Paeds · preventive-and-community-paediatrics
Vaccine contraindications, precautions and adverse events
Also known as Vaccine contraindications · Vaccine precautions · AEFI · Adverse events following immunisation · Vaccine anaphylaxis · False contraindications vaccination
A fellowship approach to paediatric vaccine safety: true contraindications versus precautions and false contraindications; live-vaccine rules in immunocompromise and pregnancy; AEFI recognition including anaphylaxis, intussusception and ITP; bedside screening; resuscitation; reporting; and regional guidance across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A six-week-old arrives with a runny nose and a temperature of 37.8°C. The nurse asks whether to cancel the primary schedule. The fellowship answer is almost always vaccinate if the child is otherwise well, because mild illness is not a true contraindication. Under-vaccination is driven more by missed opportunities than by genuine safety stops. [1] [27]
A contraindication is a condition that markedly increases the risk of a serious adverse reaction. The vaccine should not be given. A precaution is a condition that might increase risk, might impair immune response, or might confuse interpretation of a later illness. You usually defer or seek specialist advice rather than permanently withhold. A false contraindication is a commonly believed barrier that does not justify delay. [1]
An adverse event following immunisation (AEFI) is any untoward medical occurrence after a vaccine. Temporal association is not automatic causation. Passive systems such as VAERS detect signals; they do not, alone, prove product-related harm. [15] [25]
Safe immunisation encounter
Identify and check due vaccines
Confirm identity, age and record — not parental recall alone.
Screen for true stops
Prior anaphylaxis, severe immunocompromise, pregnancy for live vaccines, vaccine-specific rules.
Decide give, defer or withhold
Separate false barriers from precautions and absolute contraindications.
Administer and observe
Correct product, route and site; observe; keep adrenaline available.
Safety-net and document
Expected reactions, when to return, batch/lot, and any AEFI report.
Classification
Start with the child, then place the concern into one of three safety buckets. [1]
True contraindications
These are uncommon and usually antigen-specific. Classic examples include anaphylaxis to a previous dose or a known vaccine component; live vaccines in severe immunocompromise; live vaccines in pregnancy; and encephalopathy within seven days of a pertussis-containing vaccine with no other cause identified. SCID adds absolute avoidance of rotavirus and BCG because vaccine-strain disease can be severe. [1] [3] [23] [24]
Precautions
