Paeds · preventive-and-community-paediatrics
Rural, regional and remote child-health inequities
Also known as Rural child health inequities · Remote paediatric care access · Regional paediatric workforce and retrieval · Rural-urban child health disparities · Geographic inequity in paediatric care
Fellowship guide to rural, regional and remote child-health inequities: remoteness classification, workforce and distance mechanisms, paediatric readiness, telehealth and retrieval decisions, medical-home models, farm and water injury prevention, and ANZ/UK/US/Canada system differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
R.U.R.A.L. decision frame
Overview & Definition
Picture a toddler with fever in a small town ED at 02:00. The nearest paediatric ward is hours away. The family has already driven past two closed clinics. Your first job is still ABC. Your second job is different from the tertiary floor: you must decide what this place can safely do tonight, who can help by video, and when the retrieval clock starts. [3] [6]
Rural, regional and remote child-health inequities are unfair, avoidable differences in child health opportunity and outcomes linked to place. They include harder access to primary and specialty care, thinner preventive coverage, higher injury risk in some environments, and worse outcomes when emergency systems are not paediatric-ready. [1] [3] [7]
This page owns the geographic equity frame, disposition logic, shared-care models and rural-specific prevention. Deep telehealth examination technique, retrieval pharmacology detail, and Indigenous culturally safe care have dedicated leaves — cross-link them rather than hiding second textbooks here. [9] [12]
Classification
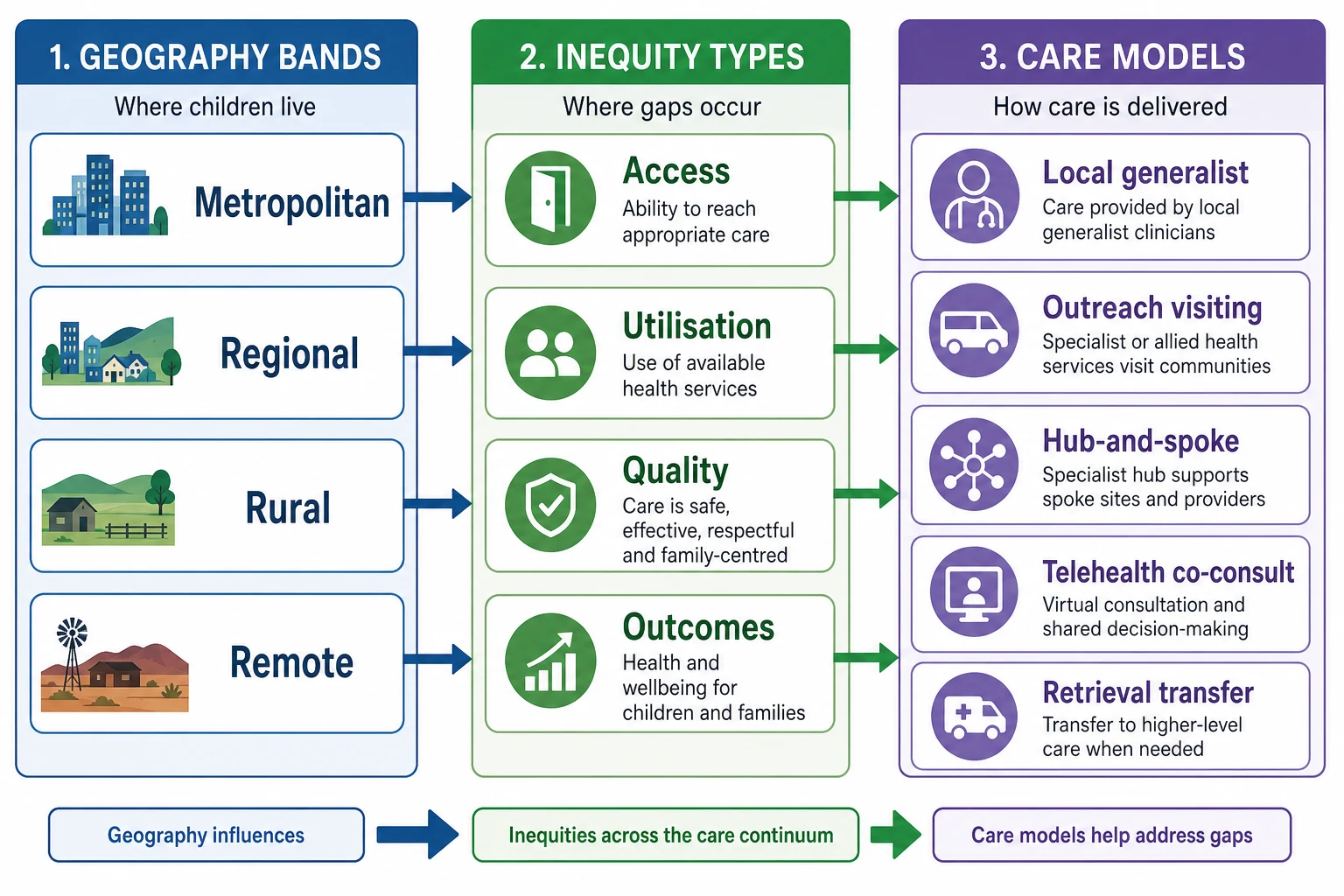
Sort the problem three ways: where, what gap, and which care model. [1] [3]
Geography. Jurisdictions use different maps. Australia commonly uses ASGS remoteness and the Modified Monash Model for workforce planning. The US uses rural-urban commuting codes and similar tools. The UK and Canada have their own rural and northern classifications. In exams, name the local system and describe the functional meaning (travel time, on-site services, after-hours cover). Do not invent numeric cut-points from memory if you are unsure. [1] [2]
Inequity type. Access (can the family reach care?). Utilisation (do they actually attend?). Quality (is the care paediatric-ready and continuous?). Outcomes (mortality, disability, developmental vulnerability, missed school). A town can have a clinic door open and still fail on quality or continuity. [19] [21]
