Paeds · professional-practice-and-evidence
Confidentiality with children and adolescents
Also known as Adolescent confidentiality · Conditional confidentiality paediatrics · Mature minor doctrine · Gillick competence confidentiality · Fraser guidelines contraception · Information sharing in child health · Privacy and the young patient
Fellowship-level approach to confidentiality with children and adolescents: conditional confidentiality, Gillick/Fraser competence and the mature-minor doctrine, the three narrow overrides (serious harm, abuse, legal duty), parental requests for information, electronic-record and billing breaches, safeguarding overrides and regional frameworks across ANZ, UK and North America.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A 15-year-old sits opposite you and asks, "If I tell you something, will you tell my parents?" The answer you give in that moment is the whole topic. Get it right and the young person talks; get it wrong and they go quiet, then go elsewhere. Confidentiality is the duty to protect personal health information shared within the clinical relationship, and for an adolescent it is also a developmental claim on their own privacy. [1] [2]
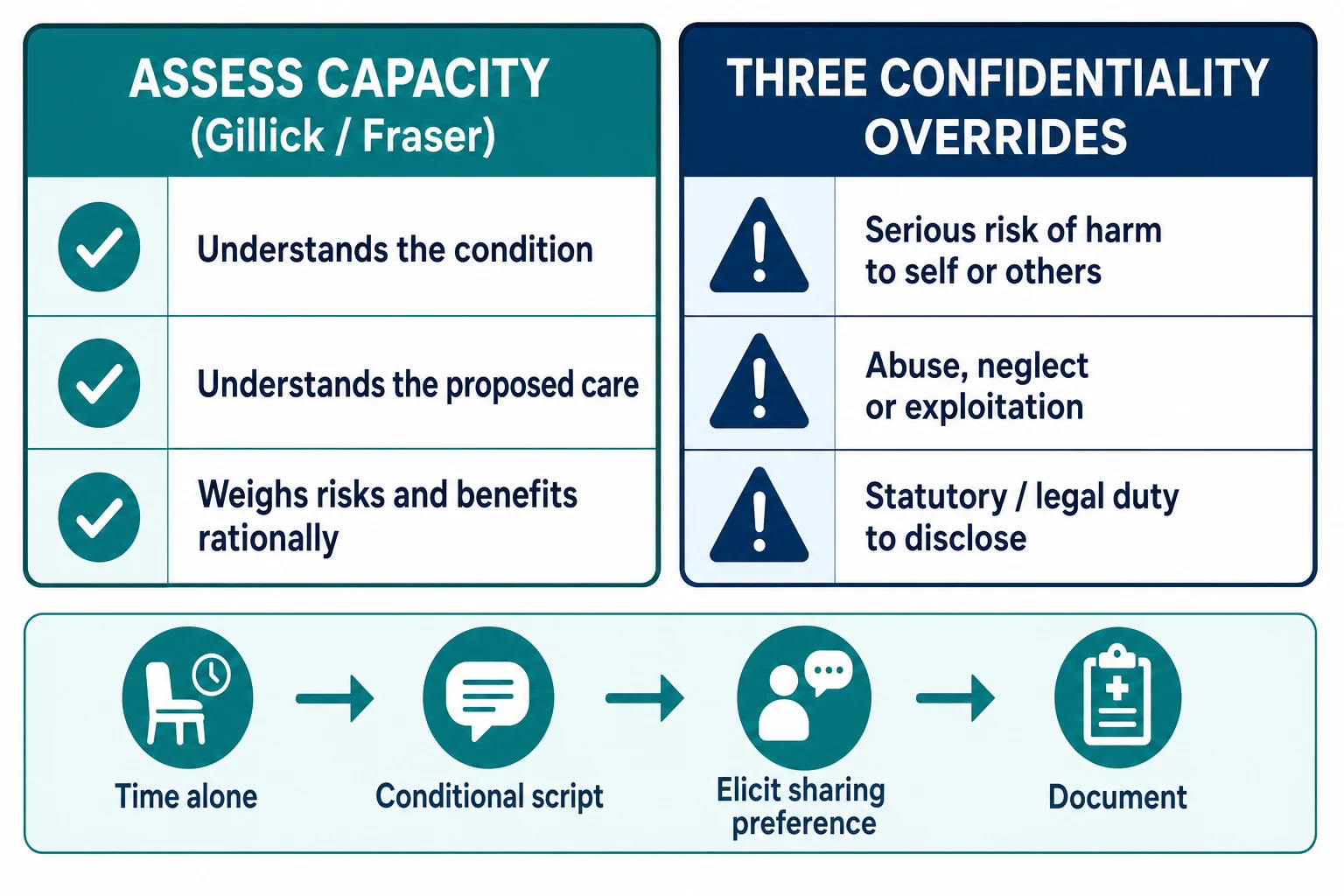
Confidentiality is not secrecy. The clinical relationship cannot run on a promise that nothing will ever leave the room, because some disclosures must be acted on. What you offer instead is conditional confidentiality: private unless there is serious risk of harm to the young person or others, abuse or neglect, or a legal duty to act. The conditional framing is the safeguard that lets you keep the promise you actually make. [6] [8]
Two legal tools sit underneath the practice. Capacity decides whether the young person can consent to care and control their own information — assessed by the Gillick or Fraser test in the UK and by the mature-minor doctrine in common-law Australasia. The override threshold decides when the duty to protect outranks the duty to keep confidence. Your job is to hold both, for every young person, every visit. [9] [10]
Classification
Sort the work along two axes that must be held together. [6]