Moderate or severe acute illness is the everyday precaution. You defer so that a later deterioration is not blamed on the vaccine and so the child is not vaccinated while unstable. Recent antibody-containing blood products are a precaution for many live vaccines because passive antibody can blunt replication and response. Evolving undiagnosed neurologic illness may justify temporary delay of selected antigens while the diagnosis is clarified. [1]
False contraindications
Mild upper respiratory infection, low-grade fever, otitis media, diarrhoea without severe illness, antibiotics, breastfeeding, prematurity managed by chronological age, stable neurologic conditions, family history of seizures, and family history of autism are not reasons to cancel. These false barriers create coverage gaps. [1] [9] [11]
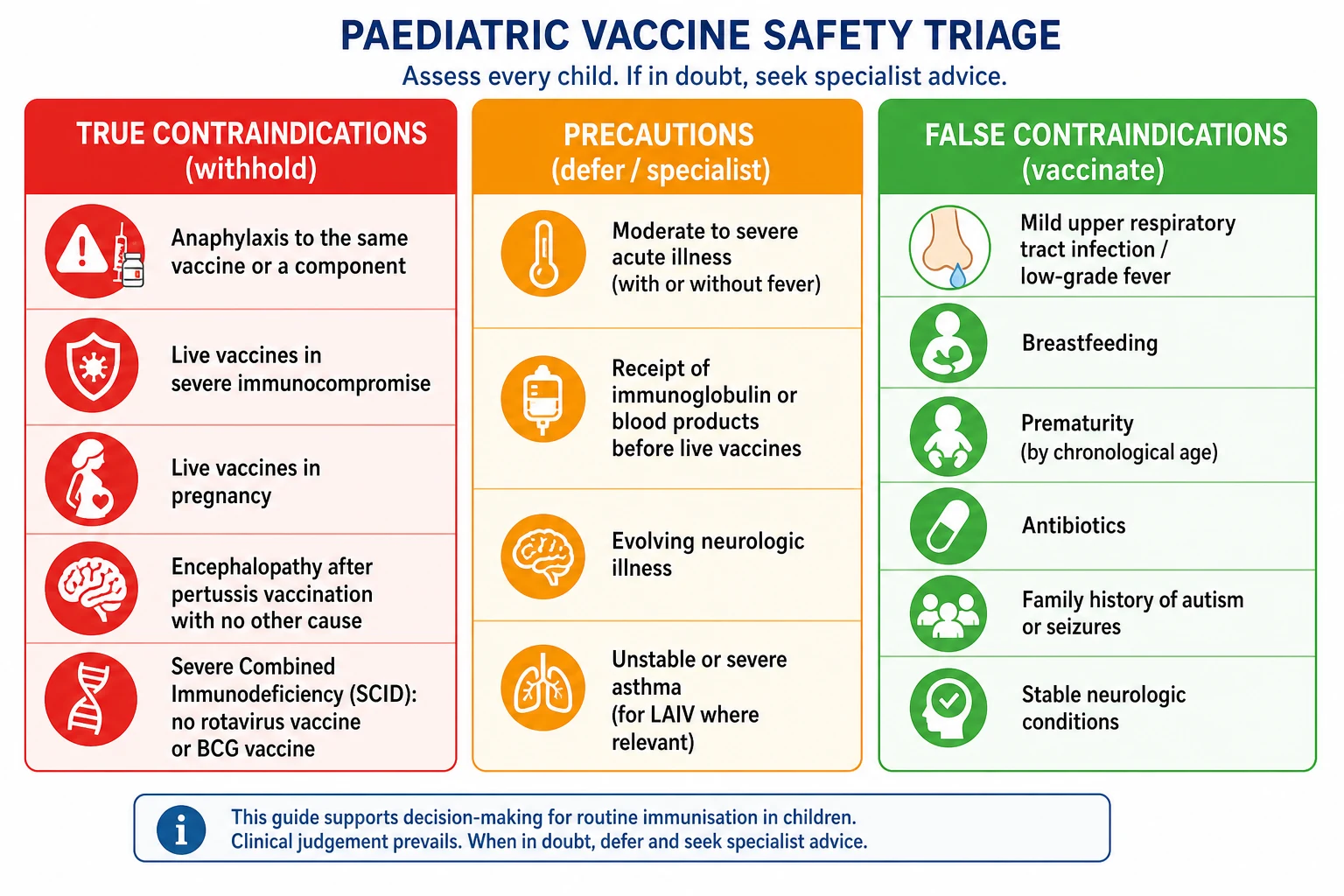
Read the figure like this: if the reason for delay is “a bit snuffly,” you are usually looking at a false contraindication. If the reason is “anaphylaxis to this product last time,” you are looking at a true, antigen-specific stop. [1] [2]
Contraindication
Do not give this vaccine
- Anaphylaxis to same vaccine or component
- Live vaccines in severe immunocompromise
- Live vaccines in pregnancy
- Selected antigen-specific absolute rules
Precaution
Defer or specialist review
- Moderate or severe acute illness
- Recent IG/blood products before live vaccines
- Unstable or evolving conditions needing diagnosis
- Some product-specific temporary concerns
False barrier
Vaccinate today
- Mild URTI or low-grade fever
- Breastfeeding or antibiotics
- Prematurity by chronological age
- Family autism or seizure history
Epidemiology & Risk Factors
True vaccine anaphylaxis is rare. Large surveillance analyses place the risk in a very low range per million doses, which is why observation and adrenaline readiness remain mandatory despite low absolute numbers. [2]
Common local and systemic reactions are frequent and expected. They reflect inflammatory activation, not product failure. Serious rare events that candidates must know by name include intussusception after rotavirus vaccines, ITP after MMR, and febrile seizures after some fever-inducing vaccines. Modern rotavirus products carry a small excess intussusception risk that is far lower than the historical RotaShield experience that led to withdrawal. [4] [5] [6] [7] [8]
Risk concentrates in host and system factors: severe immunodeficiency for live vaccines; programme error for wrong route or contaminated multi-dose vials; incomplete screening; and clinics without observation capacity. Social disadvantage increases both disease risk and the chance that a mild illness becomes an indefinite deferral. [3] [15] [21]
Pathophysiology
Vaccine safety decisions rest on mechanism, not slogans. [16]
Live attenuated vaccines replicate enough to train immunity. In a child with severe T-cell failure, replication can become progressive infection. That is why BCG and rotavirus are catastrophic in undiagnosed SCID, and why live vaccines are restricted after intensive chemotherapy, early post-HSCT and many transplant states. [3] [20] [23] [24]
