Paeds · preventive-and-community-paediatrics
Lead exposure and poisoning prevention
Also known as Childhood lead poisoning · Blood lead level · Lead toxicity in children · Plumbism · Lead screening · Lead chelation · Environmental lead exposure
Fellowship-level approach to childhood lead exposure and poisoning prevention: no-safe-level principle, sources, screening and venous confirmation, CDC blood lead reference value, source removal, nutrition and development support, chelation thresholds, and regional practice differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Lead has no biological role in the child. Measurable blood lead, even at levels once called “acceptable,” links to lower IQ, attention problems and poorer school performance. Population blood lead fell after controls on petrol and paint, but residual hazards remain in housing, water, soil, consumer products and some traditional remedies or cosmetics. Your job is primary prevention first, then early detection and source control. [2] [5]
Lead exposure means contact that raises body burden. Lead poisoning (toxicity) usually refers to higher levels with illness that needs urgent medical care. Most modern paediatric cases are silent. The laboratory value alone never tells the whole story — the home, habits and developmental trajectory matter. [1]
Classification
Organise every case on three axes: how high the venous blood lead is, whether the child is symptomatic, and whether the source is still active. Those axes drive urgency, public-health action and whether specialist chelation is considered. [1] [2]
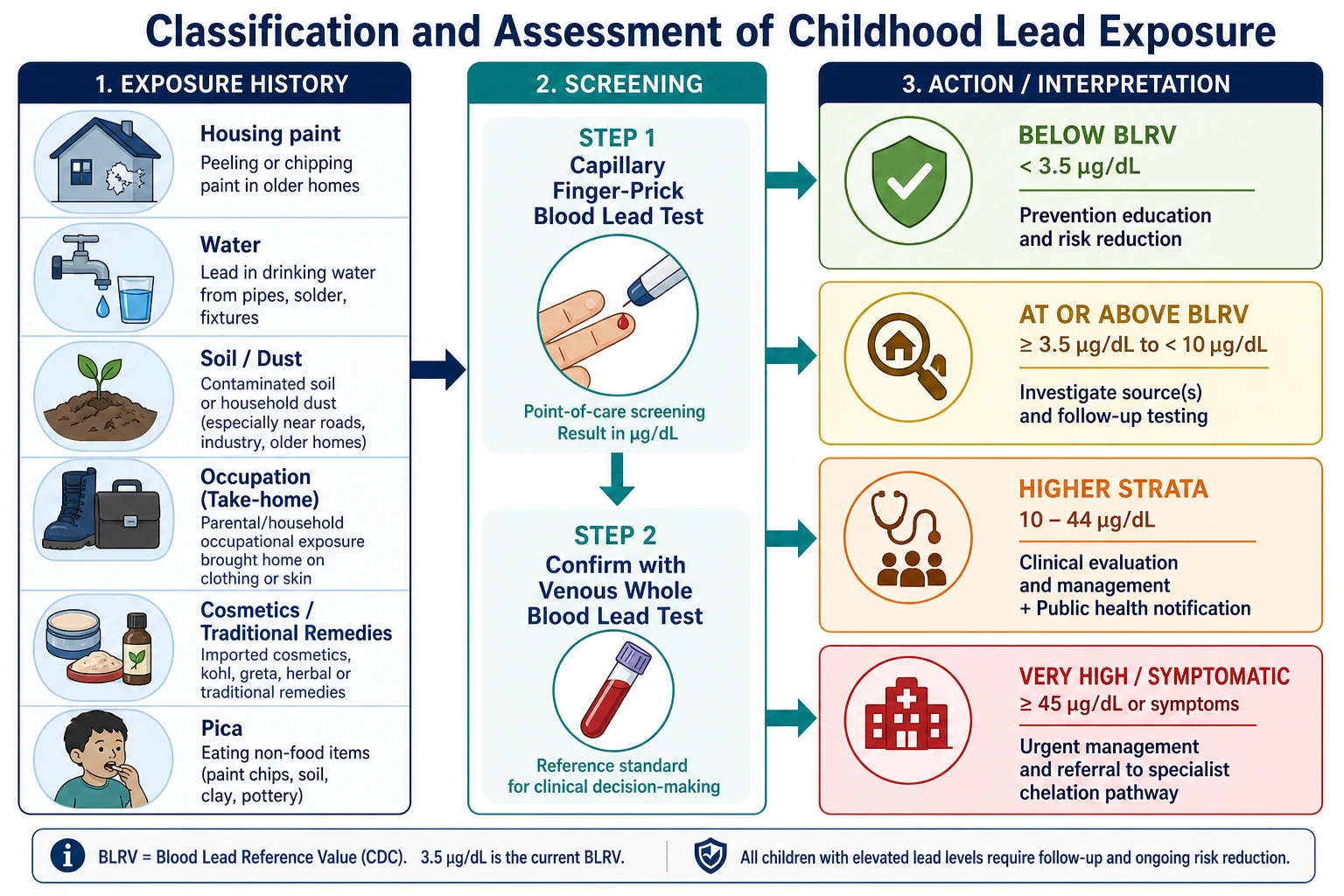
CDC blood lead reference value (BLRV). As of 2021, CDC uses 3.5 micrograms/dL as the BLRV for children. It is the approximate 97.5th percentile of the US childhood distribution. It is a population reference used to prioritise action, not a line between safe and toxic. Levels below the BLRV are not a guarantee of no harm. [2]
Practical clinical strata (US CDC-aligned actions, for exam fluency): [1]
| Confirmed venous BLL | Core response (summary) |
|---|---|
| Below BLRV | Prevention education; routine development and nutrition counselling; retest per local age/risk rules |
| At or above BLRV (e.g. 3.5–19 micrograms/dL band in CDC tables) | Education, exposure history, report as required, environmental investigation per jurisdiction, iron assessment, developmental surveillance, scheduled retest |
| Higher (e.g. 20–44 micrograms/dL) | Full clinical assessment, stronger environmental response, consider abdominal imaging if pica/ingestion suspected, specialist/PEHSU advice as needed |
| ≥45 micrograms/dL or symptomatic severe disease | Urgent specialist pathway; consider hospital admission and chelation with toxicology guidance; secure a lead-safe environment |
