Paeds · preventive-and-community-paediatrics
Māori child health, Te Tiriti and culturally safe care
Also known as Māori child health · Te Tiriti o Waitangi paediatric care · Cultural safety Aotearoa · Hauora Māori children · Whānau-centred paediatric care · Kawa Whakaruruhau
Fellowship-level approach to Māori child health in Aotearoa New Zealand: Te Tiriti-informed practice, cultural safety versus competence theatre, Hui Process and Meihana-style engagement, equity pathways for SUDI, immunisation, ear health, skin infection and rheumatic fever, and regional contrasts with other indigenous frameworks.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
You will meet tamariki Māori in every setting — newborn clinic, ED, ward, school-linked services and rural outreach. The clinical diseases are familiar: otitis media, skin infection, incomplete immunisation, sleep-environment risk, respiratory illness, rheumatic fever risk. What changes the quality of care is whether you treat inequity as structural and service-designed, or as a story about families who “don’t engage.” [11] [18]
Te Tiriti o Waitangi is the founding constitutional relationship between Māori and the Crown in Aotearoa New Zealand. In health practice language, examiners expect you to operationalise principles such as partnership, active protection, equity/options, and participation — without inventing claim numbers or statute sections you cannot cite. Te Tiriti is not a cultural optional extra. It shapes how services are designed and how you share power in the room. [19]
Cultural safety (Kawa Whakaruruhau in the Ramsden lineage) is different from knowing a few facts about Māori culture. Safety is defined by the recipient of care. If a whānau leaves feeling diminished, stereotyped or unsafe, the encounter failed cultural safety even if your checklist looked complete. Curtis and colleagues argue that cultural competence language often keeps power with the clinician and underplays racism and equity. [1] [4]