IgE-mediated allergy to a vaccine component can trigger mast-cell degranulation and anaphylaxis. The clinical lesson is antigen- and component-specific avoidance after proven anaphylaxis, not a lifelong ban on every immunisation. [2] [1]
Expected reactogenicity is non-IgE inflammation: sore arm, fever, irritability. Aluminium-adjuvanted products often cause local symptoms. These are unpleasant, usually self-limited, and not contraindications to future doses. [16] [1]
Passive antibody interference explains why recent immunoglobulin or selected blood products can reduce live-vaccine take. The interval is a timing precaution, not proof of permanent intolerance. [1]
Non-immune events matter in exams. Vasovagal syncope after injection, especially in adolescents, is anxiety-related physiology. It needs positioning and injury prevention, not an anaphylaxis label that wrongly contraindicates future care. [1] [2]
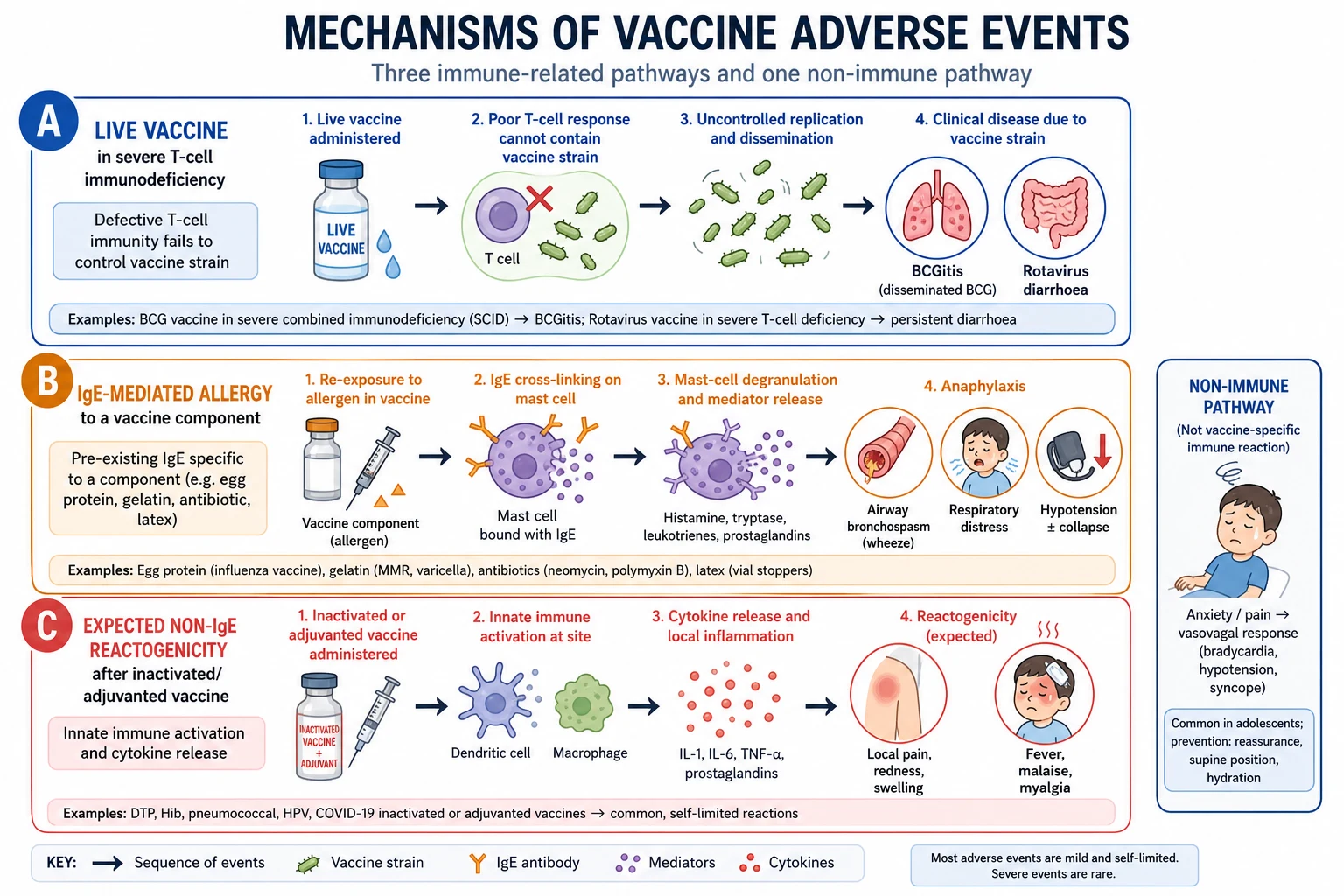
Read the figure like this: when a parent says “the last vaccine made them sick,” ask which pathway you are in before you cancel the next visit. [1]
Clinical Presentation
Anaphylaxis usually declares within minutes of injection: airway compromise, bronchospasm, hypotension or collapse, with or without urticaria and angioedema. Skin findings alone without systemic features are not anaphylaxis. [2]
Common reactions include injection-site pain, redness, swelling, fever and irritability. They cluster in the first one to two days for many inactivated products and around one to two weeks for some live vaccines such as MMR. [1] [10]
ITP after MMR presents with bruising or petechiae in the weeks after vaccination. It is rare and usually self-limited, and wild measles carries a higher ITP risk than vaccine. [4] [5]
Intussusception after rotavirus presents with intermittent severe abdominal pain, vomiting, pallor or bloody stool, classically in a short window after early doses. Treat the surgical emergency first; causality discussion comes later. [6] [7]
BCG complications range from local abscess or ipsilateral lymphadenitis to rare disseminated disease in immunodeficiency. [23] [32]
Adolescent syncope presents with prodrome, brief loss of consciousness, and rapid recovery without airway swelling or wheeze. Prevent falls; do not convert the event into a universal vaccine ban. [1]
Differential Diagnosis
| Finding after vaccination | Prefer | Discriminators | Action |
|---|---|---|---|
| Collapse with rash, wheeze, hypotension | Anaphylaxis | Onset minutes; multi-system | IM adrenaline immediately |
| Collapse with pallor, bradycardia, rapid recovery | Vasovagal | No airway/breathing threat | Lie flat, observe, injury prevention |
| Fever day 1 after DTaP-containing shot | Reactogenicity | Well between spikes | Supportive care; continue schedule |