Care models. Local generalist primary care. Visiting outreach. Hub-and-spoke specialist clinics. Telehealth co-consult with the local GP or nurse. Retrieval and interhospital transfer. Residential specialist service in larger regional centres. Most real systems mix these. [10] [16] [28]
Epidemiology & Risk Factors
Primary care for children is geographically maldistributed. Many regions have too few clinicians relative to child population, while other areas are relatively saturated. That is a structural access problem, not a parent motivation problem. [1] Workforce policy statements treat paediatrician supply, distribution and team composition as levers that change access. [2]
Specialty density falls as distance from cities rises. Families travel farther for surgical and medical subspecialty care; relative supply is thinner outside major centres. [4] [5] Rural environments also carry specific hazards: farm machinery, open water and dams, vehicles on private land, and burns exposures documented in rural paediatric cohorts. [3] [24] [25]
Developmental opportunity tracks place and neighbourhood adversity. School readiness is a paediatric equity outcome, not only an education metric. Children who miss early hearing, vision, language and preventive visits lose developmental windows that later therapy cannot fully buy back. [31] [32]
Indigenous and remote communities often face layered barriers: geography plus racism, housing, food security and service design that was not built with them. Geography alone never explains the full gap. [3] [33]
Pathophysiology
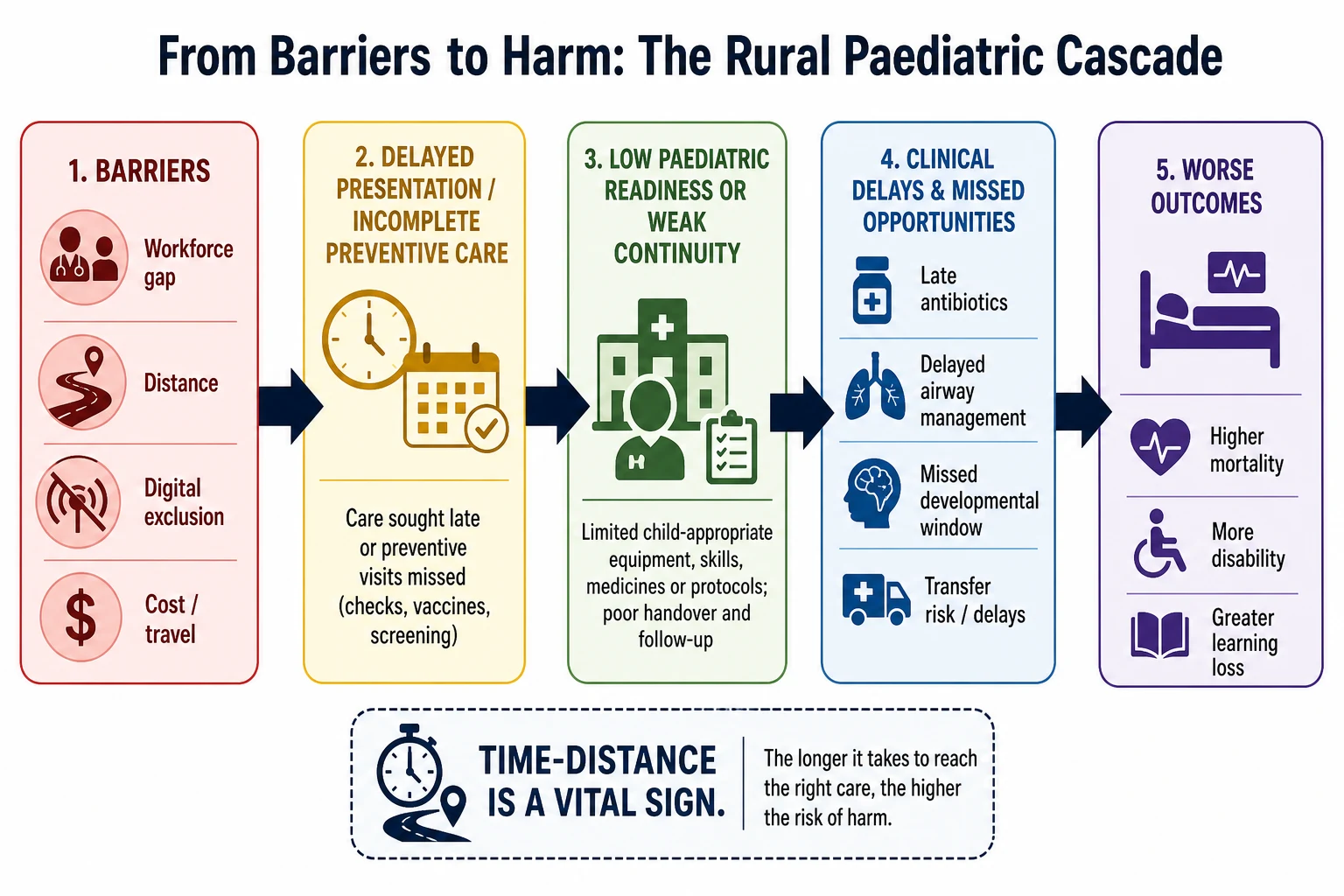
Think mechanisms that change Tuesday night, not slogans. [3] [7]
Time-distance. Every extra hour before antibiotics, airway support or haemorrhage control is physiology, not logistics theatre. Distance converts reversible disease into organ failure. [3] [7]
Thin continuity. Lower continuity of care associates with higher emergency-department use and hospitalisation in children. When every visit is a stranger, plans fragment and early warning is missed. [19] [21]
Paediatric readiness. National assessments show wide variation in how prepared emergency departments are for children. Higher paediatric readiness associates with lower short- and long-term mortality among children receiving emergency care, including injured children. A rural ED without paediatric dosing tools, equipment and protocols is a causal pathway, not a cosmetic audit score. [6] [7] [8] [34]
