Paeds · preventive-and-community-paediatrics
Toddler health supervision: 1 to 3 years
Also known as Toddler well-child visit · 1 to 3 year health supervision · 12 to 36 month preventive care · Toddler Bright Futures visit · Toddler health check
Fellowship approach to toddler (12–36 months) health supervision: growth trajectories, developmental surveillance and autism screening, injury and oral-health anticipatory guidance, feeding and sleep, iron and lead risk assessment, positive discipline, equity and safeguarding, with regional schedule differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
T.O.D.D.L.E.R. visit
Overview & Definition
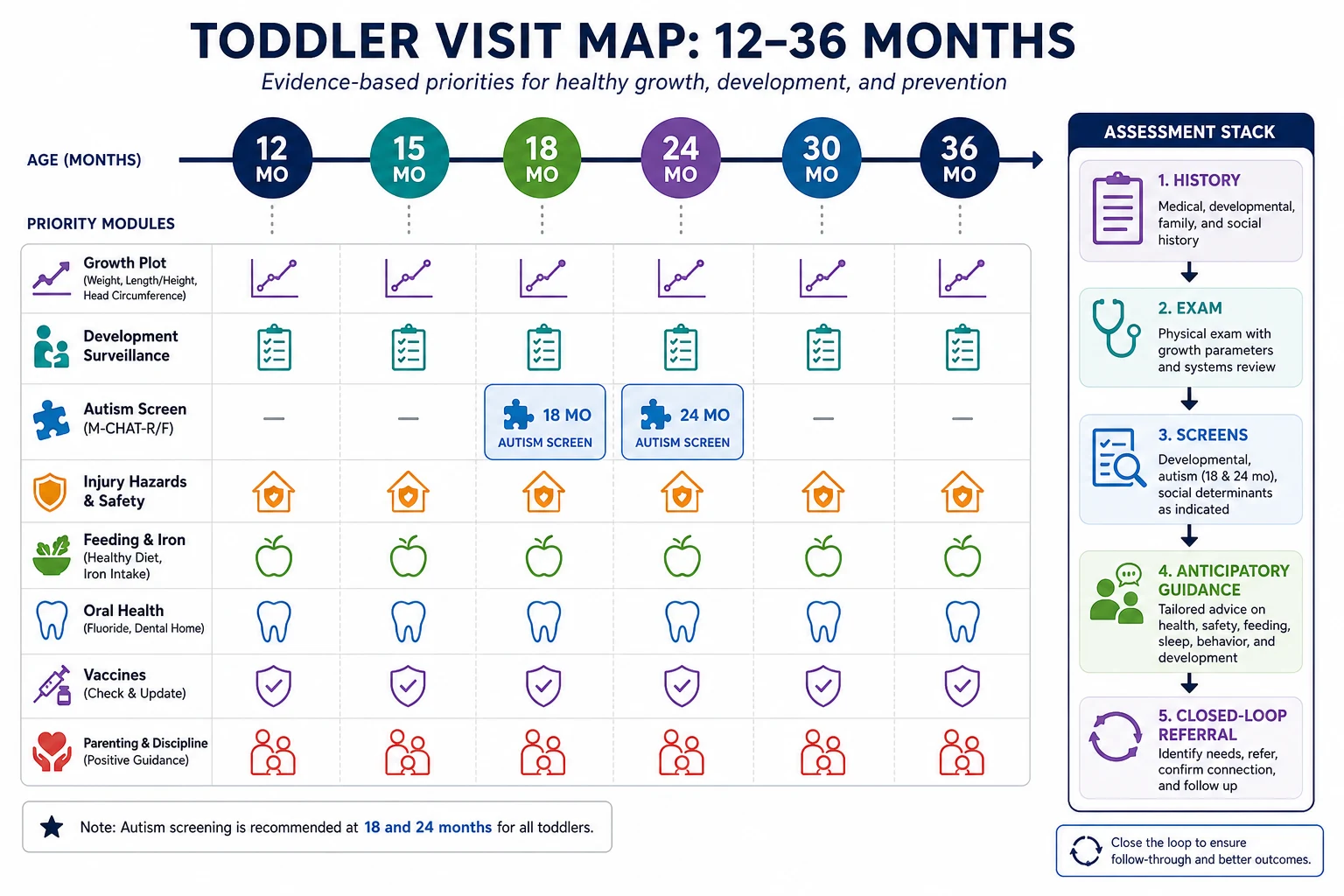
Picture an 18-month-old climbing off the parent’s lap while you try to open the chart. The parent wants “the needles done.” Your real job is broader. Toddler health supervision is structured preventive care for children from about 12 to 36 months. It combines measurement, developmental surveillance, autism-specific screening at recommended ages, oral health, injury prevention, feeding and sleep guidance, iron and lead risk assessment, immunisation reconciliation, and family psychosocial care. [1] [2]
AAP preventive periodicity recommendations organise these visits as a repeating package across 12, 15, 18, 24, 30 and 36 months rather than a single birthday ritual. Local child-health books in Australia and Aotearoa New Zealand, UK Healthy Child Programme contacts, and Canadian tools such as the Rourke Baby Record use different forms but the same idea: find problems while early services still change trajectories. [1]
This page owns the toddler package. Cross-link dedicated leaves for full immunisation schedules, deep developmental assessment tools, growth charting mechanics, and full child-protection workups rather than hiding whole second chapters here. [1] [2]
Classification
Sort the visit by purpose and by finding. [1] [2]
By purpose. Full well-child toddler visit. Catch-up after missed care. Opportunistic preventive add-on during a mild illness review. Hybrid telehealth check-in that still needs in-person measurement and exam for complete supervision. [1]
By finding. Normal with anticipatory guidance only. Isolated language lag. Multi-domain delay. Social communication pattern concerning for autism. Faltering growth or rising weight trajectory. Iron deficiency risk. Lead risk. Early childhood caries. Incomplete immunisation. Safeguarding concern. Medical complexity needing adapted goals. [2] [4] [5]
Surveillance versus screening versus evaluation. Surveillance is continuous: ask, watch, document every encounter. Screening uses a validated tool at key ages or on concern — including broad developmental tools and autism-specific tools such as M-CHAT-R/F with follow-up interview. Evaluation is specialist or multidisciplinary work that can diagnose and open early intervention. A positive screen is a referral trigger, not a diagnosis. [2] [4] [18]
Epidemiology & Risk Factors
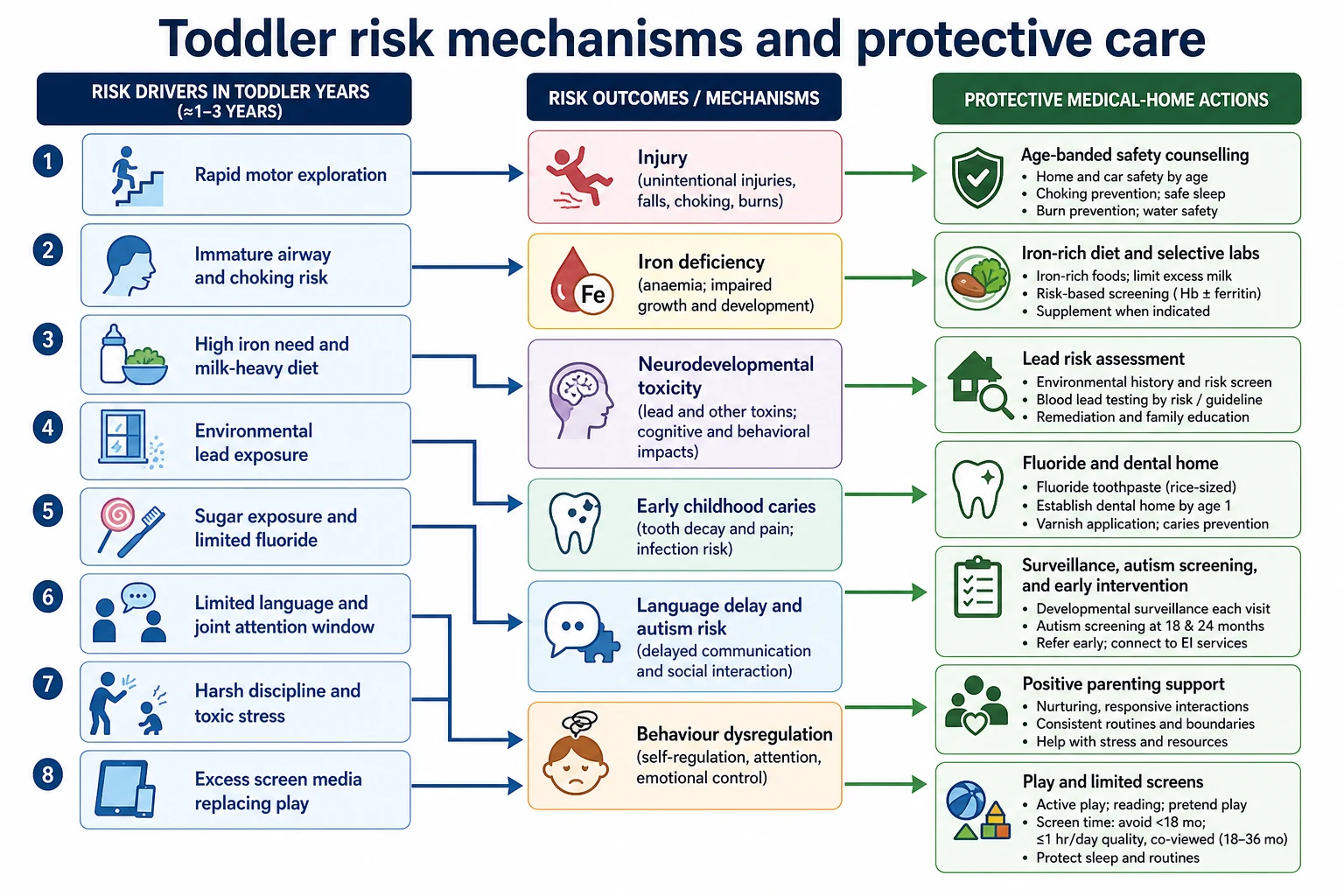
