Paeds · preventive-and-community-paediatrics
Screening test principles in children
Also known as Paediatric screening principles · Wilson Jungner children · Population screening paediatrics · False positive screening children · Predictive value low prevalence
Fellowship guide to screening test principles in children: programme criteria, sensitivity specificity and PPV in low prevalence, false-positive harm, two-step pathways, consent, net benefit, and ANZ/UK/US/Canada governance differences without duplicating bloodspot, hearing or developmental tool chapters.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A parent holds a healthy newborn and asks why the heel-prick and hearing check are needed “when nothing is wrong.” The clinical answer is simple: some serious conditions start quietly. If you wait for symptoms, the chance to protect the brain, hearing or metabolism may already be smaller. Screening means offering a test to children who look well, aiming to find disease or high risk early enough that a planned action improves outcome. [4] [22]
That sentence hides three traps. First, screening is not diagnostic testing of a sick child. Second, a positive screen is a flag, not a label. Third, a negative screen reduces risk; it does not make risk zero. Examiners listen for those three distinctions. [4] [5] [17]
A screening pathway is the full chain: invitation and information, consent, the index test, interpretation, timely confirmatory testing, treatment or surveillance, and programme audit. If any link is missing, the “screen” is incomplete even when the swab or blot looks perfect. [2] [3]
Five questions before you offer any paediatric screen
Is the condition important?
Serious enough, early enough, and common enough in this group to justify looking.
Is there an acceptable accurate test?
Workable in real children, with known sensitivity and specificity.
Does early action help?
Treatment or prevention started after screen must beat waiting for symptoms.
Is the pathway ready?
Confirmatory tests, specialists, drugs and follow-up must exist now—not next year.
Is net benefit clear after harms?
Count false positives, anxiety, overdiagnosis, cost and equity—not only true positives found.
Classification
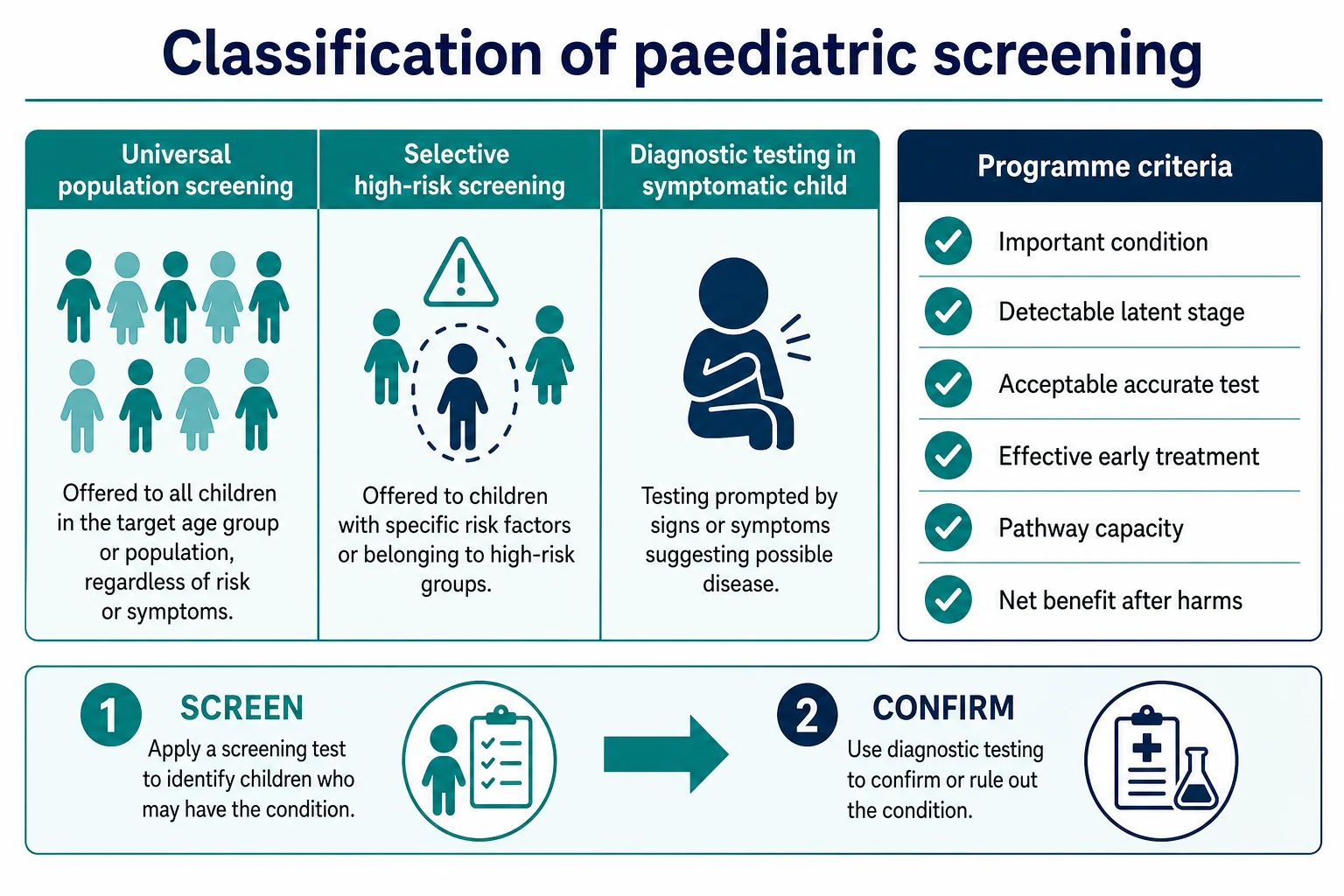
Start with the child in front of you, then name the pathway type. Classification is not taxonomy for its own sake—it changes consent language, cut-offs and what you do with a positive result. [4] [11]
Pathway types you must separate
Universal (population) screening offers the same test to a defined age or setting group—for example newborn bloodspot or universal newborn hearing programmes—because early silent disease can be missed by risk history alone. [20] [22]
Selective (high-risk) screening targets children with higher pre-test probability: family history, exposure, migration history, or a clinical risk flag. The same assay can be wise in a high-risk group and wasteful in a low-risk group because prevalence changes predictive values. [5] [6]
Case-finding hunts for disease during care for another problem. Diagnostic testing answers “what is wrong in this symptomatic child?” Mixing those words with “screening” is a classic viva fail. [4]
Cascade screening tests relatives after an index diagnosis. It is family-directed risk work, not population screening of all children. [1]
Classic and modern programme criteria
