Paeds · professional-practice-and-evidence
Ethical allocation of resources in paediatrics
Also known as Distributive justice in child health · Triage and rationing of paediatric resources · Allocation of scarce medical resources for children · Accountability for reasonableness in paediatrics · Fair allocation of critical care and expensive therapies · Macro, meso and micro rationing in child health
Fellowship-level approach to ethical allocation of resources in paediatrics: distributive justice, absolute versus relative versus cost-based scarcity, the four allocation principles, accountability for reasonableness, pandemic surge triage, organ transplant listing, expensive gene and enzyme therapies, ECMO and chemotherapy-drug-shortage allocation, equity for disabled and disadvantaged children, and regional differences across ANZ, UK, US and Canada.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
Picture two deteriorating children on a winter night, one PICU bed, and a retrieval ambulance thirty minutes away. Your job is not to pretend the scarcity away, and it is not to choose by instinct. It is to apply a defensible, transparent method that a reasonable person can accept even when they grieve the outcome. [1] [4]
Five ideas do most of the work. Distributive justice is the ethical principle that governs how scarce and beneficial resources are shared across a population — distinct from best interests, which governs one child's benefit-versus-burden balance. Allocation assigns a scarce resource to a recipient; rationing withholds a beneficial resource because it cannot be offered to everyone who needs it. The two often travel together, and naming the difference keeps you honest about what you are doing. [1] [2]
Scarcity comes in three flavours that change the pathway. Absolute scarcity is demand that exceeds any supply — a pandemic surge, a mass-casualty disaster. Relative scarcity is demand that exceeds supply right now — a full PICU, a single ventilator, a long wait for a sub-specialty opinion. Cost scarcity is a therapy too expensive to offer to all who could benefit — a gene therapy costing millions, a donated organ. Each calls for a different locus of decision. [3] [12]
Accountability for reasonableness is the procedural standard Daniels and Sabin set for fair allocation: the criteria are public, they are relevant to stakeholders, there is an appeals and revision process, and there is enforcement. A defensible decision is one a reasonable person can accept even when they disagree with the outcome — which is why process matters as much as principle. [2]
[1] [2] [3]Classification
Classify by the kind of scarcity, because the pathway depends on it. Start from the supply side, not from the bedside emotion. [3] [12]
Absolute scarcity is the triage territory. Demand overwhelms any conceivable supply, as in a pandemic surge or a mass-casualty event, and the standard obligation to give each child the best care must give way to the obligation to give the population the best chance. Here a pre-agreed triage protocol, applied by a triage officer separated from the treating team, is the defensible pathway. [6] [7]
