Paeds · professional-practice-and-evidence
Best-interests decisions and treatment limitation
Also known as Best-interests standard in paediatrics · Limitation of life-sustaining treatment in children · Withholding and withdrawing treatment · Goals-of-care and treatment-limitation decisions · Medical futility in children · DNACPR and Allow Natural Death decisions · End-of-life decision-making for children
Fellowship-level approach to best-interests decisions and treatment limitation in paediatrics: the best-interests balance of benefits against burdens, the zone of parental discretion, futility, withholding and withdrawing life-sustaining treatment, goals-of-care conversations, DNACPR/Allow Natural Death, ethics consultation and the courts, paediatric palliative care, and regional differences across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture a seven-year-old with a progressive neurodegenerative disease back in PICU for the third time this winter, now ventilated and not weaning. The team believes intensive care can no longer help her. Your job is not to decide alone, and it is not to walk away. It is to work out, with the family, what is now in this child's best interests. [1]
Four terms do most of the work. The best-interests standard is the test for a child who cannot decide for themselves: it balances the benefits of a treatment against its burdens from the child's point of view. Life-sustaining treatment (LST) is any treatment that prolongs life without curing the underlying condition — ventilation, CPR, artificially delivered nutrition and hydration, cardioactive drugs. Withholding means never starting a treatment; withdrawing means stopping one already begun, and the two are morally equivalent. [4] [1]
Limitation of treatment is the umbrella term for deciding not to start, or to stop, life-sustaining interventions judged no longer beneficial. Futility describes a treatment that cannot achieve its physiological goal. And a goals-of-care order documents what the team will and will not offer, and what comfort will be provided — it is far more than a single resuscitation decision. [1] [4]
[1] [4]Classification
Start from the stakes of the decision, not from a statute book. The pathway you follow depends on whether the decision sits inside the parents' zone of discretion, at the best-interests threshold, or in a disputed refusal that engages the harm principle. [2] [3]
The zone of parental discretion covers low-stakes, reversible, routine decisions — what to eat, when to treat a minor infection, which antibiotic. Parents decide within this zone, and clinicians advise. Here the parent's view ordinarily governs because the decision does not risk serious harm. [2]
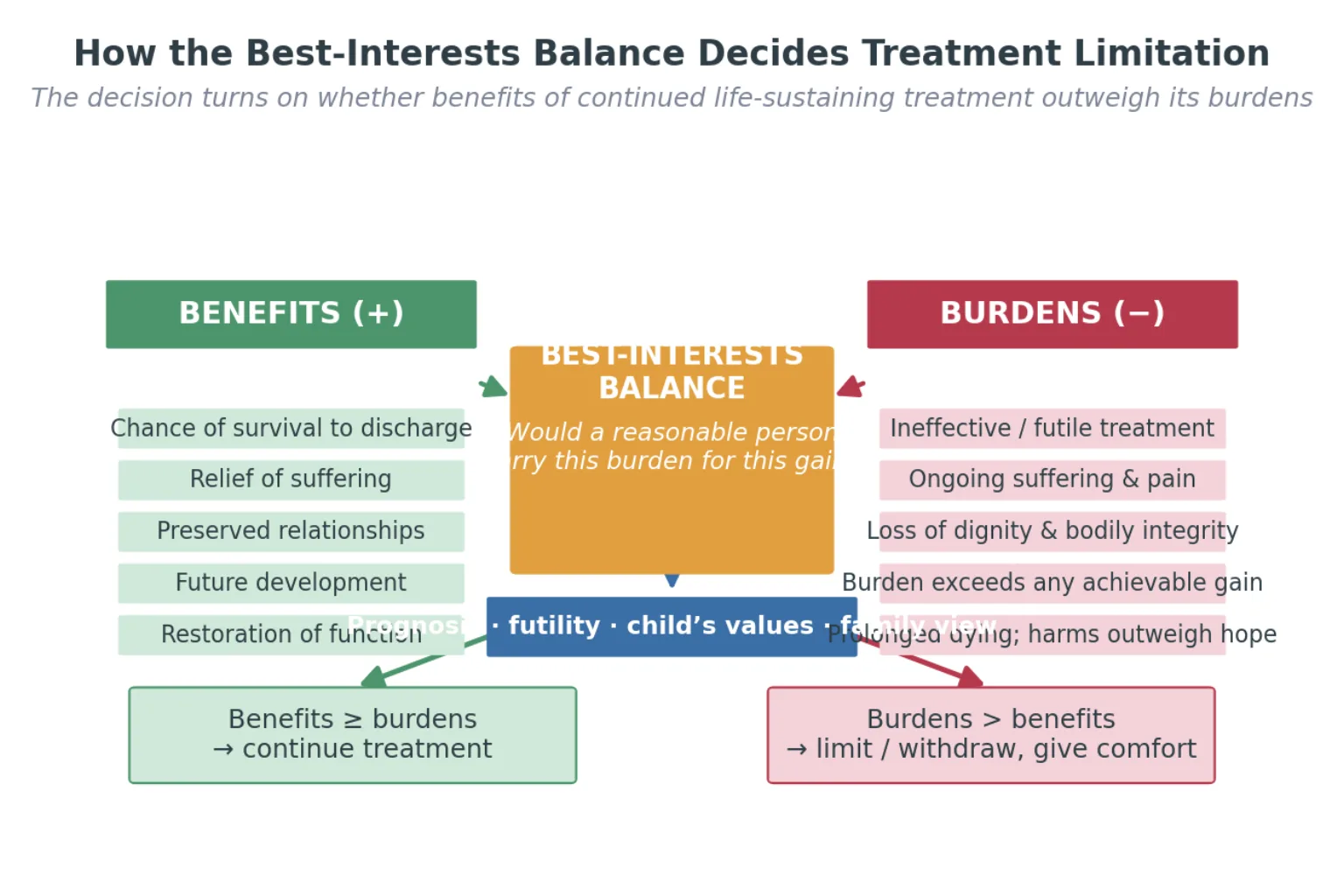
The best-interests balance governs high-stakes, life-sustaining decisions where benefits and burdens must be weighed. This is the core territory of treatment limitation: would a reasonable person carry this burden for this gain? You seek shared agreement with the family, but the child's interests, not parental preference alone, set the limit. [1] [3]
The harm-threshold pathway engages when parents refuse treatment that would prevent serious, foreseeable and imminent harm, or demand treatment the team judges non-beneficial. Here senior escalation, ethics consultation and usually the courts arbitrate — never a solo bedside override. [2] [12]
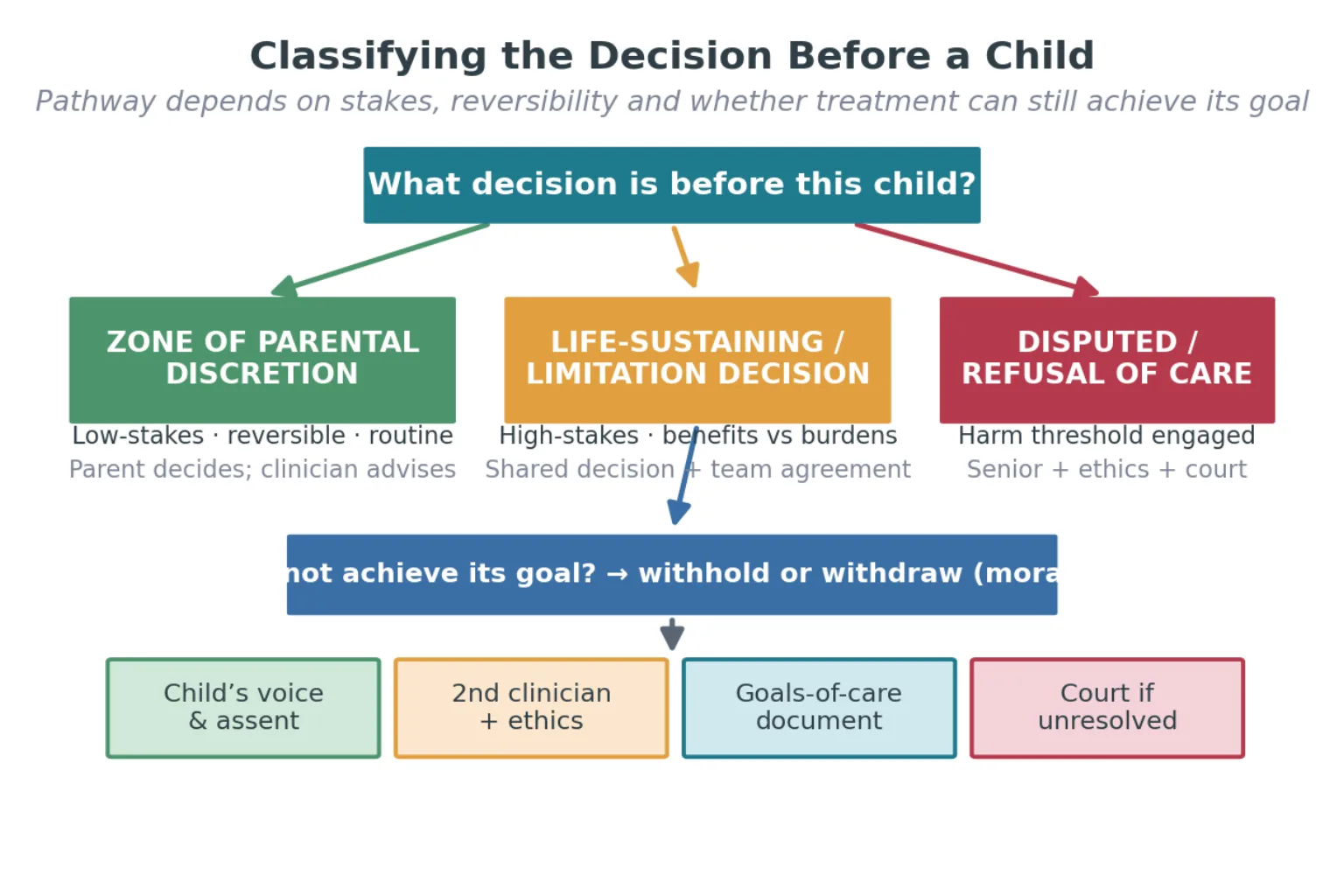
Decision pathway by stakes
Epidemiology & Risk Factors
Most children who die in hospital do so after an active decision to limit treatment. In PICU cohorts the majority of deaths follow withdrawal or withholding of life-sustaining treatment rather than failed resuscitation, and the same pattern holds across neonatal intensive care over recent decades. [8] [11]
