Paeds · preventive-and-community-paediatrics
Infant health supervision: birth to 3 months
Also known as Well-baby visits birth to 3 months · Infant well-child care 0–3 months · Early infancy health supervision · Postnatal infant checks · Bright Futures early infancy
Fellowship-level health supervision from hospital discharge through 3 months: visit structure, growth and feeding, examination, newborn screening loop-closure, immunisation, safe sleep, maternal mental health, red-flag triage and region-aware anticipatory guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A family brings a 10-day-old for a “check.” They want to know if weight is fine, if breastfeeding is enough, and when vaccines start. Your job is larger than a centile stamp. Early infancy is when jaundice peaks, weight bottoms out, milk supply is still establishing, sleep environments are set, and subtle congenital problems declare themselves. Health supervision in this window means planned visits that combine prevention, early detection and family support. [15] [5] [6]
Infant health supervision from birth to 3 months covers the period from hospital discharge through roughly 12–13 weeks of age. It includes the early post-discharge review (often day 3–5), the 1–2 week visit, the 1-month visit and the 2-month visit, plus opportunistic contacts. Frameworks differ by country — Bright Futures and the AAP periodicity schedule in the United States, personal health records and primary-care pathways in Australia and Aotearoa New Zealand, the Healthy Child Programme and NICE postnatal guidance in the UK, and tools such as the Rourke Baby Record in Canada — but the clinical tasks cluster the same way. [15]
This page owns ambulatory and medical-home preventive care in that age band. It links to dedicated pages for full immunisation schedules, safe-sleep depth, faltering growth algorithms and acute neonatal sepsis rather than hiding those whole chapters here. [15]
Classification
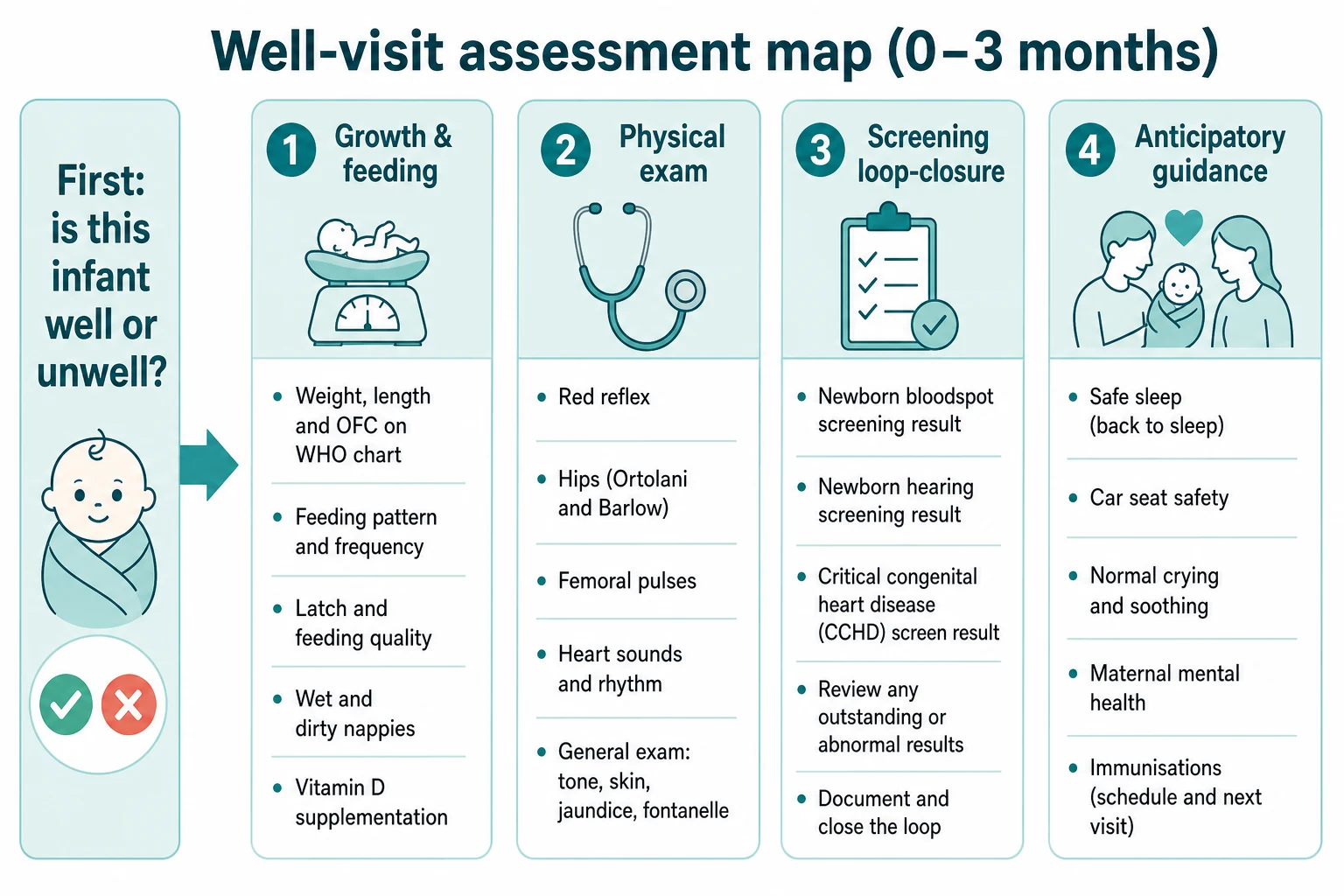
Classify the visit purpose and the infant state separately. [15]
