Paeds · professional-practice-and-evidence
Conflict, complaints and difficult clinical encounters
Also known as Difficult consultations in paediatrics · De-escalating the angry parent · Goals-of-care and treatment conflict · Managing patient and family complaints · Second victim and clinician welfare after complaint
Fellowship guide to difficult clinical encounters, conflict and complaints in paediatrics: recognising the difficult consultation and its clinician and system drivers; structured verbal de-escalation of the angry or aggressive parent; managing goals-of-care and treatment disputes with ethics consultation and mediation; responding to formal complaints with service recovery and learning; the second-victim phenomenon and clinician welfare; and ANZ/UK/US/Canada complaint systems and apology-law differences.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
De-escalate the angry parent — VERBAL in the room
Overview & Definition
A father corners you on the ward. His daughter's scan result, promised yesterday, is still not back, and he is shouting. Your pulse rises, you feel defensive, and every sentence you offer seems to make it worse. That is a difficult encounter, and it is one of the commonest tests of professionalism in paediatrics. [3] [4]
Three overlapping problems meet in this territory, and naming which one you are in changes what you do. A difficult encounter is any consultation in which the clinician feels ineffective, frustrated or stuck; the feeling is the diagnostic feature, and it usually reflects a mismatch of agenda or expectations rather than the child's illness. Conflict is a live disagreement over a decision — what to do next, whether a treatment is worthwhile, who is right. A complaint is a formal expression of dissatisfaction with care, made through a defined route with timeframes and a paper trail. [1] [2]
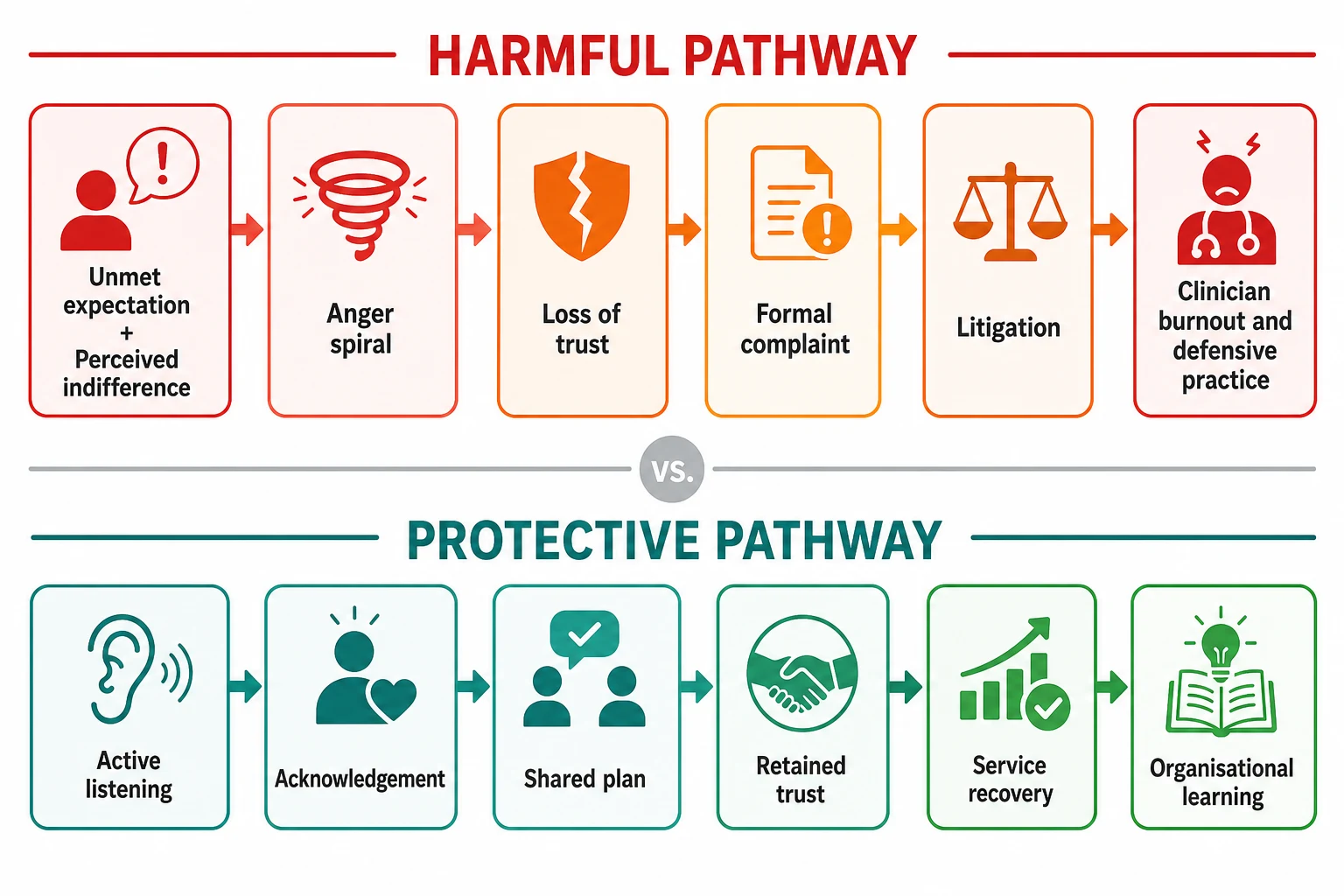
A difficult encounter that is handled badly becomes conflict; conflict that is handled badly becomes a complaint; and a complaint that is handled badly becomes litigation, attrition and clinician burnout. Good management works upstream — calm the encounter early, and most conflict and complaint never form. [1] [11]
This page owns the process and skills. Cross-link the dedicated leaves for consent and mature-minor frameworks, shared decision-making and assent, breaking bad news, open disclosure and duty of candour, best-interests decisions and treatment limitation, trauma-informed care and working with interpreters. Do not rebuild their content here. [6] [7]
Classification
Sort the work by the shape the problem takes when it reaches you, because each shape has a different first move. [3] [5]
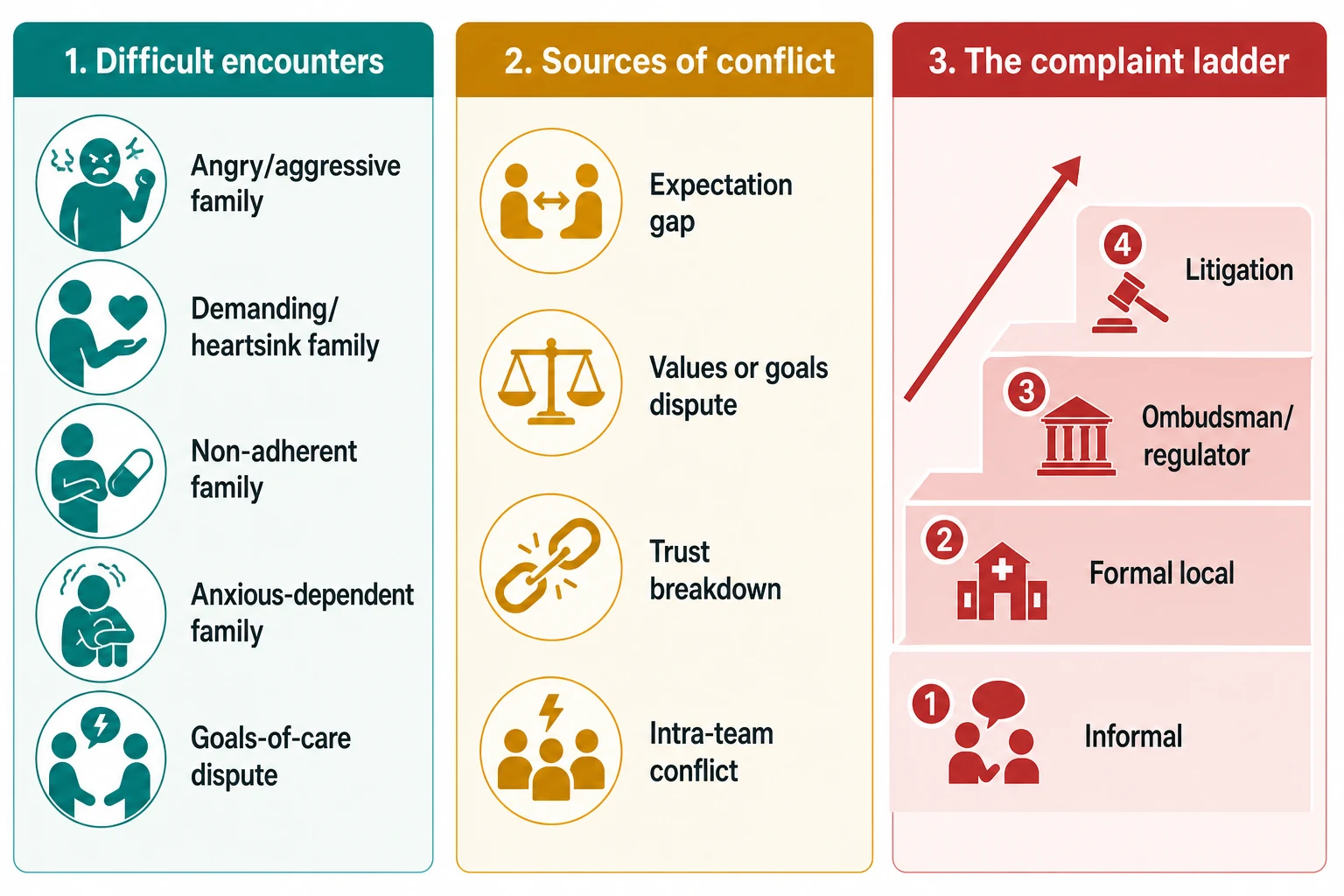
Difficult-encounter phenotypes. The angry or aggressive family, where the emotion has overtaken the content. The "heartsink" or demanding family, who generate a wave of dread before they even sit down, with endless lists and requests. The non-adherent or disengaged family, who miss appointments or do not give the medication. The anxious-dependent family, who need constant reassurance and never feel heard. And the family in goals-of-care or treatment dispute, where you and they want different things for the child. [3] [4]
Sources of conflict. An information or expectation gap ("no one told me it would be like this"). A values conflict, where what the family most wants is not what the team most recommends. A goals-of-care or futility dispute, especially in neonatal and paediatric intensive care. A trust breakdown, often after a delay, an error or a perceived slight. And intra-team or inter-agency conflict, where the family is caught between clinicians giving different messages. [6] [7]
