prognosis strategy. [3] [13]
Clinical Presentation
Most children with important environmental risk look well on the day you meet them. The examination can be normal while the history is screaming. Teach yourself to hear housing, work, water and products as clinical signs. [1] [5]
Common clinic patterns: [1] [9] [6]
- Recurrent wheeze or cough worse in a damp, mouldy or poorly ventilated home
- Developmental plateau, attention or behaviour change after a new home, renovation or farm season
- Family asking about organic food, “toxins” or detox after social media content
- Acute GI or cholinergic symptoms after pesticide access
- Irritability, tremor or respiratory distress after a mercury spill or vapour exposure
- Hearing or tinnitus concerns after repeated loud leisure noise
Atypical and high-yield: the calm infant whose parent renovates a 1950s house; the refugee child with prior industrial exposures not listed on any local housing form; the adolescent using high-volume headphones for hours; the toddler on a private well never tested for nitrates or microbes. [5] [6] [7]
Differential Diagnosis
Environmental exposure is often a contributor, not a solitary cause. Hold both truths: do not miss a remediable hazard, and do not attribute every developmental or respiratory problem to “toxins” without a coherent pathway. [2] [9]
| Presentation | Exposure-favouring clues | Key alternatives |
|---|---|---|
| Developmental/behavioural concern | Housing renovation, confirmed lead risk, methylmercury high-fish diet, pesticide access | Genetic/neurodevelopmental conditions, hearing loss, adversity, iron deficiency |
| Recurrent respiratory symptoms | Damp/mould, indoor combustion, traffic corridor housing | Viral infection, atopy, foreign body, aspiration |
| Abdominal pain / GI upset | Acute pesticide or metal ingestion history | Surgical abdomen, constipation, infection |
| Parental “heavy metal” worry | Social-media detox narrative, unvalidated urine tests | Anxiety, true lead risk that needs proper venous testing |
| Cluster of similar cases | Shared school, well, product or workplace | Coincidence, infectious outbreak |
Unvalidated provoked urine metal testing is a differential for the test, not the child. Chelating agents used before urine collection can raise metal excretion in people without clinical poisoning and lead families into unnecessary “detox.” Do not use these panels as paediatric standard of care. [11] [13]
Clinical & Bedside Assessment
Start with partnership, not accusation: “I ask every family about home, water and work because those details change how we protect learning and breathing.” Shame closes the story about renovation, traditional products or unstable housing. [1] [12]
A practical structure is CH2OPD2 (Community, Home, Hobbies, Occupation, Personal habits, Diet, Drugs/products). Walk the domains in under five minutes at a well visit; expand when risk appears. [12]
Five-minute environmental history (CH2OPD2)
Community
Traffic, industry, agriculture, school or childcare location, known local advisories.
Home
Age and condition of housing, renovation, damp/mould, heating/cooking fuel, pests and pesticide sprays.
Hobbies
Soldering, ceramics, shooting, art solvents, loud music or motorsports.
Occupation (caregivers)
Farm, demolition, battery, pest control, manufacturing — and whether clothes or dust come home.
Personal habits
Hand-to-mouth behaviour, pica, outdoor soil play, second-hand smoke/vape (air leaf for depth).
Diet and water
Private well versus municipal, fish intake pattern, imported foods or remedies.
Drugs and products
Medicines, traditional remedies, cosmetics (e.g. kohl/surma), plastic food heating habits if relevant.