Injury mechanisms shift as walking, climbing and curiosity explode. Falls, choking, drowning, burns, poisoning and passenger restraint errors peak or change pattern across the second and third years. Office-based anticipatory guidance targets the hazards that match the child’s current skills. [12] [9]
Families who miss well-child visits often carry the same burdens that raise risk: poverty, transport barriers, housing instability, language discordance and fragmented out-of-home care. Those children have higher rates of incomplete immunisation, untreated caries, iron deficiency risk and delayed developmental support. Food insecurity links to higher health-care use and must be asked about directly. [15]
Iron deficiency risk rises with prolonged exclusive milk diets, delayed introduction of iron-rich solids, premature birth history and some dietary patterns. Lead exposure clusters with older housing, renovation dust, contaminated soil or water, and some imported products; there is no identified safe blood lead level for neurodevelopment. [5] [6]
Early childhood caries rates are higher in Indigenous communities and in families with limited fluoride access or frequent sugar exposure. Language delay and later autism diagnosis timing make the toddler window high-stakes for surveillance. Excess screen media in under-twos and toddlers competes with serve-and-return talk that builds language. Harsh discipline associates with harm; positive parenting is a clinical topic, not optional soft advice. [16] [11] [10] [14]
Pathophysiology
Between one and three years, motor exploration races ahead of hazard judgement. An immature swallow and small airway turn grapes, nuts, hard sweets and coins into choking threats. Rapid brain and language development make early intervention timing biologically important — plasticity is real, and delayed referral wastes it. [12] [2]
Iron deficiency impairs oxygen delivery and affects toddler behaviour and development even before frank anaemia. Lead is absorbed more readily in young children and injures developing neural systems at low exposures; primary prevention of sources beats late chelation of mild elevations. [5] [6]
Frequent sugar exposure, prolonged bottle use and limited fluoride drive early childhood caries through biofilm acid attack on enamel. Night-waking and failed sleep consolidation raise family stress and daytime behaviour problems. Coercive feeding around picky eating can worsen intake battles without improving growth. Excessive early screen media displaces joint attention and conversation. Toxic stress from maltreatment or harsh discipline alters regulation and attachment. [7] [8] [11] [10]
Clinical Presentation
Many toddlers look well. Caregivers may present for “needles,” tantrums, night-waking, picky eating or “not talking yet.” Listen for quieter signals: limited joint attention, few words or phrases for age, no pointing or showing, ignoring name, walking with a limp, mouth pain, or a flat weight curve despite a chubby appearance. [2] [3]