The children most often facing limitation decisions share recognisable profiles: extreme prematurity with severe brain injury, progressive neurodegenerative disease, relapsed refractory cancer, severe acquired brain injury, and technology-dependent children with complex chronic illness who accumulate recurrent critical episodes. [1] [9]
Conflict grows where prognostic uncertainty is high and the 'false hope' window stays open. Evolving diagnoses, optimistic early messaging, and families told different things by different clinicians all feed a sense that more time will bring a different answer. Mistrust, prior loss, cultural or religious expectations of miracle, and low health literacy each raise the chance that a limitation conversation lands as abandonment. [10]
Social determinants change access to the supports that make limitation decisions humane. Rurality, migrant or refugee status, poverty and language discordance all alter whether a family meets palliative care, ethics support and community services before a crisis forces the conversation in an emergency department. [9] [10]
Clinician variability is itself a risk factor. Moral distress, fear of complaint, and personal views about quality of life drive inconsistent limitation practice between teams and even between shifts, so structured frameworks and second opinions exist partly to discipline that variability. [1]
Pathophysiology
There is no enzyme for futility, but there is a mechanism. The trajectory of the underlying condition shapes when limitation becomes appropriate, and the balance between benefit and burden shifts as the disease evolves. [5]
A catastrophic, irreversible brain injury opens what Wilkinson called the window of opportunity — a period when prognosis is at its clearest and withdrawal, if it is to happen, is most defensible. As time passes the picture muddies, complications accumulate, and the same withdrawal becomes harder to justify and harder to execute well. [5]
Physiological futility is a factual claim: the treatment cannot achieve its physiological goal, so a ventilator cannot oxygenate, or CPR cannot restore a perfusing rhythm. Qualitative (overall) futility is a value judgement: even if the treatment works physiologically, the overall burden to the child exceeds any achievable gain. Both can justify limitation, but only the first is purely factual, which is why qualitative futility demands shared deliberation, not a unilateral declaration. [4] [1]
Cumulative burdens erode the benefit side of the balance. Pain, repeated procedures, loss of bodily integrity, prolonged separation from family and loss of dignity all count, and they accrue silently. A child who 'tolerated' intensive care a month ago may now be bearing a burden that no longer buys meaningful benefit. [4]
The dying process itself generates symptoms that comfort care must anticipate. Dyspnoea, secretions, pain, agitation and terminal restlessness are predictable, and a limitation plan that ignores them produces a distressed death. This is why withdrawal of ventilation is an active comfort procedure, with opioid and benzodiazepine given for symptom relief, the family present, and aftercare planned. [9] [4]
Clinical Presentation
From the doorway, a well-run limitation meeting looks calm, private and unhurried. The room is right, the right people are present, an interpreter is booked if needed, and it is clear who is leading the conversation and why it is happening now. [10]