Wilson and Jungner’s classic public-health criteria still frame the conversation: important condition, recognisable latent stage, suitable test, accepted treatment, agreed policy, and facilities for diagnosis and treatment. Modern reviews keep those bones and add equity, programme quality, informed choice, and explicit harm assessment—especially as genomic panels expand. [1] [2] [22]
Harris and colleagues stress that proposed programmes need a clear analytic framework: how screening changes outcomes, what harms count, and whether real-world delivery can deliver the trial benefit. Dobrow’s consolidation work packages principles for decision-makers so “we can detect it” never becomes the only argument. [2] [3]
| Label | Bedside meaning | Exam trap |
|---|---|---|
| Index test | The first screening tool | Calling it diagnostic |
| Reference standard | The confirmatory truth test | Skipping it after a “positive” |
| Target condition | The disease you meant to find | Expanding to every abnormal variant |
| Screen positive | Needs next step | Equals disease |
| False positive | Positive screen, no target disease | “No harm done” |
| Overdiagnosis | True finding that would not have harmed | Same as false positive |
| Residual risk | Risk left after a negative screen | Zero risk |
Universal screen
Whole defined group
- Same offer by age/setting
- Catches silent disease without risk flags
- Needs high coverage and strong pathway
- PPV often low because prevalence is low
Selective screen
Higher pre-test group
- Triggered by risk history
- Higher yield if risk is real
- Misses cases outside the risk group
- Still needs confirmation
Diagnostic test
Symptomatic child
- Answers a clinical problem
- Different thresholds and urgency
- Not a population programme
- Sibling Bayesian topic owns depth
Epidemiology & Risk Factors
There is no single “screening rate” that proves a programme is good. What matters is who is offered the test, who completes it, who returns after a positive result, and whether true disease is treated earlier with better outcomes. [2] [3]
Prevalence is the quiet killer of positive predictive value. In a rare childhood condition, most children are truly well. Even a specific test can generate more false positives than true positives among those who flag positive. That is arithmetic, not pessimism. [5] [11]
Age band, geography, season, vaccination coverage, family history and social determinants all shift pre-test probability. A migrant child with incomplete prior preventive care may need catch-up of missed programme screens. A child in out-of-home care may have consent and record gaps that break follow-up. Rural and remote families can complete the first test and still lose the confirmatory step if travel or telehealth fails. [2] [16]
Programme metrics worth knowing in a viva: coverage (offered and completed), screen-positive rate, true-positive yield, false-positive rate, time to confirmation, time to treatment, and missed cases presenting clinically. Incomplete follow-up after a positive screen is a population-level false reassurance even when the laboratory performed correctly. [2] [20]
Commercial expansion and defensive culture can drive low-value testing. European paediatric statements warn that overtesting and overtreatment are real in child health, not only in adult medicine. Your job is stewardship: offer high-value programme screens well, and refuse low-value panels dressed as “peace of mind.” [15] [16]
Pathophysiology