Autism-spectrum concerns may appear on surveillance or M-CHAT-R/F before parents volunteer them. Iron deficiency may hide in a diet history of excess milk and few iron-rich foods more than in obvious pallor. Lead exposure is often asymptomatic. Early caries shows on lift-the-lip inspection before pain. Safeguarding may present as inconsistent injury stories, delayed care or fearfulness. Food insecurity may present as running out of food rather than thinness alone. Hearing or vision problems may be mislabelled as behaviour. [4] [5] [6] [8] [15]
Differential Diagnosis
Tantrums and “no.” Normal toddler autonomy versus developmental red flags versus autism-related social communication difference versus sleep debt versus pain (including dental). Watch joint attention and language quality, not only volume of protest. [2] [3] [10]
Picky eating. Physiologic neophobia with normal growth versus true inadequate intake and faltering growth versus excessive milk crowding out solids. Plot first; do not treat a normal trajectory as disease. [5] [17]
Language concern. Isolated speech-language delay versus hearing impairment versus autism versus global developmental delay versus extreme psychosocial deprivation. Keep hearing on every list. [2] [3]
Sleep disruption. Primary behavioural night-waking versus pain, iron deficiency symptoms, unsafe sleep regression, or family stress. Do not reintroduce soft bedding or shared sleep hazards as “solutions.” [5]
Injury. Developmental stage-appropriate accident versus supervision gap versus inflicted injury. Pattern, delay in presentation and story consistency matter. [13]
Growth concern. Measurement error, nutritional insufficiency, chronic disease, neglect, or early excess weight trajectory. Use WHO standards for length/height, weight and age; comment on trajectory. [17] [20]
Clinical & Bedside Assessment
Start with agenda-setting: “What worries you most today?” and “Any concerns about talking, walking, hearing, seeing, sleep, eating or behaviour?” Watch the toddler: gait, fine motor play, joint attention, words or phrases, pointing, stranger response and caregiver interaction. [2] [3]
Growth. Measure weight and length (or standing height when technique is reliable). Plot on WHO Child Growth Standards used by your service. Read trajectory across visits, not a single percentile. Head circumference remains relevant early in the band when indicated. Rising BMI-for-age later in the band needs early lifestyle counselling without adult cut-offs. [17] [20] [1]
Development and autism screening. Use evidence-informed milestones rather than family folklore. Deploy validated general developmental screens per local programme. For autism risk in the supported toddler window, M-CHAT-R/F with follow-up interview risk-stratifies; meta-analysis supports its screening role while reminding you that sensitivity and specificity are imperfect and clinical concern still counts. A positive screen means timely referral and interim supports — not “watch until preschool.” [2] [3] [4] [18]