| Petechiae 1–6 weeks after MMR | ITP vs other cause | Platelet count; smear | Haematology pathway; antigen-specific plan |
| Bilious vomiting and bloody stool post-rotavirus | Intussusception | Age and timing window | Emergency imaging/surgery pathway |
| “Allergy because sibling has autism” | False barrier | No causal MMR–autism link | Vaccinate and counsel with evidence |
Separate coincidental illness from vaccine reaction by baseline incidence and biologic plausibility. A first afebrile seizure days after a visit may be unrelated. A multi-system allergic reaction within minutes is not coincidence. [15] [1]
Clinical & Bedside Assessment
Ask the same safety screen every time. [1]
- Is the child well enough today? Mild symptoms usually allow vaccination; moderate or severe illness is a precaution.
- Any anaphylaxis to a previous dose or component? Name the product if known.
- Any severe immunocompromise, transplant, chemotherapy or high-dose steroids? Live-vaccine gate.
- Any pregnancy or chance of pregnancy before live vaccines?
- Any recent immunoglobulin or blood product before live vaccines?
- Any prior serious AEFI, and what exactly happened?
- Household contacts who are severely immunocompromised? Still vaccinate the well child with most live vaccines; avoid transmitting OPV where that product is used. [1] [3]
Examination is brief: does the child look systemically unwell, and is the planned injection site free of active infection? There is no role for routine bloods before standard vaccines in a well child. [1]
Investigations
Most children need no laboratory testing before routine vaccination. [1]
Investigate when the result changes the live-vaccine decision or the AEFI plan: [1] [3]
- Clinical immunodeficiency concern, HIV staging, or transplant timeline before live vaccines. [3] [20] [21]
- Pregnancy testing when a live vaccine is planned and pregnancy is possible. [1]
- After suspected anaphylaxis: acute management first; later allergy referral and selected tryptase timing as directed by local allergy pathways. [2]
- Suspected intussusception: ultrasound or surgical pathway, not delayed by AEFI paperwork. [6]
- Suspected ITP: full blood count and smear, with haematology input. [4]
AEFI investigation is also an investigation: lot number, timing, concurrent illness, cold-chain status, route and site, and whether other recipients of the same session are affected. Clusters raise programme-error concern. [15]
Management — Resuscitation
Vaccine anaphylaxis is rare and time-critical. [2]
- Recognise multi-system allergic features.
- Call for help and stop further vaccine exposure.
- Give IM adrenaline into the anterolateral thigh without delay. Age-banded IM adrenaline dosing is the standard emergency approach in paediatric anaphylaxis algorithms used in immunisation settings; antihistamines and steroids are adjuncts only. [2] [1]
- Airway and oxygen, then IV access and crystalloid if hypotensive.