Think in two layers: the mathematics of a single result, and the biology of early disease versus harmless variants. [5] [6]
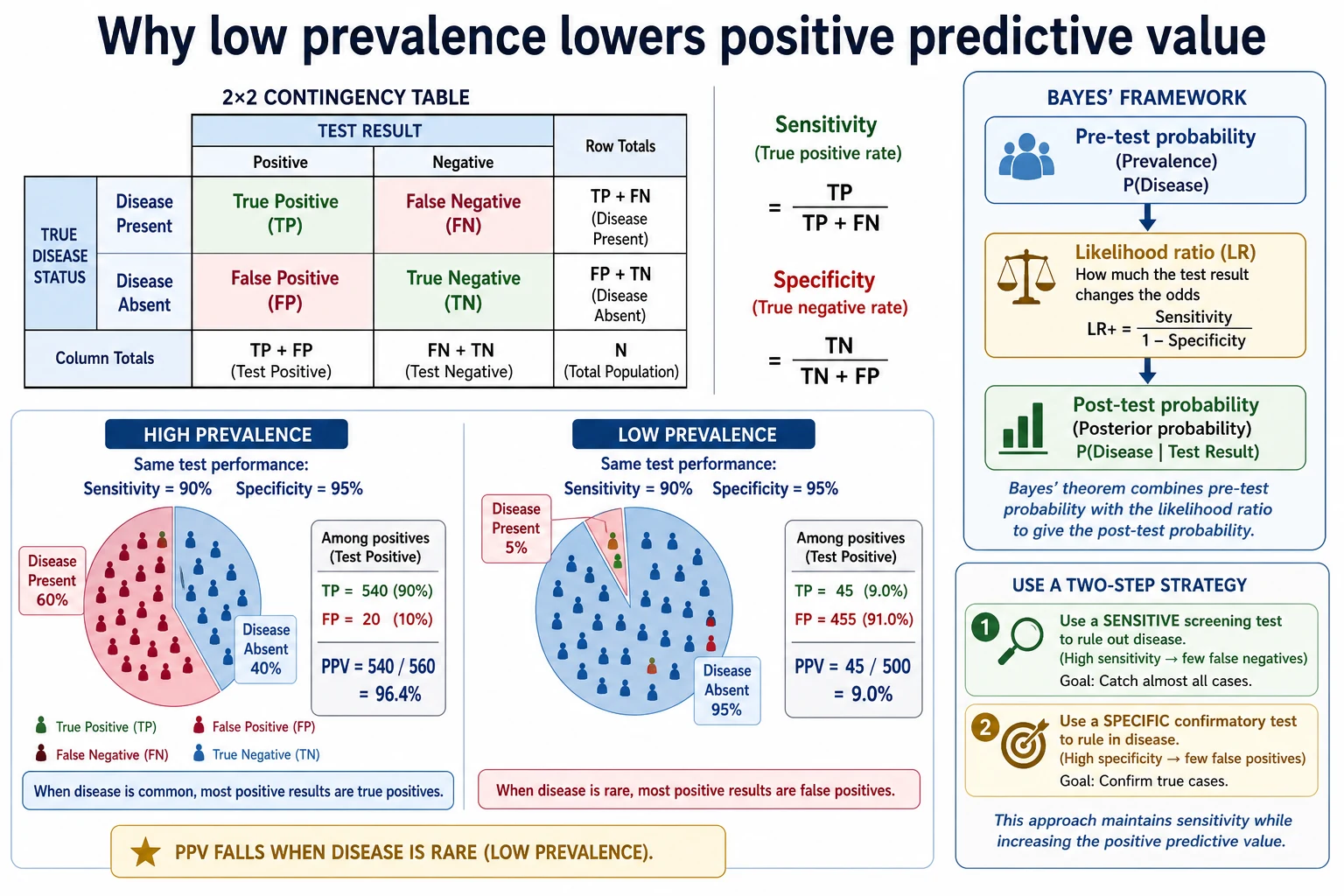
The 2×2 table you must own
Every dichotomous screen sorts children into true positives, false positives, false negatives and true negatives. Sensitivity is the proportion of diseased children the test correctly flags. Specificity is the proportion of well children the test correctly clears. Those two numbers do not depend on prevalence. [5] [11]
Positive predictive value (PPV) is the proportion of positive results that are true disease. Negative predictive value (NPV) is the proportion of negative results that are truly free of the target condition. Both depend on prevalence. When disease is rare, PPV falls hard. That is why a “highly specific” test can still flood a clinic with false alarms if you screen everyone. [5] [11]
Likelihood ratios restate accuracy in a form that updates pre-test odds to post-test odds without baking prevalence into the test property itself. At the bedside you still start with a pre-test probability for this child, then move it with the result. Fagan-style nomogram thinking is the classic teaching tool. [6] [8] [9]
Worked low-prevalence intuition (hypothetical numbers for teaching)
Imagine a target condition present in 1 in 1,000 children (0.1%). A screen that is 99% sensitive and 99% specific sounds excellent. In 100,000 children you expect about 100 true cases and about 99 true positives found. You also expect about 999 false positives among the well majority. Among roughly 1,098 positives, only about 99 are true—so PPV is under 10%. Families hear “positive” as “probably diseased” unless you translate. [5] [11]
That is why many programmes use a two-step design: a sensitive first screen to miss few cases, then a more specific confirmatory test before a disease label or long treatment. [4] [11]
Biology of benefit and overdiagnosis
True screening benefit appears when early detection of progressive disease allows action that improves function or survival. Harm appears when the pathway finds mild, transient or non-progressive variants that would never have mattered—overdiagnosis—or when false positives trigger anxiety, procedures and cascade testing. Overdiagnosis is not the same as a false positive: the finding can be “real” on the reference standard and still not help the child. [17] [21] [23]
Lead-time bias and length-time bias matter conceptually in exams: earlier detection can create the appearance of longer survival without changing the disease course, and screening prefers slower cases. In paediatrics you more often defend against false-positive cascades and mild-variant expansion than classic cancer lead-time arithmetic—but the intellectual trap is the same: detection is not automatically benefit. [3] [4] [12]
Threshold thinking (Pauker) asks whether post-test probability has crossed a test or treatment threshold. If a result cannot move you across a decision line, do not order the test. [10]
Clinical Presentation
Screening “presents” as offers, results and family reactions—not as fever or rash. [14]
At the newborn window, families meet bloodspot, hearing and other early programme screens while still absorbing birth. Timing, consent quality and clear next steps matter as much as the assay. In infancy and preschool, growth, vision, developmental tools and catch-up of missed newborn steps appear in well-child visits. At school age and adolescence, opportunistic and school-linked screens sit beside autonomy and confidential care. [2] [20]