The complaint ladder. Informal, ward-level dissatisfaction; a formal local complaint to the hospital or practice; escalation to an external ombudsman or health regulator; and finally litigation. Each rung has a longer paper trail and a higher cost, which is why early, in-room resolution matters. [1] [2]
Epidemiology & Risk Factors
Difficult encounters are common, not rare. Across paediatric wards, outpatient clinics and emergency departments, most clinicians meet them weekly. They cluster around three predictors: a mismatch between what the family expected and what happened, a communication failure (delayed results, vague plans, perceived indifference), and a family already carrying fear, grief or fatigue. [1] [3]
Complaints carry real downstream weight. In a landmark study, physicians with the most patient complaints carried the highest malpractice risk — complaints are an early warning signal of the communication and relationship problems that later drive litigation. [1] Complaints are also a safety dataset: aggregated and triangulated with incident reports, they expose problems that no single reporting system catches. [2]
Clinician factors raise the chance of any encounter turning difficult. Fatigue, heavy workload, inexperience, and a clinician's own stress lower the threshold for frustration. Language and cultural barriers, prior adverse experience, and untreated parental mental illness all tilt an ordinary visit toward a hard one. Naming these upstream factors is part of the management, because a family labelled "difficult" without examining the system is misdiagnosed. [3] [11]
Pathophysiology
Think about the mechanisms that turn a frustrated parent into a complaint, and about what interrupts the chain. [5] [9]
The anger arousal cycle. Anger is fuelled by perceived threat, injustice or indifference, and it rises in a cycle that confrontation prolongs. When you justify, argue or match a parent's tone, you confirm the threat and the cycle climbs. When you acknowledge the feeling and listen, you interrupt it, and the arousal begins to fall. This is why de-escalation feels counter-intuitive: the move that lowers the temperature is the opposite of defending yourself. [5]
Unmet expectation to complaint cascade. Most complaints begin with an unmet expectation — a result that did not come, a plan that was not explained, a pain that was not relieved — read as indifference. The family loses trust, the relationship sours, and the family turns to a formal route. Early acknowledgement and service recovery (a sincere apology and a fix) can abort this cascade even after a genuine shortcoming. [1] [13]
The "difficult" label is a system finding. A family feels difficult when the clinician's and family's agendas are misaligned, when the system has failed them, or when the clinician is depleted. The label tells you more about the consultation than about the family. Re-label it as a problem to solve and the encounter often unlocks. [3] [4]
The second-victim trajectory. When a clinician is involved in an adverse event or a hostile complaint, they follow a recognisable recovery path: chaos and shock, intrusive reflections, then either supported recovery or — if unsupported — anxiety, depression, defensive practice and attrition. Unsupported clinicians leave, or they stay and practise defensively, ordering more and listening less. Looking after the clinician is therefore part of looking after the next patient. [8] [9] [10]
Clinical Presentation
You will meet this territory in several recognisable shapes. [3] [5]
