Paeds · preventive-and-community-paediatrics
Vaccine hesitancy and risk communication
Also known as Vaccine hesitant parents · Immunisation refusal counselling · Vaccine risk communication · Parental vaccine concerns · Vaccine confidence
Fellowship approach to vaccine hesitancy as a continuum, SAGE confidence–complacency–convenience assessment, evidence-based clinic communication, motivational interviewing, ethical response to delay and refusal, documentation and regional programme context.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
You are in a six-week check. The baby is well. The parent says, "We are not anti-vaccine — we just want to wait a bit." That sentence is the clinical problem this page is built for. It is not a debate club. It is a preventive consultation with a child who still needs protection, a family who still needs a relationship with you, and a schedule that still has a clock.[1]
Vaccine hesitancy is delay in acceptance or refusal of vaccines despite availability of vaccination services. The SAGE Working Group definition matters because it separates attitude from access. A family who cannot get an appointment is not the same clinical problem as a family who can but will not.[1][3]
Think of hesitancy as a continuum, not a binary. At one end sit confident acceptors. In the middle sit parents with specific questions, selective delays, or requests to "spread out" antigens. At the far end sit firm refusals. People move along that line after a fever, a news story, a trusted relative, or a good conversation with you.[1][2]
Risk communication here has four practical aims:[5]
- Help the caregiver see disease risk and vaccine risk in proportion.
- Support an informed decision without bullying.
- Preserve trust so the child can return.
- Where clinically appropriate, improve on-time uptake.[5][6]
Full antigen schedules, catch-up tables, and true contraindications live on sibling pages. This leaf owns the conversation, assessment of determinants, and ethical plan.[1]
Classification
Use a map that an examiner can follow in thirty seconds.[1]
Continuum of acceptance
| Position | What you hear | What it is not |
|---|---|---|
| Full acceptance | "We are up to date — what is next?" | Not immunity from future questions |
| Questioning | "Is aluminium safe?" | Not automatic refusal |
| Delay | "Can we leave MMR until after birthday parties?" | Not a medical contraindication |