Capacity axis. Is the young person competent to understand the condition, the proposed care, and its risks, and to weigh them rationally? If yes, they consent and they control their information. If no, a parent or guardian decides and you seek assent. Capacity is decision-specific and fluctuates with illness, fear and development. [9] [13]
Override axis. Which disclosures must leave the room against the young person's wishes? Three categories justify an override: serious risk of harm to self or others; abuse, neglect or exploitation; and a statutory or legal duty to report. Everything else stays private. [1] [6]
Capacity and override side by side
Epidemiology & Risk Factors
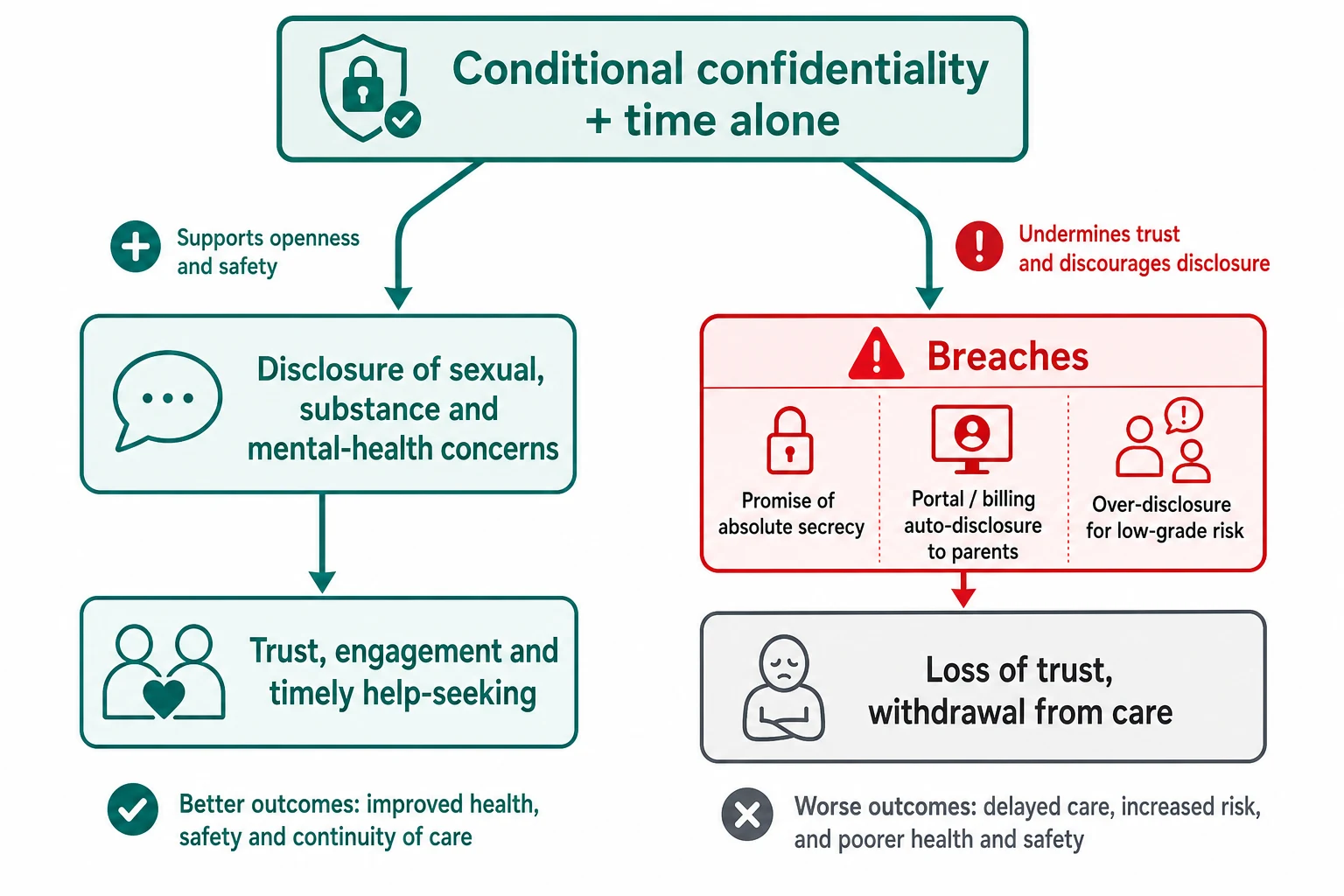
Confidentiality is not an abstract nicety; it changes behaviour. Adolescents who are assured of private, confidential care are more willing to disclose sexual activity, substance use and mental-health concerns, and more willing to seek the care those disclosures trigger. When the assurance is absent, disclosure falls and the young person may avoid the clinic altogether. [2] [6]
Time alone with the clinician is the practical hinge. Parents often accept it once it is framed as standard developmental care rather than suspicion, and adolescents disclose far more when a parent is not in the room. Yet time alone is still offered inconsistently, which is why it is treated as a measurable quality step. [3]
Modern breaches come through infrastructure, not conversation. Electronic health records, patient portals, billing statements and insurance explanation-of-benefits notices can all surface a contraception, mental-health or sexual-health encounter to a parent who opens the mail or the app. In the United States the 21st Century Cures Act opened notes to patients by default, which is good for autonomy and dangerous for adolescent confidentiality unless sensitive-note workflows are configured. [4] [7]
Pathophysiology
There is no enzyme for trust, but there is a mechanism. When a young person believes the clinician will keep confidence within the stated limits, they disclose more honestly, engage with the plan and return when they are in trouble. Disclosure drives accurate diagnosis, and accurate diagnosis drives the right care. [2] [6]