The angry parent at the bedside or in clinic. Volume is up, pace is fast, and the content is a grievance — a delay, a result, a decision. Your job is to lower the temperature before you defend the content. [5]
The entrenched treatment or goals-of-care dispute. Parents want a treatment the team judges non-beneficial, or refuse care the team recommends, often in neonatal or paediatric intensive care. The stakes are existential and the room is full of grief. [6] [7]
The non-adherent or disengaged family. Repeatedly missed appointments, medication not given, clinic non-attendance. The instinct is to label them non-compliant; the work is to find the barrier — cost, understanding, chaos, fear or a genuine values choice. [3]
The demanding or "heartsink" family. Every visit lands with a thud. Endless lists, multiple unmet requests, a sense that nothing is ever enough. The strong negative emotion in you is data about the relationship, not a verdict on the family. [3] [4]
The family who has already complained, or threatens to. The encounter is now also a documentary one — what you say and write will be read again. Stay calm, stay factual, and respond through the proper channel. [1] [11]
The threatening or aggressive family member. This is a safety problem first. If there is any threat, weapon or intoxication, you stop trying to de-escalate and you summon security. [5]
Differential Diagnosis
Before you reach for a script, name what is actually driving the encounter, because each driver has a different remedy. [3] [6]
| You see | More likely | The trap |
|---|---|---|
| Sudden anger at a result or delay | Unmet expectation, fear, a genuine service failure | Defending instead of acknowledging |
| Demand for non-beneficial treatment | A values or goals conflict, inadequate prior prognostic discussion | Calling it "futile" and withdrawing abruptly |
| Refusal of agreed care | Misunderstanding, cost barrier, or a genuine values choice | Labelling it non-compliance |
| Dread before every visit | Heartsink pattern, clinician burnout magnifying the ordinary | Blaming the family alone |
| Hostility with intoxication or threat | Safety risk | Attempting de-escalation in an unsafe situation |
Anger driven by fear or grief, not personality. Most parental anger in paediatrics is fear, grief or guilt wearing an angry face. Treat the fear and the anger falls. A smaller share is driven by personality, intoxication or coercive control — and that share is where safety, not empathy, leads. [5] [7]
Goals conflict versus misunderstanding. Families who demand treatment the team judges futile are usually asking for hope and time, not for a specific drug. The remedy is a goals-of-care conversation, not a definition of futility. [6] [7]
Clinical & Bedside Assessment
Assess before you respond. The first assessment is always safety, then the driver, then yourself. [5]
Assess safety first. Is there a threat, a weapon, intoxication, or risk to the child, to staff or to you? If yes, withdraw to a safe distance and call security or your local code-grey equivalent. De-escalation is for the agitated-but-not-dangerous; it fails, dangerously, against an active threat. [5]
Assess wants and feelings. Ask openly — "Help me understand what has happened, and what you most need from us today." Most angry families calm measurably once they believe they are being heard, because being heard is often exactly what they wanted. [3] [5]
Assess the underlying driver. Is this an unmet expectation, a service failure, fear, grief, guilt or misinformation? Each points to a different fix: a result, an apology, a plan, a correction. [1] [2]
