Paeds · preventive-and-community-paediatrics
Passenger, bicycle, pedestrian and firearm safety
Also known as Child passenger safety · Car seat safety · Booster seat counselling · Bicycle helmet safety · Pedestrian injury prevention · Firearm safe storage · Child access prevention · Road traffic injury prevention children
Fellowship-level anticipatory guidance for child passenger restraints, bicycle helmets, pedestrian safety and firearm safe storage: staged transitions, mechanism-based counselling, equity, acute injury response, and ANZ/UK/US practice differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Injury is not random noise around childhood. Most severe paediatric trauma still clusters around transport, wheels, roads and accessible lethal means. Your preventive job is to turn four high-yield domains into concrete, age-staged plans: passenger restraints, bicycle and wheeled-sport helmets, pedestrian behaviour and environments, and firearm safe storage. This page is about counselling and systems, not operating on a ruptured spleen — but the same mechanisms explain both clinic advice and the trauma bay. [1] [9] [11]
Child passenger safety means matching the child to the most protective restraint that still fits: rear-facing harness as long as possible, then forward-facing harness, then belt-positioning booster, then adult lap–shoulder belt, with rear seating for younger children. Bicycle safety is more than a slogan about helmets; helmets reduce head injury risk when a crash happens, while infrastructure and rider behaviour reduce crash opportunity. Pedestrian safety recognises developmental limits: most children under about 10 need adult supervision in traffic. Firearm safety for paediatric practice is harm reduction through storage and access counselling, not a political monologue. [1] [6] [9] [13]
Classification
Classify prevention the way examiners classify trauma: by mechanism domain, then by stage of protection. The four domains share one principle — energy transfer to a developing body — but the practical checklist differs. [2] [10] [12]
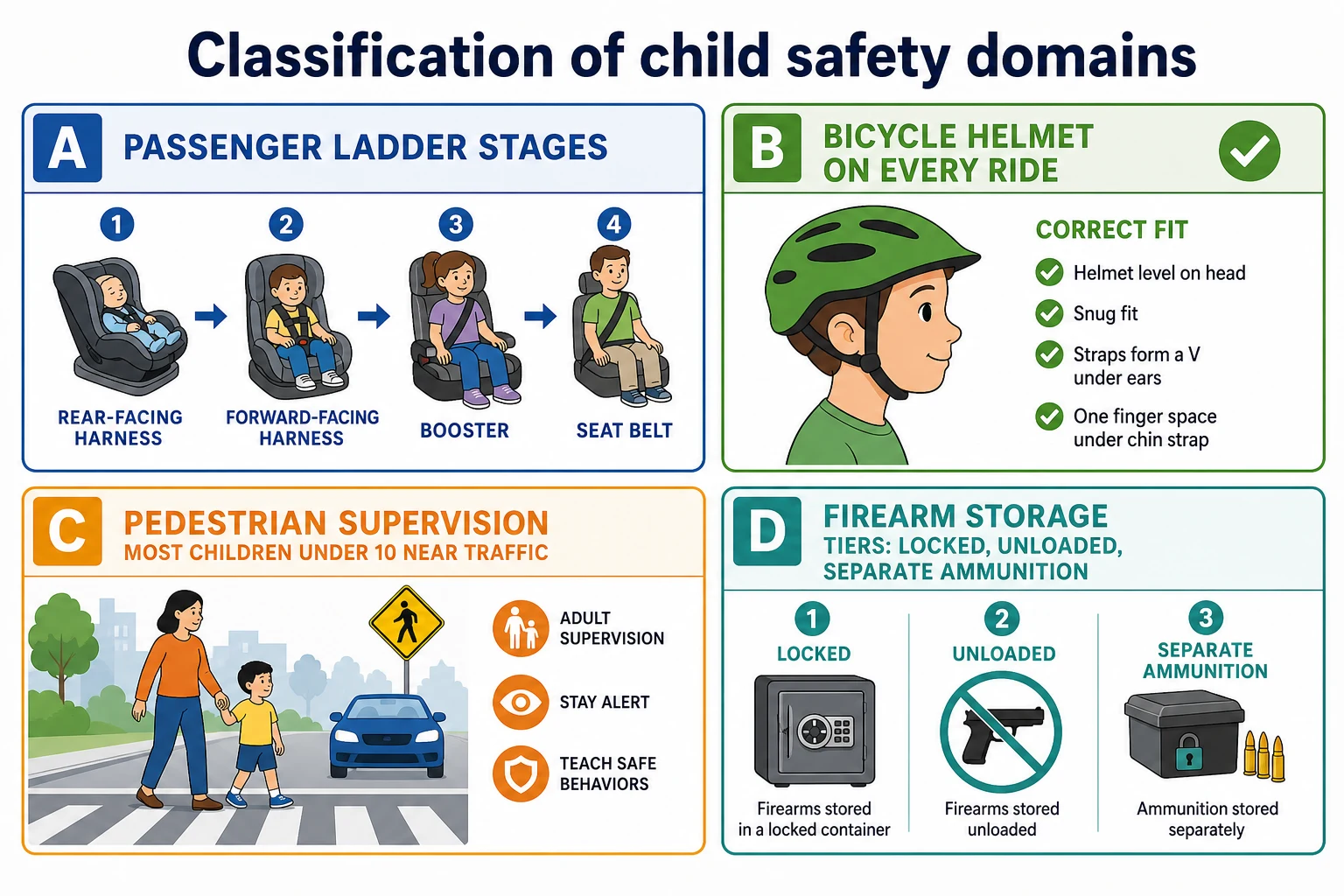
Four domains you must not blur
- Rear-facing → harness → booster → seat belt
- Fit and installation matter as much as product brand
- Rear seat preference for younger children
- Helmet correct fit and every ride
- Visibility, lights, traffic rules
- Helmet laws differ by region; efficacy of helmets remains
- Supervision for most under ~10 near traffic
- Driveway and dusk risks
- Built environment and distraction
- Locked, unloaded, ammunition separate
- Means counselling in suicide and IPV contexts
- CAP laws and regional legality vary
Within passenger safety, misuse is its own category: loose harness, wrong recline, expired seat, aftermarket products, and early graduation to the next stage. Early transition is not a developmental milestone — it is a reduction in protection. [1] [2] [17]