Examine growth, development, skin, chest, abdomen and neurology as the presentation dictates. In acute toxicity, prioritise airway, breathing, circulation and conscious state over a perfect housing history. Always ask who else shares the environment — siblings, other children in care, pregnant household members. [7] [11]
Investigations
Test the hypothesis the history creates. There is no universal paediatric environmental blood panel. [11] [12]
Often useful when indicated: [5] [7] [13]
- Venous blood lead when housing, renovation, products or pica raise lead risk (see lead leaf for strata and chelation limits)
- Carboxyhaemoglobin when combustion exposure or CO risk is plausible (coordinate with air/poisoning pathways)
- Cholinesterase activity or specific toxicology when acute organophosphate/carbamate poisoning is suspected — with poison-centre guidance
- Targeted metals (e.g. mercury) only with a coherent exposure story, not as fishing expeditions
- Public-health environmental sampling of water, dust or air — often more informative than another blood tube
Usually not first-line in asymptomatic children: broad commercial urine metal panels, hair analysis marketed for “toxicity,” or post-chelation provoked collections. These confuse families and can delay real source control. [11] [13]
Private wells are a special investigation setting: municipal treatment rules do not automatically apply. AAP guidance emphasises testing for microbes, nitrates and local geologic contaminants (which may include arsenic in some regions) with a plan for treatment or alternative water when results fail standards. [5]
Management — Resuscitation
If the child is unstable, the environment still matters — but life support comes first. Remove the child from ongoing gas, vapour or chemical contact when safe for rescuers. Decontaminate skin and clothing for dermal agents. Call your poison centre early. [1] [7]
For severe pesticide poisoning, elemental mercury vapour illness, or multi-casualty product exposures, treat as a toxicologic emergency: ABCDE, monitoring, antidotes only under specialist protocols, and protection of other household members. Do not wait for a perfect laboratory confirmation before stopping exposure. [1] [7]
Management — Definitive & Stepwise
Definitive care is a ladder. Most children need only the lower rungs. [3] [12]
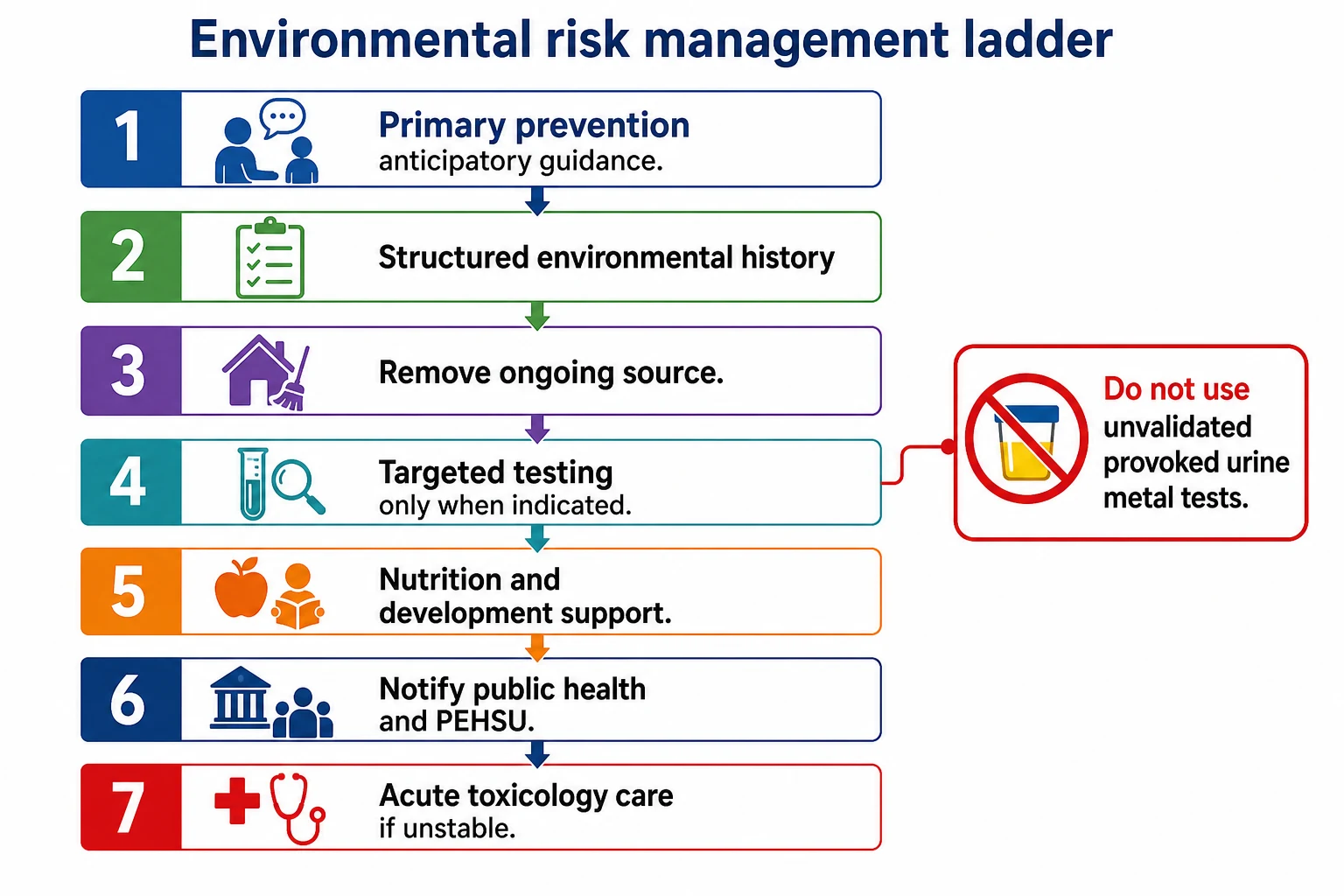
1. Primary prevention and anticipatory guidance. Age-band the advice. Infants: safer sleep environment free of combustion hazards and accessible chemicals. Toddlers: lock pesticides and medicines, wet-clean dust, hand washing after outdoor play. School-age and adolescents: noise protection, vaping/tobacco avoidance (air leaf), safer product choices. Farm families: integrated pest management (IPM), keep spray equipment and work clothes out of living spaces. [1] [6]
2. Source control is treatment. Stop unsafe renovation practices. Fix leaks and dry damp materials. Switch to safer pest control. Provide alternate water when a well fails testing. Relocate temporarily when the home cannot be made safe quickly. [5] [9] [13]
3. Targeted testing and clinical care. Order the right biomarker when it will change action. Treat coexisting iron deficiency when metal absorption is relevant. Support asthma plans when indoor air and dampness drive symptoms. [9] [13]
4. Development and nutrition. Early intervention referral, hearing checks after noise risk, and diet quality matter. Organic produce can lower some pesticide residues for families who choose and can afford it, but AAP guidance does not require organic food for a healthy diet — the priority remains a varied diet rich in fruits and vegetables, washed and prepared safely. [8]
5. Public health, PEHSU and poison centres. Report notifiable exposures and clusters. PEHSUs (US model) and analogous toxicology/environmental services elsewhere provide clinician consultation, education and case support. Use them for complex chronic exposure questions, unusual products and community incidents. [11] [12]