Read the child and safeguarding. Where is the child in the room, and is hostile adult behaviour placing them at risk? A difficult encounter can surface domestic violence, neglect or coercion, and you follow your safeguarding pathway exactly as you would anywhere else. [7]
Assess your own state. Notice your pulse, your urge to argue, your wish to escape, your counter-transference. These are signals that shape your next sentence. A clinician who recognises being triggered can choose a different response; one who does not will simply react. [3] [11]
Investigations
The "investigations" here are preparations and fact-finding, not blood tests. [1] [2]
Review the timeline and the facts. Before you respond to a grievance, reconstruct what actually happened — the result, the delay, the conversation. Identify any genuine service failure honestly; a defensible response begins with the truth. [1]
Gather collateral and align the team. What did nursing hear overnight? What did a colleague already say? What does the record show? Never contradict a colleague in front of the family; align the team first so the family hears one message. [6] [10]
Check for an open complaint or incident. Is there already a formal complaint, an incident report, or an open-disclosure obligation? If a complaint discloses genuine harm, the clinical stabilisation and the duty of candour lead, and the complaints response follows. [2]
Document factually and contemporaneously. Write what was said, what was offered and what was agreed, in the notes, at the time. Do not editorialise, do not apportion blame in writing, and never alter a record after a complaint — addenda only. [11] [12]
Management — Resuscitation
Some moments in this territory are emergencies of safety, and safety outranks every other consideration. [5] [8]
Active threat to a person. If there is a weapon, imminent violence or dangerous intoxication, do not attempt de-escalation. Withdraw, keep an exit behind you, move other patients and staff away, and call security or police. Your safety and the child's come first. [5]
Risk of harm to the child. A hostile encounter can reveal or constitute child abuse, coercive control or neglect. Follow your mandatory safeguarding pathway: separate the child if needed, escalate to the safeguarding team, and document. [7]
Clinician at risk of harm or in acute distress. A registrar shouted at or grabbed, or one who breaks down after a hostile encounter, needs immediate removal from the situation and support. Debrief, peer contact and occupational-health or employee-assistance referral are the first aid. [8] [9]
Complaint that discloses genuine harm. Stabilise the child first. Then begin open disclosure — an honest, timely explanation of what happened, the consequences and the response — owned on its dedicated leaf but inseparable from the complaints pathway. [2] [10]
Management — Definitive & Stepwise
Match the move to the shape of the problem. The same opening — ensure safety, then listen — serves all of them. [5] [1]
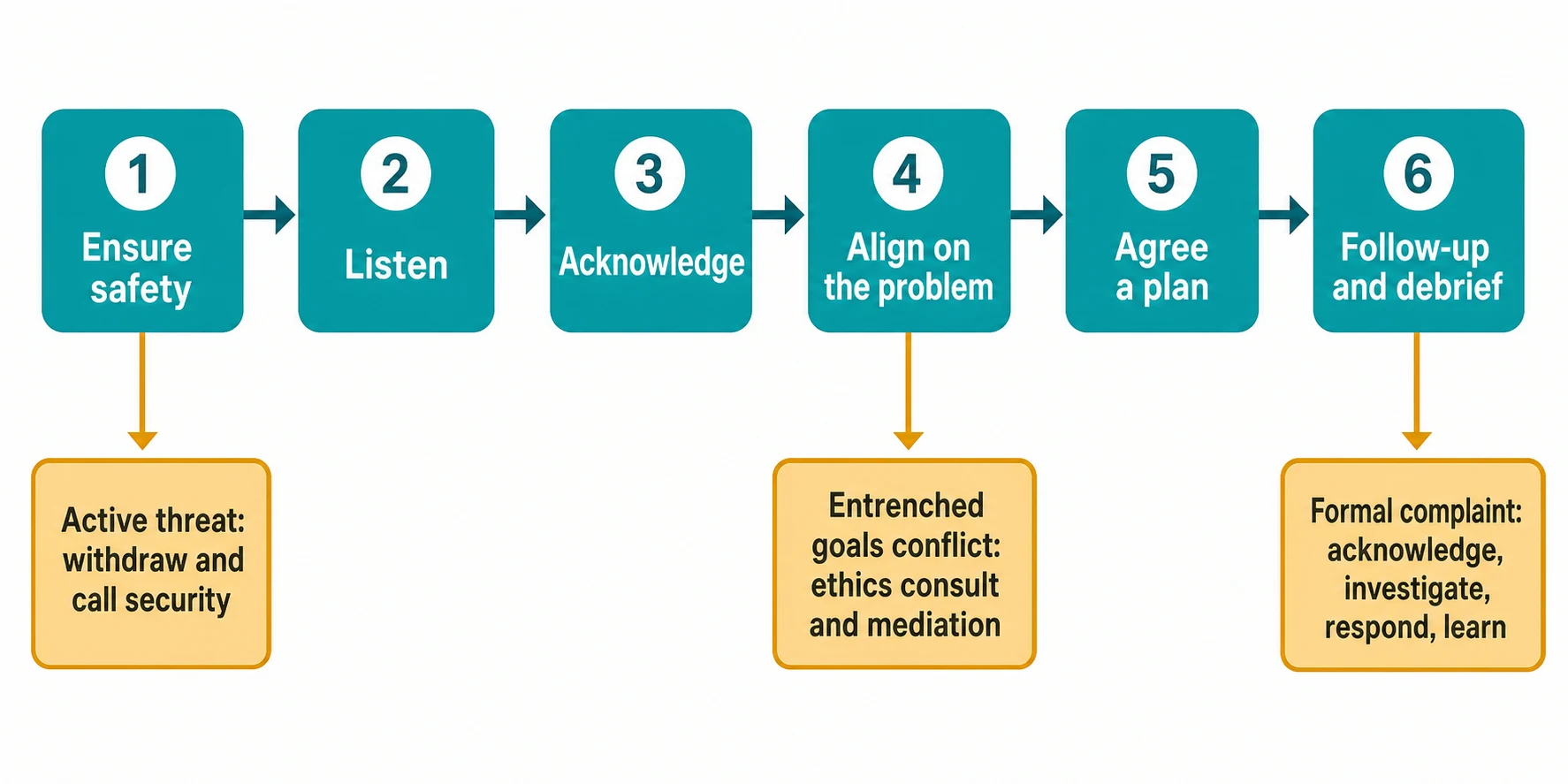
For the difficult encounter, use a shared arc. Prepare the setting (private, enough time, the right people, an interpreter if needed). Ensure safety. Listen actively to wants and feelings. Acknowledge the emotion before any content. Agree on what the problem actually is. Agree on a plan, even a small one. Arrange follow-up. Most difficult encounters resolve within this arc without ever reaching conflict. [3] [5]