- Repeat adrenaline at short intervals if there is no response, while preparing escalation.
- Observe and admit as clinically indicated after treated anaphylaxis; biphasic reactions can occur.
- Document and report the AEFI and record a permanent contraindication to the culprit vaccine or component. [2] [15]
For syncope without anaphylaxis, lie the patient flat, protect the head, and observe until fully recovered. For suspected intussusception, resuscitate fluid and pain needs and transfer for definitive care. [1] [6]
Management — Definitive & Stepwise
This is the constructive algorithm examiners want. [1]
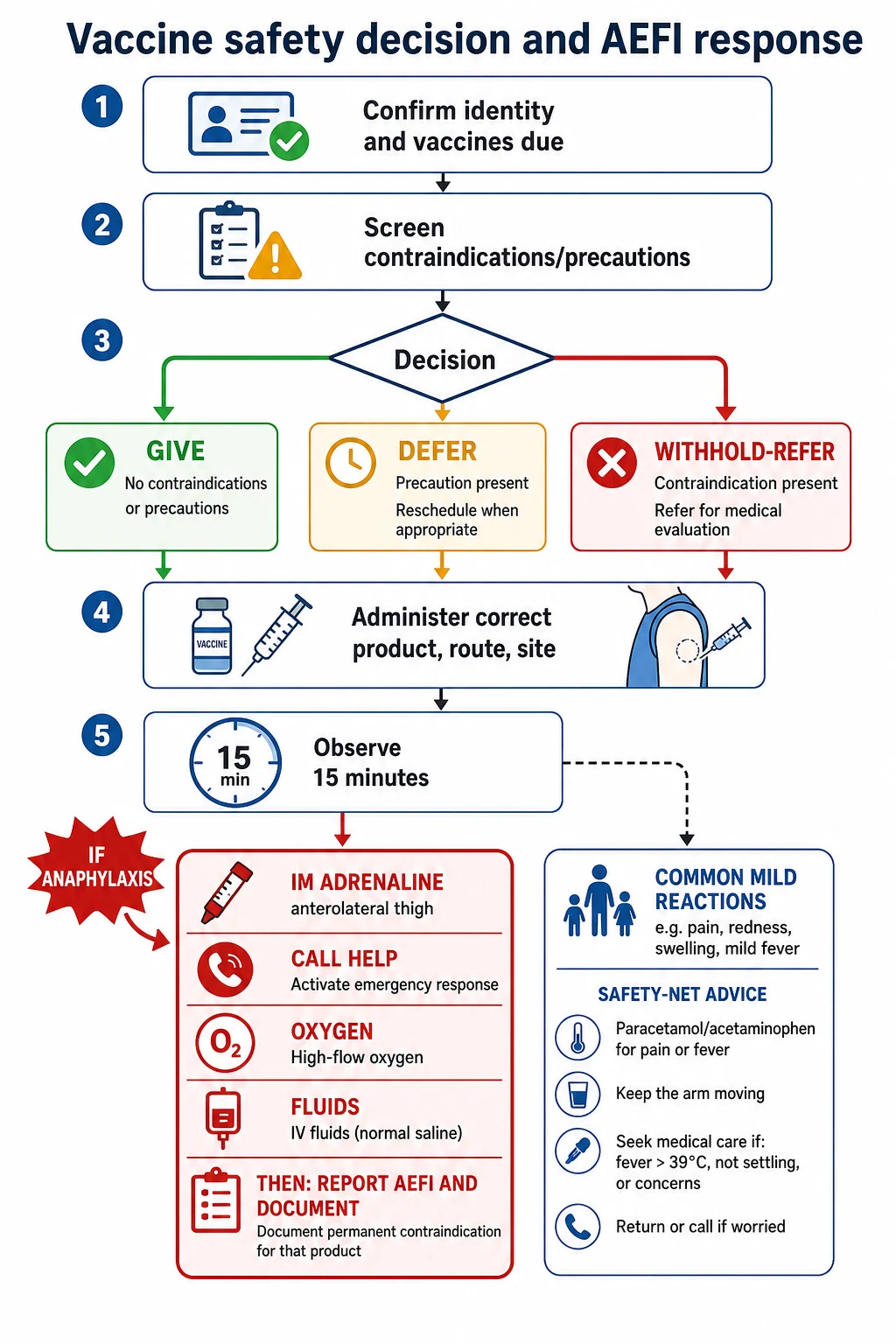
Step 1 — Confirm identity, record and products due
Do not rely on memory alone. Wrong patient and wrong product are programme errors, not immunology. [1] [27]
Step 2 — Apply the three-bucket screen
Give, defer, or withhold. Most children are in the give pathway. [1]
Step 3 — Special live-vaccine rules
Severe immunodeficiency, early post-HSCT, many transplant contexts, high-dose systemic steroids for two weeks or more, and pregnancy block live vaccines until criteria for safety return or specialist clearance is obtained. Inactivated vaccines are usually continued, though response may be blunted. [3] [20] [21] [22]
Step 4 — Administer correctly and observe
Correct route and site. Observe for at least 15 minutes in standard practice; extend observation when risk is higher. Keep an anaphylaxis kit immediately available. [1] [2]
Step 5 — Counsel expected reactions
Tell families what is common, what is urgent, and how to use antipyretic care if fever develops. Do not create fear that every fever is anaphylaxis. [1]
Step 6 — Manage AEFI and re-entry to the schedule
After a true anaphylaxis, that product is contraindicated. Plan alternatives with allergy and immunisation specialists. After a temporary precaution, rebook promptly. After ITP or intussusception, make an antigen-specific plan with the relevant specialty rather than abandoning all future protection. [2] [4] [6]
Step 7 — Report and close the loop
Serious AEFIs need national reporting pathways and clear chart flagging so the next clinician does not repeat the exposure. [15]
Specific Subtypes & Scenarios
Prior anaphylaxis to hexavalent or another combination product. Treat the emergency, report, and avoid the culprit components. Future protection may use alternative products under specialist advice rather than “no vaccines ever.” [2] [1]
SCID or suspected severe IEI. No rotavirus. No BCG. Escalate immunology urgently. Household contacts still need protection with non-transmissible schedules where possible. [3] [23] [24]
Oncology and HSCT. Follow transplant or ECIL-style frameworks: non-live vaccines according to timing, live vaccines only after defined immune reconstitution and specialist clearance. [20] [21]
Solid-organ transplant. Live vaccines are generally avoided post-transplant; selected pre-transplant opportunities matter. [22]
High-dose steroids. Temporary live-vaccine deferral after clinically important systemic steroid courses is standard teaching; inactivated vaccines may proceed if the child is otherwise suitable. Confirm local handbook thresholds. [1] [3]
Egg allergy. Modern evidence supports influenza vaccination for most egg-allergic children in appropriate settings; MMR is not contraindicated by egg allergy. Specialist pathways remain for severe prior reactions according to local allergy guidance. [17] [18] [19]