Hauora Māori is broader than disease absence. Models of wellbeing used in Aotearoa (for example Te Whare Tapa Whā teaching in many services) keep taha tinana (physical), hinengaro (mental/emotional), whānau (family) and wairua (spiritual) in view. You still make biomedical diagnoses. You just refuse to pretend housing, racism, trust and identity are “non-medical.” [3] [11]
Classification
Start by sorting frameworks, not ethnic stereotypes. Three labels get confused in exams and in practice. [1]
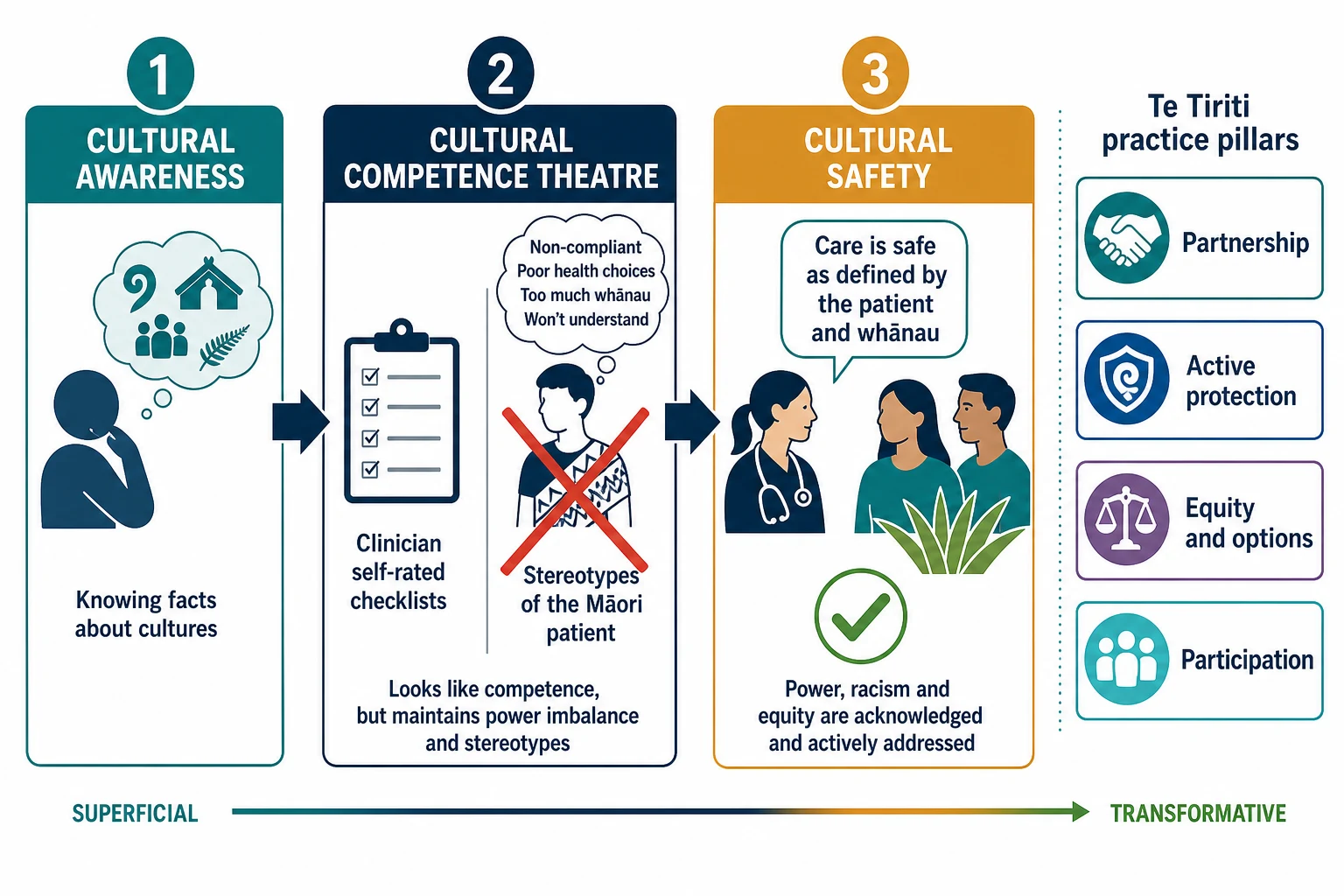
Terms you must not blur
- Knowing that cultures differ
- Necessary but not sufficient
- Can stop at trivia without changing care
- Clinician self-rates ‘skills with Māori patients’
- Risk of static checklists and stereotyping
- Often underplays racism and power
- Defined by patient/whānau experience
- Examines power, bias and system design
- Aims at equity of outcomes, not politeness alone
Also classify racism the way anti-racist health scholarship does: interpersonal (what is said or assumed in the room), institutional (policies, DNA processes, clinic hours, funding that systematically disadvantage), and structural (housing, income, colonisation’s long tail). A “did not attend” rate is often an institutional quality metric, not a cultural personality trait. [18] [19]
Finally, classify populations carefully. Māori and Pacific children both experience major inequities in Aotearoa, and programmes sometimes serve both. They are not interchangeable. Collapsing them into one “brown child” category fails epidemiology and fails respect. [14] [20]
Epidemiology & Risk Factors
Equity epidemiology for tamariki Māori is not one disease. It is a cluster of preventable burdens that reappear across decades of data: sudden unexpected death in infancy (SUDI) risk environments, immunisation lag at enrolment and early infancy, middle-ear disease and hearing inequity, skin infection, acute rheumatic fever (ARF) and rheumatic heart disease risk, respiratory illness, oral health and injury. Exact national percentages change by year and source; examiners reward mechanism and service response more than memorised tables you cannot verify. [5] [11] [12] [14]