The mechanism runs in reverse just as cleanly. A promise of absolute secrecy collapses trust the moment an inevitable override arrives and the young person learns the clinician lied. A portal that leaks a mental-health visit to a parent does the same damage silently. Over-disclosure for low-grade risk — telling parents about occasional vaping, say, with no defensible threshold — teaches the young person that nothing is safe to share. [4] [1]
The public-health argument completes the loop. A population of adolescents who trust the system seeks preventive and mental-health care earlier; a population that does not, presents later and sicker. Confidentiality is therefore a clinical intervention with measurable downstream effects, not a courtesy. [1] [8]
Clinical Presentation
Confidentiality questions present in the room long before they present on an ethics form. A young person asks, "Will you tell my parents?" A parent demands full access to portal notes or test results. A disclosure arrives prefaced by, "Please don't tell anyone." Each is a live test of how you handle information. [1] [5]
The highest-stakes presentation is the safety disclosure delivered with a plea for secrecy: suicidality, self-harm, abuse, pregnancy, sexual exploitation or dangerous substance use. The young person is handing you information they have told no one else, and they are watching to see whether you betray them. Your handling in the next five minutes sets the trajectory. [6] [8]
System-level presentations are quieter but common. A billing statement reveals a sexual-health visit. A portal notification flags a mental-health result. A school nurse, a police officer or a lawyer asks for information about a child. Each requires a deliberate decision about what may be shared, not a reflexive yes. [4] [7]
Differential Diagnosis
Not every confidentiality question is what it first appears. Separate the genuine capacity issue from the parental over-reach, the safeguarding disclosure from the routine sensitive disclosure. [6] [9]
| Surface story | Confidentiality reading | Must-not-miss alternative |
|---|---|---|
| Parent wants the 16-year-old's full record | Assess capacity; the competent young person controls access | Safeguarding concern driving the request — handle separately |
| "Please don't tell anyone — I want to die" | Safety override is in play; secure the young person first | Ambivalent statement mistaken for settled intent — assess properly |
