Paeds · preventive-and-community-paediatrics
Sun protection and skin cancer prevention
Also known as Photoprotection · Sunscreen counselling · UV protection children · Childhood skin cancer prevention · Indoor tanning prevention · Slip Slop Slap
Fellowship-level approach to childhood sun protection and skin-cancer prevention: UV biology, age-banded counselling, layered photoprotection, indoor tanning, vitamin D balance, high-risk phenotypes, and regional practice differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A caregiver asks at a well-child visit: “Is sunscreen enough for the beach this weekend?” The short clinical answer is no. Sun protection means reducing harmful ultraviolet (UV) dose while still supporting outdoor life. Skin-cancer prevention in paediatrics is mostly primary prevention — building habits before cumulative DNA injury becomes adult disease. [1] [2]
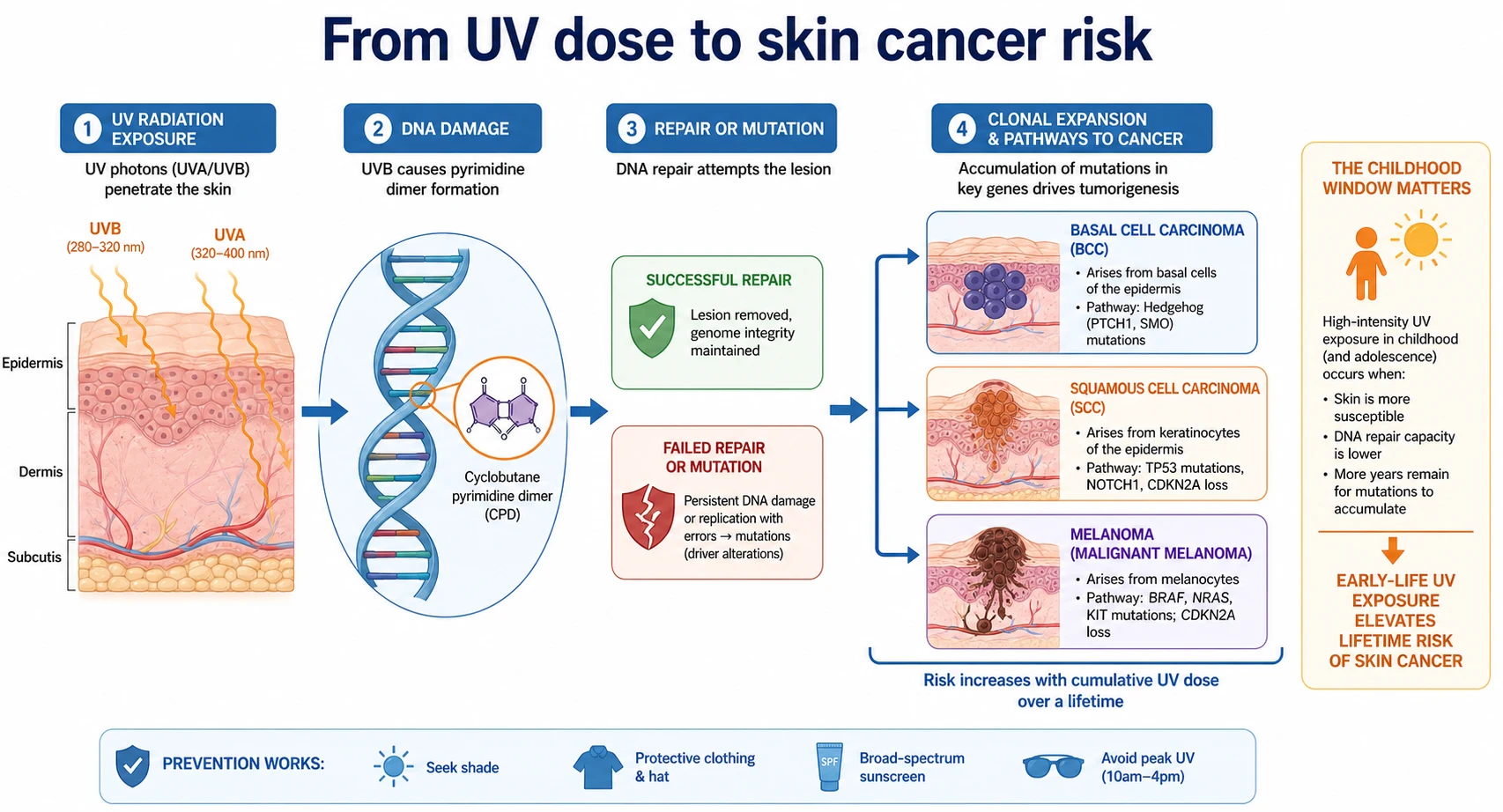
UV radiation from sunlight and artificial sources drives the three main skin cancers: basal cell carcinoma (BCC), squamous cell carcinoma (SCC) and melanoma. Children and adolescents are a critical window. Roughly a quarter of lifetime sun exposure often occurs before adulthood, and intense childhood exposure shapes later melanoma risk more than families realise. [2] [7]
Photoprotection is not the same as locking a child indoors. You want the child outside for play, sport and mental health — with a plan that stops sunburn and lowers long-term risk. That plan is layered behaviour, not a single product. [1] [4]
Classification
Separate three counselling axes: what UV does, who is most vulnerable, and how exposure is patterned. Mixing them confuses families and exams. [2] [6]
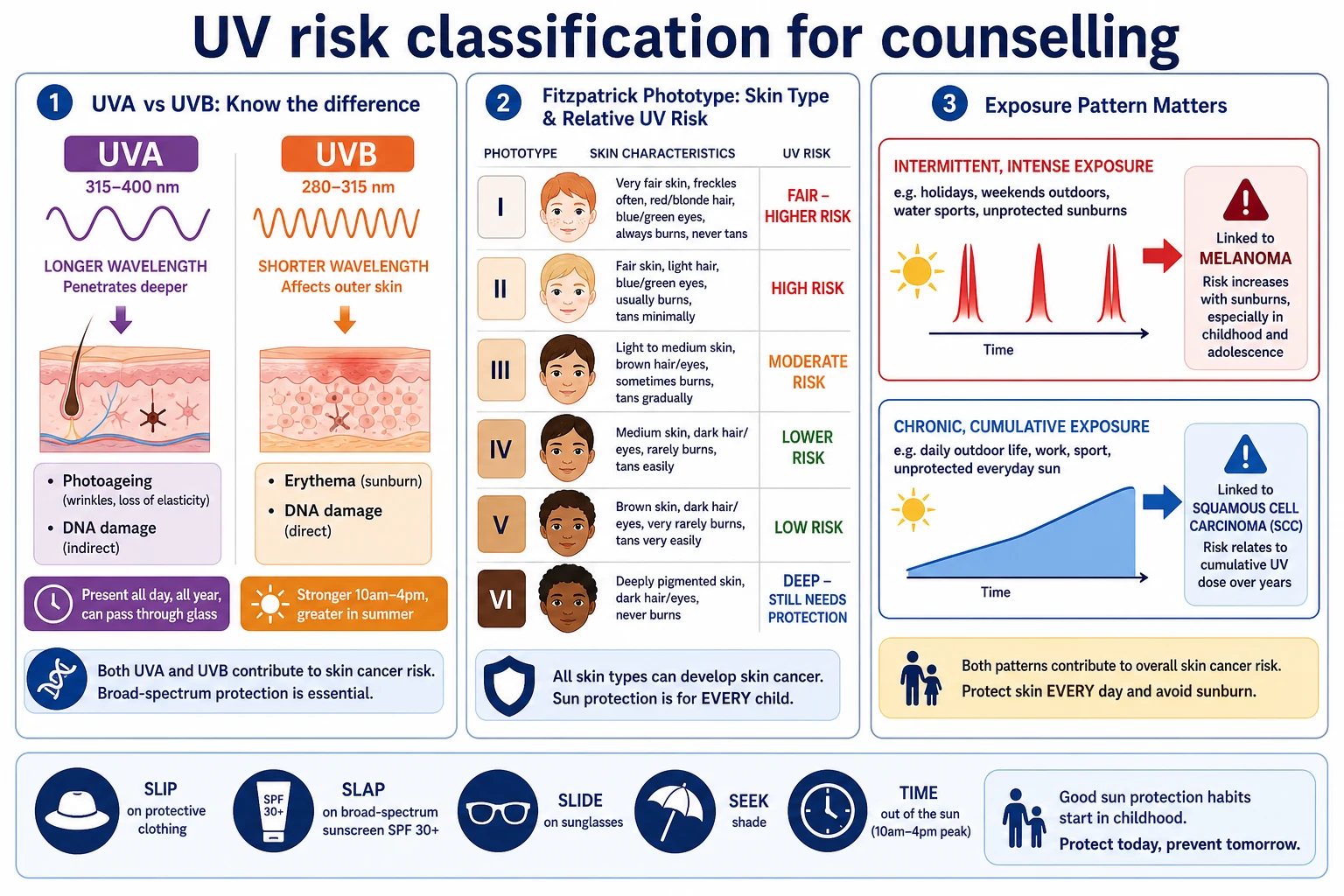
UVB is the main driver of sunburn (erythema) and is central to DNA damage that leads to skin cancer. UVA penetrates deeper, contributes to photoageing and also damages DNA; it passes through ordinary window glass more readily than UVB. Broad-spectrum products matter because both bands are clinically relevant. [2] [4]
Fitzpatrick phototype (I–VI) estimates how readily skin burns versus tans. Fair, freckled, red-haired children burn easily and need tighter plans. Darker phototypes still burn, still develop skin cancer, and still need protection — especially for eyes and for intense outdoor exposure. Phototype is a risk tool, not a racial stereotype. [2] [4]