Use local public-health tables for exact retest intervals. Do not invent a home-country cut-off if your jurisdiction uses different operational numbers — state the principle and name the source you are following. [1] [14]
Epidemiology & Risk Factors
Population childhood blood lead has fallen over decades in high-income countries, yet inequity persists. Children in older housing, lower-income households and some racial and ethnic minority groups still carry higher risk. Housing with deteriorated lead paint and dust remains a dominant pathway where lead paint was historically used. [2] [11]
High-yield sources to ask about every time: [1]
- Deteriorated lead paint and house dust (especially renovation without safe work practices)
- Contaminated soil near old housing or industrial sites
- Drinking water via lead pipes, solder or fittings
- Take-home dust from battery work, smelting, demolition, shooting ranges, soldering or pottery with lead glaze
- Traditional cosmetics (surma/kohl) and some imported remedies or ceramics
- Pica for paint chips, soil or other non-food items
Outbreaks still occur. Informal processing of lead-rich ore for gold caused mass paediatric poisoning in Zamfara, Nigeria. Contaminated water systems (for example Flint) show how infrastructure failure becomes a paediatric emergency and a public-health story. [9] [12]
Pathophysiology
Children absorb a larger fraction of ingested lead than adults and explore the world with hands and mouths. Iron and calcium deficiency increase absorption, so nutrition is part of toxicology. Lead travels in blood, deposits in soft tissues and bone, and crosses the placenta. Bone stores can remobilise later, including during pregnancy. [1] [2]
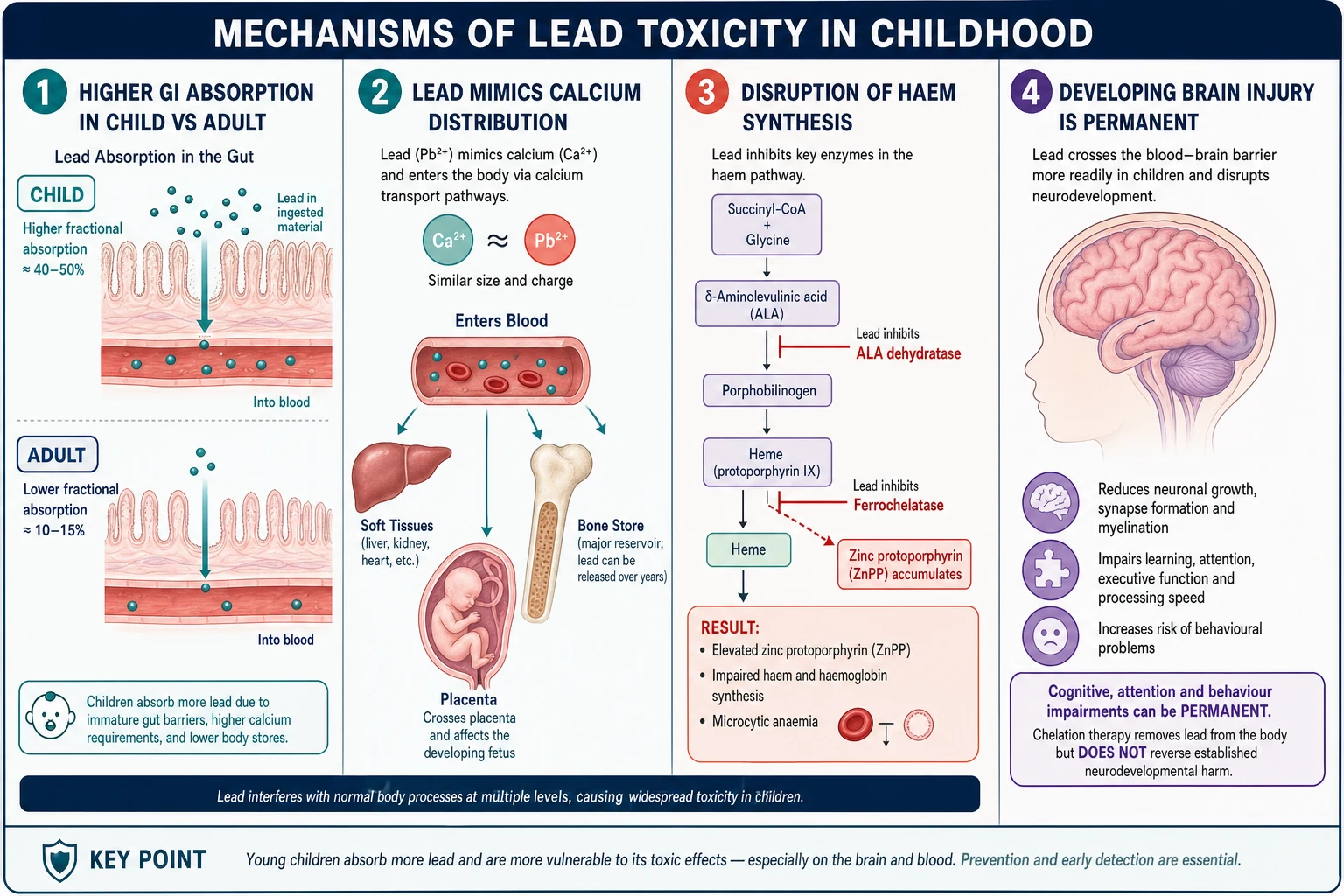
Lead inhibits ALA dehydratase and ferrochelatase in haem synthesis. That biochemistry explains microcytic sideroblastic anaemia patterns, basophilic stippling on the film, and elevated zinc protoporphyrin (ZPP), which integrates exposure over the red-cell lifespan. Neurotoxicity is the public-health core: synaptic and developmental disruption with lasting cognitive and behavioural effects. [1] [5]
Canfield and colleagues showed inverse IQ associations at blood lead concentrations below 10 micrograms/dL. Lanphear’s international pooled analysis strengthened the case for harm at low levels and a steeper slope at the lowest concentrations. That is why “wait until it is high” is the wrong preventive strategy. [4] [5] [10]
Clinical Presentation
Most children with elevated blood lead look well. The history often outruns the examination. Ask about housing age, peeling paint, recent sanding or renovation, water source, parental jobs and hobbies, imported cosmetics or remedies, and mouthing or pica. [1] [3]
When symptoms appear, they are non-specific until late: [1]
- Developmental plateau or regression, inattention, irritability or school difficulty