After a positive screen, families often present with fear, internet catastrophising, or a letter they only half understand. After a false-positive newborn screen, qualitative work describes lasting worry, altered bonding and lingering doubt even when confirmatory tests later clear the child. Your job is to name that harm, not dismiss it. [14] [21]
Incomplete coverage presents as mobile families, missing records, declined offers never revisited, or positive results with no owner for follow-up. A child who later becomes symptomatic after a prior negative screen presents a different problem: residual risk and new disease, not “the screen failed so ignore symptoms.” [4] [5]
Differential Diagnosis
When a screen is positive, the differential is not only “disease versus no disease.” Sort true target disease needing treatment; false positive with no disease on the reference standard; carrier or non-actionable variant depending on the programme; mild or late-onset form that may be overdiagnosis if treated as classic disease; and lab or sample error, wrong identity, or wrong cut-off for age. [4] [17] [21]
When a screen is negative but the child looks wrong, the differential expands to missed disease (false negative), wrong timing, disease outside the panel, and new-onset disease after the screen date. Never use a past negative screen as a reason to skip indicated diagnostic testing. [5] [24]
Distinguish programme failure (not offered, not completed, lost follow-up) from test failure (offered and done, still wrong answer). Both harm; the fix differs. [2]
Clinical & Bedside Assessment
Before every offer, say the five questions out loud—condition, test, early action, pathway, net benefit. If any answer is no, stop. [1] [2] [3]
Take a focused risk history that might justify selective screening: family diagnoses, consanguinity when relevant, migration and prior programme access, exposures, and prior incomplete screens. Check who holds parental responsibility and how results will be delivered. [2]
Assess understanding before consent. Families need plain language for: why we look; what a positive means (more tests, not a diagnosis); what a negative means (lower risk, not zero); and what happens next if they decline. Document the offer, the decision, and the follow-up owner. [12] [14]
Bedside red flags to pause opportunistic screening: the child is unstable and needs resuscitation, consent is not free, identity is uncertain, or the family is already mid-cascade from a prior false positive without a clear exit plan. [15] [24]
Investigations
Investigations here means how you evaluate and interpret screening data—not a shopping list of every paediatric assay. Disease-specific panels live on sibling pages. [5]
Performance metrics
Use the 2×2 definitions. Prefer likelihood ratios when you need to update risk for one child. Remember SnNOut and SpPIn heuristics mislead when prevalence and LRs are ignored. Continuous markers need cut-offs; ROC thinking shows the trade-off between sensitivity and specificity as the threshold moves. [5] [6] [7] [8]
Quality of published accuracy
STARD and QUADAS-type tools remind you to ask: was the reference standard fair, was the spectrum of children realistic, and were results interpreted without circular logic? Published sensitivity from a severe hospital series may not transfer to a well-baby clinic. [18] [19]