Exposure patterns that change the message
- Beach, snow, sports day, holidays
- Strong link with sunburn history
- Important in melanoma risk messaging
- Outdoor work, daily high ambient UV
- Stronger classic link with SCC patterns
- Still relevant for children in high-UV regions
- Intentional high-intensity exposure
- Associated with melanoma risk
- No safe paediatric use
Epidemiology & Risk Factors
Skin cancer is among the most common cancers in fair-skinned populations, and incidence has been a major public-health problem for decades. Absolute rates vary by latitude, ambient UV, phenotype and behaviour. Australia and Aotearoa New Zealand sit at the hard end of ambient UV for many children. [2] [6]
Host factors raise risk: fair skin, freckling, light hair and eyes, numerous melanocytic naevi, personal or family history of melanoma, and rare genetic photosensitivity syndromes. Environmental factors include high ambient UV, altitude, reflective surfaces (water, sand, snow), outdoor sport, and time outdoors around solar noon. [2] [6]
Childhood sun exposure is not a minor footnote. Ecological and epidemiologic syntheses show that high childhood UV environments strongly influence later melanoma risk, even though adult exposure also matters. Intermittent exposure and sunburn history are repeatedly linked with melanoma risk in meta-analysis. [7] [8]
Indoor tanning adds avoidable risk. A large systematic review and meta-analysis found higher melanoma odds with ever use of tanning beds, with stronger association after more than ten sessions. Newer technology was not shown to be safe. Adolescents are a key target for prevention messaging. [9] [3]
Inequity shapes who gets protected. Cost of sunscreen and UPF clothing, school shade policy, language access, outdoor work for older teens, and cultural beauty norms around tanning all change adherence. Parent knowledge does not automatically become practice. [11] [13]
Pathophysiology
UV photons hit skin and create DNA lesions, classically cyclobutane pyrimidine dimers at dipyrimidine sites. If repair fails, mutations accumulate. Over years this can drive BCC, SCC and melanoma pathways. You do not need to recite every molecular step in a viva — you do need to explain why dose reduction in childhood matters. [2] [6]