Visit purpose. Newborn follow-up after discharge focuses on weight trajectory, feeding, jaundice and maternal recovery. The 1–2 week visit rechecks growth after the expected nadir and reviews screening results. The 1-month visit consolidates feeding, development and family stress. The 2-month visit adds routine immunisation in most national schedules and broader anticipatory guidance. Opportunistic visits fill gaps when families miss booked care. [15]
Infant state. [15]
- Well preventive — thriving, safe environment, screens closed or scheduled, caregiver coping.
- At-risk preventive — late-preterm, social vulnerability, borderline weight loss, incomplete screens, maternal mood concern — still outpatient capable with a tighter plan.
- Acutely unwell — physiology or trajectory unsafe; switch to ABCDE and acute pathways. [12] [11]
A useful end-of-visit problem representation names age and gestation, growth trajectory, feeding mode, screening status, immunisation status, caregiver wellbeing and the safety environment. [15]
Epidemiology & Risk Factors
Most term infants complete early well visits without hospitalisation. The high-risk tail is clinically important. Early readmissions cluster around jaundice, feeding failure with dehydration, infection and occasionally missed critical congenital heart disease. Late-preterm and early-term infants carry higher rates of feeding inefficiency, jaundice, hypothermia and parental exhaustion even when they left the nursery “well.” [5] [12] [15]
Social determinants change both disease risk and attendance. Food insecurity, unstable housing, domestic violence, limited transport and language barriers reduce timely review and increase unsafe sleep environments. Indigenous Australian and Māori/Pacific families experience inequitable infant outcomes in many datasets; culturally safe continuity, local workforce and non-judgemental counselling are part of clinical care, not optional extras. [15]
Sleep-related infant death risk is concentrated in the first months of life. Prone or side sleep, soft bedding, bed-sharing especially with parental smoking or impairment, and overheating remain major modifiable factors emphasised in 2022 AAP guidance. [1] [2]