Risk factors that matter clinically are mostly modifiable or service-addressable: crowded housing, smoke and vaping exposure, unsafe sleep surfaces and hazardous shared sleep, delayed primary-care enrolment, transport cost, clinic hours, prior racism, incomplete immunisation records, and untreated streptococcal skin or throat disease in high-incidence communities. [9] [10] [15] [17]
Protective factors include strong whānau connection, early trusted enrolment, breastfeeding support, smoke-free homes, culturally designed safe-sleep options such as wahakura or pēpi-pod programmes where available, and services that close loops rather than “offer and hope.” [7] [8] [17]
Primary-care scholarship in Aotearoa frames hauora Māori as a right to equal outcomes, not merely equal access on paper. That is the examiner’s north star when a stem asks “what does equity mean here?” [11]
Pathophysiology
Think of a cascade, not a cultural essence. Structural drivers (racism, poverty, housing, transport, distrust) increase exposures (smoke, hazardous sleep, delayed care, repeated infection). Those exposures become biology: immature arousal systems meeting unsafe sleep, middle-ear effusion impairing hearing and language, recurrent skin infection seeding invasive disease risk, and repeated group A streptococcal exposure contributing to ARF risk in susceptible children living in high-incidence settings. [6] [15] [18]
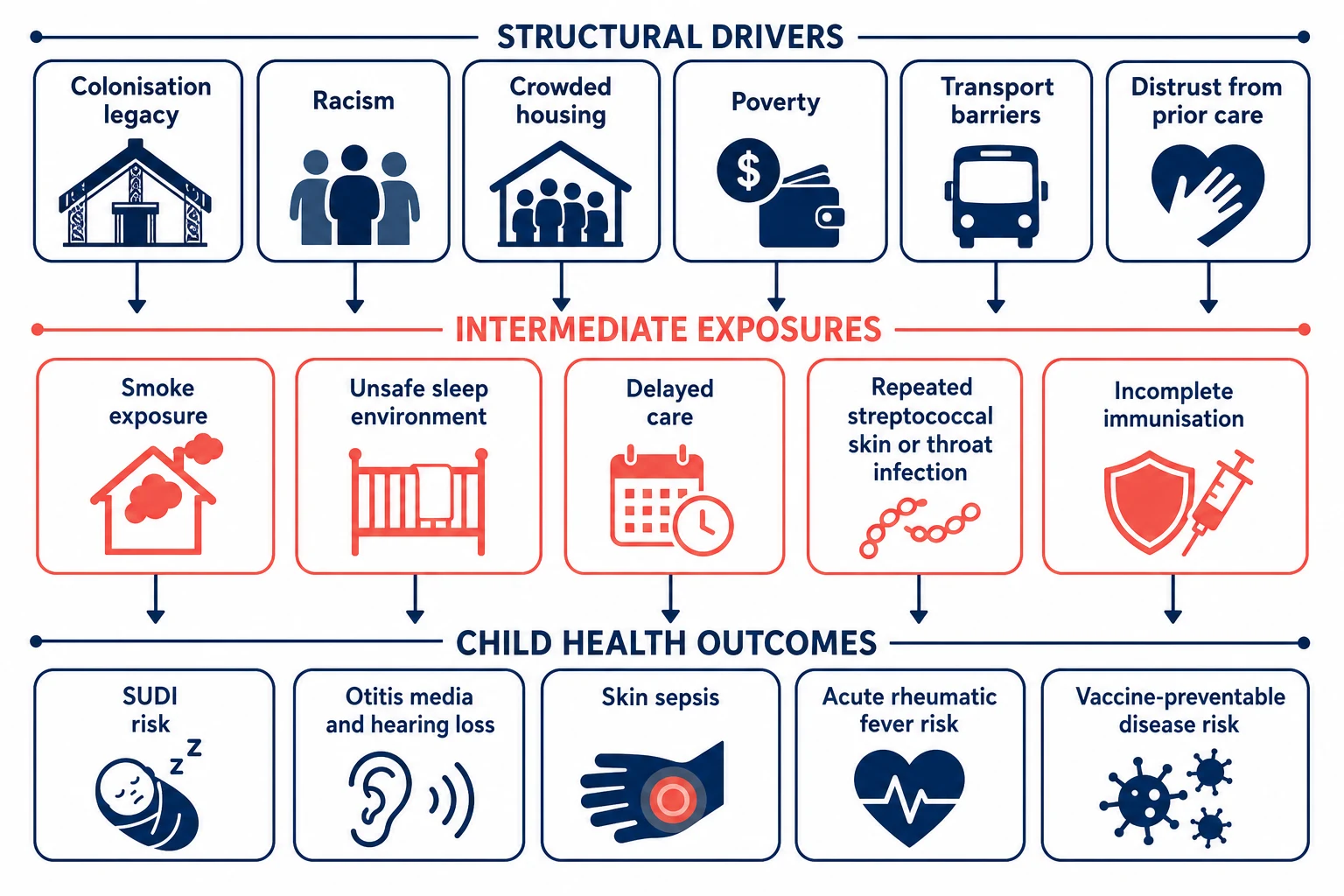
SUDI research in Aotearoa repeatedly links maternal smoking and sleep hazards with risk, including among Māori pēpē. That is not a claim that ethnicity causes death. It is a claim that hazards cluster and must be reduced without shame. [5] [6] [9] [10]
For ARF, pandemic-era analyses and programme evaluations support a practical pathophysiologic teaching point: superficial streptococcal disease burden (skin and throat) tracks with ARF incidence patterns. Mitigations that change infection pressure can change ARF rates. Your job is early recognition pathways and barrier-free treatment access in high-risk communities, not racialised fear of every sore throat in low-risk settings. [14] [15] [16]