Sunburn is acute inflammation after excessive UVB-dominant injury. It is a visible warning, not the only harmful exposure. Sub-erythemal doses still damage DNA. That is why “I only go pink, I don’t blister” is not a safety plan. [2] [4]
Epidemiology maps onto mechanism. Intermittent intense recreational exposure and sunburn history fit melanoma risk patterns in many analyses, while chronic cumulative exposure fits classic SCC patterns more closely. BCC sits between these stories depending on site and population. The counselling translation is simple: stop burning, reduce peak dose, and keep protection consistent. [6] [8]
Cutaneous vitamin D synthesis also needs UVB. That fact is often twisted into a false choice: either tan deliberately or become deficient. The clinical resolution is diet, fortified foods and supplements when indicated, while still using photoprotection. Intentional tanning is not a paediatric vitamin D prescription. [1] [2]
Clinical Presentation
Most “presentations” are preventive. The family wants a brand name, a school-camp letter, or permission to skip hats. Your job is a concrete plan for the next high-UV day. [3] [10]
- Infant or toddler: “Can we use sunscreen yet?” Lead with shade, pram covers that allow airflow, long sleeves and timing; use sunscreen on small exposed areas when physical protection cannot cover everything, following age-appropriate product labelling and clinician judgement. [1] [4]
- School-age athlete: burns after Saturday sport because sunscreen was applied once at 8 am. Teach amount, reapplication and clothing. [4] [12]
- Adolescent: wants a pre-formal tan or has used a salon. Address appearance motives directly and state that indoor tanning is not safe. [3] [9]
Acute presentations include painful erythema, blistering, facial swelling, photophobia after snow or water reflection, and coexisting heat illness. Severe burns in infants are a capacity and safety concern, not only a cream problem. [4]
High-risk phenotypes may present with extreme freckling, many naevi, albinism, transplant immunosuppression, or a family melanoma story. These children need tighter plans and often dermatology partnership. [2] [4]
Differential Diagnosis
Not every red patch after outdoor time is “just sunburn.” [4]
- Phototoxic drug reaction (for example some antibiotics or retinoids) can exaggerate burn on exposed skin.