Epidemiology & Risk Factors
Road traffic injury remains a leading cause of severe paediatric injury and death globally. Within vehicles, unrestrained or incorrectly restrained children carry disproportionate risk. Premature movement out of rear-facing seats, harness seats or boosters is common and driven by convenience myths, peer pressure and incomplete clinician knowledge. [1] [2] [16]
Bicycle and wheeled-sport injuries cluster around head impact when helmets are absent or ill-fitting. Meta-analyses associate helmet use with substantially lower odds of head and serious head injury among injured cyclists. Mandatory helmet laws show population-level head-injury reductions, with ongoing debate about effects on cycling participation — your clinic message still remains helmet every ride for children. [6] [7] [8]
Pedestrian injuries rise with exposure, speed environments, poor lighting, driveway play, and adolescent distraction (phones, headphones). Inequity is structural: higher rates track neighbourhoods with less safe infrastructure. [9] [10]
Firearm injuries in children and youth include unintentional shootings, suicide, homicide and community violence. Household access and storage practices are the modifiable paediatric levers. Locked storage, unloaded status and separate locked ammunition each associate with lower risk of youth suicide and unintentional injury in case-control data. CAP-style laws that create liability for negligent storage associate with fewer paediatric firearm deaths in multi-state analyses. Absolute epidemiology differs sharply by country — ANZ and UK have far lower civilian firearm density than the US — but storage counselling still applies wherever firearms exist. [11] [12] [13] [14]
Pathophysiology
Injury prevention is applied biomechanics. A child’s head is relatively large, the cervical spine more mobile, the thorax more compliant, and the pelvis not yet shaped for adult belt geometry. In a frontal crash, a rear-facing restraint spreads crash forces across the back and reduces relative head excursion. A forward-facing harness distributes load through shoulders and pelvis. A booster lifts the child so the lap belt sits on the bony pelvis rather than the soft abdomen and so the shoulder belt crosses the mid-clavicle rather than the neck. [1] [2] [3]
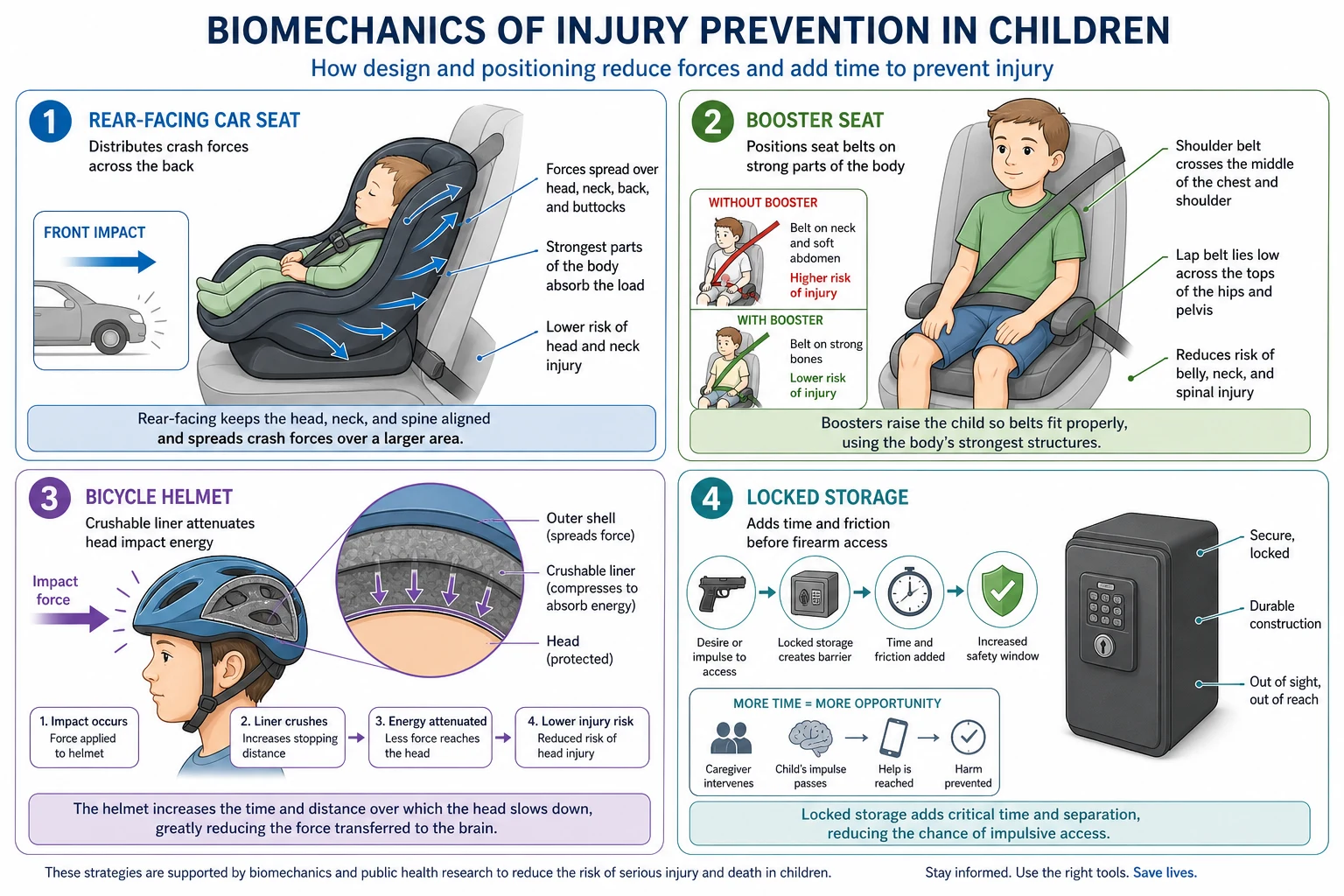
On a bicycle, kinetic energy at the head in a fall or vehicle collision is reduced by a properly fitted helmet’s crushable liner. Helmets do not make a child invincible; they change the probability and severity of brain injury when impact occurs. [6] [8]
Pedestrian injury severity rises steeply with vehicle speed and with limited visibility (dusk, dark clothing, driveways). Developmental patho-cognition matters: young children misjudge speed and gap acceptance and are easily distracted. [9] [10]