Mouth. Lift the lip. Look for white spots, cavities, pain or abscess. Ask about brushing with fluoride toothpaste in an age-appropriate smear amount, bottle or sippy cup with sweet drinks, and whether a dental home exists. Fluoride varnish belongs only within trained local programmes. [7] [8]
Exam pragmatism. In a mobile toddler, examine what you can: skin, gait, ears, heart, soft neurologic signs, and age-appropriate genital exam when indicated. Opportunistic does not mean incomplete documentation. [1]
Safety and lifestyle. Car seat type and position, water safety, falls, burns, poisoning storage, choking hazards, second-hand smoke, sleep routine, and screen media. Media guidance for young children emphasises limited high-quality co-viewed content, not unrestricted solo screens. Promote play as a developmental intervention. [9] [12] [11] [14]
Discipline. Ask how caregivers handle tantrums. Counsel against corporal punishment and harsh verbal shaming. Teach positive strategies: clear limits, praise for wanted behaviour, time-in or brief time-out used calmly, and caregiver self-regulation. [10]
Psychosocial risk. Food security, housing, caregiver mental health, intimate partner violence cues and who else cares for the child. Models such as SEEK show that structured psychosocial inquiry can change primary-care practice. Use professional interpreters when language is discordant — never the toddler or a sibling. [19] [15] [22]
Investigations
Most thriving asymptomatic toddlers need no blood test. Investigate when the story, risk or examination demands it. [1] [5]
Iron. Risk-based assessment and prevention dominate: iron-rich diet, appropriate milk volumes, and testing when risk or findings (pallor, excess milk, poor growth, developmental concern) justify haemoglobin or iron studies. Do not invent a universal lab age not supported by your cited local pathway. Baker and colleagues frame diagnosis and prevention for 0–3 years. [5]
Lead. Primary prevention of sources is first. Testing follows risk, geography and local public health policy; action levels are jurisdiction-specific. Do not invent a single global action number from memory. There is no identified safe blood lead level for the developing brain. [6]
Hearing and speech. Audiology and speech pathology after language concerns, failed screens or caregiver worry. [2]
Developmental evaluation. Formal assessment or early-intervention referral after failed screens or strong clinical concern. Do not wait for a perfect tool score. [2] [4]
Dental. Urgent dental referral for pain, swelling or abscess; routine dental home for all. [8]
Vision. Refer for strabismus, asymmetric red reflex or persistent visual concern; follow local office-screening capability. [1]
Avoid shotgun metabolic panels in an asymptomatic thriving toddler with a normal trajectory. [1]
Management — Resuscitation
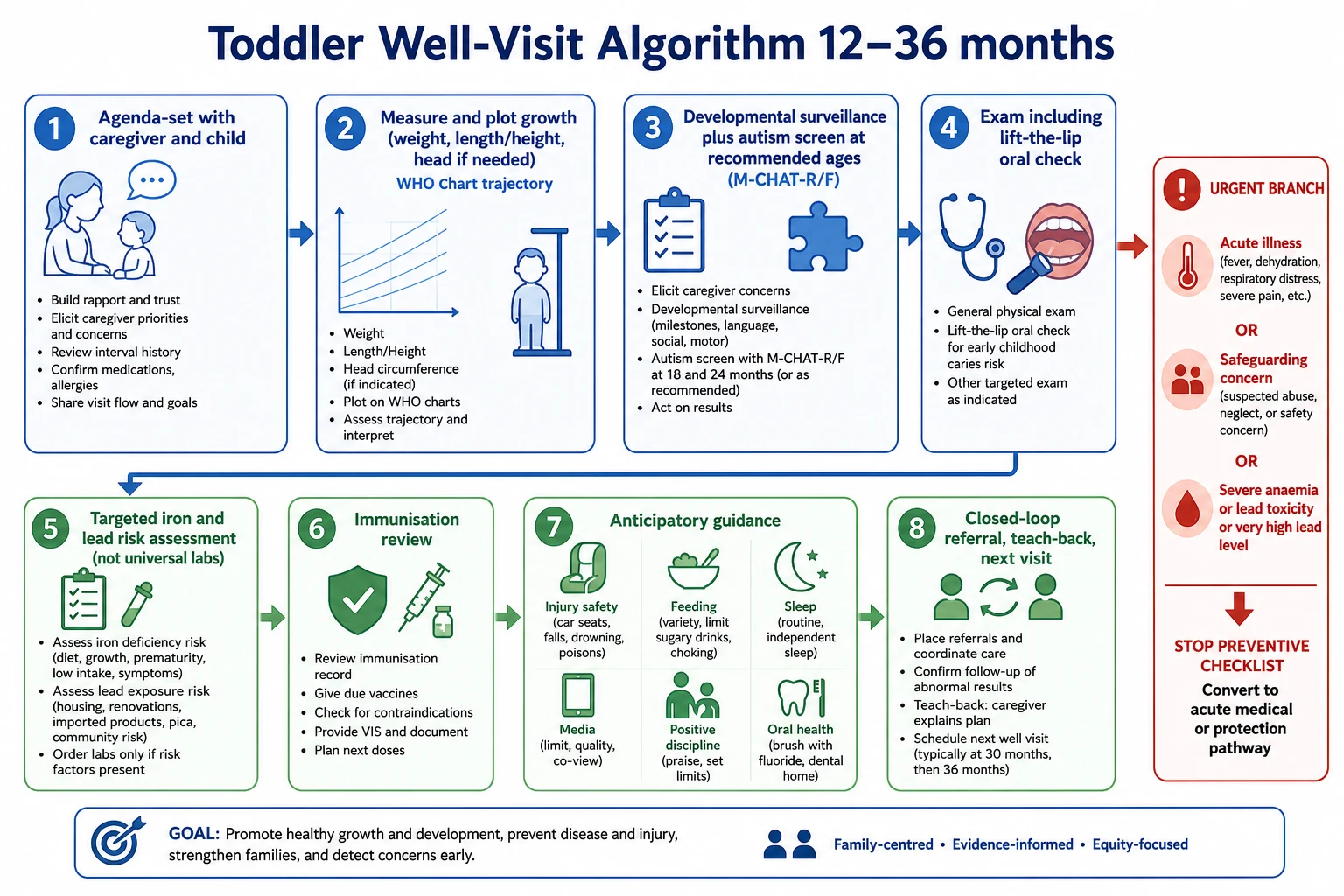
A well-child clinic still finds emergencies. Respiratory distress, shock, seizure, severe dehydration or collapse needs acute paediatric pathways immediately — not a completed anticipatory guidance checklist. [21]
