Paeds · professional-practice-and-evidence
Communicating risk and uncertainty to families
Also known as Risk communication in paediatrics · Communicating numerical risk and uncertainty · Natural frequencies and pictographs · Shared risk and benefit-harm communication · Prognostic uncertainty communication
Fellowship guide to communicating risk and uncertainty to families in paediatrics: risk versus uncertainty, aleatory versus epistemic uncertainty, natural frequencies and pictographs, absolute versus relative risk, framing effects, numeracy and graph-literacy barriers, prognostic uncertainty and honest hope, decision aids, teach-back and documentation; with ANZ/UK/US/Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Present any number in five moves
Overview & Definition
A mother reads online that a treatment "reduces harm by 50%". In your clinic she asks whether her child should have it. Before you answer a single clinical question, you face a communication problem: that 50% is a relative reduction, and she has no idea what it is relative to. Whether she consents well or badly now depends on how you handle the number. [1] [10]
Risk communication is the work of conveying the probability and magnitude of potential benefits and harms in a form a family can use to make decisions. In paediatrics the family is the unit of decision, and the child or young person is included developmentally, so the numbers must reach not only a parent but the right people in the right language. [14]
Uncertainty sits beside risk in every such conversation. It has two flavours. Aleatory uncertainty is irreducible chance — the run of luck in who is affected. Epistemic uncertainty is the gap in what we know, which better evidence can narrow but rarely close. Prognosis in a relapsing illness, the meaning of an incidental finding, and the long-term effects of a new treatment all carry epistemic uncertainty that families deserve to hear named. [4] [13]