- Photoallergic dermatitis is less common but itchy and eczematous.
- Contact dermatitis from plants, sunscreen ingredients or sports equipment can mimic or coexist.
- Viral exanthem or heat rash may be mislabelled after a sunny day.
- Changing pigmented lesion is a different pathway: examine and refer rather than only counselling SPF. [4]
After high UV exposure, also think about heat exhaustion/heat stroke and photokeratitis. Those need different immediate actions than aloe for mild sunburn. [4]
Clinical & Bedside Assessment
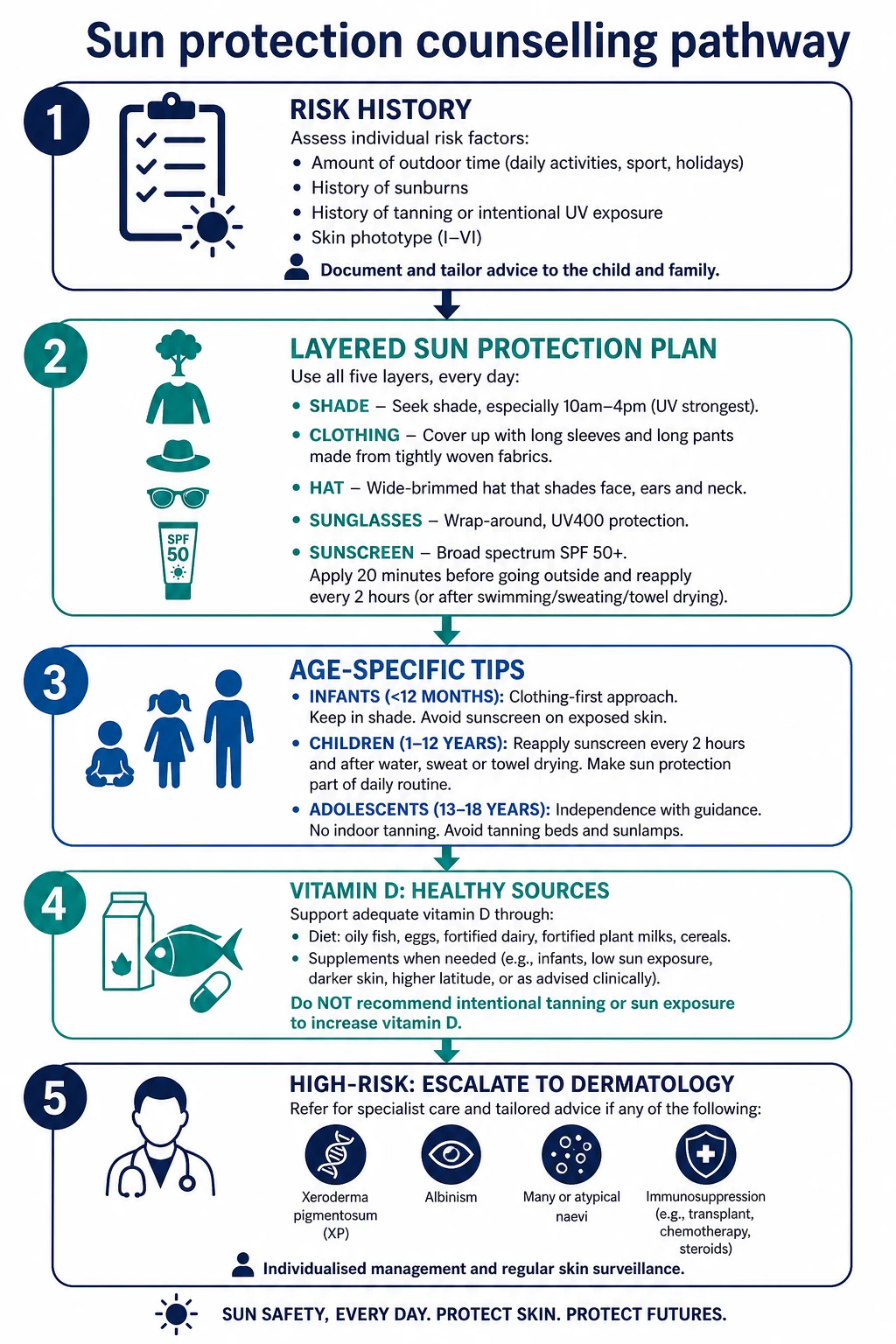
Take a behavioural UV history, not a brand quiz. [3] [4]
- When is the child outdoors, and for how long around the middle of the day?