Financial and digital exclusion. Travel, lost wages, accommodation and poor connectivity block follow-up. Telehealth can reduce some costs for rural maternal and child health, but only if infrastructure and workflow exist. [17] [29]
Caregiver load. Complex care without coordination turns parents into unpaid case managers. That load predicts incomplete therapy and unsafe gaps. [20] [22]
Clinical Presentation
You will not always hear “we are rural” as the chief complaint. Listen for the place story. [3]
Preventive gaps. Overdue immunisations, missed newborn screens follow-up, late speech concern, uncorrected vision, no dental path. [3] [32]
Acute undifferentiated illness. Fever, respiratory distress, abdominal pain or head injury in a facility with limited imaging, limited bloods or no inpatient paediatrics. [3] [6]
Complex chronic travel burden. Ventilator- or feed-dependent children with multi-specialty appointments that require multi-day trips. [20] [22]
Rural injury patterns. Farm burns, quad-bike and machinery trauma, dam and open-water near-drowning, road trauma on long rural stretches. [24] [25] [26]
Mental health and behaviour. Adolescent crisis or developmental-behavioural need with no local child psychiatry and long waitlists. Tele-mental-health models were developed for exactly this gap. [18]
Retrieval interface. The “presentation” may be a phone call: a local team asking whether to keep, watch or move. [14] [26]
Differential Diagnosis
In rural work, the differential includes disease and system failure. [3] [21]
| What you see | Disease-side possibilities | System-side possibilities | Discriminators |
|---|---|---|---|
| Late severe illness | Sepsis, surgical abdomen, cardiac, metabolic | Delayed first contact, no transport, after-hours desert | Timeline of first worry versus first assessment |
| Recurrent ED visits | Poorly controlled chronic disease | No medical home, cannot afford clinic, no bulk-billing | Named usual clinician? Missed preventive visits? |
| Developmental concern found at school entry | Autism, language disorder, hearing loss | Missed surveillance, no audiology access | Prior screens, ear disease history, attendance |
| Growth faltering | Coeliac, CKD, endocrine, neglect | Food insecurity, interrupted care, housing mobility | Diet, benefits, kitchen access, record gaps |