| Occasional vaping, teen begs secrecy | Keep private; no override threshold met | Escalating dependence with harm — raise the threshold conversation |
| Portal showed the contraception note | Structural breach; repair workflow and support the young person | Parent using access to coerce — safeguarding review |
| Court order or police request | Disclose only what the order or statute requires | Fishing expedition with no lawful basis — decline |
Safeguarding is the override that most often hides under a softer label. A disclosure of abuse or serious self-harm must be acted on even when the young person begs secrecy. The skill is to act on the override while keeping the young person with you, not against you. [1] [9]
Clinical & Bedside Assessment
Start with capacity. Does this young person understand the condition, the proposed investigation or treatment, the alternatives, and the risks of each? Can they weigh that information and hold it in mind long enough to decide? Gillick and Fraser frame the UK test; the mature-minor doctrine does the same work across Australasia and much of North America. The test is decision-specific: competent for the contraceptive pill today does not mean competent to refuse insulin tomorrow. [9] [13]
Then secure time alone. Frame it as standard, not suspicious: "Part of every visit at this age is a few minutes on your own — it's how we look after teenagers." Parents usually accept this when it is normalised, and the disclosure that follows justifies the arrangement. [3] [5]
Deliver the conditional script explicitly. Name the limits before you ask the sensitive questions, not after. A workable script: "What we talk about is private — between us — unless I'm worried you're at serious risk of being hurt, of hurting yourself, or of hurting someone else, or unless the law requires me to share something. If I ever do need to share, I'll tell you first and we'll plan it together." [2] [1]
Finally, ask what the young person wants shared and what they want kept private, and write that down. The sharing preference is clinical data. [5] [12]
SCRIPT
Investigations
There is no blood test for confidentiality. The investigation is structured assessment and documentation, and it is what an examiner or a coroner will read later. [9] [12]