High concern for inflicted injury requires simultaneous medical care and child-protection pathways while the child remains safe. Possible lead encephalopathy or cardiovascular compromise from severe anaemia needs same-day escalation. Facial swelling from dental infection needs urgent dental or medical care. Extreme aggression or parental obstruction that blocks examination needs senior support and a safety plan, not abandonment of the child. Rural teams convert clinic concern into capability-matched retrieval when required. Document and hand over acute findings discovered during preventive care. [13] [6] [5]
Management — Definitive & Stepwise
- Agenda-set with caregiver and child; list top concerns first.
- Measure and plot growth; interpret trajectory on WHO standards. [17]
- Run developmental surveillance and autism screening at recommended ages; act on positives. [2] [4]
- Examine, including lift-the-lip oral check. [8]
- Target iron and lead risk assessment — selective testing, not reflexive universal labs without indication. [5] [6]
- Reconcile immunisations against the official jurisdictional schedule; plan catch-up from the handbook, not memory. [1]
- Prioritise anticipatory guidance when time is short: injury hazards matching current motor skills, car seats, water safety, iron-rich diet and bottle weaning, juice limits, sleep routines, media limits, play, and positive discipline without corporal punishment. [12] [9] [5] [11] [10] [14]
- Address food insecurity and social risk with concrete resources and follow-up. [15] [19]
- Close with teach-back, written plan, next visit timing, and a chase plan for every referral. [21]
Strong clinical concern justifies referral even if a family declines a paper screen or a tool is incomplete. [2]
Specific Subtypes & Scenarios
12-month visit. Walking onset or near-walking, bottle use review, diet transition to family foods, first structured autism surveillance intensity rising, fall and choking hazards, immunisation review. [1] [2] [12]
15–18-month visits. Language expectations accelerate; M-CHAT-R/F timing per local schedule; tantrums and limit-setting; car seat transitions; sleep routines. [4] [10] [9]
24-month visit. BMI interpretation begins to matter more; speech intelligibility concerns; autism rescreen where indicated; dental home and fluoride; peer play. [20] [2] [8]
30–36-month visits. Preschool readiness precursors, toilet-training readiness, peer play, vision and hearing pathways as local programmes allow. [1] [3]
Picky eating with normal growth. Reassure on trajectory, protect iron-rich foods, avoid coercive pressure, limit milk crowding. Picky eating with faltering growth. Full intake history, plot carefully, investigate and refer as indicated. [5] [17]
Positive M-CHAT-R/F. Explain that the tool risk-stratifies, not diagnoses; arrange early intervention and developmental evaluation; offer interim communication strategies; safety-net the wait. [4] [18]
Multiple ED injury visits. Review hazards and supervision, but also consider neglect or inflicted injury patterns. [13] [12]