A child with a progressive neurodegenerative condition presents the 'burden now exceeds benefit' inflection point. Each admission is harder to wean, the baseline function has fallen, and the family and team share an unspoken sense that the trajectory has changed. The presentation is often a respiratory failure admission that this time does not turn around. [1]
An extreme preterm infant with severe intraventricular haemorrhage and progressive post-haemorrhagic hydrocephalus presents the limitation question early. The window-of-opportunity logic applies: the prognosis is clearest in the first days, and a decision made then is more defensible than one made after weeks of complications. [5] [11]
An oncology patient with relapsed refractory disease presents the transition from cure-focused to comfort-focused care. The trigger is often cumulative treatment-related toxicity alongside disease progression, and the conversation is about redefining success, not giving up. [9]
A child with severe acquired brain injury after a cardiac arrest or near-drowning presents the acute withdrawal decision. Here the prognosis, not the family's wishes alone, may drive the team's recommendation, and the timing of the conversation matters. [5]
A family may present ambivalence, false hope, or a request to 'do everything' that masks unspoken fears — fear of abandonment, of pain, of losing their child without a fight. A reassuring, agreeable family can still hide an outdated or misunderstood plan, so you check what is actually documented, not just what was said. [10]
Differential Diagnosis
When the team feels a child is being overtreated, your first task is to work out what kind of problem it is. The label changes everything downstream. [1]
| Surface presentation | What it might actually be | Must-not-miss alternative |
|---|---|---|
| "The child is being overtreated" | Clinician burnout or prognostic pessimism | True physiological futility with a defensible plan |
| "The family wants everything" | Unspoken fear, not a clinical instruction | Genuine value conflict needing ethics and court |
| "It's futile" | A prognosis the clinician merely finds grim | Physiologically defined non-benefit |
| "We're withdrawing care" | A limitation of life-sustaining treatment | Brain death, which is death, not a withdrawal |
Discriminate physiological futility from a prognosis you simply find grim. A treatment is physiologically futile only when it cannot achieve its goal; a low probability of success is not the same as futility, and conflating them forecloses a time-limited trial that might still be appropriate. [4]
Distinguish a limitation decision from brain death. Brain death is death, and testing for it follows statutory and clinical criteria; it is not a treatment withdrawal. Conflating the two is a serious and examinable error. [4]
Separate a value dispute from a factual dispute. When the team and family disagree about the prognosis, more information, second opinions and time may resolve it. When they disagree about what an acceptable outcome would be — what counts as a life worth living — that is a value dispute, and it belongs with ethics and, if needed, the courts. [6] [12]
When prognosis is uncertain, prefer a time-limited trial over a permanent decision. Treat intensively to a defined endpoint — a number of days, or a specific reassessment — and agree in advance what will happen if the trial fails. This respects uncertainty without committing to indefinite non-beneficial treatment. [1]
Clinical & Bedside Assessment
Open a limitation meeting by setting the scene and giving a warning shot. Name who is present, state that the meeting is about the direction of care, and prepare the family before delivering hard information. [10]