This page owns the process and skills of presenting numbers and uncertainty. Cross-link the dedicated leaves for shared decision-making and assent, breaking bad news, vaccine-hesitancy counselling, consent frameworks, health literacy, and working with interpreters — do not rebuild their content here. [14]
Classification
Sort the work by the kind of number you are sharing and the format that fits it. [1] [7]
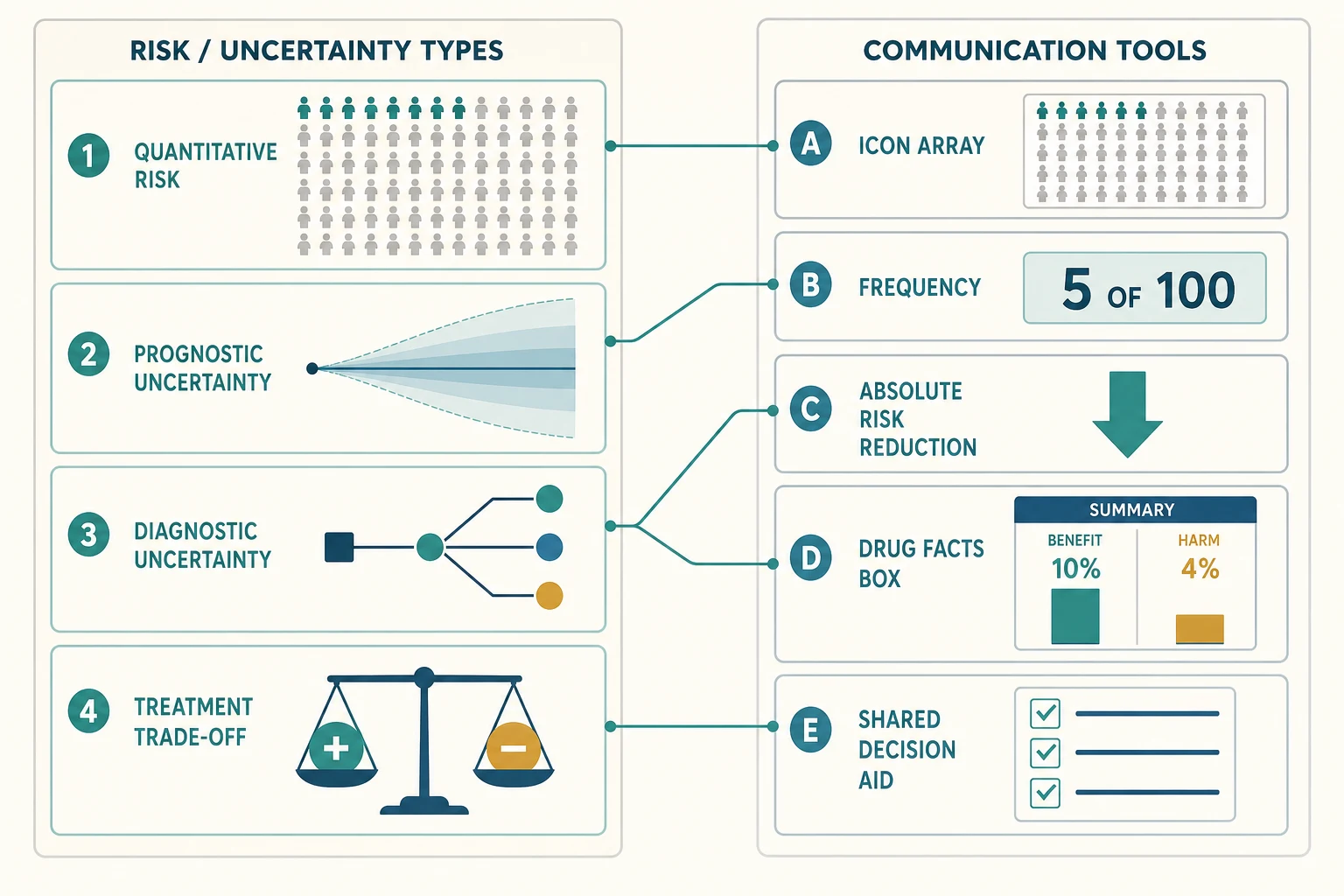
Kinds of risk and uncertainty. Quantitative risk — the chance of a defined outcome, such as a surgical complication or a vaccine side effect. Prognostic uncertainty — a forecast that fans out over time, as in a chronic or relapsing illness. Diagnostic uncertainty — the residual chance that a screen or test is wrong, or that a finding is incidental. Treatment trade-off — a choice where benefits and harms compete, such as surgery against observation. [4]
Presentation formats. Natural frequencies (5 in 100). Absolute risk and absolute risk reduction with the baseline stated. Pictographs or icon arrays that make the denominator visible. A drug-facts box that pairs benefit and harm side by side. A full patient decision aid for high-stakes, preference-sensitive choices. These are not interchangeable fashions; each serves a different cognitive job. [3] [5] [7]
What to avoid. Relative risk without the absolute baseline, single point estimates where a range is honest, inconsistent denominators, and one-sided framing. Each of these misleads a family and is a recognised failure mode. [1] [10]
Epidemiology & Risk Factors
Most adults, including highly educated ones, struggle with the statistics that clinicians trade in daily. Cross-cultural population surveys show that only a minority can answer basic probability and numeracy questions correctly, and graph literacy varies widely between and within countries. [12] [11] This is not a fringe problem — it is the default, and it is the reason a percentage handed over without support so often fails.