| “Just behaviour” | ADHD, anxiety, trauma | Classroom mismatch, bullying, no allied health | Multi-setting history, safeguarding screen |
Never let “they live far away” become a diagnosis that stops you looking for organic disease. Never let a rare-disease hunt ignore an empty fridge and a 300 km specialist wait. [31]
Clinical & Bedside Assessment
Open with capability and time, then the child. [6] [12]
- Threat scan. Work of breathing, perfusion, consciousness, glucose, temperature, trauma pattern. [6]
- Place history. Travel time tonight, road conditions, who can drive, phone signal at home. [3]
- Usual care. Named GP or remote clinic nurse? Shared record? Last specialist letter? [19]
- Local inventory. Airway equipment sized for children, oxygen, imaging, blood gas or i-STAT, antibiotics on shelf, escort options, weather for rotary wing. [6]
- Family capacity. Fuel money, other children, leave from work, cultural supports. [17]
- Consent and culture. Interpreter needs; Indigenous liaison where available; avoid using children as interpreters. [22] [33]
Communicate in plain language. Say what you fear, what you can do here, and what transfer would add. Families make better decisions when the trade-offs are explicit. [22]
Investigations
Order tests that change the next safe step, not tests that decorate a referral. [12] [27]
Do locally when available and time-critical: glucose, blood gas or lactate if accessible, focused imaging for trauma or acute abdomen pathways your site supports, cultures before antibiotics when they will not delay drugs. [6] [12]
Delay safely when the child is stable and the test is elective: non-urgent MRI, routine specialty panels better done with the receiving team’s protocol. [12] [27]
Do not transfer solely for a test that can wait, unless local delay creates real risk. Structured non-urgent transfer tools such as PaNURAMA support nurse-escort and risk assessment for interhospital moves — use local validated processes rather than inventing escort rules. [27]
Telehealth adjuncts (photo, video, parent-assisted exam, tele-otoscopy where trained) can refine disposition, but they do not replace hands-on assessment when red flags exist. [9] [30]
Hand over every result already obtained. Duplicate radiation and lost samples are rural own-goals. [26]
Management — Resuscitation
Resuscitation principles do not change with postcode. Resource limits do. [6] [7]
- Open the airway, support breathing, treat shock, correct glucose, control external haemorrhage, and give timely antimicrobials when sepsis is likely.