Deficit pathophysiology is real too — in the relationship. If prior care was racist or dismissive, cortisol and trust are not metaphors. Families delay, withhold information, or avoid the service. That looks like “non-compliance” only if you stop thinking. [1] [18]
Clinical Presentation
In preventive care, inequity often looks ordinary: a six-week visit with no primary-care enrolment completed, an infant still sharing an unsafe sleep surface, a preschooler with recurrent otorrhoea, a school-entry hearing screen that never reached ENT, a child with impetigo returning three times, an adolescent who will not return after a rushed consult. [12] [17]
Whānau may present with prior harm. They might test whether you will stereotype. They might bring multiple supports. They might prefer te reo greetings, or not. Do not assume language, religion, iwi connection or traditional practice. Ask. [2] [3]
Acute presentations are the same life threats as for any child — sepsis from skin infection, respiratory failure, carditis in ARF, an infant found unresponsive. Cultural safety never delays airway and circulation. It runs in parallel: keep whānau informed, invite presence when safe, avoid accusatory language. [14]
Differential Diagnosis
The main differential is interpretive. [1]
| What you might say | Better formulation | Why it matters |
|---|---|---|
| “Non-compliant Māori family” | Barriers: transport, cost, hours, trust, prior racism | Changes the plan from blame to access design |
| “Cultural preference against vaccines” | Specific concerns + access friction + trust | Many incomplete schedules are logistics, not ideology |
| “Just glue ear, cultural speech delay” | Treatable middle-ear disease until proven otherwise | Hearing inequity is biomedical |
| “DNA = disengaged” | System DNA metric; call and rebook actively | Institutional quality, not ethnicity |
| “Safeguarding automatic / never” | Assess risk without racial over- or under-call | Bias harms children both ways |