- Abdominal pain (lead colic), constipation, anorexia, vomiting
- Pallor from anaemia
- At very high levels: ataxia, seizures, altered consciousness, encephalopathy
Do not wait for wrist drop, gum lines or classic textbook signs. Those are late or uncommon in modern paediatric practice. The silent child in risky housing is the usual exam case. [1]
Differential Diagnosis
| Presentation | Lead-favouring clues | Key alternatives |
|---|---|---|
| Microcytic anaemia | Exposure history, basophilic stippling, elevated blood lead/ZPP | Iron deficiency, thalassaemia trait |
| Abdominal pain | Diffuse pain without peritonism, constipation, anaemia | Surgical abdomen, constipation alone, AIP |
| Developmental/behavioural concern | Housing risk, confirmed elevated BLL | Autism spectrum, ADHD, hearing loss, psychosocial adversity |
| Encephalopathy | Very high BLL, source history | Infection, metabolic disease, trauma, other toxins |
Acute intermittent porphyria can mimic lead with abdominal pain and neuropathy because both disturb the haem pathway. Lead typically elevates ALA with a different porphyrin pattern and comes with exposure history and haematological clues. Confirm with blood lead rather than debating enzyme lists at the bedside. [1]
Capillary contamination is a differential for the test, not the child. An elevated finger-prick result needs venous confirmation before you commit a family to major interventions. [1]
Clinical & Bedside Assessment
Start with a calm script: “We check for lead because it can affect learning even when children look well. Can we walk through where your child spends time?” Shame blocks disclosure of renovation work, traditional products or unstable housing. [1] [2]
Five-minute lead exposure assessment
Housing and renovation
Age of home, peeling paint, recent sanding or DIY, temporary housing or frequent moves.
Water and soil
Pipe materials if known, private well versus municipal supply, outdoor play areas and soil access.
Occupation and hobbies
Battery, smelting, demolition, ranges, soldering, pottery glazes — and whether work clothes come home.
Products and pica
Surma/kohl, sindoor, imported remedies, ceramics, paint chips, soil mouthing.
Child factors
Age under 6, iron deficiency risk, developmental status, siblings and other household children.
Plan and teach-back
Explain testing, what the number means, and the next environmental step in plain language.
Examine growth, development, blood pressure, pallor, abdomen and neurology. In an acute high-level presentation, prioritise airway, seizures and conscious state over perfect history-taking. Always ask who else lives in the same environment. [1]
Investigations