Confirmatory pathway
A confirmatory test must be available, timely, age-appropriate and owned by a named service. For time-critical newborn positives, delay is itself harm. For low-urgency school screens, over-rapid labelling without proper confirmation is the usual error. [20] [21]
Users’ guides to screening recommendations ask whether the guideline’s evidence actually links early detection to better child outcomes, not merely to more detection. [12] [13]
Management — Resuscitation
Screening is usually preventive, but a few results behave like emergencies. If a critically actionable newborn screen arrives while confirmatory samples are pending, treat the communication and the protective plan as time-critical: contact the family, involve the responsible specialist service, and follow local emergency protocols for the suspected condition. Do not invent disease-specific doses on this page—use the condition pathway and specialist advice. [20] [21]
Never delay ABCDE care to chase non-urgent screening paperwork. If a child presents acutely and was previously “screen negative,” manage the emergency first; the prior screen is background, not a shield. [24]
Severe parental distress after an unexpected positive is a clinical problem. Sit down, remove jargon, explain the next confirmatory step and timeframe, and arrange support. False-positive psychosocial harm is documented; dismissiveness is not care. [14]
Management — Definitive & Stepwise
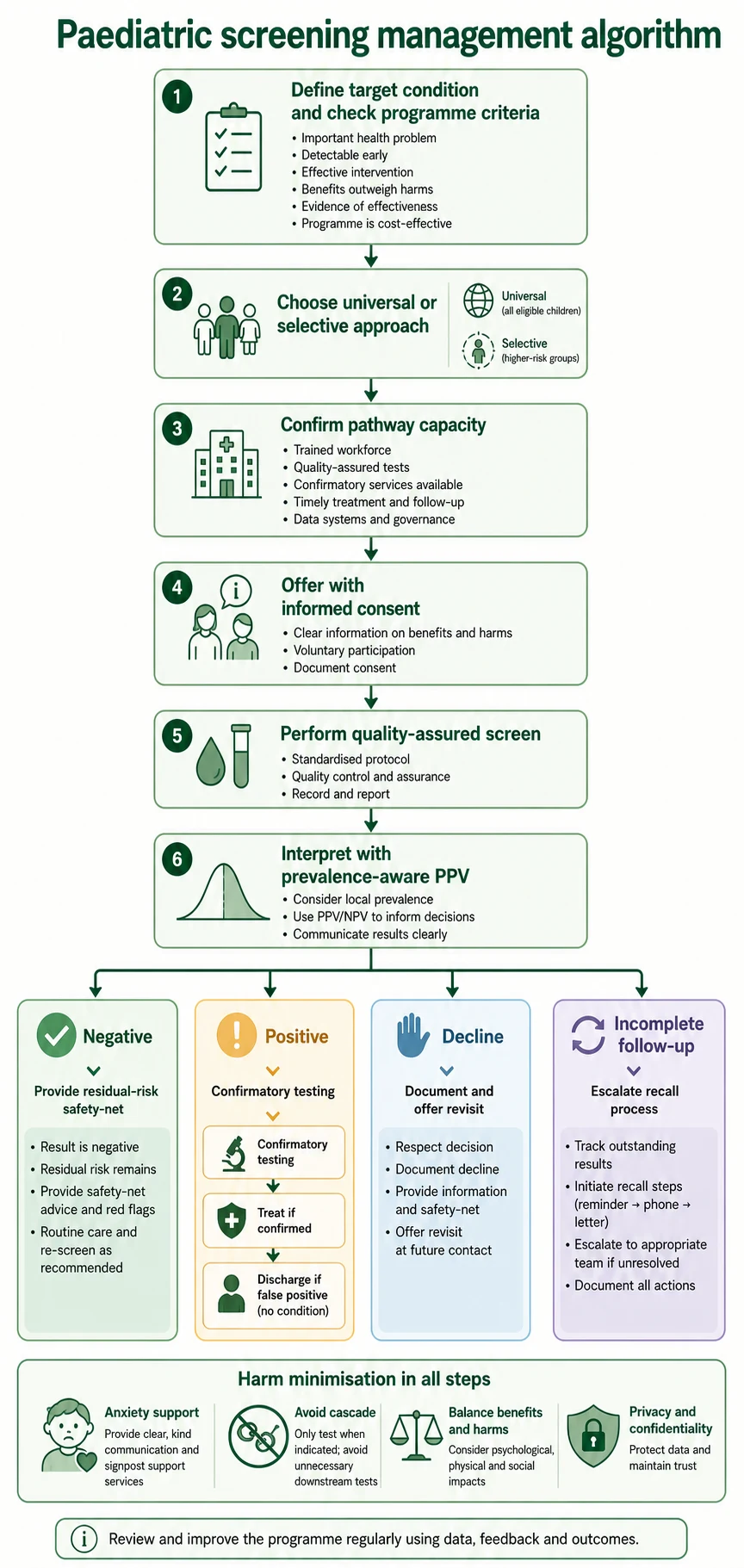
Work the pathway in order: define the target condition and child group; check programme criteria including harm and equity; choose universal versus selective based on prevalence; confirm pathway capacity before the first offer; obtain informed consent with false-positive and residual-risk language; perform a quality-assured test; interpret with prevalence-aware predictive values; then act on the branch—negative residual-risk safety-netting, positive confirmatory testing with a named owner, inconclusive protocol, non-coercive decline documentation, or active recall for lost follow-up—and audit coverage, yield, intervals and harms. [1] [2] [3] [5] [12] [14] [21]
Counselling scripts examiners want
Negative: “This result makes the target condition much less likely. It does not make every future problem impossible. If new symptoms appear, we assess them on their own.” [5]
Positive: “This is a screening flag, not a final diagnosis. The next step is a confirmatory test. Many flags clear. We will stay with you until that answer is clear.” [4] [14]
Decline: “You can decline. I will record that and explain what we might miss. You can restart later. I will not pressure you.” [12]
When not to start a screen
If detection will not change action, if pathway capacity is fantasy, if harms dominate, or if a commercial panel is being sold without programme evidence—do not start. “We can measure it” is not a criterion. [3] [15] [23]
Specific Subtypes & Scenarios
Newborn bloodspot. Teaches time-critical true positives, high false-positive counselling load, and governance of panel expansion. Condition lists and follow-up algorithms belong on the bloodspot sibling page; principles live here. [20] [21]
Newborn hearing. Classic universal early screen with a two-step audiology pathway. Residual risk after a pass still matters if later concerns arise. Detail sits on the hearing sibling page. [2] [4]
