Paeds · preventive-and-community-paediatrics
Safe sleep and sudden unexpected death prevention
Also known as Safe sleep · SIDS prevention · SUDI prevention · SUID prevention · Sudden infant death syndrome · Sleep-related infant death · Back to sleep
Fellowship-level approach to safe infant sleep counselling and sudden unexpected death prevention: definitions, triple-risk model, modifiable hazards, AAP-aligned core rules, equity, NICU transition, unexpected death response, and regional practice differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
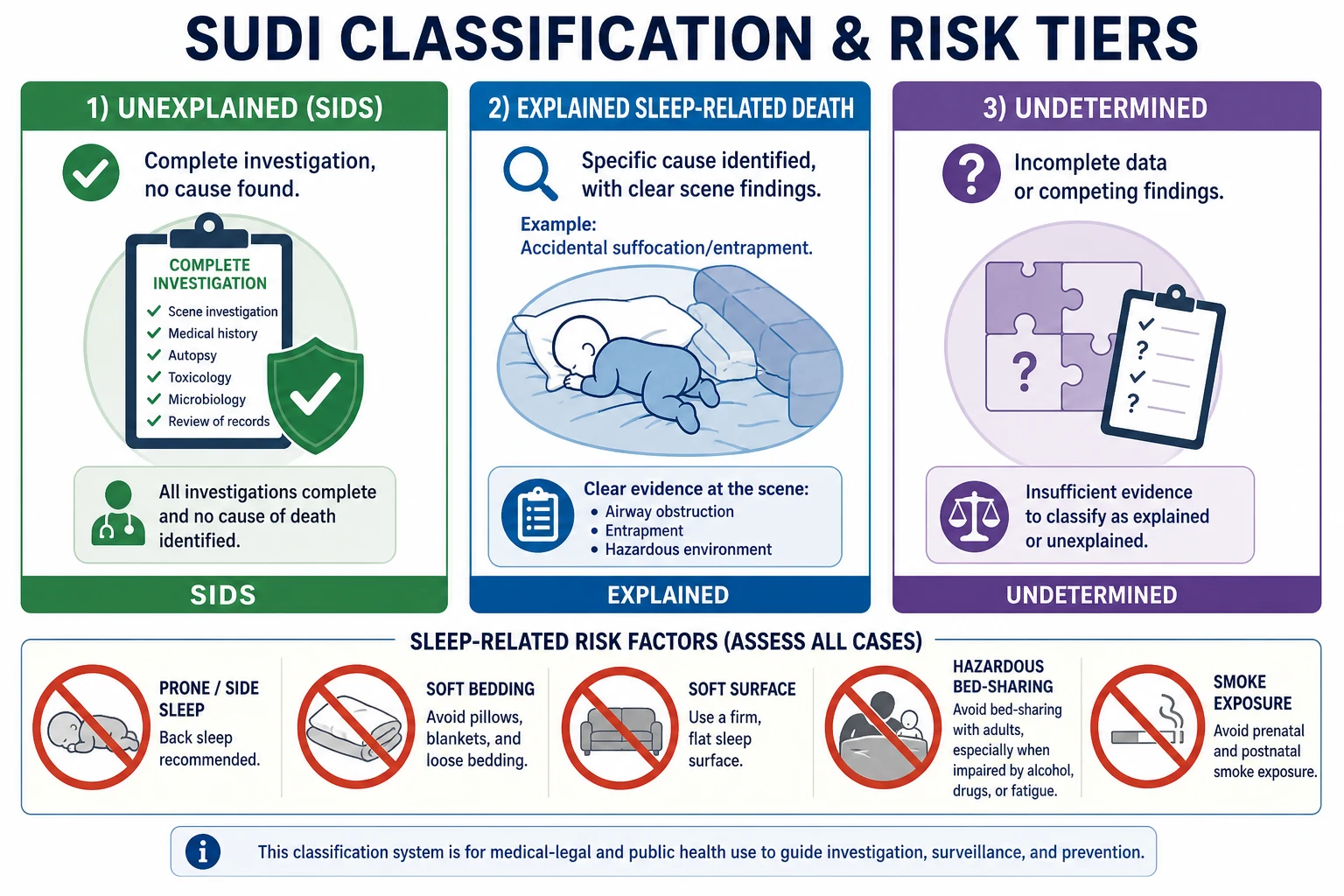
A family brings a well newborn home. Sleep is the first daily safety task you must teach well. Sudden unexpected death in infancy (SUDI) is an umbrella term for an infant death that was not anticipated. After investigation, some deaths remain unexplained (SIDS in many systems; SUID is a related US framing). Others are explained — most often accidental suffocation or entrapment in an unsafe sleep environment. Your job is prevention first, clear language second, and a calm emergency response if an infant is found unresponsive. [1] [20]
Safe sleep is not one slogan. It is a set of modifiable environmental rules that reduce exogenous stressors on a still-maturing cardiorespiratory and arousal system. Campaigns that moved infants onto their backs cut population rates sharply. Residual deaths cluster where hazards still stack: soft bedding, shared sleep with risk modifiers, smoke exposure, and inconsistent hospital modelling. [2] [5]
Classification
Think in two layers: how the death is classified after investigation, and how hazardous the sleep environment was before any event. Those layers meet in counselling and in multi-agency review, but they answer different questions. [1] [20]
Terms you must not blur
- Death not anticipated from history
- Umbrella before or during investigation
- Includes explained and unexplained outcomes
- Complete investigation without sufficient cause
- Diagnosis of exclusion, not a clinical bedside label in life
- Language with families must stay careful and non-accusatory
- Scene/autopsy support a mechanism such as entrapment or overlay
- Still often preventable by the same environment rules
- Does not require blaming a grieving caregiver
Age matters. Prevention focus is strongest through the first year, with the steepest risk window commonly described around 2 to 4 months, when many infants still have immature arousal responses and families may relax early habits. Premature infants remain at elevated risk after discharge even when chronological age is higher. [1] [3]
Epidemiology & Risk Factors
After Back-to-Sleep, absolute rates fell, but the mix of remaining risks shifted. Soft bedding, bed-sharing patterns, and other environmental hazards became relatively more visible as prone sleep declined. That is why modern counselling is broader than position alone. [5] [12] [13]