| Selective | "Everything except MMR" | Not the same as total refusal |
| Refusal | "We will not vaccinate" | Still needs documentation and a door left open |
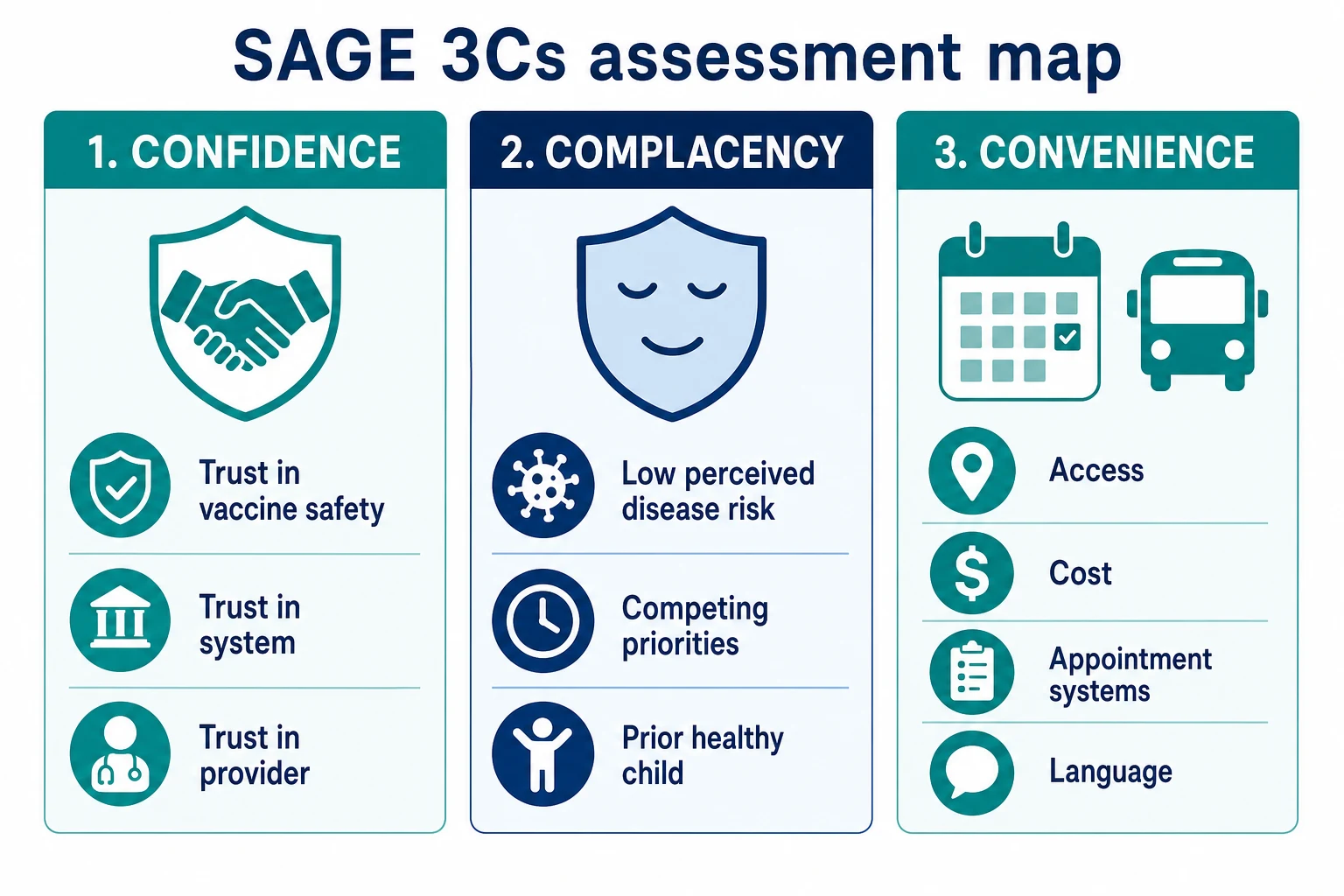
SAGE 3Cs — confidence, complacency, convenience
The SAGE determinants model organises why people hesitate:[1]
- Confidence — trust in vaccine safety and effectiveness, in the system that delivers it, and in the clinician who recommends it.
- Complacency — low perceived need because disease feels rare, the child looks well, or other life pressures win.
- Convenience — access, cost, appointment design, language, and how easy the service is to use. [1]
If you only treat confidence myths, you will miss the family who never returns because clinic is only open when the parent works. If you only fix access, you will miss the parent terrified by an online story.[2][3]
Conversation classification
Separate legitimate medical deferral (true contraindication or precaution) from hesitancy-driven delay. Also separate research tools such as the Parent Attitudes about Childhood Vaccines (PACV) survey from bedside law. PACV can identify hesitant parents in research and quality work; it is not a mandatory score you must quote in every clinic note.[12][4]
Epidemiology & Risk Factors
Hesitancy is global and local at once. Coverage can look high at national level while pockets of under-immunisation support measles or pertussis outbreaks. Systematic reviews show that determinants cluster around trust, social norms, prior experiences, and service design — not a single "type" of parent.[2][3]
Caregiver factors that raise concern for delay include prior adverse-event narratives, dense vaccine-critical social networks, and previous negative healthcare experiences. System factors that look like hesitancy include rural distance, inflexible appointments, cost, and missing immunisation register data after migration.[2][10]
Provider factors matter more than many registrars expect. Clinicians often overestimate how many parents are deeply opposed and may soften or skip a clear recommendation. Healy and colleagues showed parent–provider perception gaps around concern intensity — do not assume the room is hostile before you open your mouth.[14]
Adolescent programmes (especially HPV) add peer influence, school-based delivery, and parent–teen disagreement. Outbreak periods change risk perception quickly: families who felt complacent last month may now want same-day catch-up — use that window without shaming past delay.[2]