The format a clinician chooses changes the decision a family makes. Relative-risk framing inflates perceived benefit; the same drug described as halving harm sounds more attractive than when described in absolute terms. Decades of behavioural research show this effect is robust and is exploited, knowingly or not, in marketing and sometimes in clinical summaries. [1] [10]
Inequity runs through the field. Families with low health literacy, limited language proficiency, or fewer resources are most often given the hardest-to-parse formats, and they carry the consequences. Communication gaps compound when screening results, vaccine choices, and life-limiting prognoses arrive without a pictograph, an interpreter, or a decision aid. [4] [14]
Paediatrics keeps this work in constant view. Newborn and prenatal screening, immunisation, medication choices for chronic disease, surgical decisions, and prognostic conversations in oncology and neurodisability all turn on how well a probability is shared. [14]
Pathophysiology
Think about why a number lands wrong, and what protects it. [1] [4]
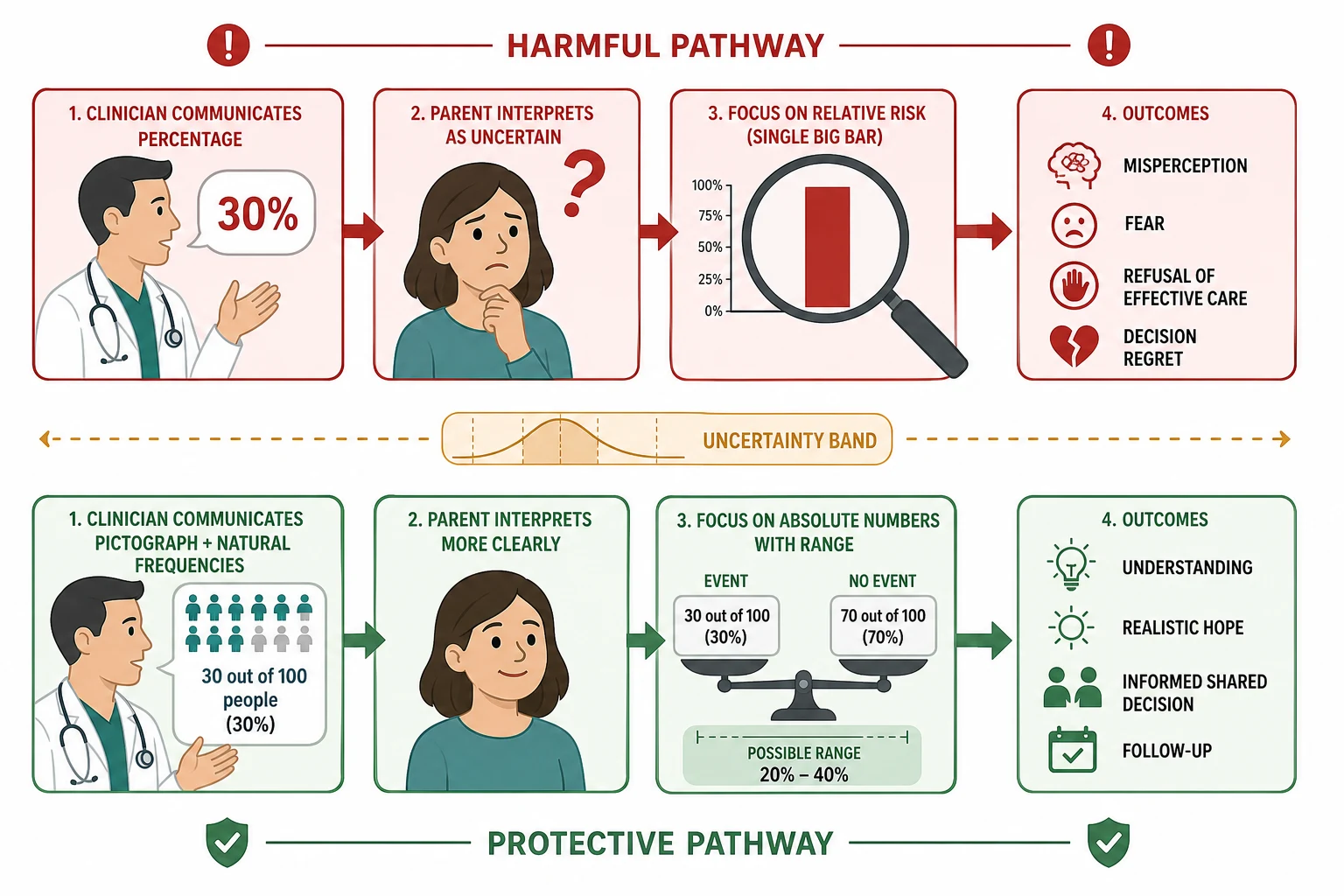
Denominator neglect and base-rate neglect. A percentage is just a numerator divorced from its denominator, and the human mind anchors on the numerator. "5%" feels small or large depending on nothing but the number five, whereas "5 in 100" carries the population with it. This is why natural frequencies outperform percentages for nearly everyone, expert and lay alike. [1] [8]
Relative-risk inflation. A 50% reduction is meaningless without the baseline. Halving a risk from 2 in 1000 to 1 in 1000 is a 50% relative reduction and a 0.1 percentage-point absolute reduction — the same fact, opposite gut reactions. Families asked only for the relative figure systematically overestimate benefit and agree to low-value care, or refuse effective care out of proportionate fear. [1] [10]
Framing effects. The identical statistic framed positively ("9 in 10 survive") or negatively ("1 in 10 die") produces different choices. Balanced, bidirectional framing — stating both — protects the family from being steered. [3] [10]
Hidden uncertainty erodes trust. When a clinician offers a single precise prognosis to appear confident, and events diverge, the family remembers the gap. Naming uncertainty honestly, and giving a range, builds the trust that a precise-sounding wrong answer destroys. [4] [13]
Cognitive overload. Shock, fear and grief narrow working memory. Numbers poured into an unprepared mind are not retained, which is why small chunks, a warning, and teach-back matter more than completeness. [14]
Clinical Presentation
You will meet risk communication in several recognisable shapes. [3] [14]
The screening result. A newborn or prenatal screen returns a probability of a rare condition, with a residual risk of a false positive and a confirmatory test ahead. The family needs the chance, the uncertainty, and the next step in plain terms. [4]
The vaccine-safety question. A parent asks whether an immunisation is safe, clutching a relative-risk statistic they read online. The job is to correct the number without correcting the person, and to reframe absolute benefit against rare harm. [1]
The treatment trade-off. A family faces surgery against observation, or one medication against another, where benefits and harms compete. A drug-facts box or decision aid turns the comparison from a speech into a shared artefact. [5] [6]