Also separate primary immunodeficiency from recurrent infection driven by crowding and delayed care. Investigate red-flag immune patterns on merit. Do not miss organic disease because you over-attributed social context — and do not miss social context because you only ordered labs. [15]
Clinical & Bedside Assessment
Use a relationship-first structure. The Hui Process is a practical doctor–patient framework described for enhancing relationships with Māori: mihi (greeting/engagement), whakawhānaungatanga (making a connection), kaupapa (attending to the purpose of the visit), and poroaki (closing/transition). It is not theatre. It is clinical time spent so the real history appears. [2]
The Meihana model (Waikare o te Waka o Meihana) teaches dual assessment: standard clinical axes plus Māori beliefs, values and experiences that shape the problem and the plan. You still examine ears and chart growth. You also ask what supports exist, what previous care felt like, and who holds decision-making in this whānau. [3]
History that changes management: ethnicity recorded accurately (self-identified), primary-care enrolment, immunisation record source, housing and crowding, smoke/vaping, actual infant sleep practices, transport, food security, school attendance, hearing or speech concerns, skin infections, sore throats in high-RF regions, and who else cares for the child. [5] [10] [17]
Examination: full paediatric exam as indicated. For equity-linked conditions, do not skip ears, skin, growth, dentition and development. Observe interaction without pathologising normal multiperson whānau presence. [12]
Involve Māori health workers / kaiāwhina, reo support, and community providers early when wanted — not as a discharge afterthought. [11]
Investigations
Most equity work is not a rare test. It is doing the ordinary tests and actions without drop-off. [11]
- Verify immunisation status from the national/regional record, not memory. [17]
- After middle-ear disease or failed hearing screening (including B4 School Check pathways), ensure audiology/ENT follow-up actually happens. [12] [13]