Relative scarcity is the everyday reality. Beds, staff, equipment and sub-specialty time are chronically constrained, and the question is how to allocate flow fairly rather than how to triage survival. Most paediatric scarcity lives here, and it is managed by bed managers, retrieval coordination and transparent escalation, not by bedside unilateralism. [12]
Cost scarcity is the funding territory. A therapy is beneficial but too expensive to offer to all, and the decision belongs at macro or meso level — a health-technology-assessment body, a hospital drug committee, a transplant allocation system — rather than at the bedside. [9]
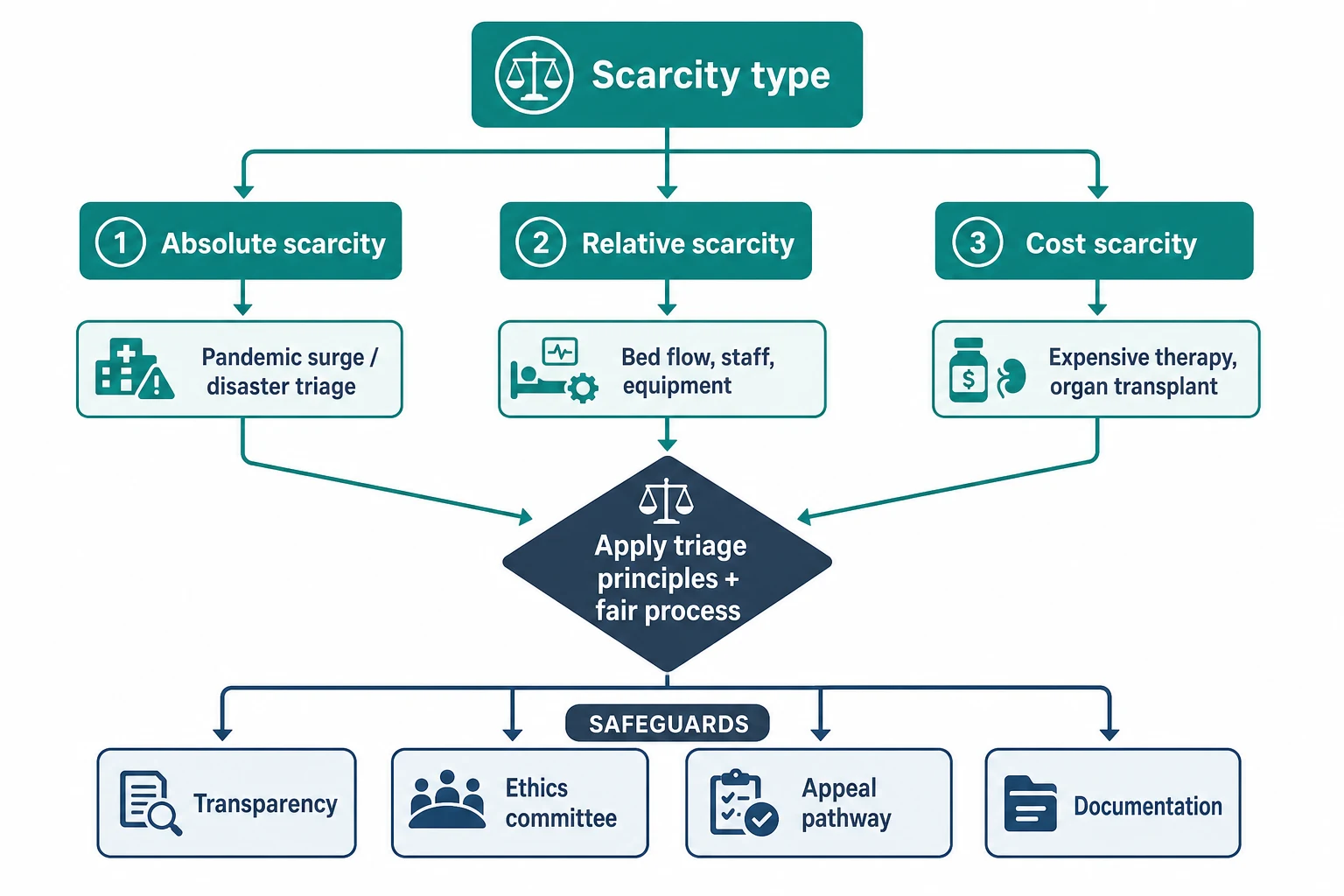
Decision pathway by scarcity type
Epidemiology & Risk Factors
Scarcity is a recurring, not exceptional, feature of paediatric practice. Seasonal bronchiolitis and influenza overwhelm PICU capacity every winter, drug shortages recur in paediatric oncology, sub-specialty waiting lists lengthen, and a single expensive therapy can absorb the budget of a whole service. [10] [12]
A pandemic can multiply critical-care demand several-fold, and the children affected are not evenly distributed. Technology-dependent children with complex chronic illness accumulate recurrent critical episodes and place concentrated demand on PICU and retrieval, while previously well children flood the system during a surge. [7]
Drug shortages are common and consequential in paediatric oncology, forcing explicit allocation of life-saving chemotherapy and supportive agents across children who all need them. The consensus position is that allocation should be by clinical priority and equipoise, with institutional ethics input and transparent documentation — never by quiet clinician preference. [9] [10]
The system-level risk factors for inequitable allocation are the familiar determinants: rurality, socioeconomic disadvantage, indigenous and migrant status, disability, and a simple lack of advocacy. When no equity correction is built in, these factors quietly concentrate resources away from the children who already have the least. [8]
Clinician moral distress is itself a marker of a failing system. When no transparent allocation process exists, individual clinicians ration covertly at the bedside, and the moral residue of those unspoken decisions accumulates into burnout and inconsistency. Building a fair, visible process is partly an antidote to that distress. [12]
Pathophysiology
There is no enzyme for fairness, but there is a mechanism. The "mechanism" of allocation is the ethical and procedural machinery that converts a constrained supply into a defensible decision, and four principles do most of the conversion. [1]
Maximise benefits asks how to save the most lives or life-years from the scarce resource. Operationalised, it means estimating short-term survival and longer prognosis and allocating where the gain is greatest — while refusing the temptation to discount the life-years of disabled children, whose years count equally. [1] [3]
Prioritise the worst off has two readings that pull against each other. "Sickest first" allocates to the child in greatest immediate need; "youngest first" (the fair-innings argument) allocates to the child who has had the least life so far. Both are defensible, and a good triage protocol weights them transparently rather than collapsing one into the other. [1] [8]