The direct prognostic question. A parent — or an adolescent — asks plainly how the illness will unfold. This is where honest uncertainty, a range, and realistic hope must replace false precision. [4] [13]
The incidental finding of uncertain significance. Imaging or surveillance turns up something unexpected. Acknowledging that "we do not yet know what this means" is itself the communication, and it is better than a premature verdict. [4]
Differential Diagnosis
Name the true problem before you reach for another number. [1] [4]
| You see | Prefer this framing | Trap |
|---|---|---|
| Parent seems to "not get it" | Genuine low numeracy, anxiety, or both | Label them difficult and repeat the percentage louder |
| Parent demands a treatment the evidence does not support | Inflated relative-risk impression; reframe absolute benefit | Assume they are unreasonable |
| Parent refuses an effective, safe intervention | Fear driven by a framed statistic or misinformation | Dismiss the concern as irrational |
| Family "in denial" about prognosis | Anticipatory grief, or prior false-precise reassurance | Offer another precise number to break through |
| Young person silenced in the discussion | Emerging autonomy overlooked | Exclude them from their own risk |
Reasonable request versus health anxiety. Wanting more information is not pathology. A pattern of repeated reassurance-seeking and catastrophising, where numbers never settle the fear, points to health anxiety that needs its own care alongside honest communication. [2]
Cultural framing versus medical disagreement. A family may understand the numbers perfectly but weigh risk through cultural or spiritual meaning. Explore the framing before treating it as a knowledge gap. [14]
Clinical & Bedside Assessment
Assess before you number. What does the family already understand and believe about this risk? What have they read or been told? What is their sense of the stakes? These questions stop you over- or under-loading them and reveal where a correction is needed before any new figure lands. [14]
Assess numeracy and graph literacy, quietly. You do not need a test. Ask how they prefer information — words, numbers, or pictures — and watch how they handle the first number you offer. Default to pictographs when there is any doubt, because they help the numerate and the innumerate alike. [3] [11]
Map the decision. How reversible is it, how much time is there, and how high are the stakes? A preference-sensitive, high-stakes choice with time to deliberate calls for a decision aid; an urgent, irreversible one calls for crisp absolute numbers and a clear recommendation. [4] [7]
Assess language, culture and health literacy. Arrange a trained interpreter — never a child or family member — and a translated decision aid where one exists. Ask how the family usually makes health decisions and who should be in the room. [14]
Teach-back every number. Ask the family to restate, in their own words, the chance and the options. A nod is not understanding. Invite their framing: "What would you tell your partner about this when you get home?". [13]
Investigations
The "investigations" here are preparations, not blood tests. [1] [4]