Pathophysiology
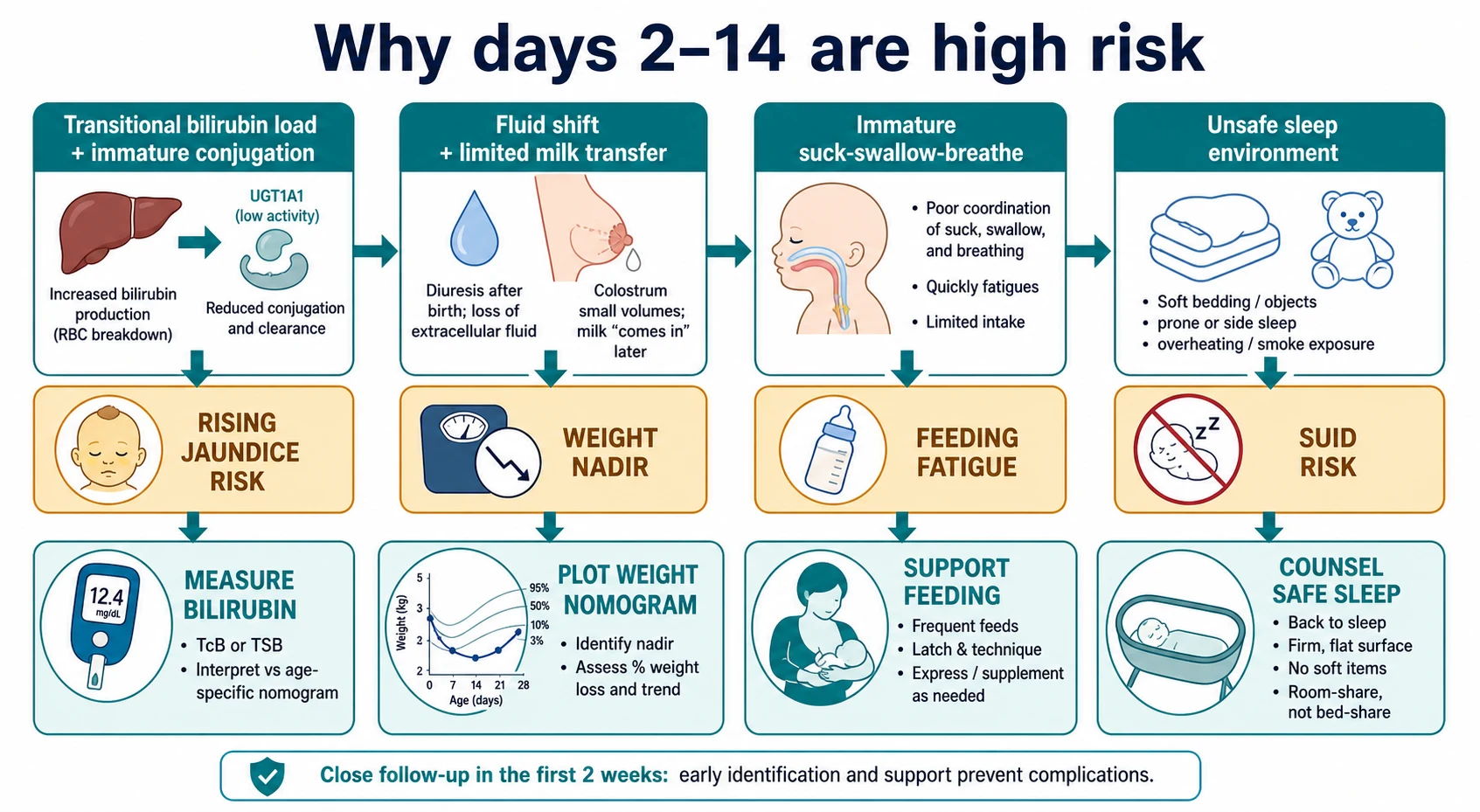
Why do the first two weeks punish small errors? [15]
After birth, the newborn’s bilirubin load rises as fetal red cells turn over and conjugation capacity is still maturing. Visual colour is a poor ruler; measured bilirubin plotted against age in hours drives decisions for infants ≥35 weeks in modern AAP-aligned pathways. [5]
At the same time, extracellular fluid is shifting and milk transfer may still be low while lactogenesis is establishing. Exclusive breastfeeding has a predictable early weight nadir. Nomograms help separate common trajectories from excessive loss that needs a feeding rescue plan rather than bland reassurance. [6]
Suck, swallow and breathe must coordinate. When coordination or stamina fails, feeds lengthen, volumes fall and energy is spent on work of breathing instead of growth. Infection and hypoglycaemia often declare as non-specific feed refusal before shock is obvious. [12] [11]
Unsafe sleep physiology is different but equally practical: rebreathing, impaired arousal and thermal stress interact with prone position and soft surfaces. Counselling targets those mechanisms with concrete environment changes. [1] [2]
Clinical Presentation
Thriving well infant. Alert periods, vigorous cry, coordinated suck, settling between feeds, frequent wet nappies, soft stools (especially if breastfed), and a caregiver who can describe a workable day-night pattern. [15]
Underfed or dehydrated infant. Long feeds with little swallowing, fewer wet nappies, dry mouth, lethargy, cool peripheries, and weight well below the expected early trajectory. Parents may say “he sleeps all the time” — sleepiness can be a danger signal, not a virtue. [6] [15]
Jaundice concern. Yellow skin or eyes, dark urine, pale stools (obstructive red flag), poor feeding, or a family history of significant neonatal jaundice. Measure rather than guess when risk or appearance worries you. [5]