Rotavirus timing. Respect upper age limits for first and final doses because intussusception risk–benefit worsens with late starts. Counsel the small excess risk and the large benefit against severe gastroenteritis. [6] [7] [8]
MMR and ITP. Rare post-vaccine ITP is usually self-limited. Further MMR doses need individualised assessment; wild measles is more dangerous than vaccine ITP risk. [4] [5] [10]
Pregnancy. Live vaccines are contraindicated. Inactivated influenza and pregnancy Tdap strategies protect mother and infant; product timing is regional. Inadvertent live-vaccine exposure is not an automatic indication for termination — specialist counselling is required. [1] [31]
Adolescent injectables. Prevent syncope-related injury with seated or lying administration and post-vaccine observation. [1]
Complications & Pitfalls
- Deferring for mild illness and never rebooking. [1]
- Treating autism family history as a contraindication despite robust contrary evidence. [9] [10] [11]
- Labelling vasovagal syncope as anaphylaxis and blocking future care. [2]
- Giving live vaccines in unrecognised SCID. [23] [24]
- Omitting observation time or adrenaline readiness. [2]
- Using passive AEFI reports as proof of causation in exams. [15]
- Restarting whole schedules after one antigen-specific event. [1]
- Ignoring household protection for immunocompromised siblings. [3]
- Missing programme-error clusters. [15]
- Confusing hesitancy with a medical contraindication. [26]
Prognosis & Disposition
Most children leave the same day after brief observation with expected minor symptoms only. Common reactions resolve with supportive care. [1]
After treated anaphylaxis, disposition is observation or admission according to severity and local anaphylaxis pathways, plus allergy follow-up and chart flagging of the permanent product contraindication. [2]
After temporary precautions, the prognosis for completing the schedule is excellent if rebooking is active. After rare serious AEFIs, prognosis depends on the event — for example self-limited ITP versus surgical intussusception — and on whether alternative protection is arranged. [4] [6]
Safety-net every visit: when to return for breathing difficulty, persistent lethargy, unresponsiveness, persistent vomiting, bloody stool, or widespread rash with systemic features. [1] [2]
Special Populations
Preterm infants. Vaccinate by chronological age with full doses when stable enough; prematurity itself is not a contraindication. [1]
Immunodeficiency and transplant. Live-vaccine restriction is the dominant safety theme; inactivated vaccines remain important, sometimes with altered timing or reduced response. [3] [20] [21] [22]
Asplenia and complement deficiency. These children need more protection against encapsulated bacteria, not fewer vaccines. Safety screening still applies, but asplenia is not a routine contraindication to indicated products. [29] [1]
Migrant, refugee and foster care. Incomplete records and prior “reaction” stories need careful history. Do not convert uncertain history into permanent under-immunisation. [1] [27]
Disability and neurodiversity. Adapt communication and observation environment. Do not invent medical contraindications from behavioural distress alone. [1]
Rural and remote. Cold chain, adrenaline, observation space and transfer plans are part of safety, not optional extras. [1]
Evidence, Guidelines & Regional Differences
Evidence spine for exams: [1] [2]
- ACIP general immunisation recommendations — contraindications, precautions and false contraindications. [1]
- Anaphylaxis risk after vaccination from large surveillance. [2]
- Live-vaccine guidance in immunodeficiency and transplant frameworks. [3] [20] [21]