Developmental and behavioural tools. Screening tools differ from ongoing developmental surveillance. A pass does not erase caregiver concern. Tool-specific content sits on the developmental screening sibling page. [4] [15]
Growth and vision continuous measures. Cut-offs trade sensitivity for specificity; age norms matter. [5] [7]
Selective high-risk examples. Family-history or exposure-based strategies change prevalence and therefore PPV; they miss cases outside the risk group. [5] [4]
Commercial or expanded genomic panels in well children. Detection expands faster than proven childhood benefit. Apply full programme criteria and harm frameworks before you endorse. [1] [15] [21]
Cascade testing. After an index diagnosis, relatives may need targeted testing—this is not the same as offering a multi-disease panel to all well classmates. [1] [4]
School-entry and adolescent offers. Autonomy, confidential delivery of results, and school–health system handoffs become part of the pathway. [2] [12]
Complications & Pitfalls
Common pitfalls include treating screen positive as diagnosis; reassuring with sensitivity while ignoring low PPV; using a negative screen to dismiss new symptoms; screening without treatment access; losing families between positive result and confirmation; wrong-age norms or adult cut-offs; coercive consent that hides uncertainty; cascade testing after incidental findings without a stop rule; and expanding panels because technology can, not because children benefit. [1] [2] [3] [4] [5] [7] [12] [14] [15] [17] [20] [24]
Psychosocial harm after false-positive newborn screens is not theoretical; families describe ongoing worry. Build exit counselling into the pathway. [14]
Prognosis & Disposition
For a true positive on a high-value programme, prognosis tracks time to confirmation and time to effective treatment—own the clock. For a resolved false positive, disposition includes clear “you do not have this disease” language, optional psychosocial support, and return to usual care without indefinite limbo. [14] [21]
Programme prognosis is measured in population outcomes: fewer late presentations, acceptable false-positive burden, equitable coverage, and sustainable follow-up—not in the number of abnormalities detected alone. [3] [12]
If confirmatory care is unavailable locally, disposition is transfer of care or sample, specialist telehealth, or deliberate non-offer—not a hopeful letter with no appointment. [2]
Special Populations
Preterm and NICU infants. Timing, transfusions, parenteral nutrition and illness can alter screen performance and scheduling; use local neonatal protocols rather than copying the well-baby calendar blindly. [20]
Medical complexity. Baseline abnormal numbers and devices change what “screen abnormal” means; avoid naive interpretation. [15] [24]
Disability and neurodiversity. Tool choice and communication must fit the child; a generic questionnaire can misclassify. [15] [4]
Indigenous and equity-focused design. Same policy offer can still under-serve if transport, language and trust barriers are ignored. [2]
Migrant and refugee children. Reconstruct which programme screens were completed overseas; offer catch-up of high-value screens without assuming records are complete. [2] [16]
Out-of-home care. Clarify consent, ensure results reach a durable medical home, and chase incomplete follow-up aggressively. [2] [16]
Adolescents. Respect emerging autonomy, confidentiality limits, and the difference between public-health offers and personal diagnostic work. [12] [15]