Cardiorespiratory concern. Sweating with feeds, colour change, prolonged feeding with tachypnoea, weak femoral pulses, or a murmur with poor growth. Pulse-oximetry screening programmes aim to catch critical congenital heart disease before discharge, but some lesions still present later — do not assume a normal nursery screen closes the issue forever. [9]
Crying peaks. Many infants have evening fussiness that peaks around 6–8 weeks. Teach normal crying curves and never-shake messages. Still examine for hair tourniquet, corneal abrasion, otitis, fracture or other pain when the story or exam is atypical. [15]
Maternal mental health. Tearfulness, anhedonia, intrusive fears, or delayed bonding may appear while you weigh the baby. Perinatal depression is common enough that paediatric visits are a recognised detection opportunity. [7] [8] [14]
Differential Diagnosis
At a scheduled visit, keep a short threat list ready if the infant is not well: [15]
- Sepsis or serious bacterial infection. [12]
- Severe hyperbilirubinaemia risk. [5]
- Dehydration and hypoglycaemia from feeding failure. [11] [6]
- Critical congenital heart disease. [9]
- Non-accidental injury.
- Inborn error or metabolic crisis presenting as poor feeding.
For ambulatory concerns, separate: [15]
- Normal early weight loss versus pathological faltering. [6]
- Physiological jaundice trajectory versus pathological early, rapidly rising or prolonged jaundice. [5]
- Normal regurgitation versus red-flag vomiting (bilious, projectile progressive, blood, failure to thrive).
- “Colic” as a late label after pain, illness and safeguarding screens are negative.
- Latch or supply problems versus infant illness.
Clinical & Bedside Assessment
Run a repeatable sequence so you do not skip the quiet essentials. [15]
- Doorway impression and caregiver agenda. Who is worried, and about what?
- Interval history. Gestation, birth course, nursery problems, current feeds (type, frequency, duration, volume if measured), wet and soiled nappies, vomiting, colour, breathing, sleep place, smoke exposure, medications, family supports.