- Water, snow, altitude or reflective surfaces?
- Hat, long sleeves, shade access at school or sport?
- Sunscreen: product type, amount, reapplication after water or sweat?
- Any indoor tanning, spray tans used as false reassurance, or intentional baking?
- Medicines that increase photosensitivity?
- Prior blistering burns, freckling pattern, family skin-cancer history? [3] [4]
Examine exposed skin for freckling, burn, blistering and naevus pattern. Look at the lips, ears, neck and dorsal hands — families often miss these. Ask about eye protection. For adolescents, ask without a parent in the room if tanning-bed use is possible. [3] [4]
Five-minute sun-protection assessment
Exposure map
Sport, commute, lunch outdoors, holidays, snow or water days.
Physical barriers
Shade, timing, UPF clothing, wide-brim or legionnaire hat, wraparound sunglasses.
Sunscreen reality check
Broad-spectrum product, enough volume, water resistance, reapplication plan.
Tanning and beauty pressure
Salons, intentional midday tanning, social media norms.
Vitamin D and diet
Intake, supplements if indicated; never prescribe intentional burning.
Teach-back
Ask the family to restate the plan for the next outdoor event.
Investigations
Routine sun-protection counselling needs no blood test and no imaging. The work is history, examination and a written or verbal plan. [1]
Consider 25-hydroxy vitamin D when there are risk factors for deficiency: limited intake, exclusive breastfeeding without supplementation in infancy, dark skin at high latitude with low intake, malabsorption, or clinical concern for rickets/osteomalacia pathways. A low level is a nutrition problem to fix — not a licence for unprotected tanning. [1] [2]
Refer to dermatology for suspected melanoma, atypical evolving lesions, xeroderma pigmentosum pathways, complex naevus syndromes, or severe photosensitivity. Do not invent a universal mole-mapping protocol for every freckled child. [4]
Management — Resuscitation
Severe acute UV injury is uncommon in routine clinic, but you will see it after camps, beaches and snow trips. [4]
- Assess airway, breathing, circulation if the child is systemically unwell or heat-stressed.
- Cool the skin with tepid water; avoid ice that freezes damaged skin.
- Give age-appropriate analgesia; assess hydration and oral intake.
- Leave intact blisters when possible; keep skin clean; counsel about secondary infection signs.
- For eye pain, photophobia or vision change after intense UV (especially snow/water), arrange urgent eye assessment.
- Safety-net infants, extensive blistering, facial involvement, inability to drink, or caregiver inability to manage care. [4]
Do not let acute burn care end without a prevention reset for the next exposure. [3]
Management — Definitive & Stepwise
This is the core fellowship skill: a stepwise, layered plan that a family can actually run. [1] [4]
Step 1 — Make outdoor life the goal
Frame protection as enabling play and sport, not as fear. Families disengage when advice sounds like house arrest. [1] [11]
Step 2 — Layer protection (in order families can remember)
- Shade — trees, tents, built shade, UV-aware positioning.
- Timing — when possible, move intense outdoor blocks away from peak UV.
- Clothing and hat — densely woven long sleeves, rash vest for water, wide-brim or legionnaire style for ears and neck.
- Sunglasses — wraparound UV-protective lenses.