- Rotavirus efficacy/safety and intussusception policy history. [6] [7] [8]
- MMR safety regarding autism and ITP. [4] [5] [9] [10]
- Interpretation limits of passive AEFI systems. [15] [25]
- Egg-allergy influenza vaccine safety literature. [17] [18]
ATAGI and the Australian Immunisation Handbook operationalise contraindications, precautions and AEFI reporting for Australian practice. New Zealand uses Medsafe/Immunisation Handbook aligned guidance. Principles match international general recommendations even when product names and reporting portals differ. Use the current national handbook for product-level detail rather than memorising every brand footnote. [1]
The Green Book is the operational source for contraindications, live-vaccine rules and AEFI processes, with Yellow Card reporting. MRCPCH expects the same three-bucket logic and strong rejection of false contraindications. [1] [15]
ACIP general best-practice guidance and the childhood schedule footnotes drive US practice; VAERS and VSD inform safety surveillance. Canadian guidance is closely aligned on true versus false contraindications, with provincial programme details. [1] [27] [15] [25]
Controversies to handle cleanly: egg-allergy clinic setting requirements have liberalised with evidence; COVID-era AE surveillance taught signal detection methods but should not be carelessly generalised to every routine infant antigen; and “too many vaccines overwhelm the immune system” has no mechanistic or epidemiologic support comparable to proven disease prevention. [17] [25] [16] [10]
Exam Pearls
- Say contraindication / precaution / false contraindication before you say “delay.” [1]
- True stops are rare; missed opportunities are common. [1]
- Live vaccines: severe immunocompromise and pregnancy are classic absolute contexts. [3] [1]
- Anaphylaxis → IM adrenaline first; then report and antigen-specific planning. [2]
- Mild illness, antibiotics, breastfeeding, prematurity by chronological age, family autism history → vaccinate. [1] [9]
- SCID → no rotavirus, no BCG. [3] [24]
- Passive AEFI systems find signals; they do not alone prove causation. [15]
- Rotavirus: protect early; respect age windows because intussusception risk–benefit changes later. [6] [7]
- ITP after MMR is rare; wild measles is worse. [4] [5]
- Hesitancy is a communication problem, not a medical contraindication. [26]
References
- [1]Kroger AT General recommendations on immunization: recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm Rep, 2006.PMID 17136024
- [2]McNeil MM Risk of anaphylaxis after vaccination in children and adults. J Allergy Clin Immunol, 2016.PMID 26452420
- [3]Medical Advisory Committee of the Immune Deficiency Foundation Recommendations for live viral and bacterial vaccines in immunodeficient patients and their close contacts. J Allergy Clin Immunol, 2014.PMID 24582311
- [4]France EK Risk of immune thrombocytopenic purpura after measles-mumps-rubella immunization in children. Pediatrics, 2008.PMID 18310189
- [5]Miller E Idiopathic thrombocytopenic purpura and MMR vaccine. Arch Dis Child, 2001.PMID 11207170
- [6]Haber P Postlicensure monitoring of intussusception after RotaTeq vaccination in the United States, February 1, 2006, to September 25, 2007. Pediatrics, 2008.PMID 18519491
- [7]Murphy TV The first rotavirus vaccine and intussusception: epidemiological studies and policy decisions. J Infect Dis, 2003.PMID 12696011
- [8]Vesikari T Safety and efficacy of a pentavalent human-bovine (WC3) reassortant rotavirus vaccine. N Engl J Med, 2006.PMID 16394299