- Maternal wellbeing. Sleep, mood, pain, bonding, domestic safety. Use a validated perinatal depression screen when indicated and know your local referral path. [7] [8] [14]
- Growth. Naked weight when practical, length, head circumference. Same technique, same equipment culture, plot on WHO standards; correct for prematurity. Interpret the trajectory, not a single point. [6] [15]
- Examination. Undress the infant. Check tone, alertness, skin (jaundice, rash, bruises), red reflexes, palate, heart sounds, femoral pulses, abdomen, hips (Ortolani and Barlow with care and training), genitalia, spine, sacral signs, and primitive reflexes. Age-aware vital-sign norms matter if the infant looks unwell. [13]
- Feed observation when concern exists: latch, swallow cadence, fatigue, colour, caregiver handling. [17]
- Screening and immunisation status. Bloodspot, hearing, CCHD pulse-ox results, any pending referrals. [9]
- Anticipatory guidance and safety-net. Teach one or two high-yield topics deeply rather than a rushed checklist blur. Book the next contact explicitly.
Investigations
Most thriving infants at routine visits need no blood tests. Investigations are for a clinical question. [15]
Usually indicated when risk is present [15]
- Total serum bilirubin (or transcutaneous bilirubin with confirmatory serum when action thresholds approach) for jaundice concern or risk-based early follow-up. Plot against age in hours using the local implementation of modern hyperbilirubinaemia guidance for ≥35-week infants. [5]
- Point-of-care glucose when the infant is lethargic, jittery, hypothermic or feeding poorly. [11]
- Infection evaluation tailored to age and appearance when sepsis is plausible. [12]
- Pulse oximetry if cyanosis is suspected or screening was incomplete. [9]
Loop-closure investigations/results [15]
- Newborn bloodspot result documented or urgently chased.
- Hearing screen result and any diagnostic audiology pathway.
- CCHD pulse-ox screening documentation. [9]
Usually low yield [15]
- “Routine” labs in an asymptomatic, growing 2-month-old with a normal exam.
- Imaging without a specific indication (for example, do not ultrasound every click without following your local hip pathway). [15]
Management — Resuscitation
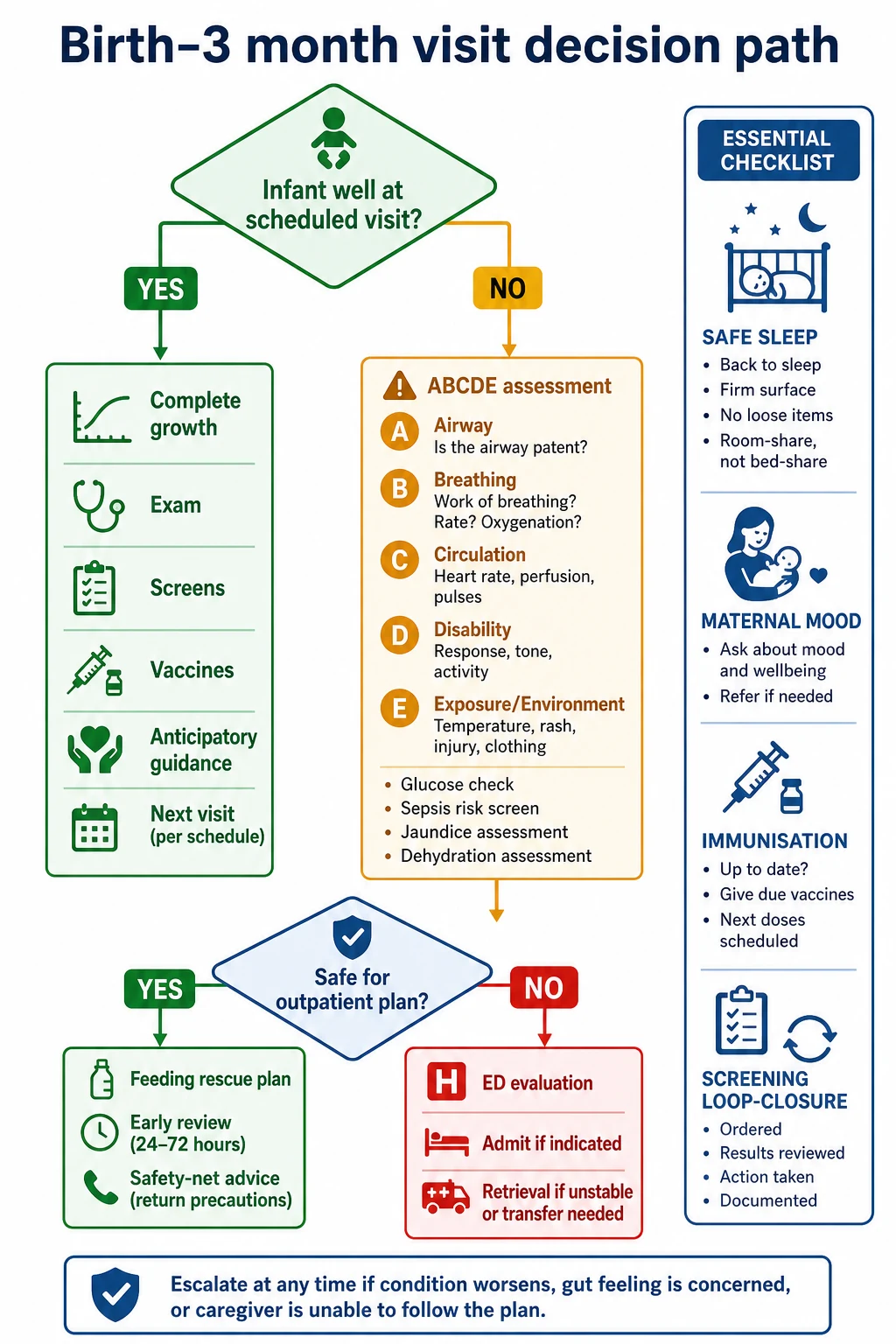
If the “well-child” infant is grey, floppy, poorly responsive or in respiratory distress, you are no longer in a preventive visit. [15]