Then assess the medical facts that drive the balance. What is the diagnosis and prognosis? Is the deterioration reversible or a progression of the underlying condition? Can the treatment still achieve its goal, or is it physiologically futile? What cumulative burden has the child already borne? [4] [1]
Assess the child's voice directly, developmentally. A school-age or adolescent child can often express preferences about continued treatment or stopping, and their assent or dissent deserves weight even when they are not the legal decision-maker. Excluding the child from a conversation that concerns them is a recognised error. [7] [10]
Assess family understanding, values and fears. What matters most to this family? What would the child have wanted? What cultural, spiritual or faith framing shapes how they hear prognosis? Bring trusted community or faith support into the room when the family wants it. [9]
Bring a second senior clinician and the wider team to consensus before proposing limitation. A limitation recommendation that comes from one registrar in isolation is fragile; one that emerges from the treating team, documented and shared, is defensible. [1]
Assess whether prognosis is certain enough to limit now, or whether a time-limited trial is more honest. Certainty is rare, and a defined trial often serves the child better than a premature permanent decision. [1] [5]
Investigations
There is no blood test for best interests, but several investigations confirm the irreversibility or prognosis that a limitation decision rests on. Neuroimaging, EEG, somatosensory evoked potentials and ancillary testing clarify prognosis after brain injury, and they inform but never replace the best-interests judgement. [5]
A time-limited trial of intensive treatment is itself the investigation of an uncertain prognosis. When you cannot know whether a child will recover, you treat intensively to a defined endpoint and then reassess, turning uncertainty into information rather than paralysis. [1]
Multidisciplinary inputs function as adjuncts to the decision. Palliative care, clinical ethics, allied health, psychology and faith leaders each bring a perspective the treating team lacks, and involving them early is part of the assessment, not an admission of failure. [9] [10]
Symptom assessment tools guide comfort care after a limitation decision. Validated paediatric pain, agitation and dyspnoea scales help you anticipate and treat what the dying process will produce, so comfort is planned, not improvised. [9]
A prior documented goals-of-care or advance care plan must be interpreted in light of current clinical change. A plan written months ago may no longer fit a child whose condition has moved on, so you revisit it rather than apply it mechanically. [1]
When a limitation decision is genuinely contested, the appropriate 'investigation' becomes the consultation itself: a second opinion, an ethics consultation, or legal advice is the right next step rather than another scan. [6] [12]
Management — Resuscitation
When a child with an active limitation or comfort plan deteriorates, you escalate comfort, not resuscitation. An active limitation order means you do not initiate CPR or escalation that the plan has already judged non-beneficial. [4] [1]
Distinguish a reversible intercurrent event from progression of the underlying condition. A child on a comfort plan may still develop a treatable, distressing problem — a blocked tracheostomy, a treatable seizure, a painful fracture — and you treat what relieves suffering even as you hold the overall direction. [9]