Firearm injury pathophysiology is lethality of mechanism. In suicide and unintentional shootings, seconds of access matter. Storage that adds time and friction between impulse and discharge is prevention. [11] [13]
Clinical Presentation
In clinic, families rarely present saying “please audit my restraint ladder.” They present for immunisation, school forms, asthma review — and you insert safety questions. Ask: What seat is your child in? Rear or forward facing? Can you show me a photo of the install? Helmet every ride? Who walks them across roads? Is there a firearm in any home where the child stays, including grandparents? [1] [16]
After injury, presentations range from minor soft-tissue wounds to multi-system trauma: unrestrained child ejected or with abdominal belt marks; cyclist without helmet and scalp laceration or reduced consciousness; pedestrian struck in a driveway; adolescent with gunshot wound or self-inflicted injury. History must capture restraint use, seating position, helmet, speed environment, and access to means without accusation. [18] [11]
Differential Diagnosis
For preventive visits there is no laboratory differential — the differential is which hazard is active today. For acute injury, do not let mechanism tunnel vision hide alternative or concurrent diagnoses: non-accidental trauma, medical syncope before a fall from a bike, intoxication in an adolescent pedestrian, or intentional injury framed as accidental. Firearm injury always requires trauma care first, then careful documentation and, where indicated, safeguarding and police pathways per local law. [11] [9]
Clinical & Bedside Assessment
Use a non-shaming inventory. “Lots of families graduate seats early because the child looks big — can we check fit together?” Observe if a car seat is visible in the clinic car park. For wheeled sports, ask about scooters and e-bikes as well as bicycles. For pedestrians, ask about the school route and driveway play. For firearms, ask every caregiver home, not only the primary address. [1] [11] [16]
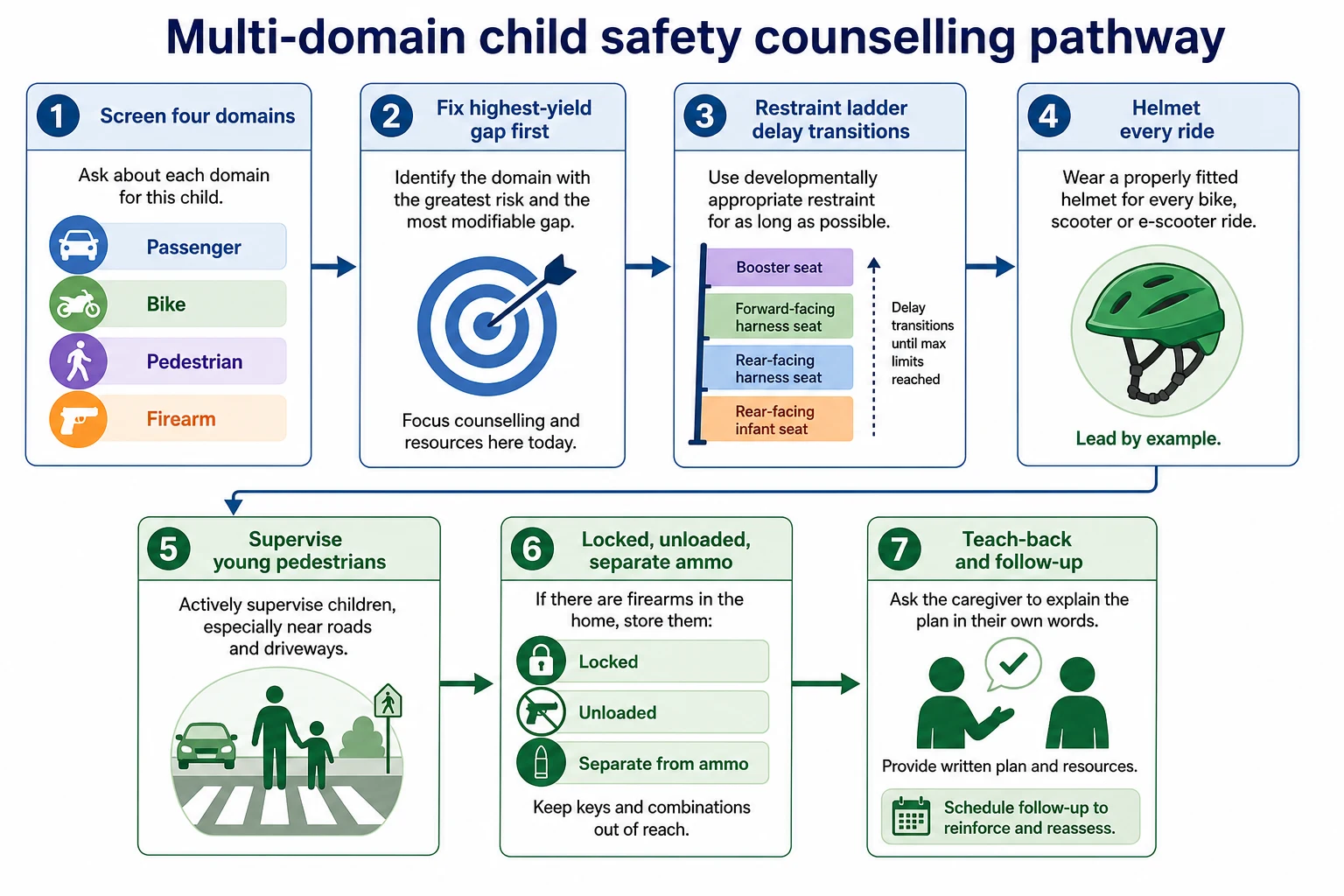
Five-minute multi-domain safety screen
Passenger stage
Identify current restraint stage, direction, harness fit, booster need, and rear-seat position; note premature transitions.
Installation reality
Ask about ISOFIX/LATCH vs belt install, tightness (less than an inch of movement at the belt path), and expired or second-hand seats.
Wheels and helmet
Helmet every ride for bike, scooter and similar; check fit — level, snug straps, two-finger rule under chin.
Walking and roads
Supervision plan under ~10 years, driveway rules, dusk visibility, phone-free crossing for older children.
Firearm access