- Call for help appropriate to your setting.
- ABCDE with oxygen and airway support as needed.
- Measure glucose and treat hypoglycaemia per local neonatal/infant protocol informed by ABM principles for at-risk neonates. [11]
- Obtain access, cultures and antibiotics on a sepsis pathway when indicated; do not delay for a perfect history. [12]
- Measure bilirubin urgently if severe jaundice is possible and escalate for phototherapy or higher-level care using age-based thresholds. [5]
- Arrange ED, ward or retrieval based on capability — not on the original appointment type.
Management — Definitive & Stepwise
For infants who remain outpatient-suitable, use a ladder. [15]
1. Growth and feeding plan
- Celebrate what is working.
- For breastfeeding: improve position and latch, increase effective sessions, consider short-term expressed milk, involve lactation support early, and define clear criteria for temporary supplementation and early reweigh. Primary-care breastfeeding support improves process reliability when systems are designed for it. [3] [4] [17]
- For formula: correct preparation, safe water, volume targets, and avoidance of over-dilution.
- Reweigh timing should match risk: sometimes 24–48 hours, not “see you at 6 weeks.”
2. Jaundice plan
- Measure when indicated, plot, treat, and recheck. Visual assessment alone is not enough when risk is material. [5]
3. Screening loop-closure
- Document results. Book missing hearing or bloodspot actions the same day. Explain why “pending” is not “normal.” [15]
4. Immunisation
- Offer vaccines at the nationally scheduled ~2-month visit unless a true contraindication exists. Mild intercurrent illness without significant fever is usually not a reason to cancel without counselling the delay risk. Use your jurisdiction’s handbook for exact antigens and ages (Australian Immunisation Handbook; UK schedule; US ACIP/AAP; Canadian schedules). [15]
5. Micronutrients
- Discuss vitamin D for exclusively or partially breastfed infants according to local product and dose guidance; bone-health policy statements support attention to vitamin D in early life. Do not invent a milligram figure from memory — use the current national recommendation in front of you. [10]
6. Safe sleep and home safety
Core 2022 AAP-aligned messages to teach with teach-back: [1] [2]
- Back to sleep for every sleep.