Treat people equally means that when candidates are genuinely comparable on benefit and need, the tie is broken by a fair method — a random lottery or first-come — rather than by who the family knows or how loudly they advocate. Promote instrumental value gives some priority to health-care workers who can return to save others, a principle that sits uncomfortably and is used sparingly and explicitly. [3]
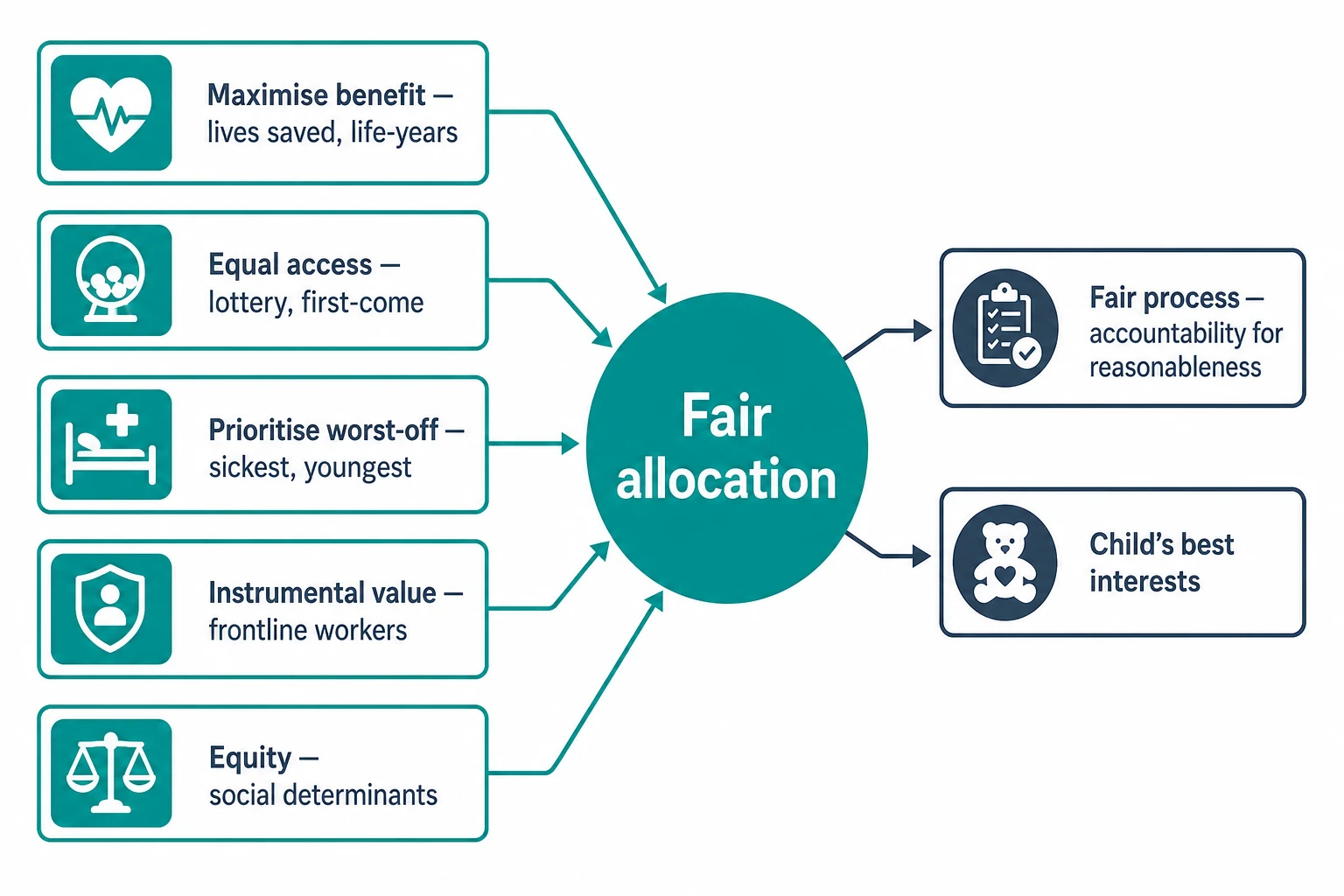
Process is the part candidates understate. Daniels and Sabin argued that the legitimacy of an allocation decision rests on accountability for reasonableness: criteria are public, relevant to stakeholders, appealable and enforced. A community can accept a painful outcome if it can see how the decision was made; it cannot accept one made in secret. [2]
Social determinants operate on the mechanism as a bias. Without an equity correction, distance, poverty and weak advocacy distort allocation away from disadvantaged children, so the same principles produce unequal outcomes. Naming this is the first step to correcting it. [8]
[1] [2] [3]Clinical Presentation
From the doorway, an allocation problem announces itself differently depending on the scarcity. Recognising the shape tells you which pathway to invoke. [3]
The everyday presentation of relative scarcity is a full PICU with no bed for an incoming retrieval, a single ventilator for two deteriorating children, or a sub-specialty waiting list that has stretched past a safe interval. The pain is real, but the pathway is coordination and escalation, not survival triage. [12]
The surge presentation is a pandemic or disaster in which demand overwhelms capacity and the framework shifts from best care for each child to best care for the population. This is where a pre-agreed triage protocol must be invoked, and where improvisation is most dangerous. [6] [7]
The cost-scarcity presentation is a family and clinician seeking a high-cost therapy — CAR-T for relapsed leukaemia, a gene therapy for spinal muscular atrophy, an enzyme replacement for a lysosomal storage disorder — that the health system will fund for only some children or none. The decision is principled but the locus is the funding body, not the bedside. [9]
The organ-transplant presentation is a child listed for a scarce donated organ, where allocation score, waiting time and urgency compete within a transparent system. The clinician's role is to assess and advocate within the system, not to route around it. [11]
The drug-shortage presentation is a paediatric oncology service that must allocate limited stock of a life-saving agent across children who all need it. Here the consensus is to allocate by clinical priority, with ethics input and full documentation. [9] [10]
The rural and remote presentation is a child whose access to the scarce resource is limited by geography and retrieval time rather than by need — a reminder that distance can become covert rationing if it is not actively corrected. [8]
Differential Diagnosis
When a team feels a child is being denied a resource, your first task is to work out what kind of problem it is. The label changes everything downstream. [1]
| Surface presentation | What it might actually be | Must-not-miss alternative |
|---|---|---|
| "We're rationing this bed" | Poor flow or planning, not true scarcity | A fixable process failure |