If a child arrests before any plan exists, ask whether resuscitation itself is non-beneficial. In a child with end-stage disease, a witnessed and prolonged arrest, or a clearly irreversible cause, CPR may add burden without benefit, and the team may reasonably not attempt it — but this judgement must be defensible and documented. [4]
Allocate roles so comfort and family support run in parallel. One clinician leads symptom care, another supports the family, and the limitation plan is handed over explicitly at every shift change so the direction of care never depends on who is on. [9]
Reframe withdrawal of ventilation as an active comfort procedure. Opioid and benzodiazepine are given for symptom relief, the family is present, extubation is planned, and aftercare is arranged — this is the opposite of abandonment, and the family needs to hear that. [9] [4]
Anticipate and treat the reversible symptoms of dying: pain, dyspnoea, agitation, secretions and terminal restlessness are predictable, and a comfort plan that does not address them produces a distressed death. [9]
Management — Definitive & Stepwise
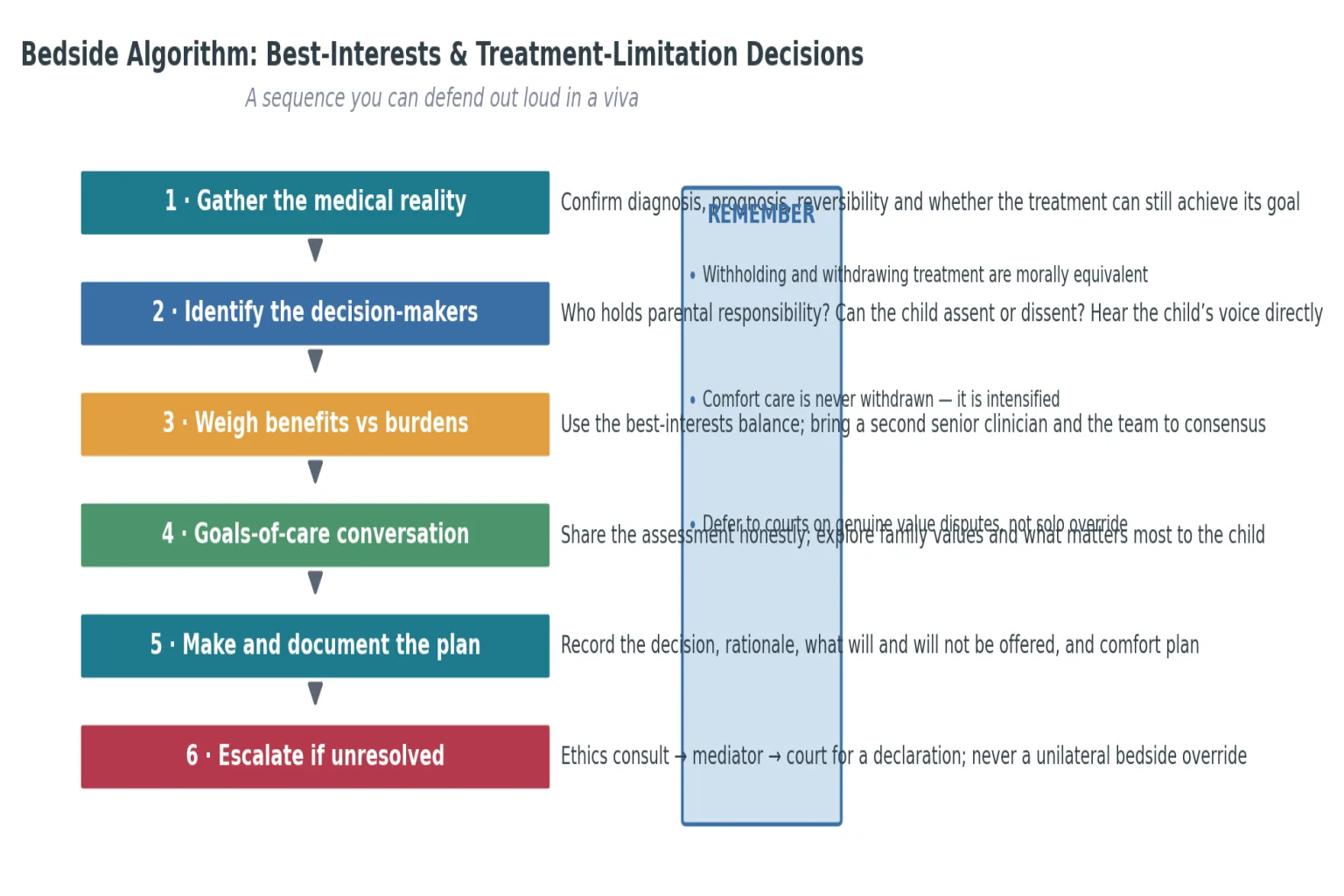
Use a sequence you can defend out loud in a viva, anchored on the best-interests balance and the RCPCH limitation framework. [1] [4]
Best-interests and limitation algorithm
Gather the medical reality — diagnosis, prognosis, reversibility, can the treatment still achieve its goal?
Identify the decision-makers — who holds parental responsibility, and what does the child think?
Weigh benefits against burdens — survival, relief, relationships against suffering, futility, dignity
Bring a second senior clinician and the team to consensus
Hold the goals-of-care conversation — share information, explore values, agree a plan
Make and document the decision — what will and will not be offered, and the comfort plan
Escalate to ethics consultation, mediation and the courts only if a genuine value dispute remains
Plan bereavement follow-up and staff debrief
Structure the goals-of-care conversation with a recognised framework — the Serious Illness Conversation Guide, Ask-Tell-Ask, or SPIKES. Ask what the family understands and what matters most, give a warning shot, share the prognosis honestly, explore their values, and agree a plan you both own. [10] [7]
Decide between continuing treatment, a time-limited trial, and limiting or withdrawing treatment using the certainty of prognosis. When the trajectory is clear and burdens outweigh benefits, limit. When it is uncertain, run a time-limited trial with a defined review date. [1] [5]
Operationalise a DNACPR or Allow Natural Death decision as part of an overall limitation plan, never as an isolated order. An order that says 'no CPR' but leaves ventilation, escalation and comfort undefined is incomplete and examinable. [1]
Conduct a planned withdrawal with attention to setting, family presence, symptom medication and aftercare. Integrate paediatric palliative care early and in parallel with disease-directed therapy, so comfort expertise is already in place when the balance shifts. [9]
Specific Subtypes & Scenarios
Extreme preterm infant with severe bilateral IVH. The window of opportunity applies: prognosis is clearest early. Weigh the probability of severe neurodevelopmental outcome against the burden of prolonged intensive care, and either continue, run a time-limited trial, or redirect to comfort — with the family, second clinician and team. [5] [11]
Progressive neurodegenerative disease with recurrent PICU admissions. Run a ceiling-of-care and goals-of-care conversation between crises, not during one. Agree what will and will not be offered at the next deterioration, and document it so the plan survives a 3 a.m. admission. [1]