Venous whole blood lead is the confirmatory test that drives action. Capillary samples are useful for screening but overestimate when skin is contaminated. CDC tables set urgency for confirmatory venous sampling after an elevated capillary result — faster confirmation as the capillary value rises. [1]
Supportive tests when clinically indicated: [1]
- Full blood count and film (microcytosis, basophilic stippling)
- Iron studies (coexisting iron deficiency is common and treatable)
- ZPP/FEP as a chronic-exposure adjunct where available
- Renal function in higher-burden or symptomatic disease
- Abdominal X-ray if ingestion of paint chips or other radiopaque material is suspected
Do not order an extensive metabolic panel “for lead” in an asymptomatic well-child visit. The decision test is blood lead plus a real exposure history. [1] [3]
Management — Resuscitation
A child with lead encephalopathy or seizures is a time-critical emergency. Call for help. Protect the airway. Treat seizures with your local paediatric status pathway. Support circulation and glucose. Involve intensive care early. [1] [8]
For severe symptomatic poisoning, chelation is a specialist process. Contact a poison centre, paediatric toxicologist or PEHSU-equivalent service. Severe regimens historically combine agents in a defined sequence so that mobilised lead is not driven into the brain. Do not improvise multi-agent chelation from memory in an exam answer without naming specialist involvement. Secure a lead-safe environment in parallel — chelation without source control fails. [8] [9]
If imaging shows retained lead-containing material in the gut, plan bowel decontamination with specialist advice while preparing definitive therapy. [1]
Management — Definitive & Stepwise
Definitive care is a ladder. Most children never need the top rungs. [1] [2]
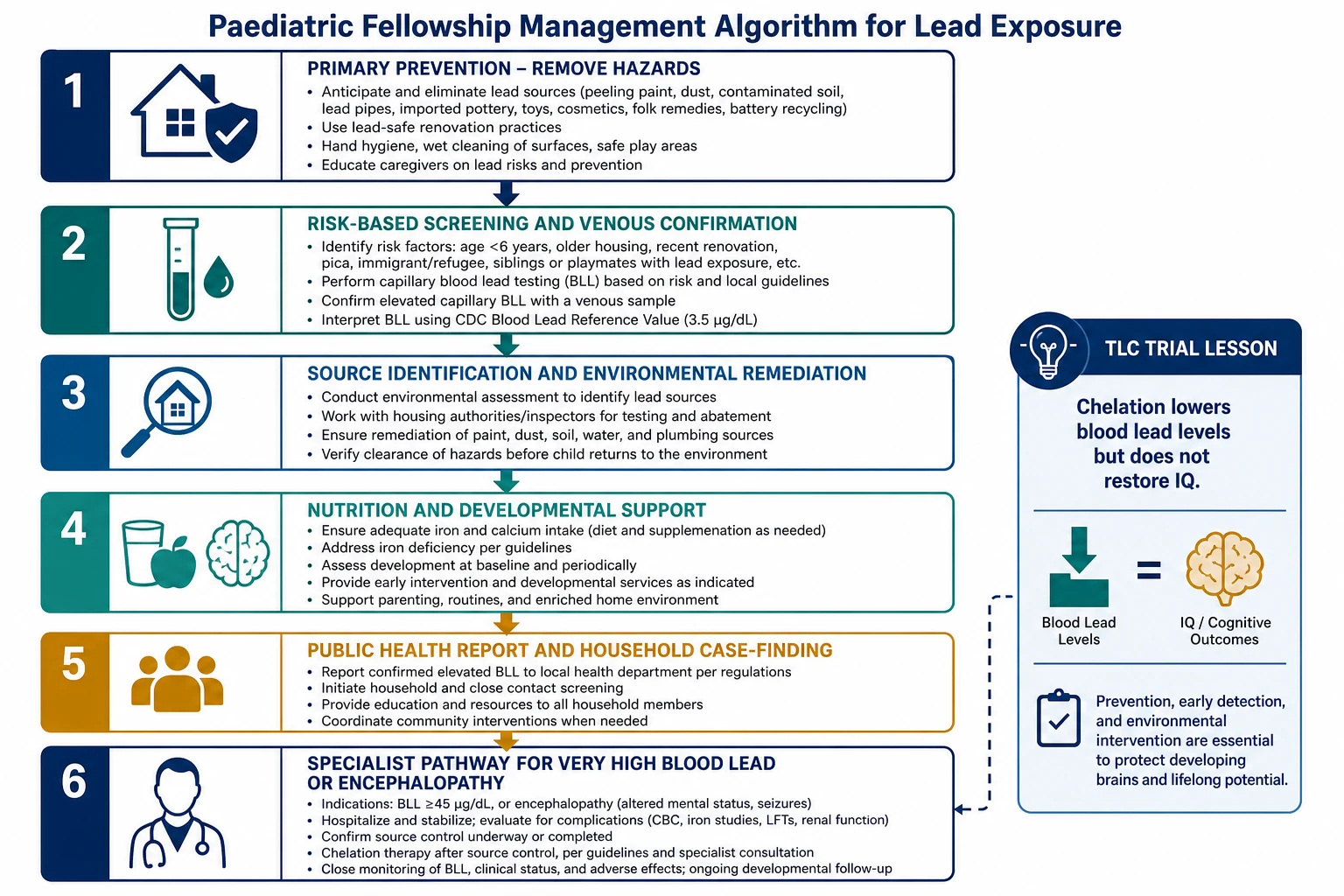
1. Primary prevention. Keep children out of lead dust. Use certified methods for paint hazard control. Avoid dry sanding old paint. Address water hazards through local plumbing programmes where they exist. Stop use of leaded cosmetics and contaminated remedies. Keep workplace lead off clothes and car seats. [2] [3]
2. Screening. Follow local public-health policy. In the US, Medicaid requires testing at 12 and 24 months (or later if never tested), and CDC supports targeted plans based on housing and demographic risk; without a local plan, universal testing is recommended. In many ANZ and UK settings, testing is more selective — but risk history still belongs in the well-child visit. [2]
3. Confirm and stratify. Convert elevated capillary results to venous whole blood lead on an urgency schedule. Interpret with symptoms and source status, not the number alone. [1]
4. Source identification and remediation. This is the treatment for almost every elevated level. Environmental investigation, interim controls (cleaning, relocation if needed), and durable hazard reduction protect the child and siblings. Never discharge a highly exposed child back to the same hazard without a plan. [2] [3]