- Use paediatric weight-based dosing aids and length-based tapes if available; readiness includes tools, not only goodwill. [6]
- Activate retrieval early when local capability is exceeded or trajectory is downward. Do not wait for the “perfect package” before calling for help. [26]
- Tele-emergency consultation can change transfer decisions and reduce some medication prescribing errors compared with telephone-only advice in trial settings. Prefer video when the platform and clinical tempo allow. [14] [15]
- For farm trauma, burns and drowning, concurrent life support and destination planning matter; prevention counselling comes after the child is safe. [24] [25]
Management — Definitive & Stepwise
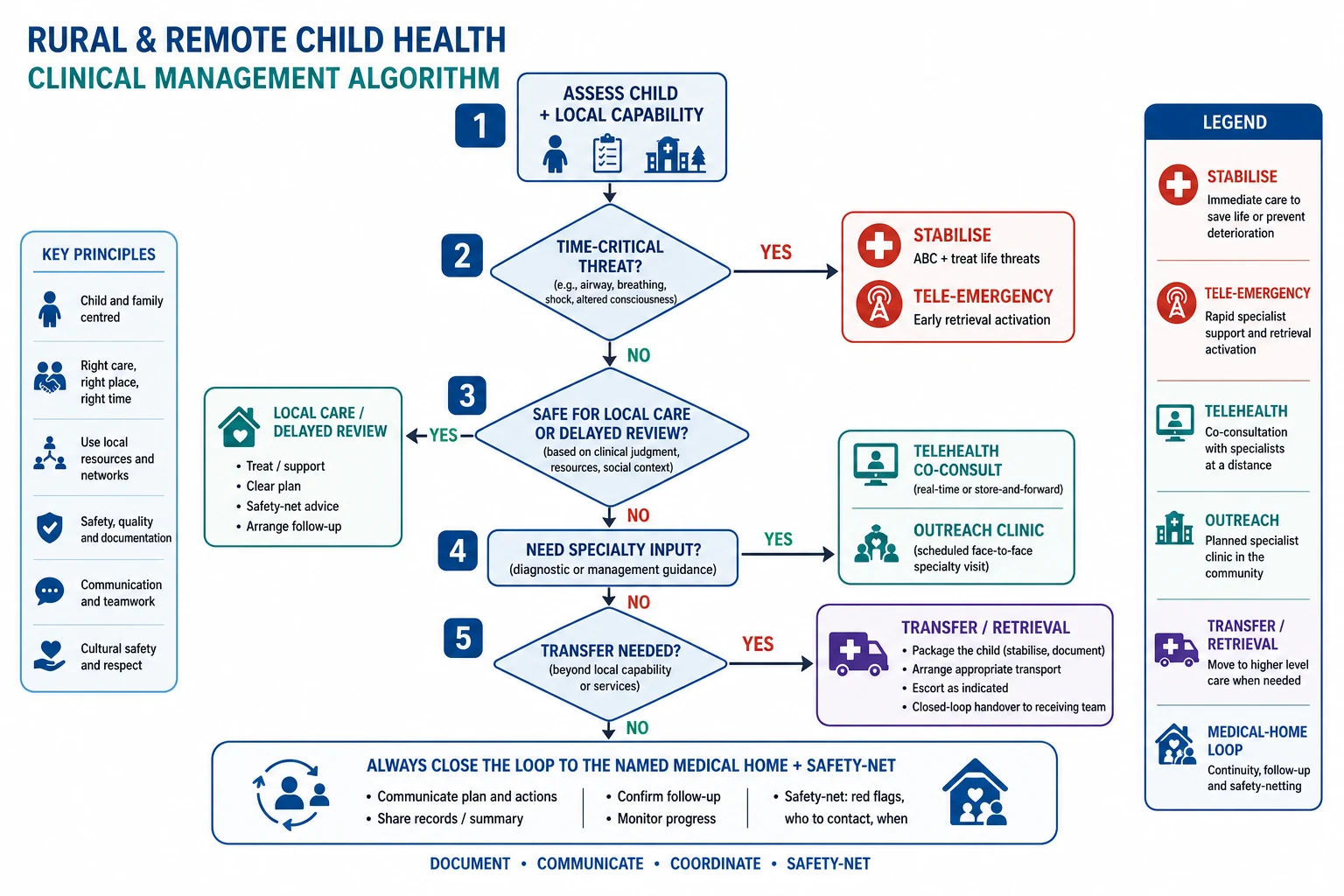
Use a capability-matched ladder, not a prestige ladder. [12] [16]
- Stabilise and reassess.
- Local definitive care when skills, monitoring and follow-up exist.