Relapsed refractory oncology with treatment-related toxicity. Transition from curative to palliative intent by redefining success. Parallel-track palliative care early so the shift is a change of emphasis, not an abrupt abandonment of the team the family trusts. [9]
Severe acquired brain injury after cardiac arrest. Apply the window-of-opportunity logic. Confirm prognosis with neuroimaging and electrophysiology, and if recovery to a meaningful baseline is not achievable, bring a recommendation to the family within the clearest window. [5]
Technology-dependent child with recurrent aspiration. Review the ceiling of care over time. A tracheostomy and home ventilation that served the child well a year ago may now sit above the burden line, and a goals-of-care review is overdue rather than defeatist. [1]
Family requesting ventilation the team judges futile. This is a value dispute, not a factual one. Engage ethics consultation, mediation and a second opinion; if consensus cannot be reached, seek a court declaration rather than overriding or capitulating unilaterally. [6] [12]
Adolescent voicing a wish to stop treatment. Hear the young person directly. Their voice deserves weight even when they are not the legal decision-maker, and a wish to stop may reflect fear, pain or depression that is itself treatable. [10] [7]
Child in out-of-home care. Identify the statutory decision-maker for a major limitation decision. Routine care may sit with the carer, but a limitation decision usually requires the statutory guardian and, sometimes, the court. [1]
Migrant or refugee family expecting a miracle. Use a professional interpreter, pace the conversation for trauma, and bring a trusted faith leader into the room. Honour the hope while sharing the prognosis honestly. [9] [10]
Sudden unexpected death in the ED before any plan. Recognise when resuscitation itself is non-beneficial — a prolonged arrest in a child with end-stage disease — and shift the team's energy to family-centred care rather than continuing CPR that cannot succeed. [4]
Complications & Pitfalls
- Treating an isolated DNACPR order as a complete limitation plan. [1]
- Equating the emotional weight of withdrawing with a moral difference from withholding. [4]
- Declaring futility unilaterally without a second clinician, the team and ethics input. [1]
- Conflating brain death with a treatment-limitation decision. [4]
- Continuing invasive treatment past the point of benefit because no one raised limitation early. [5]
- Excluding the child or young person from a conversation that concerns them. [7]
- Using family members as interpreters for high-stakes limitation meetings. [9]
- Framing limitation as giving up rather than redirecting to comfort and what matters. [10]
- Failing to anticipate and treat symptoms after withdrawal, causing a distressed death. [9]
- Letting a value dispute escalate to court without first trying ethics consultation, mediation and time. [6]
Prognosis & Disposition
A good limitation process pays off in the short term. A peaceful death, better family bereavement adjustment and reduced staff moral distress all follow a conversation in which the family understood, was heard, and felt accompanied to the end. [9] [10]
A time-limited trial is an appropriate disposition while prognosis evolves. Treat intensively to a defined endpoint, agree in advance what happens if the trial fails, and convert the trial into a definitive plan at the reassessment rather than letting it drift. [1]