- Firm, flat surface designed for infant sleep.
- No soft bedding, pillows, loose blankets or inclined sleepers.
- Room-share without bed-share.
- Smoke-free environment.
- Avoid overheating; consider pacifier for sleep once breastfeeding is established if family chooses. [15]
Also cover rear-facing car restraints, water safety for baths, and smoke/carbon-monoxide alarms. [15]
7. Crying and never-shake
Explain normal crying peaks, caregiver relief plans, and that shaking is never safe. Offer concrete “put baby down and call someone” scripts. [15]
8. Maternal mental health action
Positive screens need a warm handover, not only a leaflet. Safety-net suicidal or infanticidal ideation as emergency psychiatry/ED pathways. [7] [8] [14]
9. Next contact
Write the date, the reason for earlier review if any, and after-hours instructions. [15]
Specific Subtypes & Scenarios
Day 3–5 weight check with ~10–12% loss. Assess hydration and alertness, observe a feed, support lactation, consider temporary supplementation criteria, reweigh soon, measure bilirubin if jaundiced or high risk. [6] [5]
Late-preterm sleepy feeder. Higher jaundice and readmission risk; lower threshold for feeding support and early review. [15]
2-month immunisation visit. Confirm growth trajectory, complete exam items still due, give vaccines, reinforce safe sleep as rolling approaches later, and check maternal mood. [15] [1]
Incomplete hearing screen. Treat as open loop until diagnostic testing is booked; do not wait for “maybe next time.” [15]
Mother with positive depression screen. Infant exam still matters, but adult mental-health action is part of paediatric duty of care in this context. [7] [8]
Bed-sharing family. Explore reasons (culture, housing, breastfeeding logistics). Counsel risk without humiliation; offer room-sharing alternatives and address smoking and impairment risks. [1]
Rural telehealth. Useful for counselling and some visual checks; inadequate alone when weight, hips, red reflex or illness assessment is required — arrange in-person completion. [15]
Complications & Pitfalls
- Reassuring large early weight loss without output and feed assessment. [6]
- Relying on visual jaundice alone. [5]
- Skipping red reflex, femorals or hips because “the baby looks fine.”
- Labelling all crying as colic.
- Leaving newborn screens as “probably done.”
- Deferring vaccines casually.
- Ignoring the mother’s mental health. [7]
- Mixed sleep messages that undo safe-sleep teaching. [1]
- Cultural or socioeconomic judgement that drives families away from care.
Prognosis & Disposition
Most well infants regain birth weight over the early weeks and settle into a growth channel. Disposition after a visit is a clinical decision: [15]
- Home with routine interval — thriving, safe, screens closed or scheduled, caregiver coping.
- Home with early review — borderline weight, feeding plan started, social risk, late-preterm.
- Same-day higher care — dehydration, significant jaundice thresholds, suspected sepsis, unsafe caregiver situation, or critical exam findings. [5] [12]
Longitudinal continuity in a medical home improves chance to complete vaccines, detect problems early and support the dyad through the peak crying weeks. [15]
Special Populations
Late-preterm and early-term infants need feeding and jaundice vigilance. [15]
Multiples need individual growth tracking and extra parental support. [15]
Infants of mothers with substance use or severe mental illness need safeguarding, feeding safety and coordinated adult services. [15]
Out-of-home and kinship care need record reconstruction for screens and vaccines. [15]
Post-NICU complex infants need handoff of oxygen, tubes, medications and red-flag plans into the community visit. [15]
Indigenous, migrant and refugee families need interpreter access, culturally safe communication and attention to housing and discrimination barriers. [15]
Socioeconomic disadvantage is a clinical risk factor for unsafe sleep and missed visits — address practically (local supports, transport, formula access when needed). [15]
Evidence, Guidelines & Regional Differences
Use state or national personal health records for visit timing. Follow the Australian Immunisation Handbook or New Zealand schedule for exact 6-week/2-month antigens. SIDS Safe Sleeping / national SUDI prevention messages align with back-sleeping, smoke-free and safe surface principles also emphasised internationally. [1] Local maternity and child-health nursing pathways often share early weight and feeding reviews with general practice and paediatrics.