Record the capacity assessment and its reasoning, not just the conclusion. Document the conditional-confidentiality discussion, including that the limits were stated. Write down the young person's expressed sharing preference. If an override occurred, record the clinical and legal basis, what was shared, with whom, and how the young person was informed. [1] [6]
Check the infrastructure before it betrays you. Know which portal and billing configurations your service uses for sensitive encounters, and confirm that mental-health, sexual-health and substance-use results route to the right recipient. In the United States, understand your state's minor-consent and privacy statutes and how the local electronic record handles adolescent confidentiality, because variability between states is substantial. [4] [7]
Management — Resuscitation
In a safety crisis — active suicidal intent, disclosure of abuse, a young person in immediate danger — the override is not a debate. Secure the young person first. Share the minimum necessary with the people who must act: the parent or carer where they are part of the safety plan, the mental-health crisis team, or child protection. [1] [8]
Never buy a disclosure with a lie. If you have already promised absolute secrecy and a crisis now forces an override, tell the young person directly what has changed and why, involve them in planning the disclosure where it is safe to do so, and keep the relationship open. The damage from a silent override is worse than the damage from an honest one. [6] [9]
In the resuscitation phase share only what each recipient needs to act. The crisis team needs the risk picture; the parent needs the safety plan; child protection needs the safeguarding facts. You do not hand over the whole sexual or substance history to everyone in the room. [1] [12]
Management — Definitive & Stepwise
Use a sequence you can defend in a viva and reproduce at the bedside. The steps hold for a routine visit and for a crisis; what changes is the threshold question and the urgency. [1] [6]
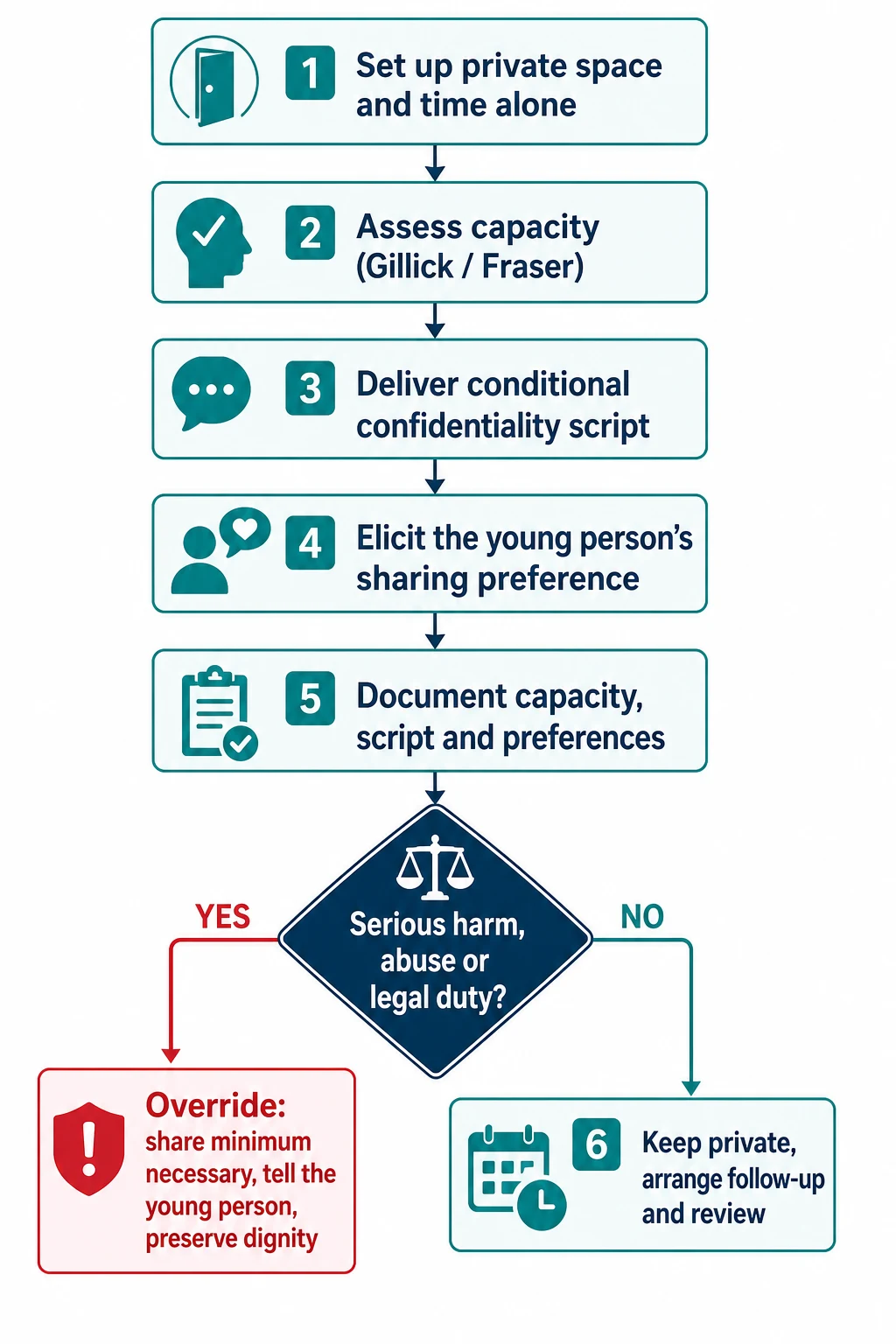
Confidentiality management algorithm
Set up: private space and time alone with the young person
Assess capacity: Gillick or Fraser, decision-specific
Deliver the conditional-confidentiality script and invite questions
Elicit and record the young person's sharing preference
Decide: is there serious harm, abuse, or a legal duty?