A contested limitation decision may require keeping the child in hospital pending ethics or court resolution. Do not discharge a deadlock to an unsafe environment, and do not press ahead with a unilateral withdrawal while a value dispute is live. [6] [12]
Many children can be discharged home on a comfort plan with community palliative support. Coordinate with community services, write an accessible plan, and ensure the family knows who to call and what to expect. [9]
Court or guardianship processes change who must be notified. Hand over the limitation plan at every shift change — what will and will not be offered, what comfort is in place, and what escalation is live — so the direction of care never depends on who is on. [1]
Bereavement follow-up and staff debrief belong to the disposition, not an afterthought. A structured debrief helps the team process a difficult withdrawal, and bereavement contact with the family closes the relationship rather than ending it abruptly. [9] [10]
Special Populations
Neonates and extreme preterm infants. Limitation decisions turn on prognosis, long-term neurodevelopmental outcome and the window of opportunity; decisions are most defensible when made early and with the family. [5] [11]
Children with severe neurodisability. Avoid quality-of-life bias. Weigh benefits and burdens in the child's own terms and lived experience, not in an outsider's projection of what their life is worth. [3] [9]
Technology-dependent children. Review the ceiling of care and goals over time. A tracheostomy, home ventilation or feeding tube that was right a year ago may now sit above the burden line. [1]
Adolescents with life-limiting illness. Hear the young person directly, respect emerging autonomy, and weight assent and dissent even when they are not the legal decision-maker. [7] [10]
Indigenous families. Run culturally safe, kinship-inclusive goals-of-care conversations. Identify kinship decision-makers and respect wishes around dying on country where the family seeks it, while still verifying legal authority. [9]
Migrant and refugee families. Use professional interpreters, pace the conversation for trauma, and explain local norms and palliative services the family may not know exist. [9] [10]
Out-of-home care and youth justice. Identify the statutory decision-maker for major limitation decisions. Routine care may sit with the carer; a limitation decision usually does not. [1]
Faith communities expecting miracle. Engage respectfully and honestly. Share the prognosis, avoid false reassurance, and bring a trusted faith leader into the conversation when the family wants one. [10]
Socioeconomic disadvantage and low health literacy. Use teach-back, plain language, time and written materials. A plan a family cannot understand or afford to enact at home is not a workable disposition. [9]
Children facing sudden unexpected death. Recognise when resuscitation itself is non-beneficial and shift the team to family-centred care rather than continuing CPR that cannot succeed. [4]
Evidence, Guidelines & Regional Differences
The RCPCH 2015 framework (Larcher, Craig, Bhogal, Wilkinson and Brierley) is the core anchor for limiting treatment in life-limiting and life-threatening conditions in children, and it frames the language examiners expect. It sets out the best-interests balance, the value of shared decision-making, and the place of withholding and withdrawing treatment. [1]
Truog and colleagues' 2008 SCCM consensus established that withholding and withdrawing life-sustaining treatment are morally equivalent, and that end-of-life care in the ICU should be active, planned and family-centred. [4]
Kon and colleagues' 2016 SCCM/ATS shared decision-making policy frames how clinicians and families should make high-stakes decisions together, and how to respond to requests for potentially inappropriate treatment. [7]