Socioeconomic disadvantage. Missed appointments after a positive result are a safety issue; design recall that works offline as well as by app. [16]
Evidence, Guidelines & Regional Differences
Global intellectual spine. Wilson and Jungner remain the historical foundation. Andermann’s genomic-age review and Dobrow’s consolidated principles update criteria for modern programmes. Harris and USPSTF-style methods emphasise outcomes, harms and real-world implementation. Users’ guides teach how to read screening recommendations critically. [1] [2] [3] [12] [22]
Australia / Aotearoa New Zealand. Newborn bloodspot and hearing programmes are jurisdiction-organised public systems with local panels and follow-up services. Teach principles and check the current jurisdictional schedule; do not freeze a product list as eternal law. [20] [2]
United Kingdom. National screening appraisal language emphasises viability, effectiveness and appropriateness before rollout—use that governance framing in UK exams rather than inventing a frozen panel. [2] [3]
United States. USPSTF-style methods shape many preventive recommendations; newborn screening panel decisions use federal advisory processes such as RUSP nomination frameworks. State implementation still varies—name the level you mean. [3] [20]
Canada. Provincial and territorial delivery varies; Dobrow’s CMAJ consolidation is a useful Canadian-linked methods paper for principle language. [2]
Controversies. Expanded genomic newborn sequencing, commercial multi-disease panels, developmental tool thresholds, and low-value routine testing all force the same question: does early detection improve child outcomes enough to justify harms? European paediatric overuse statements push back on “more testing equals better care.” [1] [15] [16] [21] [23]
Public newborn screening programmes use jurisdictional panels and follow-up services. Check current local policy rather than memorising another country’s list. [20] [2]
Programme-level appraisal language (viability, effectiveness, appropriateness) is the exam-safe frame before rollout claims. [2] [3]
USPSTF-style evidence frameworks and RUSP-style newborn panel governance are high-yield US teaching anchors; Canadian delivery is provincial with shared principle language from methods papers such as Dobrow. [3] [20] [2]
Exam Pearls
- PPV falls when prevalence falls — say it early in any numbers viva. [5]
- Screening is a programme, not a lab slip. [2]
- Positive screen ≠ diagnosis; negative screen ≠ zero risk. [4]
- Sensitive first step, specific confirmation is classic two-step logic. [11]
- False positive ≠ overdiagnosis — different harms. [17]
- No pathway, no offer. [2] [21]
- Consent must include residual risk and false-positive possibility. [12] [14]
- Name the jurisdiction before quoting a funded panel. [20] [2]
- Symptoms after a negative screen restart diagnostic reasoning. [24]
- Detection without better outcomes is not success. [3] [12]
CATCH before you screen
References
- [1]Andermann A Revisiting Wilson and Jungner in the genomic age: a review of screening criteria over the past 40 years Bulletin of the World Health Organization, 2008.PMID 18438522
- [2]Dobrow MJ Consolidated principles for screening based on a systematic review and consensus process CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne, 2018.PMID 29632037
- [3]Harris R Reconsidering the criteria for evaluating proposed screening programs: reflections from 4 current and former members of the U.S. Preventive services task force Epidemiologic reviews, 2011.PMID 21666224