- Sunscreen — broad-spectrum, adequate amount, reapply after swimming, towelling or about two hours of ongoing exposure. [1] [4]
In Australia the public mnemonic is Slip, Slop, Slap, Seek, Slide (clothing, sunscreen, hat, shade, sunglasses). Use local language your families already hear. [4]
Step 3 — Teach sunscreen technique, not just SPF number
A high SPF fails if the child gets a pea-sized smear. Teach enough product for exposed skin, water-resistant formulations for sport/swim, and reapplication. Sunscreen is a last layer on uncovered skin, not a full-body replacement for clothes. [4] [5]
Regular sunscreen use can become a lasting habit after structured programmes, and randomised follow-up from the Nambour setting showed fewer melanomas with regular versus discretionary use in adults — supporting the public-health case for consistent application. Translate carefully: paediatric counselling still prioritises multi-layer behaviour. [5] [14]
Step 4 — Age-band the advice
- Infants: physical protection first; minimise direct peak sun; use sunscreen on small exposed areas when shade and clothing cannot cover fully, with age-appropriate products. [1] [4]
- Toddlers/preschool: hat battles and water play — plan for reapplication and rash vests.
- School-age: sport and schoolyards — written plans, shade policy, pack sunscreen in the kit. [12]
- Adolescents: address tanning culture and indoor tanning directly; negotiate autonomy with non-negotiables. [3] [9]
Step 5 — Vitamin D without intentional UV
Recommend dietary sources and supplements according to local age guidance when intake or risk factors warrant it. Do not tell families to “get 20 minutes of strong midday sun without protection” as a blanket rule. That message collides with skin-cancer prevention and is especially unsafe in high-UV regions and fair phototypes. [1] [2]
Step 6 — High-risk escalation
For albinism, xeroderma pigmentosum, heavy immunosuppression, prior melanoma in the family with high-risk phenotype, or extreme freckling/naevus burden: stricter clothing, rigorous shade, dermatology (and often ophthalmology) pathways, and school support letters. [2] [4]
Specific Subtypes & Scenarios
Beach or pool day. Rash vest, hat that stays on in wind, shade tent, water-resistant sunscreen, reapply after swimming, fluids and heat awareness. [4]
Snow sport. High UV plus reflection; goggles/sunglasses and face protection are mandatory teaching points. [2]
School sports carnival. Single early application fails. Provide a reapplication plan and clothing strategy. School-based interventions can improve protection behaviours when practical. [11] [12]
Adolescent salon tanning. State the melanoma association clearly. Offer alternatives (clothing style, spray tan if they insist on colour) without endorsing UV beds. [9] [3]
Photosensitising medicines. Review timing of outdoor exposure and tighten physical protection while the drug is used. [4]
Rural outdoor life. Practical clothing and work-pattern timing may matter more than boutique products. [6]
Complications & Pitfalls
Other traps: [4]
- SPF worship without broad-spectrum coverage and behaviour change. [4]
- False security after one application under intense midday UV. [4]
- Product reactions blamed on “all sunscreen,” leading to total abandonment rather than formulation change and clothing emphasis. [4]
- Delayed review of a changing mole because the visit was only about holiday sunscreen. [4]
Prognosis & Disposition
Most well children leave with a home plan and no follow-up beyond routine care. The “prognosis” that matters is lifelong: fewer burns now, lower cumulative injury, better adult habits. Structured programmes can shift behaviour; Nambour follow-up showed that regular use habits can persist after intervention. [11] [14]
After severe sunburn, arrange review if healing is poor, infection is suspected, or the social setting looks unsafe. High-risk phenotypes need longitudinal dermatology disposition, not one-off advice. [4]
Public-health disposition means consistent messages across maternity, primary care, schools and sport clubs. Mixed advice destroys adherence. [1] [10]
Special Populations
Indigenous children in high-UV regions need practical, respectful messaging and access to shade and products — not blame for outdoor cultural life. [6]
Socioeconomic disadvantage. Cost is real. Prioritise shade, clothing and school policy; help families choose affordable broad-spectrum products; avoid shaming brand choices. [13]
Migrant and refugee families moving into high-UV climates may lack local risk literacy. Explain ambient UV differences plainly. [2]
Disability and sensory difference. Some children cannot tolerate hats or cream textures. Adapt with UPF clothing, shade and gradual desensitisation plans. [4]