Know the absolute numbers cold. Confirm the baseline risk, the absolute risk reduction, and the number needed to treat or harm before the conversation. If you only know the relative figure, you are not yet ready to counsel. [1] [10]
Know the certainty of the evidence. Is the figure from a randomised trial, a cohort, an expert estimate, or a single centre? Name the source quality honestly, because a family is entitled to know how firmly the number is grounded. [4]
Find or build a visual aid. A pictograph, a drug-facts box, or a validated decision aid turns the conversation from memory load into a shared artefact the family can take home. Where a region-endorsed aid exists, use it rather than improvising. [3] [6]
Document the conversation. Record the numbers shared, the format used, what the family understood on teach-back, and the decision reached. This is both a clinical and a medicolegal product. [14]
Management — Resuscitation
Some moments in these conversations are emergencies of a different kind. [1] [4]
Acute anxiety from a misunderstood statistic. A parent may panic over an inflated relative risk they read, or a screening result misheard as a diagnosis. Pause, normalise the fear, reframe the absolute number, and bring a pictograph before proceeding. [3]
Imminent decision on a wrong number. A family about to refuse effective care, or demand low-value care, on the basis of a framing error needs urgent correction of the absolute figures before the decision is made. Correct the number without correcting the person. [1] [10]
Coercion or safeguarding surfaced. A family member may override a capable young person, or a decision may be made under duress. Follow your safeguarding and consent pathways exactly as elsewhere. [14]
Clinician acute distress. A contested or emotionally charged risk conversation can shake a trainee. Offer immediate peer support and ensure a debrief. [14]
Management — Definitive & Stepwise
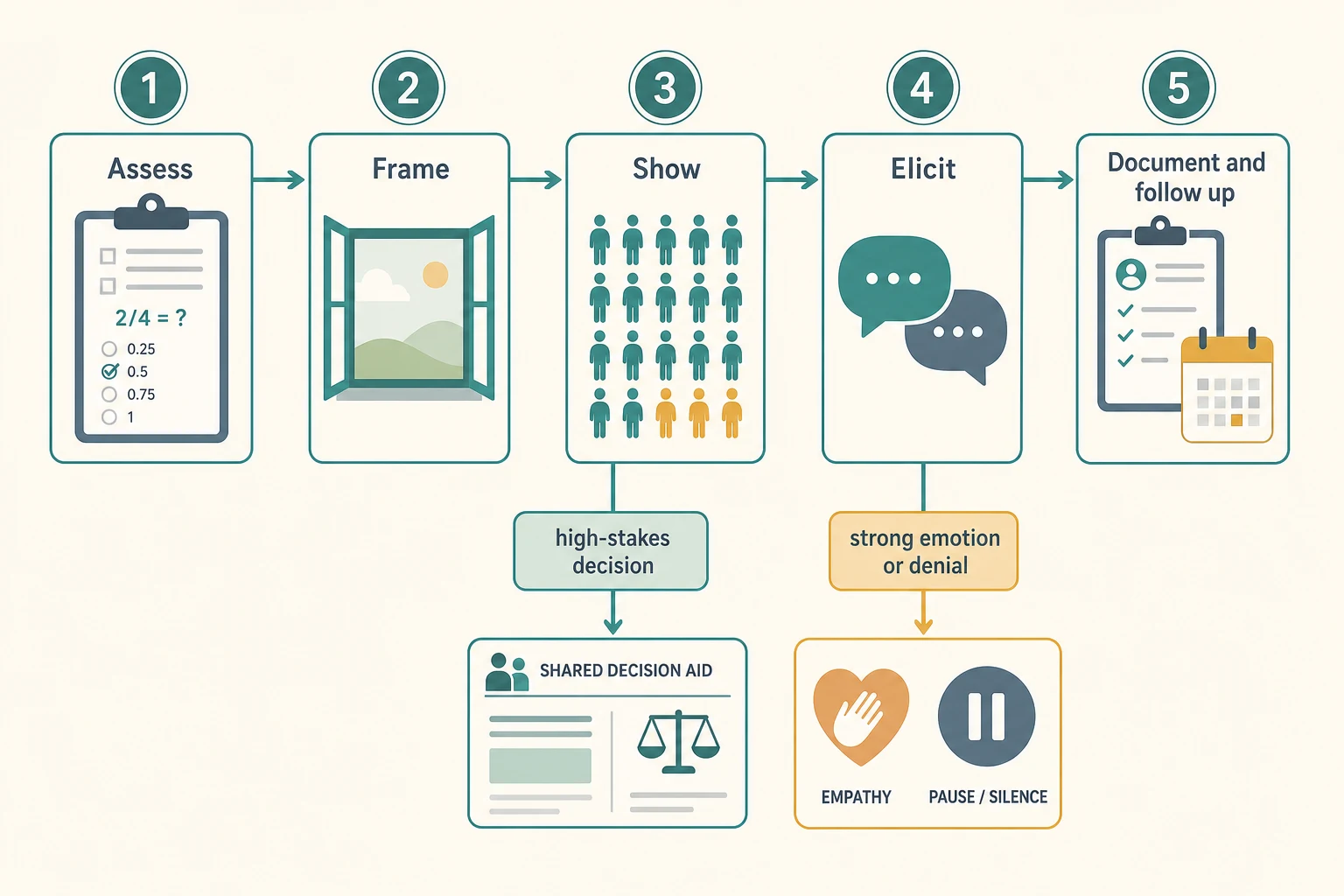
Work through five moves, in order. [3] [7]
- Assess. Establish what the family knows, believes, and wants, and gauge numeracy and language. Decide who should be present and whether an interpreter or decision aid is needed. [14]
- Frame. Choose the format: natural frequencies over percentages, absolute over relative risk, and a balanced bidirectional frame. State the baseline before any reduction. [1] [10]
- Show. Add a pictograph or icon array alongside the words, keeping one consistent denominator throughout. For medication, use a drug-facts box pairing benefit and harm. [3] [6]
- Elicit and acknowledge uncertainty. Use teach-back to confirm understanding, ask about values and preferred direction, and name epistemic uncertainty honestly with a range rather than false precision. [4] [13]
- Document and follow up. Record the numbers, format, understanding, and decision. Offer a written summary, a decision aid, and a named contact for the questions that arrive later. [14]
High-stakes, preference-sensitive decisions. Where the choice turns on values — surgery against observation, a screening boundary, a treatment with competing harms — move from a verbal explanation to a validated decision aid, and give the family time to deliberate. [5] [7]
What the evidence supports overall. A systematic review for the United States Preventive Services Task Force found that pictographs improve risk comprehension and reduce the overestimation that percentages and relative risk produce, while decision aids increase knowledge and involvement without raising anxiety. Natural-frequency formats improve Bayesian reasoning across lay and expert groups. [4] [8] [9]