Indigenous toddler with ECC risk. Culturally safe care, early dental home, fluoride counselling, community-controlled service links where available. [16] [8]
Refugee toddler with incomplete records. Professional interpreter, trauma-informed approach, catch-up prevention from official schedules, uncertain-age handling with growth and development context. [22] [1]
Out-of-home care. Assume fragmented records; complete a full package; share plans lawfully with carers and agencies. [19] [13]
Complications & Pitfalls
Reassuring “he’ll talk later” after red-flag language or autism markers without referral. Failing to plot growth or ignoring a falling trajectory while celebrating one normal percentile. Skipping oral exam and fluoride counselling. Ordering universal labs without indication — or missing high-risk iron and lead assessment. Endorsing or minimising corporal punishment. Over-pathologising normal toddler autonomy. Underestimating choking, drowning and fall risks at new motor milestones. Using screens as behavioural management without limits. Missing food insecurity by only asking about calories. Fragmented care after positive screens with no closed-loop referral. [2] [4] [8] [5] [10] [12] [15]
Prognosis & Disposition
Earlier language intervention, dental care, iron repletion when indicated, lead source control and injury prevention change outcomes. Disposition is graded: routine interval follow-up; early primary-care review; allied health referral; developmental clinic; dental urgent care; public health lead pathways; or safeguarding notification with planned medical follow-up. Positive developmental or autism screens should reach early intervention without pure “watchful waiting until preschool.” Telehealth well care converts to in-person examination when measurement, oral exam, vaccines or safeguarding concerns require it. Re-engage families who miss visits with practical outreach. [2] [4] [5] [6] [21]
Special Populations
Former preterm or NICU toddlers. Use corrected age for developmental interpretation until your local standard ends; interpret growth carefully. [2] [17]
Medical complexity and technology dependence. Adapt the preventive agenda; prevent diagnostic overshadowing. [1]
Disability and neurodiversity. Accessible rooms, longer visits, strength-based counselling. [2]
Indigenous children. Oral health, ear health, culturally safe care and community links without lowering clinical standards. [16]
Migrant and refugee families. Interpreters, catch-up prevention, trauma-informed approaches. [22]
Out-of-home care. Consent, records, extra psychosocial surveillance. [19]
Socioeconomic disadvantage and food insecurity. Write plans families can do; link concrete food resources. [15]
Rural-remote families. Hybrid telehealth plus local child-health nurse models; clear retrieval thresholds. [1]
Possible maltreatment or family violence. Parallel medical care and protection pathways. [13]
Evidence, Guidelines & Regional Differences