If yes — override: share minimum necessary, tell the young person, document the basis
If no — keep private, arrange follow-up and review the preference
Managing parental requests. A parent who asks for a competent adolescent's information is owed an honest answer, not the record. Explain that the young person has a right to confidentiality, offer to facilitate a shared conversation with the young person's agreement, and avoid simply handing over notes against the young person's wishes. Most parents accept a rights-based explanation when it is delivered respectfully. [5] [11]
Protecting the infrastructure. Configure electronic records, portals and billing so that sensitive encounters do not auto-disclose. Use local sensitive-note or confidential-encounter flags. If your service cannot prevent a portal leak, arrange an alternative channel for sensitive results and tell the young person how it works. [4] [7]
After an override. Tell the young person what was shared, with whom and why. Arrange follow-up to repair the relationship. Document the reasoning so that the next clinician understands the decision. Escalate to ethics, legal services or child protection when the override threshold is genuinely uncertain. [1] [6]
Specific Subtypes & Scenarios
The routine preventive visit. A parent attends and answers every question. Normalise time alone, deliver the conditional script, and run the sensitive history in private. This is the scenario examiners reach for first. [3] [5]
The safety disclosure with a secrecy plea. Suicidality, self-harm, abuse or exploitation disclosed with "please don't tell anyone." Assess risk fully, override only to the threshold, share the minimum necessary, and keep the young person engaged. [1] [8]
The portal or billing breach. A parent has seen a contraception or mental-health note. Acknowledge the structural problem, support the young person, repair the workflow, and consider whether the breach itself raises a safeguarding concern. [4] [7]
The hospitalised adolescent. Ward handover, multiple teams and shared whiteboards all threaten privacy. Agree a tailored information-sharing plan on admission so the right people know what they need and nothing more. [12]
Out-of-home care and youth justice. Several agencies and carers may have legitimate claims on information. Clarify who holds parental responsibility, what each agency needs, and what the young person wants controlled. Default-to-everyone is a breach in this setting. [14] [11]
The court order or third-party request. Disclose only what the order or statute lawfully requires. A request is not a command; confirm the legal basis before releasing anything. [14] [6]
Complications & Pitfalls
- Promising absolute secrecy, then being forced to override — trust collapses. [2] [6]
- Over-riding for low-grade risk with no defensible threshold — the young person learns nothing is safe. [1]
- Portal or billing auto-disclosure of sensitive care to a parent — a common, preventable structural breach. [4]
- Treating all minors as lacking capacity, so every result defaults to the parent by rule. [9] [13]
- Performing an override silently, so the young person never learns what was shared. [6]
- Confusing a parental demand for information with a right to receive it. [5] [11]
- Documenting the conclusion ("competent") without the reasoning the examiner or coroner will need. [9]
Prognosis & Disposition
Confidentiality respected predicts engagement. Young people who trust that their information is handled well disclose more, return sooner and adhere better to plans they helped shape. The relationship usually survives an override when the clinician was transparent, shared the minimum necessary and preserved dignity. [2] [6]
Disposition is explicit, not implied. Name the follow-up, write the plan in language the young person understands, and record exactly what was agreed to be shared with parents and what was kept private. When risk is high or the override decision is uncertain, escalate to mental-health crisis services, child protection, an ethics committee or legal services rather than carrying the weight alone. [1] [8]
The long view matters. Each confidentiality decision teaches the young person whether the health system is a place they can use. A population that trusts the system presents earlier and less severely; a population that does not presents late. [1] [8]
Special Populations
Younger children. Confidentiality is not only for teenagers. A school-age child has age-appropriate expectations of privacy, and the involvement of parents is graded by capacity and best interests rather than assumed. Explain to the child what you will do, and share with parents what the child needs them to know. [14] [9]
Sexual- and gender-diverse youth. Confidentiality can be life-critical. A disclosure of identity or orientation to an unsupportive family is itself a harm; protect the information and connect the young person to appropriate support. [1] [8]