Pathophysiology
This is not cellular pathophysiology. It is the mechanism of a decision under uncertainty.[1]
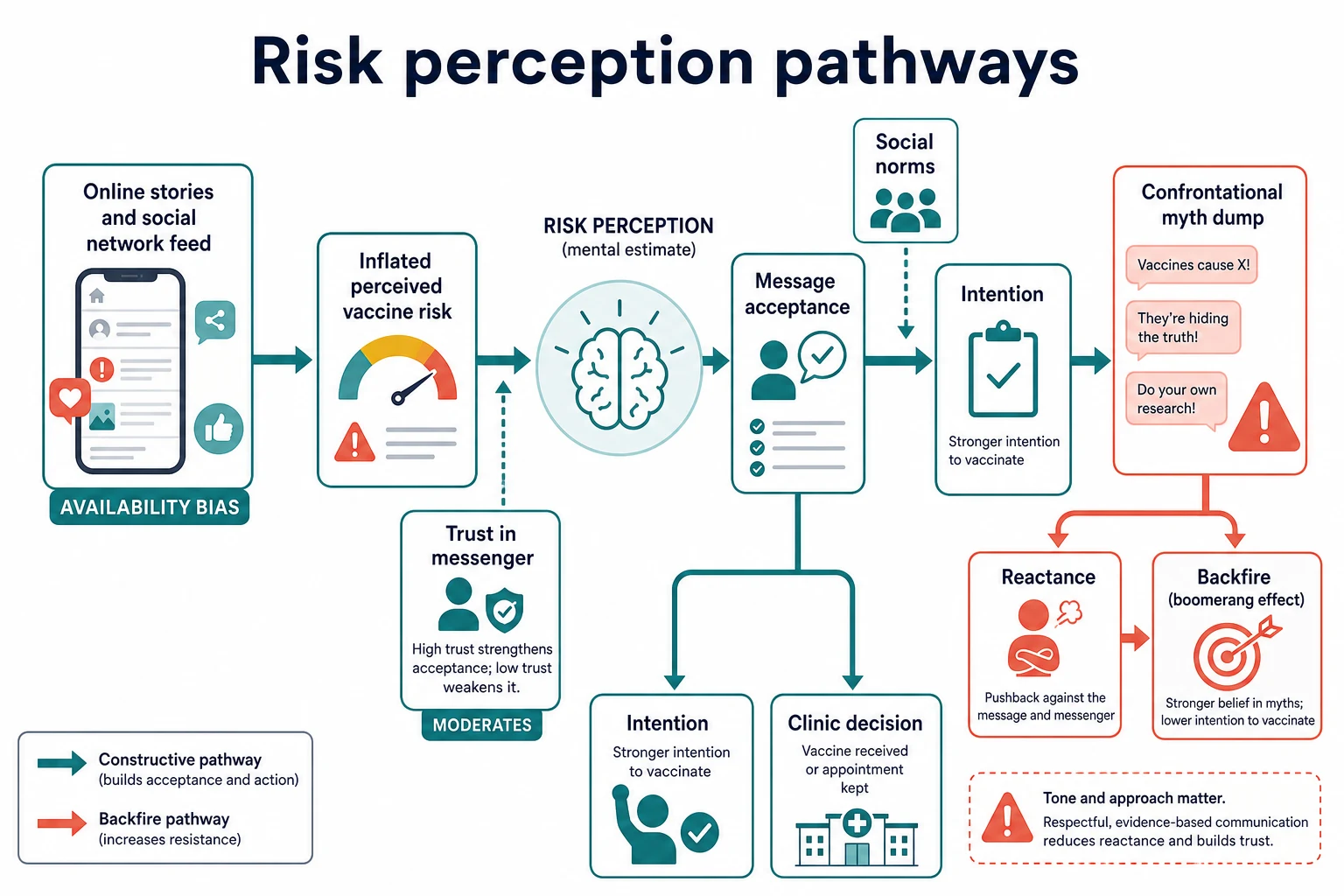
Parents do not hold a spreadsheet of absolute risks in their head. They hold stories. Dramatic online accounts make rare harms feel common — availability bias. Vaccine-critical websites can shift risk perception even in experimental settings.[10]
Trust in the messenger filters the message. The same fact from a trusted paediatrician lands differently from the same fact on a stranger's feed. Social norms ("what people like us do") pull intention toward or away from vaccination. Omission bias makes some caregivers feel safer "doing nothing" than "doing something" that might be blamed later, even when disease risk is higher.[11][5]
Confrontational myth-busting can trigger reactance — a push-back against being controlled. Nyhan and colleagues found that some message strategies intended to reduce misperceptions did not increase intent and could backfire in subgroups. That does not mean facts are useless. It means order and tone matter: elicit, empathise, then give a short accurate fact, then offer a next step.[9]
Provider behaviour is part of the mechanism. Communication style during the visit associates with acceptance and visit experience; discussion format over time relates to immunisation status trajectories.[7][8]
Clinical Presentation
Listen for the theme, not only the label "hesitant".[1]
Common themes:[1]
- Safety and "too many too soon"
- Autism or neurodevelopmental myths
- Ingredients (aluminium, preservatives)
- Preference for "natural" immunity
- Religious or philosophical frames
- Request to space antigens
- Fear after a previous fever, seizure narrative, or media scare
- Adolescent HPV concerns (sexuality stigma, safety, "not needed yet") [1]
Soft hesitancy often sounds cooperative: questions, one delayed antigen, "we are researching". Firm refusal is clearer and still deserves calm process. Some caregivers say yes in the room and then cancel; some say no and later accept after an outbreak or a second talk.[3][14]
Watch for mislabelled access: "We keep missing the nurse clinic" is logistics until proven otherwise. Watch for true medical stories: prior anaphylaxis to a vaccine component is not a communication puzzle first — it is a contraindication and specialist pathway problem (see the contraindications leaf).[5]