- [4]Grimes DA Uses and abuses of screening tests Lancet (London, England), 2002.PMID 11897304
- [5]Akobeng AK Understanding diagnostic tests 1: sensitivity, specificity and predictive values Acta paediatrica (Oslo, Norway : 1992), 2007.PMID 17407452
- [6]Akobeng AK Understanding diagnostic tests 2: likelihood ratios, pre- and post-test probabilities and their use in clinical practice Acta paediatrica (Oslo, Norway : 1992), 2007.PMID 17306009
- [7]Akobeng AK Understanding diagnostic tests 3: Receiver operating characteristic curves Acta paediatrica (Oslo, Norway : 1992), 2007.PMID 17376185
- [8]Deeks JJ Diagnostic tests 4: likelihood ratios BMJ (Clinical research ed.), 2004.PMID 15258077
- [9]Fagan TJ Letter: Nomogram for Bayes's theorem The New England journal of medicine, 1975.PMID 1143310
- [10]Pauker SG The threshold approach to clinical decision making The New England journal of medicine, 1980.PMID 7366635
- [11]Maxim LD Screening tests: a review with examples Inhalation toxicology, 2014.PMID 25264934
- [12]Barratt A Users' guides to the medical literature: XVII. How to use guidelines and recommendations about screening. Evidence-Based Medicine Working Group JAMA, 1999.PMID 10359392
- [13]Jaeschke R Users' guides to the medical literature. III. How to use an article about a diagnostic test. B. What are the results and will they help me in caring for my patients? The Evidence-Based Medicine Working Group JAMA, 1994.PMID 8309035
- [14]Tluczek A Psychosocial consequences of false-positive newborn screens for cystic fibrosis Qualitative health research, 2011.PMID 20852016
- [15]Størdal K Overtesting and overtreatment-statement from the European Academy of Paediatrics (EAP) European journal of pediatrics, 2019.PMID 31506723
- [16]Jankauskaite L Overuse of medical care in paediatrics: A survey from five countries in the European Academy of Pediatrics Frontiers in pediatrics, 2022.PMID 36177454
- [17]Newman-Toker DE A unified conceptual model for diagnostic errors: underdiagnosis, overdiagnosis, and misdiagnosis Diagnosis (Berlin, Germany), 2014.PMID 28367397
- [18]Bossuyt PM STARD 2015: an updated list of essential items for reporting diagnostic accuracy studies BMJ (Clinical research ed.), 2015.PMID 26511519
- [19]Whiting PF QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies Annals of internal medicine, 2011.PMID 22007046
- [20]Kemper AR Decision-making process for conditions nominated to the recommended uniform screening panel: statement of the US Department of Health and Human Services Secretary's Advisory Committee on Heritable Disorders in Newborns and Children Genetics in medicine : official journal of the American College of Medical Genetics, 2014.PMID 23907646
- [21]Goldenberg AJ Evaluating Harms in the Assessment of Net Benefit: A Framework for Newborn Screening Condition Review Maternal and child health journal, 2016.PMID 26833040
- [22]Schielen PCJI Historical Appreciation of World Health Organization's Public Health Paper-34: Principles and Practice of Screening for Disease, by Max Wilson and Gunnar Jungner International journal of neonatal screening, 2025.PMID 40700048
- [23]Grosse SD Screening for Neonatal Hyperbilirubinemia-First Do No Harm? JAMA pediatrics, 2019.PMID 31107538
- [24]Bordini BJ Overcoming Diagnostic Errors in Medical Practice The Journal of pediatrics, 2017.PMID 28336147