Intrinsic factors include prematurity, low birth weight, male sex, and likely biological vulnerability of brainstem arousal pathways in some infants. Extrinsic factors are the ones you can change today: prone or side sleep, soft sleep surfaces, loose bedding and soft objects, overheating, smoke exposure (prenatal and postnatal), and hazardous shared sleep. [2] [4] [10]
Protective associations include supine sleep on a firm flat surface, room-sharing without bed-sharing, breastfeeding, and pacifier use at sleep onset once feeding is established for families who choose a pacifier. None of these is a guarantee. They are risk-reducing layers. [1] [6] [7]
Inequity is part of the epidemiology. Australian data show higher clustering of modifiable risk factors in some Indigenous communities compared with non-Indigenous comparisons, which demands culturally safe support and resources rather than blame. Crowded housing, multiple caregivers, and lack of a separate infant sleep space also change what "follow the rule" looks like in real homes. [15]
Pathophysiology
The most useful teaching model is still the triple-risk model: a vulnerable infant, a critical developmental period, and an exogenous stressor. Death risk rises when those three meet. Remove the exogenous stressor and many vulnerable infants pass through the window safely. [3]
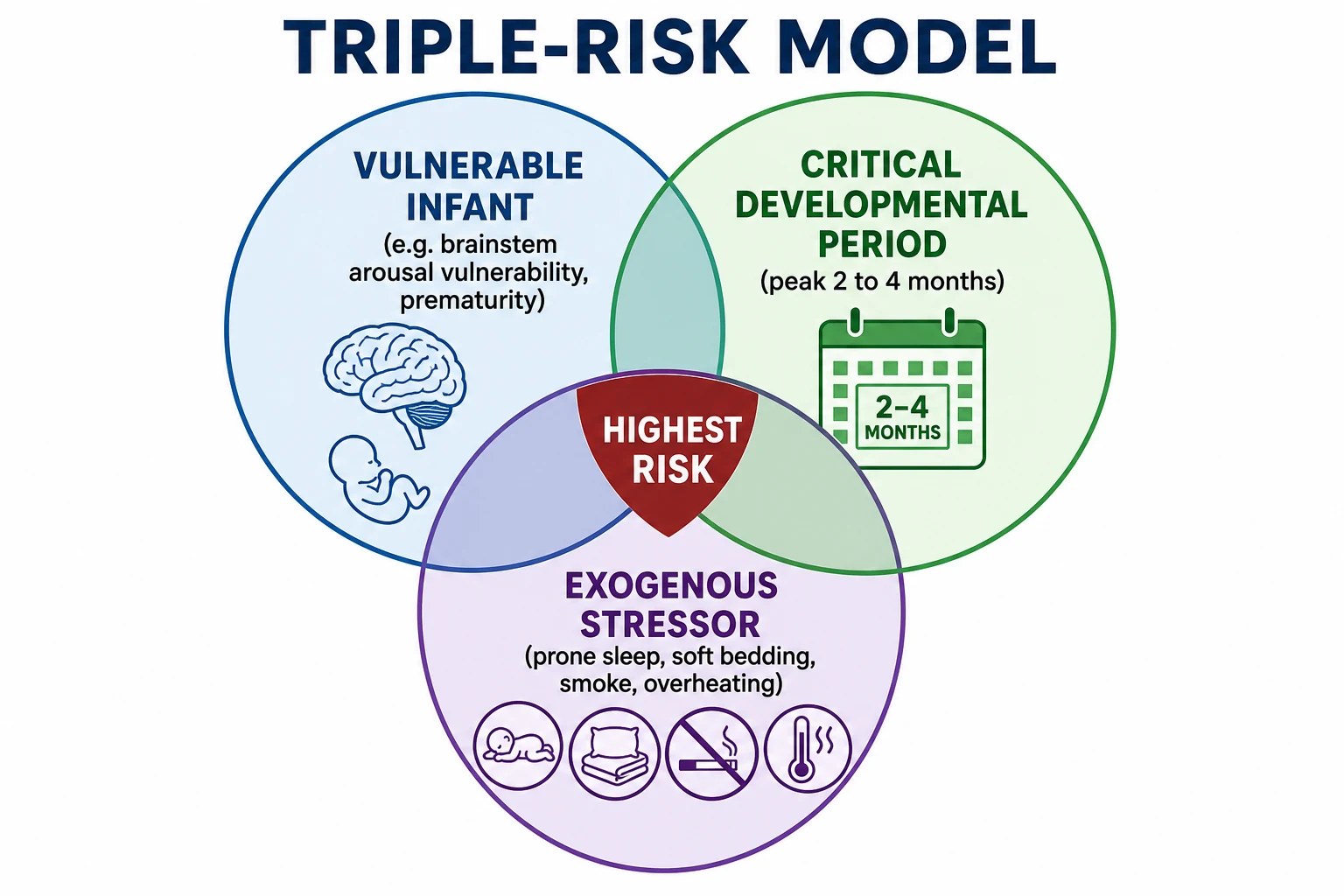
What makes an infant "vulnerable"? Research has focused on brainstem networks that control arousal and cardiorespiratory responses, including serotonergic pathways. The point for clinicians is practical: some infants may not mount a protective response to rebreathing, asphyxial stress, or thermal challenge during sleep. You cannot identify that infant reliably at a well-child visit, so you protect every infant. [4]
Prone position, soft surfaces, and soft bedding increase the chance of face-down rebreathing and impaired heat loss. Shared sleep on sofas or soft adult beds adds overlay and entrapment risk. Smoke exposure adds both prenatal and postnatal biological disadvantage. Stacked hazards matter more than any single checkbox. [2] [10]
Clinical Presentation
In clinic, the "presentation" is usually a well infant and a tired caregiver. Ask concrete questions: Where did baby sleep last night? On the back, side, or tummy? What was in the cot? Was anyone sharing the sleep surface? Any smoking in the home or car? Any sofas overnight after feeds? What about daytime naps? [1]
Families often describe intended practice, not actual practice. Night feeds, twins, visitor beds, and car-seat naps after drives are common hidden patterns. Commercial products (inclined sleepers, loungers, weighted sacks) may be offered as "safer" despite guidance against routine sleep in non-approved devices. [1] [17]