- Telehealth co-consult with paediatrics, mental health or specialty to keep care local when safe. Integrated GP–paediatrician virtual models are one implementation pattern. [28] [30]
- Planned outreach or hub clinic for non-urgent specialty review bundled with local tests.
- Interhospital transfer or retrieval when monitoring, procedure, PICU or specialty care exceeds local limits. [26] [27]
- Always close the loop to a named medical home: who reviews results, who renews medicines, who safety-nets deterioration. Continuity and care coordination improve utilisation and family experience; structured complex-care coordination has trial evidence in medical complexity. [19] [20] [21] [22] [23]
Telehealth is a tool for access, quality and sometimes cost — not a free pass to skip examination or continuity. Direct-to-consumer models that ignore the medical home can fragment care. Design for integration. [11] [12] [13]
Australian rural telehealth reviews emphasise sustainable models, workflow and relationships, not gadgets alone. Economic reviews of telehealth for regional maternal and child health often find cost savings for systems and families when programs work. [16] [17] [29]
Specific Subtypes & Scenarios
Remote neonate or young infant. Time-critical infection, congenital heart disease and metabolic disease punish delay. Lower threshold for transfer when observation capacity is thin. [3] [26]
Asthma, allergy and diabetes without local specialty. Written emergency plans, school linkage, telehealth titration and outreach education keep children in community when safe. [12] [20]
Adolescent mental health. Tele-mental-health services can bridge specialist gaps; still escalate imminent risk through local emergency and crisis pathways. [18]
Children with medical complexity. Virtual wraparound, care coordination and shared emergency information forms reduce travel burden; they do not remove the need for a local hands-on responder. [20] [22] [23]
Indigenous remote primary care. Workforce enhancement and community-controlled partnerships matter more than one-off fly-in heroics. Cultural safety is clinical quality. [33]
Farm and water injury. Anticipatory guidance: supervised water, four-sided pool fencing where relevant, dam awareness, machinery and quad-bike rules, burn prevention around hot water, fires and chemicals. [3] [24] [25]
Non-urgent interhospital transfer. Use structured risk tools and nurse-escort standards; not every move needs a critical-care team, and not every “stable” child is safe for an unescorted taxi. [27]
Complications & Pitfalls
- Treating telehealth as examination-complete when you cannot assess perfusion or work of breathing. [9] [30]
- Telephone-only advice when video tele-emergency is available and safer for decisions. [14] [15]
- Late retrieval activation while “waiting to see”. [26]
- Transfer without packaging, observations, airway plan or closed-loop handover. [26]
- No medical-home owner after outreach or tertiary admission. [19] [21]
- Ignoring travel cost as a reason medicines and appointments fail. [17]
- Urban templates that assume same-day labs, a paediatric nurse and a pharmacy open at midnight. [3]
- Culturally unsafe, extractive visiting models that never build local capacity. [33]
Prognosis & Disposition
Higher emergency-department paediatric readiness associates with lower mortality risk for children who need emergency care. That is a system prognosis lever you can advocate for, not only a research curiosity. [7] [8] [34]
Continuity and coordinated medical-home care associate with better utilisation patterns and support children with special health care needs. Structured complex-care programs can improve coordination outcomes in trial settings. [20] [21] [23]
Disposition choices after a rural encounter: [12] [19] [26]
| Situation | Default direction |
|---|---|
| Stable, local plan executable, medical home intact | Local care + timed review |
| Needs specialty advice, exam adequate remotely | Telehealth co-consult + local safety-net |