Nonverbal cues matter. A parent who avoids eye contact after you say "MMR today" may need space to name a specific fear. An adolescent who stares at the floor while a parent dominates may need a private minute.[5]
Differential Diagnosis
Work the differential the way you would for fever — list what else this could be.[1]
| Competing explanation | Clues | First move |
|---|---|---|
| True contraindication/precaution | Documented anaphylaxis, specific condition | Follow medical algorithm, not persuasion |
| Incomplete or foreign records | Migration, multiple clinics | Check immunisation register, reconstruct history |
| Access barriers | Transport, work, cost, language | Remove barriers, book assisted appointment |
| Informed short delay pending specialist advice | Clear end date, specialist letter | Time-bound plan |
| Hesitancy continuum | Available services, expressed concern/delay/refusal | Communication algorithm |
| Safeguarding concern in extreme contexts | Pattern of medical neglect with high disease risk | Senior/public health/safeguarding pathways per local policy |
Do not call every incomplete schedule "anti-vax". Do not call every worried question "refusal". Precision keeps you ethical and keeps the exam answer sharp.[1][13]
Clinical & Bedside Assessment
Prepare before you speak
Check the register and the record. Know which antigens are due. Know outbreak context. Know language needs. If the visit is already running late, protect a clear recommendation rather than a rushed argument.[5]
Open with a clear recommendation
A presumptive style ("Today we will give the scheduled vaccines") is associated with higher acceptance than a heavily participatory "What do you want to do about vaccines?" opening in observational work — but respect and partnership still matter. Soften without abandoning the recommendation: "These vaccines are due today and I recommend them. What questions do you have?"[7][8][18]
Elicit the specific concern
Ask: "What worries you most?" Then stop talking. Name the concern back. Parents often hold one dominant fear; answering a different fear wastes trust.[5][15]
Assess the 3Cs in plain language
- Confidence: "What have you heard that makes this feel unsafe?"
- Complacency: "What do you know about the diseases these vaccines prevent?"