Any gun in homes the child visits? Locked, unloaded, ammunition separate? Escalate storage counselling if suicidal ideation or IPV risk.
Teach-back
Ask the caregiver to restate the next single change they will make this week and document it.
Assess social context: multiple caregivers, rideshare and taxis, out-of-home care placements, disability seating needs, and language access. Complex equipment (wheelchair tie-downs, specialised restraints) needs occupational therapy or certified technician partnership rather than improvised clinic advice. [1]
Investigations
Well-child safety counselling needs no labs or imaging. The investigation is history, demonstration, and sometimes referral to a certified child passenger safety technician or local injury-prevention service. Document advice and barriers. [1] [16]
After major trauma, investigation follows ATLS/APLS and local trauma protocols: primary survey, imaging for mechanism and physiology, and forensic/safeguarding documentation when injury and history conflict. Do not invent a “car seat blood test.” [18]
Management — Resuscitation
For the injured child, mechanism does not replace ABC. Unresponsive or unstable patients need paediatric trauma activation, airway protection, haemorrhage control, spinal precautions when indicated by mechanism, and rapid transfer pathways. Firearm wounds require simultaneous trauma care and scene/safety awareness for staff. Preserve clothing and document wounds carefully when forensics may matter, without delaying life-saving care. [11] [18]
Support caregivers during resuscitation. Avoid early blame about missing helmets or seats; you can still document facts. If an unlocked firearm remains at home and siblings are present, address immediate environmental safety as part of disposition planning. [11] [13]
Management — Definitive & Stepwise
Prevention is the definitive “treatment” for this topic. Anchor passenger advice on the AAP 2018 algorithm and compatible national messaging (Kidsafe/state rules in Australia; RoSPA and national regulations in the UK). Laws set minimums; best practice often keeps children in each stage longer. [1] [2]
Passenger restraints (best-practice ladder) [1] [2]
- Rear-facing harness as long as the seat’s height/weight limits allow — longer is better; do not turn forward solely because the child turns 1 or 2. [1] [17]
- Forward-facing harness until the child outgrows harness limits — often well beyond early preschool years. Harness systems outperform seat belts alone for young children. [1] [4]
- Belt-positioning booster until the adult lap–shoulder belt fits: lap belt low on hips/upper thighs, shoulder belt mid-chest and mid-shoulder, knees bend at seat edge with feet down. Boosters substantially reduce injury risk versus seat belts alone in school-age children. [1] [3]
- Vehicle seat belt only when fit criteria are met. [1]