5. Nutrition and development. Assess and treat iron deficiency. Discuss calcium-containing foods as part of diet support. Refer for early intervention and educational support when development is delayed. These steps do not replace source control. [1] [14]
6. Public health notification and household case-finding. Report according to local law. Test other young children in the same environment. [1]
7. Chelation (selected cases). CDC clinical guidance flags specialist consideration of chelation when venous BLL is ≥45 micrograms/dL, and urgent hospital care when symptoms of severe poisoning are present. Oral succimer (DMSA) is the usual paediatric option for many non-encephalopathic high-level cases; parenteral regimens are reserved for severe disease under toxicology guidance. Expect blood lead to fall, then partly rebound as bone stores redistribute — which is why environmental control must already be in place. [1] [6] [8]
What each intervention actually achieves
- Stops ongoing intake
- Protects siblings and future visits
- Essential before and after chelation
- Treats iron deficiency that raises absorption
- Links family to early intervention
- Does not detoxify lead by itself
- Lowers blood lead in selected high-level cases
- Can be life-saving in severe poisoning
- Does not reverse established cognitive injury (TLC)
Specific Subtypes & Scenarios
Asymptomatic toddler at or above the BLRV. Confirm venous level. Take a full exposure history. Arrange environmental follow-up as required. Optimise iron status. Recheck on schedule. Counsel without panic and without false reassurance. [1] [2]
Renovation dust. Old paint sanded without containment is a classic pathway. Stop unsafe work. Wet cleaning and professional abatement beat DIY dry sanding. [2]
Water and service lines. Use local water-authority guidance. Point-of-use filters certified for lead can be interim tools while infrastructure is fixed. Blood testing still matters because dust and paint may coexist. [12]
Traditional cosmetics and remedies. Ask specifically in families who may use surma/kohl, sindoor or certain Ayurvedic products. Offer lead-free alternatives without cultural disrespect. [1]
Take-home occupational lead. Shower and change at work if possible. Keep work clothes out of the child’s space. Test the worker and the children. [13]
Pica with possible paint ingestion. Consider abdominal X-ray. Decontaminate if radiopaque material is present. Treat the developmental and nutritional drivers of pica. [1]
Refugee or new-arrival child. Prior exposure settings may differ. Do not assume housing in the destination country is the only source. Screen according to local new-arrival pathways and clinical risk. [1]
Complications & Pitfalls