The other presentation is catastrophic: an infant found unresponsive after a sleep period. History may include recent mild illness, a change in sleep location, or a caregiver who fell asleep while feeding on a sofa. Your first task is resuscitation, not reconstruction. Scene details still matter and should be captured carefully once the infant is being treated. [1]
Differential Diagnosis
After an unexpected infant death, the differential is not an academic list. It is the reason a full investigation exists. Unexplained SIDS remains a residual category when infection, metabolic disease, cardiac disease, trauma, and a clear asphyxial mechanism are not established. Accidental suffocation or entrapment is an explained sleep-related death when scene and pathology support it. Maltreatment must stay on the list without becoming the default assumption about every grieving parent. [1] [20]
In living infants, safe-sleep counselling is not the place for shotgun metabolic panels. Investigate symptoms, growth failure, apnoea concerns, or family cardiac history on their own merits. After a death in the family, specialist advice may guide sibling evaluation; do not invent a universal test panel from memory. [1]
Clinical & Bedside Assessment
Use a non-judgemental script. "Lots of families find nights hard. Can we walk through exactly where baby slept?" Shame drives concealment and blocks prevention. Observe how caregivers place the infant in a cot or bassinet if you can. Check that hospital cots model the same rules you preach. [1] [16]
Bedside safe-sleep assessment in under five minutes
Position and surface
Ask about back/side/prone and whether the mattress is firm, flat and non-inclined for every sleep, including naps.
Bare space check
Pillows, loose blankets, soft toys, bumpers, wedges and positioners should be out of the sleep space.
Room vs bed share
Same room is protective; shared sleep surface needs hazard review, especially smoke, alcohol, drugs, sofa, preterm status.
Smoke and substances
Prenatal and postnatal smoke, vaping, alcohol and sedating drugs change risk and counselling tone.
Devices and swaddle
Car seats, swings and loungers are not routine sleep spaces; stop swaddling when rolling begins.
Teach-back
Ask the caregiver to show or restate the plan for tonight, then document and offer written or visual supports.
Assess social context: housing, number of caregivers, out-of-home care placements, language needs, and access to a safe sleep space. Offer practical help (bassinet access schemes where available) rather than only rules. For complex or technology-dependent infants, balance medical positioning needs with the safest achievable sleep plan and specialist input. [14] [15]
Investigations
Well-child safe-sleep visits need no laboratory work. The investigation is the history, the demonstration, and the home plan. Document what you advised and what barriers remain. [1]