- Rear seating for children younger than 13 years when vehicle design allows. Never place a rear-facing seat in front of an active airbag. [1]
- Correct installation and harness tightness; avoid bulky coats under harnesses; replace seats after moderate/severe crashes per manufacturer guidance. [1]
Bicycle and wheeled sports [6] [7] [8]
- Helmet every ride, correctly fitted, replaced after a significant impact. [6]
- Lights, reflective gear, and route choice for school travel. [6]
- Counsel on e-bikes/scooters with age-appropriate supervision and local law. [6]
- Know your jurisdiction’s helmet legislation, but do not let law debates dilute the individual-protection message. [7]
Pedestrian safety [9] [10]
- Adult accompaniment for most children under about 10 in traffic environments. [9]
- Active modelling: crosswalks, eye contact with drivers, no mid-block darting. [9]
- Driveway and reverse-vehicle rules for toddlers/preschoolers. [9]
- Adolescent counselling on distracted walking and dusk travel. [9]
- Support environmental advocacy (speed reduction, safe routes to school) when relevant. [10]
Firearm safety [11] [12] [13]
- Ask about presence of firearms in homes the child frequents. [11]
- Recommend locked + unloaded + ammunition stored locked and separate. [13]
- In suicidal ideation, depression, or IPV, escalate to immediate means restriction and crisis pathways. [11]
- Frame as child safety and harm reduction; avoid shaming owners who are ready to store safely. [11]
- Know local reporting and CAP-style legal contexts without overclaiming law outside your jurisdiction. [14] [15]
RIDESAFE
Specific Subtypes & Scenarios
Newborn discharge. Rear-facing seat installed before leaving hospital; never leave infant unsupervised in a car seat outside the vehicle for routine sleep. [1]
Toddler who “hates” the harness. Do not graduate early for behaviour. Fix fit, trip planning, and caregiver consistency. [1]
School-age booster refusal. Demonstrate belt fit test; peer norms matter — enlist school messaging when available. Booster benefit is real. [3]
Adolescent drivers and passengers. Seat belts every trip; no front seat for younger siblings; discuss night driving and distraction as separate but related injury topics. [1] [18]
Cyclist without helmet after minor crash. Treat injuries, then use the teachable moment for fit and replacement. [6]
Driveway backover concern. Supervision, cameras/sensors as adjuncts only, and no play behind vehicles. [9]
Household with firearms and a depressed teen. Immediate lethal-means counselling: temporary off-site storage preferred; if not, locked unloaded separate ammunition with keys inaccessible to the youth. [11] [13]
Rideshare/taxi travel. Portable restraints or careful planning; never accept “it’s only a short trip” without a restraint. [1]
Complications & Pitfalls