For the angry or agitated family, use structured verbal de-escalation. The Project BETA consensus sets out the moves that reliably lower arousal: respect personal space and keep an exit; do not be provocative in posture or tone; establish verbal contact and use brief, plain language; identify the person's wants and feelings ("What do you need right now?"); listen closely to what they say back; agree, or agree to disagree, rather than argue; set clear, reasonable limits; and offer choices and optimism wherever possible. De-escalation is a skill and it is learnable. [5]
For a treatment or goals-of-care dispute, escalate up a ladder. Re-explore the family's values and what they most want for their child, and re-share the prognosis honestly — most "futility" disputes are really unmet hope and unclear prognosis. Seek a shared decision through the dedicated shared-decision-making process. Offer a genuine second opinion. If the dispute persists, call a formal ethics consultation or mediation; a randomised trial showed ethics consultation reduced non-beneficial life-sustaining treatment and conflict in intensive care. Call these supports early, not as a last resort. [6] [7]
For a formal complaint, follow the service-recovery arc and the local timeframe. Acknowledge the complaint within the time your local system requires (for example, promptly on receipt with a full written response to follow). Listen to the family's account. Apologise sincerely for any genuine shortcoming — a sincere apology is service recovery and, in many jurisdictions, is protected from use as an admission of liability. Investigate the facts. Respond in writing with a clear timeline, what was found, what will change, and who to contact next. Feed the learning back to the family and into the system. [1] [2] [13]
For the clinician, make welfare part of the management plan. Arrange a debrief, peer support and access to employee-assistance or practitioner-health services. Address the systemic contributors — workload, communication gaps, missing protocols — so that one complaint changes the service rather than merely punishing a person. [9] [10] [12]
Specific Subtypes & Scenarios
Angry parent after a delayed result. The fix is usually simpler than the emotion suggests: a private space, an honest account of what happened and why, a sincere apology for the delay, and a clear plan and timeline from here. Most of these encounters deflate the moment the family feels heard and sees a fix. [1] [3]
Parents in conflict over limiting life-sustaining treatment in PICU or NICU. The highest-stakes scenario. Run a structured family meeting, re-share prognosis honestly, explore what the family most wants for their child, seek shared goals, offer a second opinion, and call ethics consultation or mediation early. Neonatal and paediatric intensive care carry the deepest prognostic uncertainty and the most grief; pace the conversation and keep the relationship intact even when you disagree. [6] [7]
Parental refusal of recommended treatment or immunisation. First understand the reason — fear, a values choice, misinformation, a past experience. Provide honest, developmentally appropriate information, document the discussion and the refusal, explore the child's own view where they can give it, and involve ethics or safeguarding only when refusal places the child at risk of serious harm. Keep the door open; today's refusal is not necessarily tomorrow's. [6]
The demanding or "heartsink" family in clinic. Set the agenda together at the start ("let's agree the two most important things today"), bound the time, pre-empt the list, and use the team — nurse, social work, psychology — so the whole encounter does not rest on one depleted clinician. Name the pattern honestly with colleagues and supervisees so it becomes a shared problem, not a private dread. [3] [4]