| Needs procedure, imaging or inpatient paediatrics not available | Planned or urgent transfer |
| Time-critical threat or falling trajectory | Stabilise + early retrieval |
| Complex care with open loops | Assign care coordinator / medical-home owner before discharge |
Special Populations
Neonates and infants. Higher time sensitivity; lower observation threshold. [3]
Technology-dependent children. Emergency information forms, local equipment checks and retrieval packaging lists before crises. [20] [22]
Indigenous families. Partner with Aboriginal Community Controlled Health Services / Māori and iwi providers / First Nations services as relevant; respect local governance. [33]
Seasonal and migrant agricultural families. Interrupted records, language discordance, housing mobility — rebuild preventive schedules deliberately. [3]
Out-of-home care. Placement changes erase continuity; name a medical home after every move. [19]
Disability. Sparse therapy access; telehealth and school-linked models may partially bridge, but equipment and hands-on therapy still need pathways. [12]
Poverty layered on distance. Neighbourhood adversity and rural cost stack; ask about food, fuel and phone credit as clinical data. [31]
Evidence, Guidelines & Regional Differences
Core evidence clusters: geographic maldistribution of child primary care and workforce policy; distance to specialty care; paediatric readiness and mortality; paediatric telehealth access and quality statements; tele-emergency trials on transfer and prescribing safety; Australian rural telehealth model and economic reviews; continuity and medical-home coordination including complex-care trials; rural injury patterns (dams, farms); digital innovation in rural primary care. [1] [2] [4] [6] [7] [12] [14] [16] [17] [20] [23] [24] [29]
RACP Advanced Training explicitly examines regional, rural and remote paediatric care (Learning Goal 14). Written and clinical exams test disposition judgment, communication with local teams and equity reasoning — not postcode trivia. [1] [12] [22]
Use local remoteness classifications (e.g. ASGS, Modified Monash) and state/territory retrieval networks. Telehealth MBS and rural generalist models vary by jurisdiction. Partner with ACCHS and Māori health services. Do not invent retrieval drug doses or escort rules — use local retrieval service guidelines. [16] [17] [26] [27] [33]
Rural and remote island services depend on district general hospitals, networked specialist paediatrics and retrieval/transport services. Apply NICE-aligned pathways with local capability notes; school and social-care interfaces remain essential for equity. [19] [22]
RUCA and related rural definitions, AAP workforce policy, and the National Pediatric Readiness Project shape the exam vocabulary. Telehealth policy and interstate licensure affect what you can deliver. Trauma-centre access and readiness both matter for injured children. [1] [2] [6] [7] [12] [34]
Provincial systems and northern/remote care models vary widely. Complex-care coordination evidence such as CCKO is Canadian and examinable as a coordination concept, not a universal funding model. Name the province’s retrieval and primary-care structure. [23]
Controversies to handle with judgment: how far to centralise specialty care; workforce incentive design; telehealth scope and corporate direct-to-consumer risk; and whether digital innovation reduces or widens equity gaps when connectivity is poor. [11] [13] [29]
Exam Pearls
- Ask travel time and local capability in the first minute. [3]
- Name the jurisdiction’s remoteness system; avoid fake cut-points. [1]
- Paediatric readiness changes mortality — quote the concept, not a memorised score. [6] [7]
- Video tele-emergency can outperform telephone for some safety outcomes. [14] [15]
- Medical home + closed loops beat episodic outreach alone. [19] [20]
- Farm, dam and machinery hazards are rural anticipatory guidance. [24] [25]
- Disposition is capability-matched, not status-matched. [12]
- RACP Learning Goal 14 is a real curriculum target, not a soft add-on.