Other pitfalls: second-hand seats with unknown crash history; aftermarket strap clips that undermine harness geometry; clinician under-confidence leading to no advice at all; and assuming low firearm prevalence means zero counselling in ANZ/UK when rural hunting firearms still exist. [16] [11]
Prognosis & Disposition
Population prognosis improves when restraint use, helmet use, safer speeds and secure storage rise. For an individual well-child visit, disposition is home with a specific next change, written or linked resources, and follow-up of barriers (cost of a seat, no helmet, housing with shared firearms). After injury, disposition follows trauma severity plus a prevention plan before discharge when feasible. [1] [6] [14]
Special Populations
Indigenous and socioeconomically disadvantaged families may face cost and housing barriers. Link to subsidy schemes for restraints and helmets; prioritise the single highest-yield fix. [9]
Migrant and refugee families need interpreters and demonstration, not translated jargon alone. Restraint laws and road norms may differ from country of origin. [1]
Disability and complex care. Specialised seating, medical equipment in vehicles, and behavioural challenges require OT/technician collaboration; do not abandon the protection ladder. [1]
Out-of-home care and multiple households. Every caregiver and every vehicle needs the same stage-matched plan; written instructions travel better than verbal advice. [1]
Youth justice and family violence contexts. Firearm access and community violence risk require trauma-informed storage and safety planning alongside safeguarding. [11]
Evidence, Guidelines & Regional Differences
The operational spine for passenger safety is the AAP 2018 policy and technical report, updating earlier algorithms and emphasising delayed transitions and rear seating under 13. Booster and harness effectiveness data (Arbogast and colleagues) underpin the middle of the ladder. [1] [2] [3] [4] [5]
Helmet protection is supported by Cochrane-era synthesis and contemporary meta-analysis; helmet legislation meta-analyses show head-injury reductions with ongoing policy debate. [6] [7] [8]
Pedestrian guidance is updated in the AAP 2023 policy and technical report, stressing supervision, distraction, equity and environmental design. [9] [10]
Firearm prevention guidance is updated in the AAP 2022 policy and technical report, with storage evidence from Grossman and CAP-law analyses from Azad and earlier Cummings work. [11] [12] [13] [14] [15]
Australian and New Zealand practice combines legal minimum restraint ages/heights (jurisdiction-specific) with Kidsafe-aligned best practice: keep children in each stage longer when the seat allows. Bicycle helmet use is widely legislated. Civilian firearm ownership is tightly regulated relative to the US, but safe storage remains mandatory messaging for licensed owners and rural households. [1] [7] [11]