Immunocompromised children (transplant, chemotherapy) need stricter photoprotection and often specialist dermatology input. [2]
Gender and appearance pressure can drive tanning in adolescents of any sex. Address motives, peers and social media without mockery. [3] [9]
Out-of-home care. Multiple caregivers need one written plan so protection does not depend on who is rostered. [13]
Evidence, Guidelines & Regional Differences
Landmark paediatric guidance remains the AAP 2011 policy and technical report on UV hazards in children and adolescents, with later counselling guidance on sun protection and indoor tanning (2017) and practical synthesis in 2023. These documents emphasise multi-method protection, outdoor activity, vitamin D without intentional tanning, and strong opposition to indoor tanning for youth. [1] [2] [3] [4]
Epidemiologic pillars: Armstrong and Kricker on UV-related skin-cancer patterns; Whiteman on childhood exposure and melanoma; Gandini meta-analysis on intermittent exposure and sunburn; Colantonio meta-analysis on indoor tanning. [6] [7] [8] [9]
Intervention evidence: school and parent-focused programmes can improve knowledge and some behaviours; effects vary by design and setting. Habit formation after structured daily-use programmes is supported by Australian trial follow-up. [11] [12] [14]
Sunscreen and melanoma: Green and colleagues’ long-term Nambour follow-up found fewer melanomas with regular versus discretionary sunscreen use in adults randomised years earlier — a key piece of evidence supporting regular use as part of prevention. [5]
High ambient UV makes layered protection a default lifestyle message. Cancer Council SunSmart language (Slip Slop Slap Seek Slide) is the public frame many families already know. Be especially careful not to recommend intentional unprotected midday sun for vitamin D in fair children. [4] [5]
Core principles are shared: reduce UV dose, prevent burn, ban intentional artificial tanning for minors, protect eyes, and fix vitamin D nutritionally. Local product labels, school rules and ambient UV change the operational details. [2] [6]
Exam Pearls
- Layers beat SPF alone. Shade, timing, clothes/hat, sunglasses, sunscreen. [1]
- Childhood intermittent intense exposure is central to melanoma-risk counselling. [7] [8]
- No indoor tanning for children or adolescents. [3] [9]
- Infants: physical protection first. [1]
- Reapply after water, towel and prolonged exposure; teach amount, not brand snobbery. [4]
- Vitamin D ≠ intentional tan. Diet and supplements when indicated. [1] [2]
- Water, snow, altitude multiply dose. [2]
- High-risk phenotypes need stricter plans and specialist links. [2] [4]
- Enable outdoor play — do not pathologise daylight. [1]
- Teach-back the next real event (sports day, beach, snow trip). [3] [13]
SUNSAFE plan
References
- [1]Council on Environmental Health Ultraviolet radiation: a hazard to children and adolescents Pediatrics, 2011.PMID 21357336
- [2]Balk SJ Ultraviolet radiation: a hazard to children and adolescents Pediatrics, 2011.PMID 21357345
- [3]Balk SJ Counseling on Sun Protection and Indoor Tanning Pediatrics, 2017.PMID 29127209
- [4]Balk SJ Sun Protection Pediatrics in review, 2023.PMID 37002351
- [5]Green AC Reduced melanoma after regular sunscreen use: randomized trial follow-up Journal of clinical oncology, 2011.PMID 21135266
- [6]Armstrong BK The epidemiology of UV induced skin cancer Journal of photochemistry and photobiology. B, Biology, 2001.PMID 11684447
- [7]Whiteman DC Childhood sun exposure as a risk factor for melanoma: a systematic review of epidemiologic studies Cancer causes & control, 2001.PMID 11227927
- [8]Gandini S Meta-analysis of risk factors for cutaneous melanoma: II. Sun exposure European journal of cancer, 2005.PMID 15617990
- [9]Colantonio S The association of indoor tanning and melanoma in adults: systematic review and meta-analysis Journal of the American Academy of Dermatology, 2014.PMID 24629998
- [10]Balk SJ Counseling parents and children on sun protection: a national survey of pediatricians Pediatrics, 2004.PMID 15466105
- [11]Baig IT A Review of the Impact of Sun Safety Interventions in Children Dermatology practical & conceptual, 2023.PMID 36892334
- [12]Li M Sun Safety in Elementary School: Trialing Strategies for Keeping Children Protected Journal of cutaneous medicine and surgery, 2023.PMID 37947200
- [13]Akca G The Knowledge, Attitudes, and Practices of Parents Regarding Sun Protection for Their Children Advances in skin & wound care, 2024.PMID 38767427
- [14]van der Pols JC Long-term increase in sunscreen use in an Australian community after a skin cancer prevention trial Preventive medicine, 2006.PMID 16325898