Out-of-home care and youth justice. Multiple carers and agencies seek information. Clarify parental responsibility and legal sharing obligations, hear the young person's wishes, and avoid default-to-all. [14]
Migrant, refugee and asylum-seeking families. Language, culture and immigration status intersect with privacy. Use trained interpreters, be aware that disclosure may carry particular risks for undocumented families, and share only on a lawful basis. [11]
Children with disability and neurodiversity. Capacity is decision-specific and must be assessed, not assumed from diagnosis or age. Support the young person to participate to the maximum of their ability, and involve parents in line with capacity and best interests. [9] [13]
Evidence, Guidelines & Regional Differences
Practice anchors the examiner expects you to know. The AAP policy statement on confidentiality in the care of adolescents sets the North American standard, and ACOG Committee Opinion 803 aligns with it for reproductive care. Ford's foundational work on delivering confidentiality assurances and Miller's on time alone as quality of care underpin the behaviour-change evidence. Berlan and Bravender integrate confidentiality with consent in adolescent practice. [1] [2] [3] [6] [8]
The capacity framework rests on Gillick competence and the Fraser guidelines. Larcher and Hutchinson describe how paediatricians should assess competence in practice, and Wheeler argues for consistency between the Gillick and Fraser labels. The mature-minor doctrine carries the equivalent logic across Australasia and common-law North America. [9] [10] [13]
The infrastructure controversy is live. The 21st Century Cures Act opened notes to patients by default in the United States, which advances autonomy but threatens adolescent confidentiality unless sensitive-note workflows are configured. Sharko and colleagues document substantial state-by-state variability in adolescent privacy law, so the same clinical note may be protected in one jurisdiction and exposed in another. [4] [7]
Controversies you must handle calmly in viva: where exactly the "serious harm" threshold sits; how to reconcile parental demands with the competent young person's autonomy; how to operationalise confidential notes inside an open-records regime; and whether the duty to protect a third party ever outranks the duty to the young person. There is no formula for these — name the principle, the threshold and the safety net. [1] [6]
Australia and Aotearoa New Zealand apply the common-law mature-minor doctrine: a young person who is competent to understand the treatment and its consequences may consent on their own, and their information is protected under the Australian Privacy Principles or the New Zealand Health Information Privacy Code 2020. Mandatory reporting of child abuse overrides confidentiality in both countries. Frame the conditional script in plain language, and know your local mandatory-reporting statute. [11] [14]
Exam Pearls
LIMITS
References
- [1]Chung RJ, Lee JB, Alderman EM, et al Confidentiality in the Care of Adolescents: Policy Statement. Pediatrics, 2024.PMID 38646690
- [2]Ford CA, Millstein SG Delivery of confidentiality assurances to adolescents by primary care physicians. Archives of pediatrics & adolescent medicine, 1997.PMID 9158445
- [3]Miller VA, Friedrich E, Orzech N Adolescents Spending Time Alone With Pediatricians During Routine Visits: Perspectives of Parents in a Primary Care Clinic. The Journal of adolescent health, 2018.PMID 29887486
- [4]Pasternak RH, Alderman EM, Rosen DS, et al 21st Century Cures Act ONC Rule: Implications for Adolescent Care and Confidentiality Protections. Pediatrics, 2023.PMID 37010402
- [5]McKay EA, Brar P, Diaz M, et al Parents' Perspectives on Confidentiality in Clinical Preventive Services for Adolescents. The Journal of adolescent health, 2025.PMID 40580168
- [6]Berlan ED, Bravender T Confidentiality, consent, and caring for the adolescent patient. Current opinion in pediatrics, 2009.PMID 19474734
- [7]Sharko M, Jameson R, Anoshiravani A, Wilkes MS State-by-State Variability in Adolescent Privacy Laws. Pediatrics, 2022.PMID 35531640
- [8]American College of Obstetricians and Gynecologists Confidentiality in Adolescent Health Care: ACOG Committee Opinion, Number 803. Obstetrics and gynecology, 2020.PMID 32217979
- [9]Larcher V, Hutchinson A How should paediatricians assess Gillick competence? Archives of disease in childhood, 2010.PMID 19948515
- [10]Wheeler R Gillick or Fraser? A plea for consistency over competence in children. BMJ, 2006.PMID 16601020
- [11]Bird S Adolescents and confidentiality. Australian family physician, 2007.PMID 17676192
- [12]Breuner CC, Alderman EM, Grubb TK, et al The Hospitalized Adolescent. Pediatrics, 2023.PMID 36995186
- [13]Silber TJ Adolescent brain development and the mature minor doctrine. Adolescent medicine: state of the art reviews, 2011.PMID 22106735
- [14]Royal Australasian College of Physicians Privacy in paediatrics. Journal of paediatrics and child health, 2016.PMID 27124837