- Convenience: "What would make it hard to come back if we book another day?" [1]
Include the child or young person
For adolescents, invite their questions. Clarify consent rules for your jurisdiction without turning the visit into a legal seminar. Private time can surface different concerns from the parent narrative.[1]
Synthesise
End the assessment with a one-line problem representation: age, schedule gap, main concern theme, 3C emphasis, relationship risk.[1]
[14]Investigations
Most hesitancy visits need no laboratory test.[1]
Investigate records first: national/regional immunisation registers, previous clinic letters, handheld books. Serology for "immunity checks" can delay protection and is not a routine substitute for a recommended schedule — use only when a verified indication exists (for example selected post-exposure or special-risk pathways).[1]
PACV and related instruments belong mainly to research, audit, and programme evaluation. Do not invent a bedside cut-off as if it were a PEWS score.[12][4]
Refer to immunology or specialist immunisation clinics when the story suggests true adverse event following immunisation work-up rather than pure communication. That pathway is medical, not rhetorical.[5]
Management — Resuscitation
The emergency here is rarely anaphylaxis in the counselling chair. The emergency is a collapsing conversation or an unprotected high-risk child in an outbreak.[1]
Immediate priorities:[1]
- Keep the child safe in the room — no raised voices that frighten the child.
- De-escalate hostility: lower your volume, acknowledge emotion, pause persuasion.
- If the infant is unprotected in a measles outbreak, prioritise same-day public-health-aligned protection opportunities and clear disease safety-netting even while trust work continues.
- Call a senior early if the family threatens to leave care, if safeguarding thresholds may be met, or if you are out of your depth ethically.
- Never fabricate certainty ("vaccines never cause harm") to win the minute — that destroys long-term trust when a fever happens later.[13][6]
Management — Definitive & Stepwise
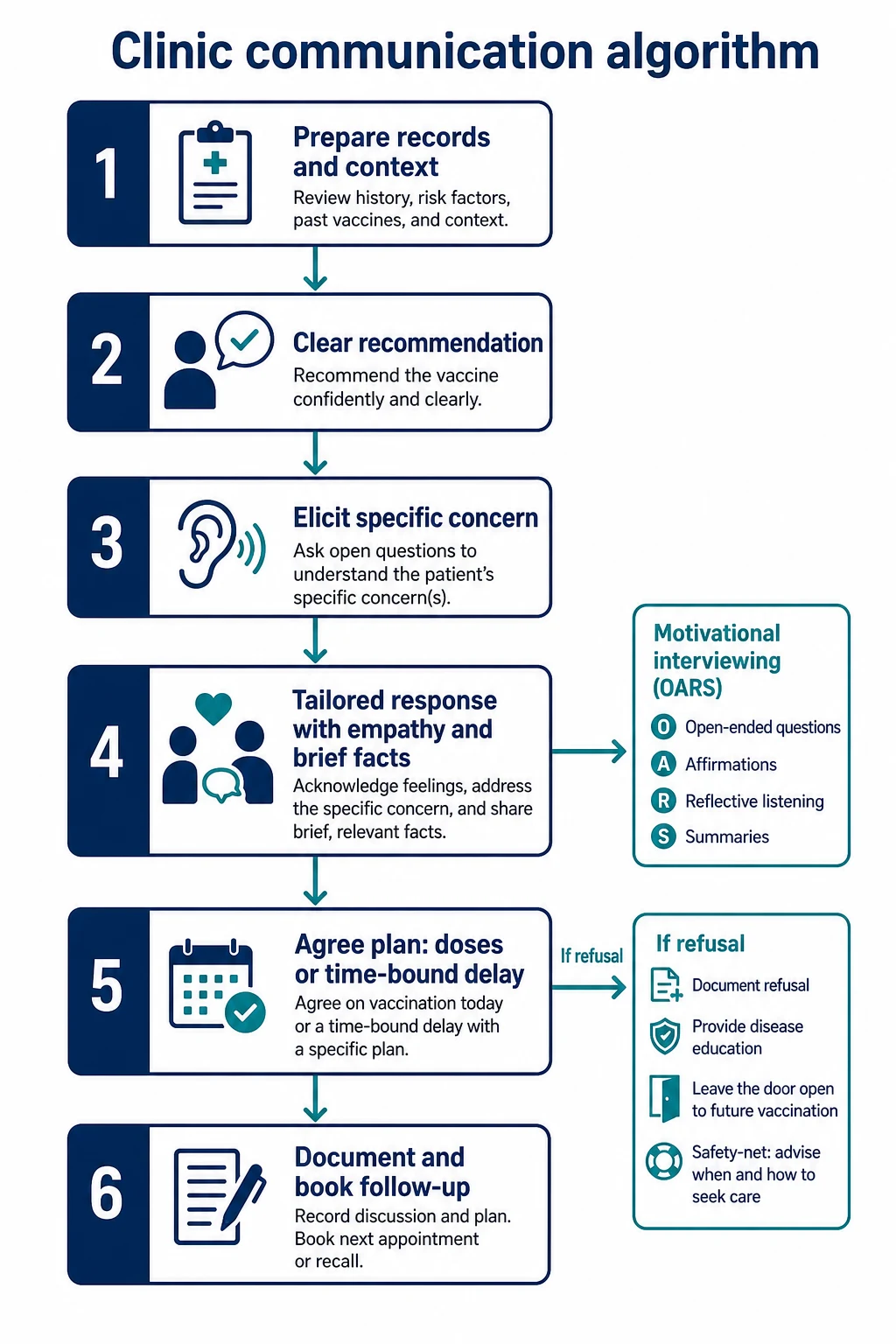
Use a repeatable algorithm.[1]
Step 1 — Prepare
Records, due antigens, language, cultural context, time.[1]
Step 2 — Recommend clearly
State the plan as routine care. Pair with openness to questions.[7][18]
Step 3 — Explore
Elicit the dominant concern in the caregiver's words. Affirm the desire to protect the child — that motive is usually shared.[15]
Step 4 — Tailor the response
Match the 3C:[1]
- Confidence → brief accurate safety/effectiveness facts; avoid myth-first headlines; use plain numbers when you have verified local resources.
- Complacency → disease severity and outbreak reality without graphic fear theatre.
- Convenience → book, recall, outreach, after-hours, interpreter. [1]
Motivational interviewing (MI) skills help when ambivalence is high: open questions, affirmations, reflections, summaries; elicit–provide–elicit for information. MI-based maternity and postpartum programmes show reductions in hesitancy measures in trial settings — transfer the skill set to paediatric clinic with humility about context.[15][16]