After unexpected death, local multi-agency protocols govern autopsy, infection work-up, metabolic testing, imaging, and death-scene investigation. Your role is to support the family, preserve information, avoid contaminating the scene unnecessarily, and ensure siblings' immediate safety and care. Phenotype clarity after death still matters for public health and research, but it does not change the immediate resuscitation priorities. [1] [20]
Management — Resuscitation
If an infant is found unresponsive, treat this as a paediatric emergency. Call for help. Start age-appropriate CPR. Open the airway, support breathing and circulation, attach monitoring, and follow local paediatric advanced life support. Do not delay airway and CPR to complete a forensic history. [1]
Once the team is working, assign someone to support caregivers and gather a calm timeline: last seen well, sleep location, position found, bedding, shared sleep, smoke, recent illness, and any resuscitation already attempted. Avoid accusatory language. If findings later raise safeguarding concerns, involve the appropriate pathway while continuing family support. [1]
Management — Definitive & Stepwise
Prevention is the definitive management for almost every visit on this topic. Anchor on the 2022 AAP update and compatible national messaging (Red Nose in Australia; Lullaby Trust-framed safer sleep in the UK). [1] [2]
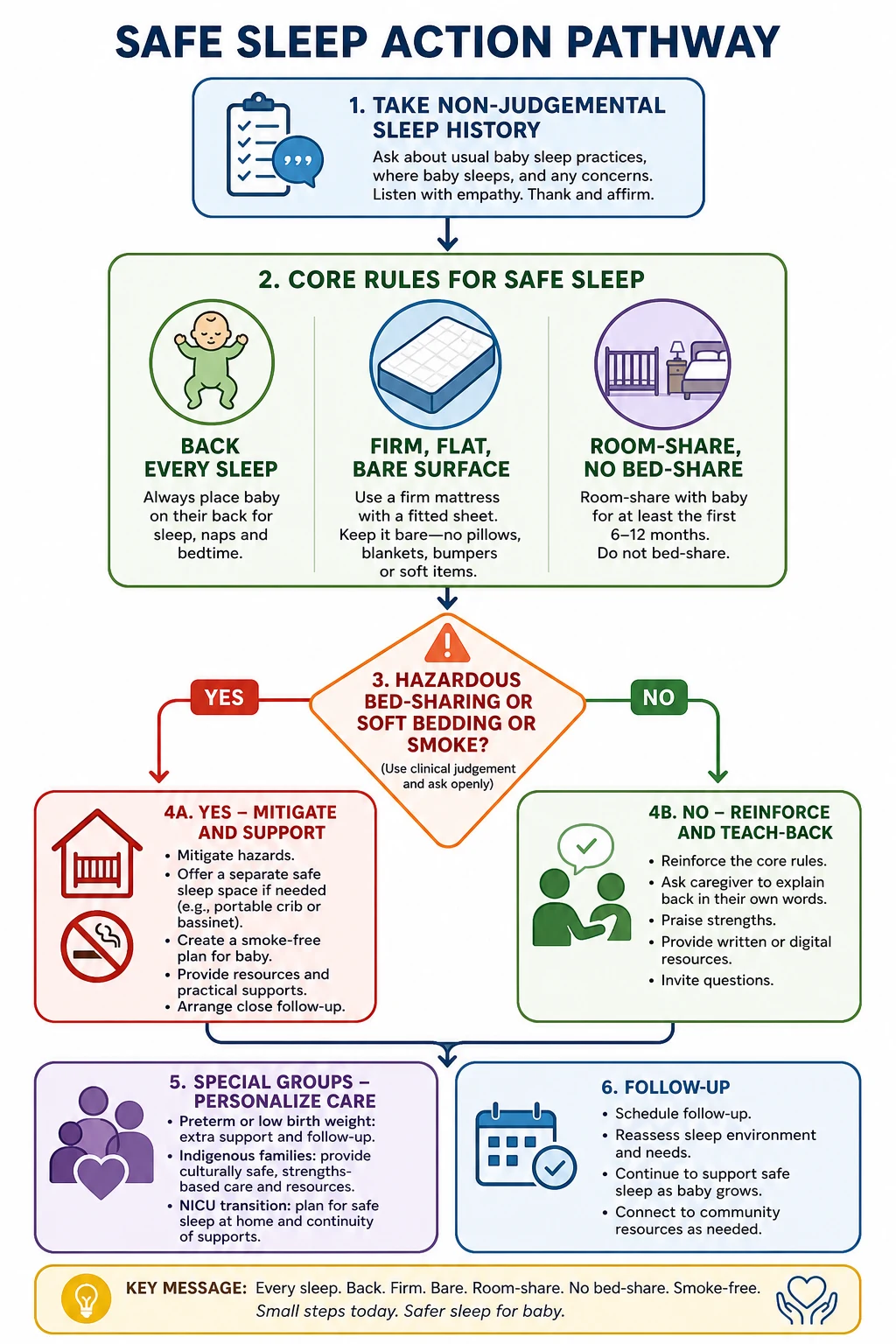
Core rules for every family [1]
- Supine for every sleep — nights and naps. Side sleep is not a safe compromise because infants roll to prone more easily. Tummy time is for awake, supervised periods only. [1]
- Firm, flat, non-inclined surface in a safety-approved cot, bassinet or portable crib with a fitted sheet only. [1]
- Bare sleep space — no pillows, soft toys, loose blankets, bumper pads, wedges or positioners. Soft bedding remains common despite long-standing advice. [1] [12]
- Room-share without bed-sharing ideally for at least the first 6 months. Adult beds and sofas are not designed as infant sleep surfaces. [1]
- Smoke-free pregnancy and home/car environments. [1] [10]
- Avoid overheating and head covering. Dress for the room; do not add heavy covers over the head. [1]
- Breastfeeding support when possible; it is associated with lower SIDS risk and is promoted for multiple health reasons. [6]
- Pacifier at sleep onset may be offered once breastfeeding is established if the family wishes; do not force or reinsert repeatedly through the night. [1] [7]
- Swaddling only if the infant is supine and not yet rolling; stop as soon as rolling begins. Swaddling with prone position is particularly hazardous. [11]
- No routine sleep in sitting devices (car seats out of the car, swings, loungers) or commercial inclined sleep products. [1]