- [9]Hviid A Measles, Mumps, Rubella Vaccination and Autism: A Nationwide Cohort Study. Ann Intern Med, 2019.PMID 30831578
- [10]Di Pietrantonj C Vaccines for measles, mumps, rubella, and varicella in children. Cochrane Database Syst Rev, 2021.PMID 34806766
- [11]Gerber JS Vaccines and autism: a tale of shifting hypotheses. Clin Infect Dis, 2009.PMID 19128068
- [12]Madsen KM A population-based study of measles, mumps, and rubella vaccination and autism. N Engl J Med, 2002.PMID 12421889
- [13]Taylor B Autism and measles, mumps, and rubella vaccine: no epidemiological evidence for a causal association. Lancet, 1999.PMID 10376617
- [14]Smeeth L MMR vaccination and pervasive developmental disorders: a case-control study. Lancet, 2004.PMID 15364187
- [15]Varricchio F Understanding vaccine safety information from the Vaccine Adverse Event Reporting System. Pediatr Infect Dis J, 2004.PMID 15071280
- [16]Pulendran B Immunological mechanisms of vaccination. Nat Immunol, 2011.PMID 21739679
- [17]Greenhawt MJ Establishing the safety of influenza vaccine in egg-allergic individuals. Pediatr Ann, 2013.PMID 23805959
- [18]Howe LE Safe administration of seasonal influenza vaccine to children with egg allergy of all severities. Ann Allergy Asthma Immunol, 2011.PMID 21530882
- [19]Greenhawt M Physician compliance with updated practice parameters for influenza vaccination in individuals with egg allergies. J Allergy Clin Immunol Pract, 2013.PMID 24565707
- [20]Cordonnier C Vaccination of haemopoietic stem cell transplant recipients: guidelines of the 2017 European Conference on Infections in Leukaemia (ECIL 7). Lancet Infect Dis, 2019.PMID 30744963
- [21]Pinto MV Immunisation of the immunocompromised child. J Infect, 2016.PMID 27233121
- [22]Hartley C Live-Attenuated Vaccines in Pediatric Solid Organ Transplant. Vaccines (Basel), 2024.PMID 38675758
- [23]Laberko A BCG Infection in Patients With Inborn Errors of Immunity Receiving the Russian BCG Strain. J Allergy Clin Immunol Pract, 2022.PMID 35470098
- [24]Pariyaprasert W Successful treatment of disseminated BCG infection in a SCID patient with granulocyte colony stimulating factor. Asian Pac J Allergy Immunol, 2008.PMID 18595532
- [25]Klein NP Surveillance for Adverse Events After COVID-19 mRNA Vaccination. JAMA, 2021.PMID 34477808
- [26]Lafnitzegger A Vaccine Hesitancy in Pediatrics. Adv Pediatr, 2022.PMID 35985708
- [27]Wodi AP Advisory Committee on Immunization Practices Recommended Immunization Schedule for Children and Adolescents Aged 18 Years or Younger - United States, 2024. MMWR Morb Mortal Wkly Rep, 2024.PMID 38206855
- [28]Schillie S Prevention of Hepatitis B Virus Infection in the United States: Recommendations of the Advisory Committee on Immunization Practices. MMWR Recomm Rep, 2018.PMID 29939980
- [29]Mbaeyi SA Meningococcal Vaccination: Recommendations of the Advisory Committee on Immunization Practices, United States, 2020. MMWR Recomm Rep, 2020.PMID 33417592
- [30]Meites E Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep, 2019.PMID 31415491
- [31]Broder KR Preventing tetanus, diphtheria, and pertussis among adolescents: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccines. MMWR Recomm Rep, 2006.PMID 16557217
- [32]Colditz GA Efficacy of BCG vaccine in the prevention of tuberculosis. Meta-analysis of the published literature. JAMA, 1994.PMID 8309034
- [33]Huh WK Final efficacy, immunogenicity, and safety analyses of a nine-valent human papillomavirus vaccine in women aged 16-26 years: a randomised, double-blind trial. Lancet, 2017.PMID 28886907