References
- [1]Shipman SA Geographic maldistribution of primary care for children. Pediatrics, 2011.PMID 21172992
- [2]Basco WT Pediatrician workforce policy statement. Pediatrics, 2013.PMID 23897908
- [3]Cherry DC Children's health in the rural environment. Pediatric clinics of North America, 2007.PMID 17306687
- [4]Mayer ML Distance to care and relative supply among pediatric surgical subspecialties. Journal of pediatric surgery, 2009.PMID 19302846
- [5]Mayer ML Disparities in geographic access to pediatric subspecialty care. Maternal and child health journal, 2008.PMID 17879148
- [6]Gausche-Hill M A national assessment of pediatric readiness of emergency departments. JAMA pediatrics, 2015.PMID 25867088
- [7]Newgard CD Emergency Department Pediatric Readiness and Short-term and Long-term Mortality Among Children Receiving Emergency Care. JAMA network open, 2023.PMID 36637819
- [8]Newgard CD Association of Emergency Department Pediatric Readiness With Mortality to 1 Year Among Injured Children Treated at Trauma Centers. JAMA surgery, 2022.PMID 35107579
- [9]Burke BL Jr Telemedicine: Pediatric Applications. Pediatrics, 2015.PMID 26122813
- [10]Olson CA The Current Pediatric Telehealth Landscape. Pediatrics, 2018.PMID 29487164
- [11]Curfman A Pediatric Telehealth in the COVID-19 Pandemic Era and Beyond. Pediatrics, 2021.PMID 34215677
- [12]Curfman AL Telehealth: Improving Access to and Quality of Pediatric Health Care. Pediatrics, 2021.PMID 34462339
- [13]Curfman A Telehealth: Opportunities to Improve Access, Quality, and Cost in Pediatric Care. Pediatrics, 2022.PMID 35224638
- [14]Marcin JP Impact of Tele-Emergency Consultations on Pediatric Interfacility Transfers: A Cluster-Randomized Crossover Trial. JAMA network open, 2023.PMID 36780158
- [15]Marcin JP Telemedicine vs Telephone Consultations and Medication Prescribing Errors Among Referring Physicians: A Cluster Randomized Crossover Trial. JAMA network open, 2024.PMID 38421649
- [16]Bradford NK Telehealth services in rural and remote Australia: a systematic review of models of care and factors influencing success and sustainability. Rural and remote health, 2016.PMID 27744708
- [17]Adella GA Economic impact of telehealth on maternal and child health in regional, rural and remote Australia: a systematic review. Systematic reviews, 2025.PMID 41419985
- [18]Ryan VN Telemedicine for rural and remote child and youth mental health services. Journal of telemedicine and telecare, 2005.PMID 16375806
- [19]Haggerty JL Continuity of care: a multidisciplinary review. BMJ (Clinical research ed.), 2003.PMID 14630762
- [20]Homer CJ A review of the evidence for the medical home for children with special health care needs. Pediatrics, 2008.PMID 18829788
- [21]Christakis DA Association of lower continuity of care with greater risk of emergency department use and hospitalization in children. Pediatrics, 2001.PMID 11230593
- [22]Council on Children with Disabilities and Medical Home Implementation Project Advisory Committee Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209
- [23]Cohen E Effectiveness of Structured Care Coordination for Children With Medical Complexity: The Complex Care for Kids Ontario (CCKO) Randomized Clinical Trial. JAMA pediatrics, 2023.PMID 36939728
- [24]Bugeja L Drowning deaths of zero- to five-year-old children in Victorian dams, 1989-2001. The Australian journal of rural health, 2005.PMID 16171505
- [25]Chua M The Causes, Characteristics and Outcomes of Paediatric Farm Burns in Australia and New Zealand. The Australian journal of rural health, 2025.PMID 39907165
- [26]McCarron M A 10-year review of paediatric trauma inter-hospital retrieval patient outcomes in New South Wales (NSW), Australia. Injury, 2026.PMID 41887088
- [27]Davison M A Validation Study of the Paediatric Non-Urgent Risk Assessment Management and Nurse Escort Assessment (PaNURAMA) Tool for Paediatric Inter-Hospital Transfers. Emergency medicine Australasia : EMA, 2025.PMID 40605406
- [28]Bullock S A Virtual Integrated General Practitioner-Pediatrician Model of Care Implemented in Metropolitan and Rural Primary Care Settings: Qualitative Analysis of Clinician Perspectives on the SUSTAIN Model of Care. Journal of medical Internet research, 2026.PMID 42085669
- [29]MacAskill W A systematic review of the scope and impact of rural primary healthcare innovations using digital health technology. BMJ open, 2026.PMID 41611458
- [30]Milne Wenderlich A Telehealth in pediatric primary care. Current problems in pediatric and adolescent health care, 2021.PMID 33547004
- [31]Jutte DP Neighborhood adversity, child health, and the role for community development. Pediatrics, 2015.PMID 25733725
- [32]COUNCIL ON EARLY CHILDHOOD The Pediatrician's Role in Optimizing School Readiness. Pediatrics, 2016.PMID 27573085
- [33]Leach AJ A workforce enhancement model for Australian remote community Primary Health Care services: implementation of a stepped-wedge cluster randomised trial (SW-CRT). BMC health services research, 2026.PMID 41612286
- [34]Melhado C Pediatric Readiness and Trauma Center Access for Children. JAMA pediatrics, 2025.PMID 39899287