Threatening or aggressive family member in the emergency department. Safety leads. Keep distance and an exit, summon security early, do not attempt de-escalation against an active threat, and separate the child if there is risk. Use de-escalation only for the distressed-but-not-dangerous. [5]
The clinician who has received a formal complaint. A common and damaging scenario. Complaints processes are stressful — doctors describe anxiety, sleep disturbance, depression and a shift toward defensive practice. Support is part of treatment: debrief, peer and practitioner-health contact, timely information about the process, and a culture that separates learning from blame. [11] [12]
Intra-team or inter-agency conflict. When clinicians disagree in front of the family, the family loses trust in everyone. Align the team privately first, nominate a single spokesperson, and present one consistent plan. Persistent team conflict is itself a patient-safety issue and warrants escalation to clinical leadership. [6] [10]
Complications & Pitfalls
- Matching or ignoring a parent's anger, which escalates the situation and hardens any later complaint. [5]
- Labelling a family "difficult" without examining the clinician and system contribution. [3] [4]
- Failing to acknowledge a genuine service failure or to apologise appropriately. [1] [13]
- Promising outcomes you cannot deliver, or deflecting blame onto colleagues in front of the family. [6]
- Continuing non-beneficial treatment, or withdrawing it abruptly, without addressing the underlying goals conflict. [6] [7]
- Attempting verbal de-escalation against an active threat, weapon or intoxication. [5]
- Ignoring clinician distress after a complaint or adverse event, leading to burnout, defensive practice or attrition. [8] [9]
- Altering the medical record after a complaint — addenda only, never revision. [11]
Prognosis & Disposition
A well-managed difficult encounter is judged not by how smoothly it ran but by what it leaves behind. [1] [9]
Markers of success. The family feels heard and can state the plan. Trust is preserved or restored, even after a genuine shortcoming. The plan is clear, with a named follow-up. The child's safety and the adolescent's voice have been protected. The team is aligned and has debriefed. [3] [6]
When to defer. If emotion is too high, the facts are unclear, or a key person is absent, it is legitimate to acknowledge, support, and reconvene. Deferral is a deliberate choice — name it and set a time, rather than drifting into avoidance. [1]
When to escalate. Persistent goals conflict, a request the team cannot meet, a breakdown of trust, or a family who remains unsafe warrants a second opinion, formal ethics consultation, mediation, or escalation to clinical leadership. Use these supports early; they work better before positions harden. [6] [7]
The disposition includes the clinician and the system. Build debrief, peer support and practitioner-health access into the routine. Feed each complaint into quality improvement so that one encounter changes the service. The ability to hold this work across a career depends on it. [9] [10] [12]
Special Populations
Adolescents. Within a family conflict, hold the young person's voice, assent and confidentiality. Where adolescent and family goals diverge, mediate; do not simply default to the parents or to the young person alone. [6]
Culturally and linguistically diverse families. Much conflict is born of simple misunderstanding. Always use a trained interpreter — never a child or family member — and consider a cultural broker. Ask how the family wishes decisions to be made and with whom. [5] [7]