Balanced benefits–harms consent resources can be acceptable without increasing hesitancy in study settings — use high-quality local tools rather than ad-hoc internet printouts.[17]
Step 5 — Agree a plan
Best outcome: vaccines given today. Next best: time-bound delay with a booked date and limited antigen list — not "someday". Partial protection beats none when a family will only accept some antigens now — still work toward the full schedule over time.[6][11]
Step 6 — Document and follow up
Document concerns, information given, vaccines accepted/refused, and the return plan. Leave the door open. Recall systems beat hope.[13]
Ethical response to firm refusal
Diekema and the AAP bioethics guidance frame a process: listen, correct misconceptions, explain benefits and risks of disease and vaccine, document, and continue care. Practice dismissal is ethically contested and jurisdiction-sensitive; many systems prioritise maintaining the medical home so future acceptance remains possible. Follow local professional guidance rather than importing another country's dismissal culture wholesale.[13]
Thirty-second version
Recommend the due vaccines as usual care
Ask what worries them most — then listen
Answer that one concern briefly and accurately
Offer today, or a booked time-bound plan
Document and keep the relationship
Specific Subtypes & Scenarios
Infant first-series delay
Often "too many too soon" or fever fear. Show the visit schedule, explain combination vaccines reduce injections, plan fever advice, avoid open-ended postponement of the whole primary course.[1]
MMR-only refusal
Name measles severity and outbreak risk without mocking. Correct autism myths briefly after empathy — do not open with "that is wrong". Offer same-day MMR; if refused, document and book revisit.[9]
"Spread out" requests
Acknowledge control motive. Explain more visits mean more delay and more risk windows. Negotiate the smallest safe compromise your handbook allows, with firm return dates — not an infinite custom schedule invented in the corridor.[1]
Adolescent HPV
Address cancer prevention indication in plain language. Separate sexuality stigma from vaccine purpose. Offer confidential space. School programmes change the logistics — coordinate rather than compete.[1]
Post-AEFI fear
Validate. Separate true medical review from internet narratives. If a real adverse event occurred, use the contraindications/AEFI pathway. If the event was expected fever, reframe and plan supportive care for the next dose.[1]
Migrant and refugee families
Lead with welcome and record reconstruction. Different schedules are not refusal. Use interpreters. Trust may need more than one visit.[2]
Outbreak surge
Prioritise unprotected infants and high-risk contacts. Keep messages short. Use public health scripts where provided. Still avoid shaming delayed families who now present.[1]
Telehealth
Good for concern exploration and booking; limited for same-day vaccination. Close the loop with an in-person immunisation slot.[1]
Complications & Pitfalls
| Pitfall | Why it hurts | Better move |