Bed-sharing needs explicit hazard counselling. Analyses differ in how they frame residual risk when no hazards are present, but there is broad agreement that risk rises sharply with sofa sharing, smoke exposure, alcohol or drugs, soft surfaces, and preterm or low-birth-weight infants. AAP guidance advises against bed-sharing as the recommended routine arrangement and emphasises room-sharing instead. If a family still shares a sleep surface, remove every modifiable hazard and keep offering a separate safe space. [1] [8] [9] [10]
Hospital and maternity modelling matters. Staff practices teach families more than pamphlets. Quality-improvement approaches can improve safe-sleep behaviours after discharge. NICU graduates need a planned transition from therapeutic positioning to a home-safe sleep environment before leaving. [14] [16]
BACKSAFE
Specific Subtypes & Scenarios
First nights at home after a term birth. Fatigue is high. Pre-plan overnight feeds so the adult does not fall asleep on a sofa with the infant. A bassinet beside the bed is often more realistic than a distant nursery. [1]
Ex-preterm or low-birth-weight infant. Treat environmental risk as higher. Be especially firm about separate sleep surface and smoke-free care. Complete NICU safe-sleep transition teaching before discharge. [14]
Cultural bed-sharing. Respect values, then negotiate safety: same room, separate surface if possible; if sharing continues, remove alcohol/drugs, smoke, soft bedding and sofa use, and never leave the infant alone on an adult bed. [9] [15]
Twins. Each infant needs a safe surface. Sharing one cot long-term is not a solution to space pressure. [1]
Sofa and armchair sleep after feeds. Call this out as high risk. Build an alternative: feed in bed only if an adult will return the infant to a bare bassinet before adult sleep, or feed in a chair with a plan that avoids falling asleep there. [10]
Unexpected death in ED. Resuscitate, support family, activate local SUDI pathway, protect siblings' care, document scene history carefully, and avoid early public statements that invent a cause. [1] [20]
Complications & Pitfalls
Other pitfalls: shaming that ends disclosure; assuming SIDS is purely genetic so counselling is pointless; ignoring smoke exposure; forgetting daytime naps; and missing genuine safeguarding concerns while trying to be kind. Stay kind and still clear. [17]
Prognosis & Disposition
Population prognosis improved after supine sleep campaigns, but preventable deaths continue where hazards remain common. For an individual family after counselling, disposition is usually home with a written or demonstrated plan and a named follow-up contact if barriers exist (no cot, housing crisis, substance use). [5] [1]