Children with medical complexity and technology dependence. These families carry the highest-stakes, highest-trust longitudinal relationships. Conflict here is costly precisely because the relationship is long and load-bearing; invest early in shared decisions, written plans and reliable access. [6] [10]
Families affected by poverty, housing instability or out-of-home care. Much apparent non-adherence or anger is structural — cost, transport, chaos, past trauma. Recognise the driver before judging the behaviour, and bring in social work and community supports. [3]
Trainees and clinicians from under-represented groups. Complaints and hostile encounters are not evenly distributed; some clinicians and trainees are exposed to disproportionately more. Make support explicit, protect them from unsafe encounters, and address the systemic patterns. [11] [12]
Evidence, Guidelines & Regional Differences
Core anchors are the Hickson study linking complaints to malpractice risk, Reader's synthesis of complaints as safety data, Steinmetz and O'Dowd on the difficult patient and heartsink phenomenology, the Richmond Project BETA verbal de-escalation consensus, the Schneiderman randomised trial of ethics consultations, Lantos on neonatal decision-making, the Wu and Scott second-victim work, Edrees on hospital support for second victims, Bourne on the impact of complaints on doctor welfare and defensive practice, and Ross on apology laws. [1] [2] [3] [4] [5] [6] [7] [8] [9] [11] [12] [13]
Complaints flow through local health-service complaint mechanisms and, beyond that, to state Health Complaints Commissioners and the Health and Disability Commissioner in Aotearoa. Regulator notifications go to the Medical Board of Australia via AHPRA, and to the Medical Council of New Zealand. The Medical Board of Australia's Good medical practice code frames professional behaviour and managing concerns. AHPRA mandatory-reporting obligations apply; use locally endorsed channels and practitioner-health services (such as doctor-health programmes) for clinician support, and do not invent statutory wording. [2] [9]
The NHS complaints procedure sets the timeframes — acknowledgement and a response within defined local windows, with escalation to the Parliamentary and Health Service Ombudsman. The GMC's Good medical practice and Raising and acting on concerns frame professional duty, and the Care Quality Commission oversees service quality. RCPCH Progress+ names communication and patient safety as core professional skills. Local palliative, ethics and practitioner-health services support complex encounters. [11] [12]
The Joint Commission frames patient-safety and complaint-handling standards, and patient-advocacy services and risk-management teams mediate many complaints in-house. Many US states have apology laws that protect expressions of sympathy (and, in some states, fault-acknowledging apologies) from use as evidence in malpractice litigation, which supports open disclosure and service recovery. Hospital ethics committees and consult services are widespread. [1] [13]
The CanMEDS roles — Communicator, Collaborator, Professional, Leader and Health Advocate — map directly onto managing difficult encounters and conflict. Complaints go to provincial colleges of physicians and surgeons and to patient-relations offices, and provincial advance-care-planning and ethics-consultation frameworks apply. Use local documents and trained interpreters. [6] [9]
Controversies: the balance between learning and blame in complaint handling; whether and how far apology laws reduce litigation; the thresholds for mandatory reporting of colleague conduct or impairment; and how to protect clinician welfare without compromising accountability. Exam answers show structured skill, honest acknowledgement, and local humility about the complaint system you work in. [1] [12] [13]