|---|---|---|
| Shame and sarcasm | Destroys trust | Respectful firmness |
| Fact-dump first | Backfire risk | Elicit then brief fact |
| Soft non-recommendation | Missed acceptance | Clear recommendation |
| Labelling access as attitude | Wrong fix | Remove barriers |
| Open-ended delay | Silent undervaccination | Booked time-bound plan |
| False absolute safety | Later betrayal | Honest common/rare framing |
| Ignoring adolescent | Incomplete consent picture | Dual conversation |
| Skipping documentation | No longitudinal plan | Structured note |
| Confusing contraindication with hesitancy | Wrong pathway | Medical algorithm first |
Prognosis & Disposition
Define success more richly than "they said yes today".[1]
Good short-term outcomes:[1]
- Relationship intact
- Specific concern addressed
- Doses given, or a dated plan booked
- Disease safety-netting understood
- Documentation complete [13]
Delayed acceptors often need two or three contacts. Practice-level outcomes include coverage, on-time rates, and re-engagement after refusal. Public health involvement follows outbreak and notifiable-disease rules, not personal frustration.[6][11]
Disposition after firm refusal: remain available, provide disease education, document, offer revisit, and do not abandon routine care for unrelated problems.[13]
Special Populations
Indigenous families — culturally safe communication, community-controlled services where available, and humility about historical medical injustice. Trust is clinical infrastructure.[5]
Refugee and asylum-seeking families — interpreters, trauma-aware pace, schedule differences, and convenience barriers.[1]
Children with medical complexity — caregivers often weigh real hospitalisation risk. Be precise about indications and household protection (cocooning) without overselling.[1]
Immunocompromised household contacts — reframe vaccination of healthy siblings and caregivers as family protection.[1]
Neurodiversity — sensory planning for the injection visit itself can be the real barrier once attitude is sorted.[1]
Out-of-home care — clarify who holds consent authority before you counsel the wrong adult.[1]
Socioeconomic disadvantage — treat convenience as first-line therapy: transport help, opportunistic dosing, fewer visits where combination vaccines allow.[1]
Evidence, Guidelines & Regional Differences
Landmark frames: SAGE definition and determinants; global hesitancy reviews; provider communication studies; psychological science of vaccination behaviour; RCTs showing that not every message strategy helps.[1][2][7][9][11]
MI-informed counselling has growing experimental support in maternity/postpartum settings and practical frameworks for vaccine motivation.[15][16]
Use the Australian Immunisation Handbook communication principles and the Australian Immunisation Register for status. Policy levers such as No Jab No Pay/Play are system context — they are not a clinic script for shaming. Aotearoa New Zealand programmes and equity priorities for Māori and Pacific families should shape outreach and trust work. Official handbook language beats memory for schedule detail.