- In high-ARF settings, use local sore-throat and skin-infection protocols; investigate possible ARF with the work-up your service uses when clinical criteria are met (do not invent a private Jones criteria variant in the exam). [15] [16]
- Document ethnicity completely and correctly; incomplete ethnicity data sabotages equity monitoring. [11]
What not to do: race-based diagnostic delay (“wait and see because this is common in Māori children”), shotgun race-based panels, or skipping organic work-up because you preferred a cultural narrative. [1]
Management — Resuscitation
If the child is critically ill, treat the physiology first. Call for help. Open the airway. Support breathing and circulation. Give oxygen, fluids, antibiotics and retrieval according to local paediatric emergency protocols. Cultural safety is how you work with whānau during that process, not a reason to pause adrenaline. [14]
Keep a calm narrative for caregivers. Invite presence at the bedside when safe. Avoid language that implies neglect while you still take a careful social history. If safeguarding concerns arise, use standard child-protection pathways without racialised over-calling or fearful under-calling. [18]
Management — Definitive & Stepwise
Prevention and ambulatory equity are the definitive work for most fellowship stems on this topic. [11]
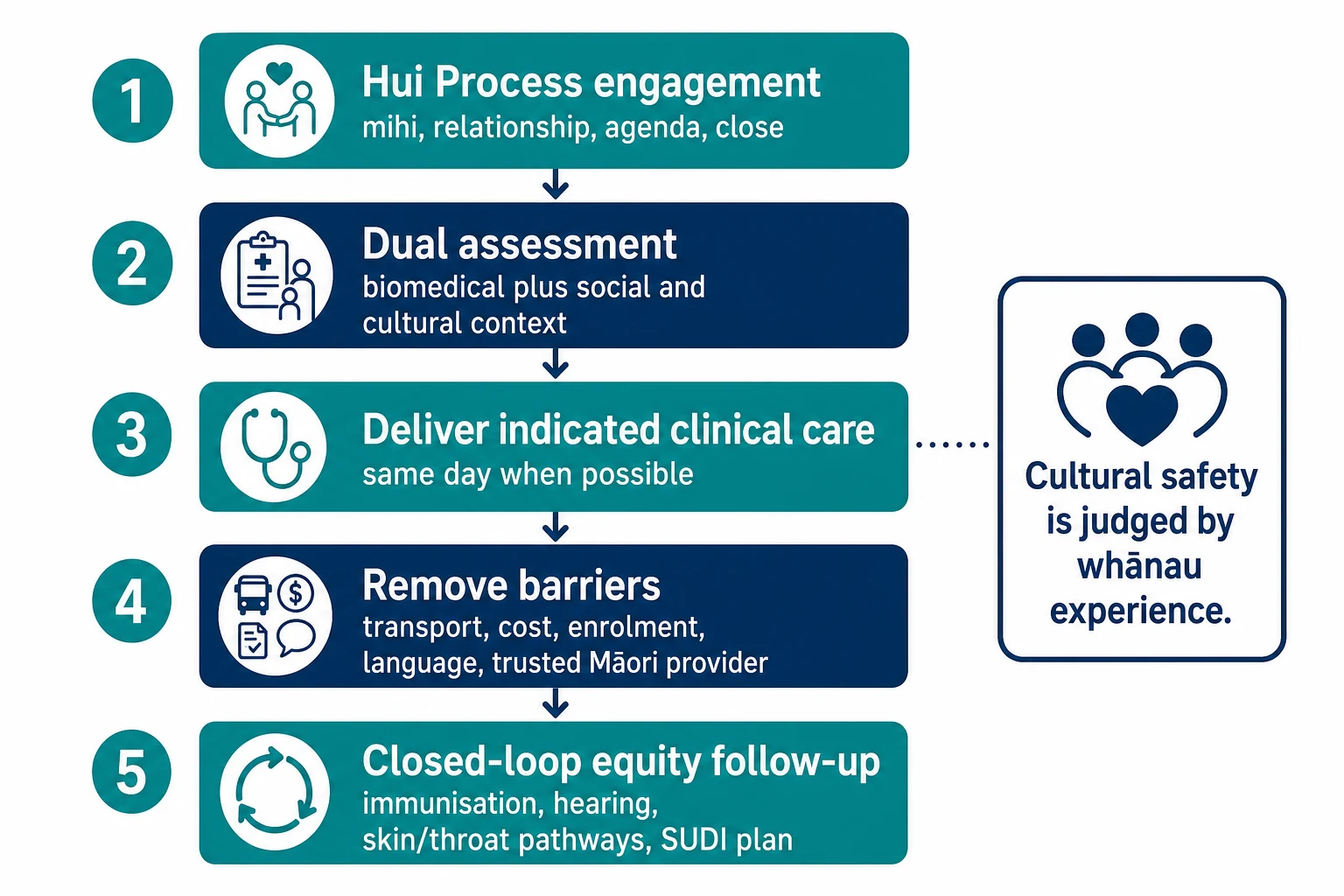
Five moves that change outcomes
Engage
Hui Process: greet, connect, set shared kaupapa, plan the close. Relationship is clinical, not optional polish.
Assess both axes
Biomedical diagnosis plus housing, smoke, sleep, transport, trust, whānau decision-makers and prior racism.
Treat today when you can
Immunisation catch-up, skin infection treatment, sore-throat pathway, hearing referral, safe-sleep plan — reduce return friction.
Design out barriers
Enrolment help, transport, flexible appointments, Māori provider options, written plan in plain language, teach-back.
Close the loop
Named follow-up owner, time frame, and what to do if the appointment fails. DNA is a system alert.