Medical complications include permanent cognitive and behavioural effects, anaemia, abdominal crises, nephropathy with high chronic burden, and life-threatening encephalopathy at extreme levels. Chelation itself can cause adverse effects and deplete essential metals; specialist protocols monitor for that. [1] [8]
Prognosis & Disposition
Cognitive injury from early lead exposure can persist. That is the prognosis fact that drives prevention policy. Population average blood lead can fall while individual children in hazardous housing still lose ground. [4] [5] [11]
Disposition follows severity: [1]
- Most asymptomatic elevated levels: home only if interim lead-safe arrangements exist, with public-health follow-up and retesting
- Higher levels or ongoing uncontrolled exposure: lower threshold for admission or temporary rehousing
- Encephalopathy or BLL in the specialist chelation range with symptoms: hospital, toxicology, intensive monitoring
Document the source plan, the retest date, developmental follow-up and who was notified. [1]
Special Populations
Infants and toddlers mouth surfaces and absorb more lead. Prioritise them for screening where risk exists. [2]
Pregnant persons and fetuses. Lead crosses the placenta. Maternal bone lead can remobilise. Reduce exposure and involve obstetric and public-health partners; chelation decisions in pregnancy need specialist advice. [1]
Iron-deficient children absorb more lead and need both nutritional care and source control. [1]
Indigenous, migrant, refugee and socioeconomically disadvantaged families face higher hazard clustering and less safe housing stock. Offer practical remediation pathways, interpreters and non-blaming communication. [2] [11]
Out-of-home care means multiple residences. Share the plan with every caregiver and the child-protection team when relevant. [1]
Evidence, Guidelines & Regional Differences
Core evidence includes Canfield (IQ effects below 10 micrograms/dL), Lanphear’s pooled analysis, AAP prevention policy, and the TLC randomised trial of succimer. Together they justify aggressive primary prevention and honest limits of chelation. [2] [4] [5] [6]
Australia and Aotearoa New Zealand do not copy US Medicaid universal timing as a single national rule for every child. Practice is more risk-based through primary care, public health and environmental health services. The clinical principles still hold: no safe level, exposure history, venous confirmation, source control, and specialist toxicology for severe cases. Use local public-health notification thresholds and environmental investigation pathways. [1] [2]
Controversies to handle cleanly. Universal versus targeted screening depends on local prevalence and housing stock. USPSTF has judged evidence for universal screening of asymptomatic children insufficient in some statements, while CDC and AAP still emphasise risk-responsive testing and action on low-level harm. Your viva answer: know your jurisdiction’s programme, take a risk history every time, and never call a low level “safe.” [1] [2] [14]