Specific Subtypes & Scenarios
Newborn or prenatal screening result. Share the residual risk honestly: most positive screens are false positives, and confirmatory testing follows. Use natural frequencies and a pictograph to place the probability in context, and give a clear next step so the family is not left with the number alone. [4]
Vaccine benefit and rare harm. A hesitant parent often arrives with a relative-risk statistic. Reframe absolute benefit against rare adverse events using consistent denominators, acknowledge the genuine uncertainty, and avoid dismissing the concern. Pair this with the shared-decision-making and vaccine-hesitancy leaves. [1]
Medication benefits and harms. A drug-facts box presents benefit and harm side by side in absolute terms, and trials show it improves comprehension and accuracy of perceived effect. Use it for chronic-disease medications where families weigh long-term trade-offs. [5] [6]
Surgery versus medical management. Present competing benefits and harms in a balanced decision aid, give absolute numbers for both arms, and let values guide the choice rather than a framed statistic. [7]
Prognostic uncertainty in a life-limiting illness. Offer a range or trajectory rather than a single date, name what is and is not known, and move hope toward what is achievable — comfort, presence, meaning — without abandoning the family. Pair this with the breaking-bad-news leaf. [4] [13]
Incidental finding of uncertain significance. Say plainly that the meaning is not yet known, give a plan for surveillance or review, and resist premature reassurance or alarm. Acknowledged uncertainty here is safer than a confident wrong answer. [4]
Complications & Pitfalls
- Quoting relative risk without the absolute baseline, inflating perceived benefit or harm. [1]
- Switching denominators (10 of 1000 then 5 percent) so the comparison collapses. [8]
- Offering a single point estimate where genuine uncertainty exists. [4]
- Neglecting low numeracy and assuming a percentage was understood. [12]
- Framing only the upside of a treatment and omitting the harms. [10]
- Hiding uncertainty for fear of causing anxiety, which later breaks trust. [13]
- No teach-back, no documentation, and no follow-up after a high-stakes number. [14]
Prognosis & Disposition
A good risk conversation is measured by what the family can do afterwards, not by how smoothly it ran. [4] [14]
Markers of success. The family can restate the chance and the options in their own words. Benefits and harms are balanced and understood. Uncertainty is named, not hidden. A decision is reached that fits the family's values, with a written summary and a named contact for follow-up. [3] [13]
When to defer. If the family is acutely distressed, the numbers are not yet confirmed, or a decision aid is unavailable, it is legitimate to share the headline, support, and return for the full conversation. Deferral is a deliberate choice, not avoidance. [14]
When to escalate. Persistent values conflict, contested prognosis, or a request the evidence cannot support warrants ethics consultation, a second opinion, or specialist counselling. Use these early. [4]