AAP 2025 periodicity recommendations structure preventive content across toddler ages. [1] Lipkin and colleagues frame developmental surveillance plus screening. [2] Zubler and colleagues supply evidence-informed milestone content. [3] Robins and colleagues validated M-CHAT-R/F with follow-up; Aishworiya and colleagues meta-analyse screening performance. [4] [18] Baker and colleagues guide iron deficiency prevention and diagnosis in 0–3 years. [5] AAP Prevention of Childhood Lead Toxicity emphasises primary prevention and no identified safe blood lead level. [6] Clark and Krol guide primary-care oral health and fluoride. [7] [8] Durbin summarises child passenger safety. [9] Sege and Siegel reject corporal punishment and promote effective discipline. [10] Media and Young Minds guides early screen advice. [11] Gardner frames office-based injury counselling. [12] Christian guides evaluation of suspected physical abuse. [13] Yogman and colleagues elevate play as developmental care. [14] Peltz links food insecurity to health-care use. [15] Holve addresses early childhood caries in Indigenous communities. [16] WHO Child Growth Standards underpin length/height and weight plotting. [17] Dubowitz SEEK models psychosocial risk inquiry. [19] Hampl obesity CPG executive summary supports early BMI attention without transplanting adolescent treatment algorithms wholesale. [20] Burvenich supports structured safety-netting. [21] Boylen supports professional interpreters. [22]
Controversies you should name honestly: universal versus selective iron and lead testing; ideal autism screen ages across jurisdictions; absolute screen-time cut-offs versus family-centred limits; and time pressure versus comprehensive Bright Futures content. State local policy rather than inventing cut-scores. [1] [5] [6] [11]
Use jurisdictional child health books, local child-health nurse frameworks, and the Australian Immunisation Handbook or New Zealand schedule for vaccines. Cultural safety and interpreter access are part of valid supervision. Confirm fluoride varnish programmes and local lead/iron pathways before promising chairside or lab actions. Cross-link ATAGI schedule detail rather than inventing dose intervals. [1] [7] [22]
Healthy Child Programme contacts, health visitor pathways, and NICE autism recognition guidance shape thresholds. Map local community paediatric and speech routes rather than importing US tool ages wholesale. Green Book schedules govern immunisation catch-up. [2]
Bright Futures and AAP periodicity tables drive many clinic checklists; Canadian provincial programmes and the Rourke Baby Record vary. State the local autism tool ages, iron and lead policy rather than inventing universal action levels. CPS statements inform Indigenous oral-health risk in Canada. [1] [6] [16]
Exam Pearls
- Toddler visit equals growth, development, safety and family context — not vaccines alone. [1]
- Plot trajectory on WHO standards; one normal point can still hide a falling curve. [17]
- Surveillance every visit; autism-specific tools risk-stratify in supported age windows. [2] [4]
- A screen is not a diagnosis; a failed screen is not “watch until school.” [4] [18]