SUDI prevention in Māori pēpē. Teach supine sleep on a firm flat bare surface, room-sharing, smoke-free environment, and avoidance of sofas and hazardous shared sleep. Smoking in pregnancy and postnatal smoke remain central modifiable risks. Culturally designed devices such as wahakura are an Indigenous innovation to support safer sleep while enabling proximity; trial data support physiological stability in an indigenous sleep device setting, and programme literature describes wahakura as a safe-sleep vision that respects practice rather than shaming it. Still counsel on smoke and surface hazards. [5] [6] [7] [8] [9] [10]
Immunisation. Early enrolment and engagement drive completion. Provider perspectives highlight system friction at newborn enrolment. Offer same-day vaccination when valid, fix record errors, and partner with trusted community pathways. [17]
Ear and hearing. B4 School Check analyses show middle-ear disease and hearing inequity remain live problems. Ventilation-tube access has shown ethnic disparity patterns in Auckland data. Screening without treatment access is theatre. [12] [13]
Skin infection and ARF pathways. In high-incidence regions, treat skin infection early, use local sore-throat protocols, and link to public-health programmes. Observational and pandemic-related analyses connect streptococcal infection pressure with ARF patterns. Pacific ARF resurgence data also show equity work must be population-specific, not one blended message. [14] [15] [16] [20]
There is no single “Māori antibiotic dose.” Use standard paediatric dosing from your local formulary for the disease in front of you. Equity changes access and follow-through, not pharmacokinetics by ethnicity. [11]
Specific Subtypes & Scenarios
Newborn weeks. Complete enrolment, immunisation start, safe-sleep plan, smoke-free counselling, and a named primary-care home. Ask who else will care for pēpē overnight. [17] [5]
SUDI counselling with bed-sharing. Lead with partnership. Map actual hazards (sofa, smoke, alcohol, soft surface, preterm infant). Offer room-sharing and culturally designed bassinet options where available. Shame drives concealment. [6] [7] [9]
Recurrent otitis media. Treat acute disease, plan hearing follow-up, accelerate ENT when indicated, and fix transport barriers to appointments. [12] [13]
Skin infection in a high-ARF area. Treat thoroughly, review household transmission, safety-net for fever or joint symptoms, and know local ARF pathways. [15] [16]
Rangatahi. Negotiate confidentiality and whānau involvement explicitly. Intersectional identity (including gender and sexuality diversity) sits inside cultural safety, not outside it. [1]
Rural/remote. Time, travel and weather are clinical variables. Bundle care, use telehealth carefully, and never assume DNA means disinterest. [11]
Hospital racism disclosure. Acknowledge, apologise for harm where appropriate, fix the immediate care plan, and escalate systems issues. Do not defend the institution first. [18]
Complications & Pitfalls
Token mihi without changing appointment length, interpreter access, or follow-up ownership is recognised quickly by whānau and by examiners. [2]
Prognosis & Disposition
Prognosis at population level improves when hazards fall and services close loops — not when intention statements multiply. Disposition after a clinic visit should answer: Who owns the next step? When? What if transport fails? Is the child enrolled? Are immunisations booked? Is hearing follow-up real? Is the sleep plan concrete? [11] [12] [17]
Service metrics that matter: complete ethnicity data, time-to-treatment equity, DNA as a system quality signal, immunisation coverage gaps, hearing follow-up completion, and ARF prevention programme reach. [11] [14]
Special Populations
Disability and medical complexity. Cultural safety plus complex-care coordination; avoid diagnostic overshadowing.
Out-of-home care. Rights-based, trauma-informed care; know local care-and-protection interfaces without inventing statute numbers.
Urban and rural diversity. Māori are not a single cultural script.
Whānau language mix. Some prefer te reo, some English, some both — ask each visit.
Intersectionality. Poverty, disability, gender diversity and mental health co-travel with ethnicity; address all. [1] [3] [18]
Evidence, Guidelines & Regional Differences
Landmark practice anchors for this leaf: Curtis on cultural safety definition; Lacey Hui Process; Pitama Meihana model; MacFarlane/Mitchell/Tipene-Leach/Baddock on SUDI and wahakura; Sheridan on equal outcomes in primary care; Oliver/Seo on ear-health inequity; Bennett/Malcolm/Wright/Sonder on streptococcal disease and ARF equity patterns; Came on anti-racist health systems. [1] [2] [3] [7] [11] [12] [15] [18]
Controversies to handle carefully: bed-sharing debates (hazard-focused counselling beats culture-blaming); whether cultural competence training without power analysis helps or harms; how aggressively race-based ARF programmes should target without stigmatising. [1] [6] [14]
Exam Pearls
SAFE-I (equity visit checklist)
- Cultural safety ≠ cultural competence theatre. [1]
- Equal outcomes, not equal paperwork. [11]
- Smoking remains central in SUDI inequity discussions. [9] [10]
- Wahakura is innovation, not folklore decoration. [7] [8]
- Ear screening without treatment access fails equity. [12] [13]
- ARF work is infection pressure + access, not ethnicity as destiny. [15]
- Do not invent Waitangi Tribunal claim numbers in the exam.