Exam Pearls
- Safety first: do not attempt verbal de-escalation against an active threat — withdraw and call security. [5]
- De-escalate with BETA: respect space, do not be provocative, brief language, identify wants and feelings, listen, agree where you can, set limits, offer choices. [5]
- The "difficult" label is a relationship and systems signal, not a property of the family. [3] [4]
- Most parental anger is fear, grief or guilt; treat the fear and the anger falls. [7]
- Ethics consultation reduces non-beneficial treatment and conflict — call it early. [6] [7]
- Complaints predict malpractice risk; communication and service recovery are preventive. [1]
- Acknowledge a complaint within the local timeframe; apologise sincerely for any shortcoming; investigate; respond in writing; feed back the learning. [2] [13]
- The clinician is a second victim after harm or complaint — debrief and support are part of management. [8] [9]
- Document factually and contemporaneously; never alter the record after a complaint. [11]
- Align the team before you align the family; never contradict a colleague in front of them. [6]
A difficult encounter at the bedside
Ensure safety: any threat, weapon or intoxication means withdraw and call security
Listen actively: what happened, and what do they most need today
Acknowledge the emotion before any content; tolerate silence
Align on the real problem: expectation gap, service failure, fear or values conflict
Agree a plan, even a small one, with a named follow-up
Debrief the team and feed any learning back into the system
References
- [1]Hickson GB Patient complaints and malpractice risk. JAMA, 2002.PMID 12052124
- [2]Reader TW Learning from healthcare complaints: challenges and opportunities. BMJ quality & safety, 2026.PMID 40908154
- [3]Steinmetz D The 'difficult patient' as perceived by family physicians. Family practice, 2001.PMID 11604370
- [4]O'Dowd TC Five years of heartsink patients in general practice. BMJ, 1988.PMID 3139188
- [5]Richmond JS Verbal De-escalation of the Agitated Patient: Consensus Statement of the American Association for Emergency Psychiatry Project BETA De-escalation Workgroup. Western journal of emergency medicine, 2012.PMID 22461917
- [6]Schneiderman LJ Effect of ethics consultations on nonbeneficial life-sustaining treatments in the intensive care setting: a randomized controlled trial. JAMA, 2003.PMID 12952998
- [7]Lantos JD Ethical Problems in Decision Making in the Neonatal ICU. The New England journal of medicine, 2018.PMID 30403936
- [8]Wu AW Medical error: the second victim. The doctor who makes the mistake needs help too. BMJ, 2000.PMID 10720336
- [9]Scott SD The natural history of recovery for the healthcare provider 'second victim' after adverse patient events. Quality and safety in health care, 2009.PMID 19812092
- [10]Edrees HH Do Hospitals Support Second Victims? Collective Insights From Patient Safety Leaders in Maryland. Joint Commission journal on quality and patient safety, 2017.PMID 28844233
- [11]Bourne T Doctors' experiences and their perception of the most stressful aspects of complaints processes in the UK: an analysis of qualitative survey data. BMJ open, 2016.PMID 27377638
- [12]Bourne T Doctors' perception of support and the processes involved in complaints investigations and how these relate to welfare and defensive practice: a cross-sectional survey of UK physicians. BMJ open, 2017.PMID 29162574
- [13]Ross NE The Role of Apology Laws in Medical Malpractice. Journal of the American Academy of Psychiatry and the Law, 2021.PMID 34011538