- Lift the lip; fluoride toothpaste counselling is core primary care. [7] [8]
- Iron and lead: risk-based prevention and testing; no invented universal numbers. [5] [6]
- Injury priorities match current motor milestones. [12]
- No corporal punishment; teach positive discipline. [10]
- Professional interpreter; never the child. [22]
- Safety-net every referral wait with teach-back. [21]
References
- [1]Committee on Practice and Ambulatory Medicine 2025 Recommendations for Preventive Pediatric Health Care: Policy Statement. Pediatrics, 2025.PMID 39914362
- [2]Lipkin PH Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening. Pediatrics, 2020.PMID 31843861
- [3]Zubler JM Evidence-Informed Milestones for Developmental Surveillance Tools. Pediatrics, 2022.PMID 35132439
- [4]Robins DL Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F). Pediatrics, 2014.PMID 24366990
- [5]Baker RD Diagnosis and prevention of iron deficiency and iron-deficiency anemia in infants and young children (0-3 years of age). Pediatrics, 2010.PMID 20923825
- [6]COUNCIL ON ENVIRONMENTAL HEALTH Prevention of Childhood Lead Toxicity. Pediatrics, 2016.PMID 27325637
- [7]Clark MB Fluoride Use in Caries Prevention in the Primary Care Setting. Pediatrics, 2020.PMID 33257404
- [8]Krol DM Maintaining and Improving the Oral Health of Young Children. Pediatrics, 2023.PMID 36530159
- [9]Durbin DR Child Passenger Safety. Pediatrics, 2018.PMID 30166367
- [10]Sege RD Effective Discipline to Raise Healthy Children. Pediatrics, 2018.PMID 30397164
- [11]COUNCIL ON COMMUNICATIONS AND MEDIA Media and Young Minds. Pediatrics, 2016.PMID 27940793
- [12]Gardner HG Office-based counseling for unintentional injury prevention. Pediatrics, 2007.PMID 17200289
- [13]Christian CW The evaluation of suspected child physical abuse. Pediatrics, 2015.PMID 25917988
- [14]Yogman M The Power of Play: A Pediatric Role in Enhancing Development in Young Children. Pediatrics, 2018.PMID 30126932
- [15]Peltz A Food Insecurity and Health Care Use. Pediatrics, 2019.PMID 31501238
- [16]Holve S Early Childhood Caries in Indigenous Communities. Pediatrics, 2021.PMID 34001640
- [17]WHO Multicentre Growth Reference Study Group WHO Child Growth Standards based on length/height, weight and age. Acta paediatrica (Oslo, Norway : 1992). Supplement, 2006.PMID 16817681
- [18]Aishworiya R Meta-analysis of the Modified Checklist for Autism in Toddlers, Revised/Follow-up for Screening. Pediatrics, 2023.PMID 37203373
- [19]Dubowitz H The safe environment for every kid model: impact on pediatric primary care professionals. Pediatrics, 2011.PMID 21444590
- [20]Hampl SE Executive Summary: Clinical Practice Guideline for the Evaluation and Treatment of Children and Adolescents With Obesity. Pediatrics, 2023.PMID 36622135
- [21]Burvenich R Effectiveness of safety-netting approaches for acutely ill children: a network meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners, 2025.PMID 39117428
- [22]Boylen S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387