6. Follow-up. Recheck symptoms, development and any biomarkers on a written schedule after remediation. Document the source plan and who was notified. [11]
What each intervention actually achieves
- Stops ongoing dose
- Protects siblings and future pregnancies
- Essential before any 'detox' narrative
- Confirms selected exposures
- Guides public-health action
- Useless as a blind fishing panel
- Specialist interpretation
- Environmental investigation links
- Education for clinicians and families
Specific Subtypes & Scenarios
Renovation of older housing. Paint dust and lead risk dominate — use the lead leaf for BLL strata and chelation limits. Immediate actions: stop dry sanding, keep children away from work zones, wet cleaning, professional hazard control. [13]
Farm and pesticide exposure. Prefer IPM. Store concentrates locked and never in drink bottles. If acute poisoning is suspected, decontaminate and call poison services; do not induce emesis as a default. Chronic low-level concerns need exposure reduction and developmental surveillance, not panic panels. [1] [2]
Private well water. Ask every rural or peri-urban family. Test on a schedule appropriate to local geology and after floods or system changes. Nitrates matter for young infants; microbes matter for all ages; region-specific metals such as arsenic need local public-health interpretation. [5]
Dampness and mould. Visible mould and persistent damp associate with respiratory symptoms. The clinical priority is fix the moisture source and clean or remove damaged materials, not prolonged “mould toxin” blood testing. Relocate when housing cannot be dried. [9] [10]
Noise. Excessive noise can injure hearing across infancy to adolescence. Counsel on volume limits for personal devices, protection at motorsports and concerts, and quieter sleep environments for infants. [6]
Elemental mercury spill. Broken devices or cultural uses can vapourise mercury. Evacuate and ventilate per public-health guidance; never vacuum liquid mercury (it aerosolises). Specialist environmental clean-up and clinical assessment for vapour exposure. [7]
Built environment. Traffic proximity, safe play space, walkability and housing quality shape activity, injury risk, heat exposure and air quality. Clinic advice still helps; systems advocacy changes the default risk. [4] [14]
Consumer products and traditional remedies. Ask specifically about kohl/surma, imported remedies and unregulated cosmetics. Offer safer alternatives without cultural disrespect. [7] [13]
Complications & Pitfalls
Medical complications of uncontrolled exposures include lasting neurodevelopmental injury, chronic respiratory disease, hearing loss, acute toxicologic emergencies and, for some agents, longer-term cancer risk signals that drive policy even when individual counselling is about reduction, not certainty. [1] [6] [14]
Prognosis & Disposition
For many developmental toxicants, prevention is the prognosis. Once critical windows pass, partial recovery is possible through supportive care, but primary prevention protects more IQ points, airways and ears than late clinic visits. [3] [13]
Disposition follows control of the source and clinical severity: [7] [11]
- Asymptomatic with remediable risk: home with a written source plan and follow-up
- Ongoing uncontrolled hazard: lower threshold for temporary rehousing and public-health action
- Acute toxicity or unstable physiology: emergency department, poison centre, possible intensive care
Document what was found, what was fixed, who was notified, and when you will recheck. [12]
Special Populations
Fetus and infant. Placental transfer and high susceptibility windows make pregnancy and infancy priority periods for smoke-free homes, safe renovation practices and chemical storage. Some agents appear in breast milk; usually the benefits of breastfeeding still dominate — counsel agent-by-agent with specialist help when a high exposure is confirmed. [3] [7]