After a death, disposition includes multi-agency investigation, bereavement support, practical help for the family, and careful communication about what is and is not known. Future pregnancy counselling should restate prevention without promising zero risk. [1]
Special Populations
Indigenous families may face higher exposure to clustered modifiable risks and structural barriers. Use culturally safe communication, community resources, and practical supports; do not equate culture with unsafe practice. [15]
Socioeconomic disadvantage and crowded housing may mean no separate room or cot. Help source a safe sleep space and prioritise the highest-yield rules that are feasible tonight. [1]
Out-of-home care and multiple caregivers require the same message to every adult who puts the infant down. Written plans travel better than verbal advice given once. [1]
Migrant and refugee families need professional interpreters for counselling, not child interpreters. Show pictures of a bare supine cot. [1]
Technology-dependent infants may need elevated head positioning or equipment that conflicts with a simple bare-cot plan. Co-design the safest achievable plan with the treating specialists and document trade-offs. [14]
Evidence, Guidelines & Regional Differences
The operational spine for this page is the AAP 2022 policy and technical report on sleep-related infant deaths, updating earlier expansions of safe-sleep recommendations beyond position alone. The evidence base reviews position, surface, bedding, room-sharing, bed-sharing, smoke, feeding, pacifiers and devices. [1] [2] [18] [19]
In Australia and Aotearoa New Zealand, public messaging is commonly aligned with Red Nose safe-sleep principles and maternity/child-health programmes: back to sleep, face uncovered, smoke-free, safe cot, and close care. Address Indigenous inequities with partnership and resources, not deficit language alone. [15]
Controversies to handle cleanly in viva. Bed-sharing risk estimates differ by dataset and hazard control (Carpenter versus Blair analyses). Your exam-safe answer: do not recommend routine bed-sharing; aggressively remove hazards; prefer room-sharing; be honest that absolute risks vary by context and that sofas and smoke are non-negotiable red flags. Another live tension is parental sleep deprivation versus exclusive messaging — acknowledge the tension, then problem-solve safer night routines rather than abandoning the core rules. [8] [9] [17]
Exam Pearls
If you remember only one chain: unsafe environment → exogenous stress on a vulnerable infant in a critical window → preventable death risk. Your counselling removes the exogenous stress. That is the fellowship answer in one sentence. [3]
References
- [1]Moon, RY Sleep-Related Infant Deaths: Updated 2022 Recommendations for Reducing Infant Deaths in the Sleep Environment Pediatrics, 2022.PMID 35726558