Sustain the clinician. Repeated difficult risk conversations carry a cumulative weight. Build debrief and peer support into the routine so the skill endures across a career. [14]
Special Populations
Low health literacy or low numeracy. Default to pictographs and natural frequencies from the outset. These formats help the numerate and the innumerate alike, so they never patronise. [3] [12]
Culturally and linguistically diverse families. Always use a trained interpreter — never a child or family member — and seek a translated, culturally appropriate decision aid and a cultural broker where available. Ask how the family wishes risk to be discussed and with whom. [14]
Adolescents. Present risk to the young person developmentally, using simple concrete numbers and pictures, and respect assent and emerging autonomy. Avoid the dual failure of either excluding them or burdening them beyond their role. [14]
Families facing life-limiting prognosis. Pair honest uncertainty with realistic hope and palliative support. A range and a trajectory serve a family better than a single false-precise date. [4] [13]
Indigenous families. Use culturally safe, family- and community-centred communication on locally endorsed pathways, with trusted workers. Do not impose a generic numerical model. [14]
Evidence, Guidelines & Regional Differences
Core anchors are the Gigerenzer review of statistical literacy for doctors and patients, the Fagerlin agenda-setting paper on risk-communication research, Paling's strategies for helping patients understand risks, the Zipkin systematic review for the United States Preventive Services Task Force, the Woloshin and Schwartz drug-facts-box and benefit-harm trials, the Bonner best-practice principles for presenting probabilities in decision aids, the Hoffrage and Garcia-Retamero evidence on natural frequencies and visual aids, the Moxey work on describing treatment effects, the Galesic numeracy and graph-literacy surveys, the Peters guidance on numeric risk communication, and the Levetown AAP report on communicating with children and families. [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14]
The RACP and RCPCH-aligned communication and evidence-based-practice curricula frame training, and state-based newborn-screening programmes publish their residual-risk figures for parent information. Use local advance-care-planning and decision-support documents, and culturally safe pathways for Aboriginal and Torres Strait Islander and Māori whānau. Do not invent jurisdiction-specific thresholds; cite the local programme directly. [14]
NHS screening programmes publish easy-read and translated parent information with absolute residual risks, and the RCPCH Progress+ curriculum names communication and evidence-based practice as core professional skills. The IPDAS criteria inform the decision aids used in NHS settings. Use nationally endorsed patient-decision aids where they exist. [7] [14]
The United States Preventive Services Task Force systematic review underpins evidence-based risk communication, and the Schwartz and Woloshin drug-facts box has been adopted in consumer drug information. AAP guidance on communicating with children and families applies across screening and chronic disease. [1] [4] [14]
CanMEDS roles (Communicator, Collaborator, Scholar, Health Advocate) map directly onto counselling families about risk and uncertainty. Provincial screening programmes publish residual-risk figures and decision aids; use local documents and trained interpreters. [14]