Children with disability or pica. More mouthing and floor time can raise dust and soil dose. Pair developmental care with environmental controls. [13]
Indigenous, migrant, refugee and socioeconomically disadvantaged families. Higher hazard clustering and less power to remediate housing. Use interpreters, non-blaming language and concrete service pathways. [4]
Rural and remote. Private wells, agricultural chemicals, delayed specialist access and different product availability. Telehealth can still deliver history and PEHSU-style consultation links. [5] [11]
Out-of-home care. Multiple residences mean multiple environments. Share the plan with every caregiver. [12]
Evidence, Guidelines & Regional Differences
Core AAP Council on Environmental Health (now Environmental Health and Climate Change) statements shape exam answers: pesticides (policy + technical report), chemical-management policy prioritising children, private wells, noise, built environment, mould spectrum, mercury technical report, organic foods clinical report, and climate policy (detail on the climate leaf). PEHSU literature describes a consultative network that multiplies clinician capacity. [1] [3] [4] [5] [6] [11]
Practice is often more risk-based than US universal lead timing. Environmental health officers, public health units and poisons information centres are the operational partners. Private wells and rural agricultural exposures are high-yield in some regions. Apply the same vulnerability and source-control principles; name local notification pathways rather than inventing US cut-offs. [5] [12]
Controversies to handle cleanly. Precautionary chemical policy versus cost-benefit regulation; organic food as residue reduction versus equity and nutrition balance; how far clinic counselling can go without housing policy. Your safe viva line: reduce what you can today, test what history justifies, escalate complex cases, and advocate for safer defaults. [3] [8]
Exam Pearls
ENVIRONS
If you remember only one chain: ongoing exposure in a developing child → dose during a critical window → lasting harm that late medicine rarely undoes. Break the exposure. That is the fellowship answer. [3] [13]
References
- [1]Council On Environmental Health Pesticide exposure in children. Pediatrics, 2012.PMID 23184103
- [2]Roberts JR Pesticide exposure in children. Pediatrics, 2012.PMID 23184105
- [3]Council on Environmental Health Chemical-management policy: prioritizing children's health. Pediatrics, 2011.PMID 21518722
- [4]Bole A The Built Environment and Pediatric Health. Pediatrics, 2024.PMID 38105697
- [5]Woolf AD Drinking Water From Private Wells and Risks to Children. Pediatrics, 2023.PMID 36995188
- [6]Balk SJ Preventing Excessive Noise Exposure in Infants, Children, and Adolescents. Pediatrics, 2023.PMID 37864408
- [7]Goldman LR Technical report: mercury in the environment: implications for pediatricians. Pediatrics, 2001.PMID 11433078
- [8]Forman J Organic foods: health and environmental advantages and disadvantages. Pediatrics, 2012.PMID 23090335
- [9]Committee on Environmental Health, American Academy of Pediatrics Spectrum of noninfectious health effects from molds. Pediatrics, 2006.PMID 17142549
- [10]Mazur LJ Spectrum of noninfectious health effects from molds. Pediatrics, 2006.PMID 17142508
- [11]Woolf AD An Update on Pediatric Environmental Health Specialty Units: Activities and Impacts, 2015-19. Academic pediatrics, 2024.PMID 38494060
- [12]Wilborne-Davis P A model for physician education and consultation in pediatric environmental health--the Pediatric Environmental Health Specialty Units (PEHSU) program. Pediatric clinics of North America, 2007.PMID 17306680
- [13]COUNCIL ON ENVIRONMENTAL HEALTH Prevention of Childhood Lead Toxicity. Pediatrics, 2016.PMID 27325637
- [14]Ahdoot S Climate Change and Children's Health: Building a Healthy Future for Every Child. Pediatrics, 2024.PMID 38374809