Shared global principles: threat-first if unwell; measure jaundice rather than guess; plot early weight thoughtfully; close screening loops; counsel safe sleep; ask about caregiver mood; immunise on time. Operational ages, products and thresholds: always name the jurisdiction. [15]
Exam Pearls
- DWE/SAQ: structure a day-5 visit with 11% weight loss — assessment, feeding plan, bilirubin decision, reweigh timing. [6] [5]
- Short case: demonstrate red reflex and hip examination with running commentary.
- OSCE: safe-sleep counselling with teach-back and non-judgemental negotiation of bed-sharing. [1]
- Communication: disclose a positive maternal depression screen and make a warm handover. [7]
- Trap: calling a sleepy underfed neonate a “good baby.”
- Trap: postponing hearing follow-up because the infant “responds to the door slam.”
- Trap: inventing vitamin D or vaccine ages from memory instead of citing the local handbook. [10]
EARLY CHECK
References
- [1]Moon, Rachel Y Sleep-Related Infant Deaths: Updated 2022 Recommendations for Reducing Infant Deaths in the Sleep Environment. Pediatrics, 2022.PMID 35726558
- [2]Moon, Rachel Y Evidence Base for 2022 Updated Recommendations for a Safe Infant Sleeping Environment to Reduce the Risk of Sleep-Related Infant Deaths. Pediatrics, 2022.PMID 35921639
- [3]Meek, Joan Younger Policy Statement: Breastfeeding and the Use of Human Milk. Pediatrics, 2022.PMID 35921640
- [4]Meek, Joan Younger Technical Report: Breastfeeding and the Use of Human Milk. Pediatrics, 2022.PMID 35921641
- [5]Kemper, Alex R Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Pediatrics, 2022.PMID 35927462
- [6]Flaherman, Valerie J Early weight loss nomograms for exclusively breastfed newborns. Pediatrics, 2015.PMID 25554815
- [7]Rafferty, Jason Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics, 2019.PMID 30559118
- [8]Earls, Marian F Incorporating Recognition and Management of Perinatal Depression Into Pediatric Practice. Pediatrics, 2019.PMID 30559120
- [9]Mahle, William T Endorsement of Health and Human Services recommendation for pulse oximetry screening for critical congenital heart disease. Pediatrics, 2012.PMID 22201143
- [10]Golden, Neville H Optimizing bone health in children and adolescents. Pediatrics, 2014.PMID 25266429
- [11]Wight, Nancy E ABM Clinical Protocol #1: Guidelines for Glucose Monitoring and Treatment of Hypoglycemia in Term and Late Preterm Neonates, Revised 2021. Breastfeeding medicine : the official journal of the Academy of Breastfeeding Medicine, 2021.PMID 33835840
- [12]Shane, Andi L Neonatal sepsis. Lancet (London, England), 2017.PMID 28434651
- [13]Fleming, Susannah Normal ranges of heart rate and respiratory rate in children from birth to 18 years of age: a systematic review of observational studies. Lancet (London, England), 2011.PMID 21411136
- [14]Currie, Janet Screening for postpartum depression at well child visits: evaluating the impact of Michigan's statewide initiative. Health economics review, 2025.PMID 40855040
- [15]Turner, Kristy Well-Child Care: Newborns and Infants. FP essentials, 2025.PMID 40523122
- [16]Weitzman, Carol Promoting Optimal Development: Screening for Mental Health, Emotional, and Behavioral Problems: Clinical Report. Pediatrics, 2025.PMID 40850690
- [17]Kawan, Mary Improving breastfeeding care & support in a large, urban, pediatric primary care practice. Journal of pediatric nursing, 2023.PMID 36424329