Canadian practice follows NACI guidance with provincial delivery differences. Globally, convenience barriers dominate in some settings while confidence dominates in others — always localise the 3C emphasis.
Exam Pearls
- Definition: delay or refusal despite availability.[1]
- Continuum, not binary.
- 3Cs: confidence, complacency, convenience.[1]
- Recommend clearly; elicit the real fear; answer that fear; plan; document.[7][5]
- Fact-dumps can backfire — tone and order matter.[9]
- Providers overestimate deep hesitancy — still give a recommendation.[14]
- PACV is a survey tool, not a mandatory bedside score.[12]
- True contraindication ≠ hesitancy.
- Time-bound delay beats open-ended delay.
- Communication exams test process and relationship under pressure.
References
- [1]MacDonald NE, SAGE Working Group on Vaccine Hesitancy Vaccine hesitancy: Definition, scope and determinants. Vaccine, 2015.PMID 25896383
- [2]Larson HJ, Jarrett C Understanding vaccine hesitancy around vaccines and vaccination from a global perspective: a systematic review of published literature, 2007-2012. Vaccine, 2014.PMID 24598724
- [3]Dubé E, Laberge C Vaccine hesitancy: an overview. Human vaccines & immunotherapeutics, 2013.PMID 23584253
- [4]Larson HJ, Jarrett C Measuring vaccine hesitancy: The development of a survey tool. Vaccine, 2015.PMID 25896384
- [5]Goldstein S, MacDonald NE Health communication and vaccine hesitancy. Vaccine, 2015.PMID 25896382
- [6]Eskola J, Duclos P How to deal with vaccine hesitancy? Vaccine, 2015.PMID 25896378
- [7]Opel DJ, Mangione-Smith R The Influence of Provider Communication Behaviors on Parental Vaccine Acceptance and Visit Experience. American journal of public health, 2015.PMID 25790386
- [8]Opel DJ, Zhou C Impact of Childhood Vaccine Discussion Format Over Time on Immunization Status. Academic pediatrics, 2018.PMID 29325912
- [9]Nyhan B, Reifler J Effective messages in vaccine promotion: a randomized trial. Pediatrics, 2014.PMID 24590751
- [10]Betsch C, Renkewitz F The influence of vaccine-critical websites on perceiving vaccination risks. Journal of health psychology, 2010.PMID 20348365
- [11]Brewer NT, Chapman GB Increasing Vaccination: Putting Psychological Science Into Action. Psychological science in the public interest : a journal of the American Psychological Society, 2017.PMID 29611455
- [12]Opel DJ, Mangione-Smith R Development of a survey to identify vaccine-hesitant parents: the parent attitudes about childhood vaccines survey. Human vaccines, 2011.PMID 21389777
- [13]Diekema DS, American Academy of Pediatrics Committee on Bioethics Responding to parental refusals of immunization of children. Pediatrics, 2005.PMID 15867060
- [14]Healy CM, Montesinos DP Parent and provider perspectives on immunization: are providers overestimating parental concerns? Vaccine, 2014.PMID 24315883
- [15]Gagneur A, Gutnick D From vaccine hesitancy to vaccine motivation: A motivational interviewing based approach to vaccine counselling. Human vaccines & immunotherapeutics, 2024.PMID 39187772
- [16]Verger P, Cogordan C A postpartum intervention for vaccination promotion by midwives using motivational interviews reduces mothers' vaccine hesitancy, south-eastern France, 2021 to 2022: a randomised controlled trial. Euro surveillance : bulletin Europeen sur les maladies transmissibles = European communicable disease bulletin, 2023.PMID 37733238
- [17]McDonald C, Leask J A Consent Support Resource with Benefits and Harms of Vaccination Does Not Increase Hesitancy in Parents-An Acceptability Study. Vaccines, 2020.PMID 32887503
- [18]Hofstetter AM, Robinson JD Clinician-parent discussions about influenza vaccination of children and their association with vaccine acceptance. Vaccine, 2017.PMID 28392141