Exam Pearls
LEADSAFE
If you remember only one chain: ongoing exposure → rising body burden in a developing brain → lasting harm that drugs do not undo. Your job is to break the exposure. That is the fellowship answer. [2] [6]
References
- [1]Mayans L Lead Poisoning in Children. American Family Physician, 2019.PMID 31259498
- [2]COUNCIL ON ENVIRONMENTAL HEALTH Prevention of Childhood Lead Toxicity. Pediatrics, 2016.PMID 27325637
- [3]American Academy of Pediatrics Committee on Environmental Health Lead exposure in children: prevention, detection, and management. Pediatrics, 2005.PMID 16199720
- [4]Canfield RL Intellectual impairment in children with blood lead concentrations below 10 microg per deciliter. The New England journal of medicine, 2003.PMID 12700371
- [5]Lanphear BP Low-level environmental lead exposure and children's intellectual function: an international pooled analysis. Environmental health perspectives, 2005.PMID 16002379
- [6]Rogan WJ The effect of chelation therapy with succimer on neuropsychological development in children exposed to lead. The New England journal of medicine, 2001.PMID 11346806
- [7]Dietrich KN Effect of chelation therapy on the neuropsychological and behavioral development of lead-exposed children after school entry. Pediatrics, 2004.PMID 15231903
- [8]Kosnett MJ Chelation for heavy metals (arsenic, lead, and mercury): protective or perilous? Clinical pharmacology and therapeutics, 2010.PMID 20664538
- [9]Thurtle N Description of 3,180 courses of chelation with dimercaptosuccinic acid in children aged under 5 y with severe lead poisoning in Zamfara, Northern Nigeria: a retrospective analysis of programme data. PLoS medicine, 2014.PMID 25291378
- [10]Jusko TA Blood lead concentrations < 10 microg/dL and child intelligence at 6 years of age. Environmental health perspectives, 2008.PMID 18288325
- [11]Raymond J Childhood Blood Lead Levels in Children Aged <5 Years - United States, 2009-2014. MMWR. Surveillance summaries, 2017.PMID 28103215
- [12]Kennedy C Blood Lead Levels Among Children Aged <6 Years - Flint, Michigan, 2013-2016. MMWR. Morbidity and mortality weekly report, 2016.PMID 27359350
- [13]Kosnett MJ Recommendations for medical management of adult lead exposure. Environmental health perspectives, 2007.PMID 17431500
- [14]Centers for Disease Control and Prevention (CDC) Advisory Committee on Childhood Lead Poisoning Prevention Interpreting and managing blood lead levels < 10 microg/dL in children and reducing childhood exposures to lead: recommendations of CDC's Advisory Committee on Childhood Lead Poisoning Prevention. MMWR. Recommendations and reports, 2007.PMID 17975528