- Keep Māori and Pacific analyses distinct even when programmes overlap. [20]
References
- [1]Curtis, E Why cultural safety rather than cultural competency is required to achieve health equity: a literature review and recommended definition International journal for equity in health, 2019.PMID 31727076
- [2]Lacey, C The Hui Process: a framework to enhance the doctor-patient relationship with Māori The New Zealand medical journal, 2011.PMID 22237570
- [3]Pitama, S Improving Maori health through clinical assessment: Waikare o te Waka o Meihana The New Zealand medical journal, 2014.PMID 24816961
- [4]Ramsden, I Cultural safety/Kawa Whakaruruhau ten years on: a personal overview Nursing praxis in New Zealand inc, 2000.PMID 11221309
- [5]MacFarlane, M Pēpē-infant sleep practices and sudden unexpected death in infancy in Aotearoa New Zealand International journal of gynaecology and obstetrics, 2021.PMID 34473352
- [6]MacFarlane, ME Infant Sleep Hazards and the Risk of Sudden Unexpected Death in Infancy The Journal of pediatrics, 2022.PMID 35120985
- [7]Tipene-Leach, D Innovation to prevent sudden infant death: the wahakura as an Indigenous vision for a safe sleep environment Australian journal of primary health, 2019.PMID 31513759
- [8]Baddock, SA Physiological stability in an indigenous sleep device: a randomised controlled trial Archives of disease in childhood, 2018.PMID 29030386
- [9]MacFarlane, M Smoking in pregnancy is a key factor for sudden infant death among Māori Acta paediatrica, 2018.PMID 29869345
- [10]Mitchell, EA Maternal Smoking, Vaping and Infant Sleep Practices in Sudden Unexpected Death in Infancy: A New Zealand Case Series Journal of paediatrics and child health, 2026.PMID 41834025
- [11]Sheridan, N Hauora Māori - Māori health: a right to equal outcomes in primary care International journal for equity in health, 2024.PMID 38413987
- [12]Oliver, T B4 School Check hearing screening and middle ear disease: a five-year analysis of prevalence and inequity The New Zealand medical journal, 2025.PMID 41264818
- [13]Seo, JY Persisting variance in middle ear ventilation tube insertion in Auckland children: why ethnic disparity continues The New Zealand medical journal, 2022.PMID 35728207
- [14]Wright, K The COVID-19 pandemic and acute rheumatic fever inequities, Aotearoa New Zealand, 2020-2022 The New Zealand medical journal, 2026.PMID 42348889
- [15]Bennett, J Pandemic mitigations reveal an association between superficial group A streptococcal infections and acute rheumatic fever incidence in Auckland New Zealand Emerging microbes & infections, 2025.PMID 40704453
- [16]Malcolm, J Rheumatic fever trends in the context of skin infection and Group A Streptococcal sore throat programmes in the Bay of Plenty: an observational study The New Zealand medical journal, 2025.PMID 39946567
- [17]Young, A Newborn enrolment, engagement, and immunisation in primary care: a qualitative study of healthcare providers' perspectives Journal of primary health care, 2026.PMID 42019944
- [18]Came, H Re-imagining anti-racist theory for the health sector The New Zealand medical journal, 2022.PMID 35728222
- [19]Came, H Equity, regulation and Te Tiriti o Waitangi: a rapid review of Putting Patients First The New Zealand medical journal, 2026.PMID 42096702
- [20]Sonder, GJ Resurgence of rheumatic fever among Pacific peoples in Aotearoa New Zealand: A 2010-2023 analysis of hospitalisation data with implications for equity Australian and New Zealand journal of public health, 2026.PMID 41447834