Controversies to handle cleanly. Exact age cut-offs differ between law and best practice — exam-safe answer: follow local law as the floor, AAP-style stage-and-fit as the ceiling of protection. Helmet law debates about cycling rates do not erase helmet efficacy in a crash. Firearm counselling is harm reduction for children, not a referendum on ownership. [1] [7] [11]
Exam Pearls
If you remember only one chain: unmatched protection stage or open access to lethal energy → preventable paediatric injury. Your counselling restores the match and adds friction to access. That is the fellowship answer in one sentence. [1] [13]
References
- [1]Durbin DR Child Passenger Safety Pediatrics, 2018.PMID 30166368
- [2]Durbin DR Child Passenger Safety Pediatrics, 2018.PMID 30166367
- [3]Arbogast KB Effectiveness of belt positioning booster seats: an updated assessment Pediatrics, 2009.PMID 19841126
- [4]Arbogast KB An evaluation of the effectiveness of forward facing child restraint systems Accident Analysis & Prevention, 2004.PMID 15094411
- [5]Durbin DR Child passenger safety Pediatrics, 2011.PMID 21422094
- [6]Olivier J Bicycle injuries and helmet use: a systematic review and meta-analysis International Journal of Epidemiology, 2017.PMID 27450862
- [7]Hoye A Recommend or mandate? A systematic review and meta-analysis of the effects of mandatory bicycle helmet legislation Accident Analysis & Prevention, 2018.PMID 30173006
- [8]Thompson DC Helmets for preventing head and facial injuries in bicyclists Cochrane Database of Systematic Reviews, 2001.PMID 11966086
- [9]Kendi S Child Pedestrian Safety Pediatrics, 2023.PMID 37337837
- [10]Kendi S Epidemiology and Prevention of Child Pedestrian Injury Pediatrics, 2023.PMID 37337844
- [11]Lee LK Firearm-Related Injuries and Deaths in Children and Youth: Injury Prevention and Harm Reduction Pediatrics, 2022.PMID 36207776
- [12]Lee LK Firearm-Related Injuries and Deaths in Children and Youth Pediatrics, 2022.PMID 36207778
- [13]Grossman DC Gun storage practices and risk of youth suicide and unintentional firearm injuries JAMA, 2005.PMID 15701912
- [14]Azad HA Child Access Prevention Firearm Laws and Firearm Fatalities Among Children Aged 0 to 14 Years, 1991-2016 JAMA Pediatrics, 2020.PMID 32119063
- [15]Cummings P State gun safe storage laws and child mortality due to firearms JAMA, 1997.PMID 9315767
- [16]Zonfrillo MR Pediatricians' self-reported knowledge, attitudes, and practices about child passenger safety The Journal of Pediatrics, 2014.PMID 25195160
- [17]Bull MJ Rear-facing car safety seats: getting the message right Pediatrics, 2008.PMID 18310211
- [18]Smola C Child passenger safety education in the emergency department: teen driving, car seats, booster seats, and more Injury Epidemiology, 2020.PMID 32532359