Controversies: absolute versus relative framing as a default; whether to give a single point estimate or a range for prognosis; how much uncertainty to disclose directly to children and adolescents; and whether pictographs should accompany every numeric statement or only low-numeracy encounters. Exam answers show structured skill, honest uncertainty, and local humility. [1] [4] [13]
Exam Pearls
- Natural frequencies (5 in 100) beat percentages (5%) for nearly everyone. [1] [8]
- Always give the absolute baseline before any relative-risk statement. [1] [10]
- Add a pictograph or icon array; it helps the numerate and the innumerate. [3] [9]
- Keep one consistent denominator throughout; never switch mid-conversation. [8]
- Name uncertainty honestly; false precision erodes trust. [4] [13]
- Balance benefits and harms with bidirectional framing. [10]
- Teach-back every number; a nod is not understanding. [14]
- Document the numbers, the format, the understanding, and the decision. [14]
Present a number at the bedside
Assess what they know, their numeracy and their language
Frame with absolute numbers and the stated baseline
Show a pictograph with one consistent denominator
Give a range or name the uncertainty honestly
Teach-back the number and elicit values
Document the figures, understanding and decision; arrange follow-up
References
- [1]Gigerenzer G Helping Doctors and Patients Make Sense of Health Statistics. Psychological science in the public interest, 2007.PMID 26161749
- [2]Fagerlin A Making numbers matter: present and future research in risk communication. American journal of health behavior, 2007.PMID 17931136
- [3]Paling J Strategies to help patients understand risks. BMJ, 2003.PMID 14512489
- [4]Zipkin DA Evidence-based risk communication: a systematic review. Annals of internal medicine, 2014.PMID 25133362
- [5]Woloshin S Communicating data about the benefits and harms of treatment: a randomized trial. Annals of internal medicine, 2011.PMID 21768582
- [6]Schwartz LM Using a drug facts box to communicate drug benefits and harms: two randomized trials. Annals of internal medicine, 2009.PMID 19221371
- [7]Bonner C Current Best Practice for Presenting Probabilities in Patient Decision Aids: Fundamental Principles. Medical decision making, 2021.PMID 33660551
- [8]Hoffrage U Natural frequencies improve Bayesian reasoning in simple and complex inference tasks. Frontiers in psychology, 2015.PMID 26528197
- [9]Garcia-Retamero R Visual aids improve diagnostic inferences and metacognitive judgment calibration. Frontiers in psychology, 2015.PMID 26236247
- [10]Moxey A Describing treatment effects to patients. Journal of general internal medicine, 2003.PMID 14687282
- [11]Galesic M Graph literacy: a cross-cultural comparison. Medical decision making, 2011.PMID 20671213
- [12]Galesic M Statistical numeracy for health: a cross-cultural comparison with probabilistic national samples. Archives of internal medicine, 2010.PMID 20212183
- [13]Peters E Communicating Numeric Risk Information to Patients. Journal of general internal medicine, 2025.PMID 40301218
- [14]Levetown M Communicating with children and families: from everyday interactions to skill in conveying distressing information. Pediatrics, 2008.PMID 18450887