On the limits of agreement, Wilkinson argued for the window of opportunity for treatment withdrawal and later made the case for medical dissensus — that in some end-of-life disputes we should agree to disagree rather than force a single answer. [5] [6]
Diekema articulated the harm principle as the threshold for overriding parental refusal, and revisited how the best-interests standard is used and misused. Freckelton and McGregor traced the emerging international judicial consensus on minors and life-saving treatment. [2] [3] [12]
Garros and colleagues showed that most deaths in the PICU follow an active decision to limit treatment, and Barry and colleagues traced the same pattern in neonatal intensive care over four decades — evidence that limitation is the norm, not the exception, in paediatric critical-care death. [8] [11] Himelstein and colleagues set out paediatric palliative care principles, and Morrison and Feudtner showed how to titrate clinician directiveness in serious illness. [9] [10]
Australia and Aotearoa New Zealand approach treatment limitation through a mix of statute, common law and the courts. The Royal Children's Hospital Melbourne framework and the 'Thinking Ahead' advance care planning resource guide goals-of-care conversations. State the principle — limitation follows a best-interests balance of benefits against burdens, and genuine disputes go to the courts — and direct examiners to local statute, hospital policy and legal advice for operational thresholds. Never invent a statutory section number or a named case citation. [1]
Exam Pearls
WEIGH
References
- [1]Larcher V, Craig F, Bhogal K, Wilkinson D, Brierley J Making decisions to limit treatment in life-limiting and life-threatening conditions in children: a framework for practice. Arch Dis Child, 2015.PMID 25802250
- [2]Diekema DS Parental refusals of medical treatment: the harm principle as threshold for state intervention. Theor Med Bioeth, 2004.PMID 15637945
- [3]Diekema DS Revisiting the best interest standard: uses and misuses. J Clin Ethics, 2011.PMID 21837884
- [4]Truog RD, Campbell ML, Curtis JR, Haas CE, Luce JM, Rubenfeld GD Recommendations for end-of-life care in the intensive care unit: a consensus statement by the American College of Critical Care Medicine. Crit Care Med, 2008.PMID 18431285
- [5]Wilkinson D The window of opportunity for treatment withdrawal. Arch Pediatr Adolesc Med, 2011.PMID 21383270
- [6]Wilkinson D In Favour of Medical Dissensus: Why We Should Agree to Disagree About End-of-Life Decisions. Bioethics, 2016.PMID 25908398
- [7]Kon AA, Davidson JE, Morrison W, Danis M, White DB Shared Decision Making in ICUs: An American College of Critical Care Medicine and American Thoracic Society Policy Statement. Crit Care Med, 2016.PMID 26509317
- [8]Garros D, Rosychuk RJ, Cox PN Circumstances surrounding end of life in a pediatric intensive care unit. Pediatrics, 2003.PMID 14595079
- [9]Himelstein BP, Hilden JM, Boldt AM, Weissman D Palliative care for infants, children, adolescents, and their families. J Palliat Med, 2006.PMID 16430356
- [10]Morrison W, Feudtner C Titrating Clinician Directiveness in Serious Pediatric Illness. Pediatrics, 2018.PMID 30385625
- [11]Barry A, Byrne S, Synnott M, O'Donoghue K, O'Connell O End-of-life care over four decades in a quaternary neonatal intensive care unit. J Paediatr Child Health, 2023.PMID 36495233
- [12]Freckelton I, McGregor S Refusal of potentially life-saving treatment for minors: The emerging international consensus by courts. J Law Med, 2016.PMID 30136557