- [2]Moon, RY Evidence Base for 2022 Updated Recommendations for a Safe Infant Sleeping Environment to Reduce the Risk of Sleep-Related Infant Deaths Pediatrics, 2022.PMID 35921639
- [3]Filiano, JJ A perspective on neuropathologic findings in victims of the sudden infant death syndrome: the triple-risk model Biology of the neonate, 1994.PMID 8038282
- [4]Kinney, HC The brainstem and serotonin in the sudden infant death syndrome Annual review of pathology, 2009.PMID 19400695
- [5]Trachtenberg, FL Risk factor changes for sudden infant death syndrome after initiation of Back-to-Sleep campaign Pediatrics, 2012.PMID 22451703
- [6]Hauck, FR Breastfeeding and reduced risk of sudden infant death syndrome: a meta-analysis Pediatrics, 2011.PMID 21669892
- [7]Hauck, FR Do pacifiers reduce the risk of sudden infant death syndrome? A meta-analysis Pediatrics, 2005.PMID 16216900
- [8]Carpenter, R Bed sharing when parents do not smoke: is there a risk of SIDS? An individual level analysis of five major case-control studies BMJ open, 2013.PMID 23793691
- [9]Blair, PS Bed-sharing in the absence of hazardous circumstances: is there a risk of sudden infant death syndrome? An analysis from two case-control studies conducted in the UK PloS one, 2014.PMID 25238618
- [10]Blair, PS Hazardous cosleeping environments and risk factors amenable to change: case-control study of SIDS in south west England BMJ (Clinical research ed.), 2009.PMID 19826174
- [11]Pease, AS Swaddling and the Risk of Sudden Infant Death Syndrome: A Meta-analysis Pediatrics, 2016.PMID 27244847
- [12]Shapiro-Mendoza, CK Trends in infant bedding use: National Infant Sleep Position study, 1993-2010 Pediatrics, 2015.PMID 25452654
- [13]Colson, ER Trends and factors associated with infant bed sharing, 1993-2010: the National Infant Sleep Position Study JAMA pediatrics, 2013.PMID 24080961
- [14]Goodstein, MH Transition to a Safe Home Sleep Environment for the NICU Patient Pediatrics, 2021.PMID 34155135
- [15]Shipstone, RA Prevalence of risk factors for sudden infant death among Indigenous and non-Indigenous people in Australia Acta paediatrica, 2020.PMID 32239524
- [16]Moon, RY The Effect of Nursing Quality Improvement and Mobile Health Interventions on Infant Sleep Practices: A Randomized Clinical Trial JAMA, 2017.PMID 28742913
- [17]Moon, RY The Tension Between AAP Safe Sleep Guidelines and Infant Sleep Pediatrics, 2024.PMID 38529562
- [18]Moon, RY SIDS and Other Sleep-Related Infant Deaths: Evidence Base for 2016 Updated Recommendations for a Safe Infant Sleeping Environment Pediatrics, 2016.PMID 27940805
- [19]Task Force on Sudden Infant Death Syndrome SIDS and other sleep-related infant deaths: expansion of recommendations for a safe infant sleeping environment Pediatrics, 2011.PMID 22007004
- [20]Wojcik, MH The fundamental need for unifying phenotypes in sudden unexpected pediatric deaths Frontiers in medicine, 2023.PMID 37332751