| "It's too expensive to offer" | A funding dispute, not clinical scarcity | A macro-level HTA decision |
| "The disabled child gets less" | Quality-of-life bias dressed as triage | Invidious discrimination to be excluded |
| "First-come, first-served" | A defensible tie-break among equals | Covert favouritism if the candidates are not comparable |
Discriminate a genuine allocation decision from a best-interests decision. Allocation is about fair distribution across a population; best interests is about one child's benefit-versus-burden balance. Confusing them makes you apply population logic to an individual, or individual logic to a population, and both are errors. [1]
Distinguish absolute scarcity from poor flow. A full PICU on a Monday morning is often a process failure to be fixed — earlier discharges, better step-down, regional coordination — rather than an ethical triage. Treating a fixable problem as a triage is itself an allocation error. [12]
Separate a cost-based allocation decision from rationing by insurer exclusion. A funding dispute is a macro-level question for the health-technology-assessment body; resolving it at the bedside by simply not offering the therapy is ethically perilous. [9]
Distinguish a defensible youngest-first priority from invidious ageism. The fair-innings argument — that a child with a whole uncompleted life has a claim on life-saving resources — is justified. Blanket de-prioritisation of disabled children on quality-of-life grounds is not, and conflating the two is a serious and examinable error. [8]
Clinical & Bedside Assessment
Begin every allocation encounter by classifying the scarcity. Is it absolute, relative or cost-based, and is a triage protocol already in force or must one be invoked? The answer sets the pathway before you touch the children. [3] [6]
Assess each candidate child against the agreed triage criteria — short-term survival probability, longer prognosis, life-years, and instrumental value — rather than against personal appeal or who is most photogenic. Validated prognostic scoring reduces individual clinician bias, though no score is perfect for children and it informs rather than replaces judgement. [7]
Assess for the biases that must be excluded. Disability, weight, socioeconomic status, family influence, race, indigeneity and migrant status must not rank children, and you say so out loud so the team hears the exclusion. [8]
Assess the child's best interests and voice within the allocation. Even in a population decision, the individual child's assent, comfort and family understanding still matter, and a developmentally appropriate explanation belongs to the encounter. [8]
Assess the procedural safeguards. Is the decision transparent, is an ethics committee available for a contested call, and is there an appeal pathway a family can use? Their presence is what makes the decision defensible. [2]
Assess the communication. Who tells the family, in what language, with an interpreter if needed, and how is the rationale documented so it survives a complaint or a court? A decision that is fair but communicated badly will be experienced as unfair. [4]
Investigations
There is no diagnostic test for fair allocation. The "investigations" are the prognostic tools and the procedural consultations that feed a defensible decision. [7]
Validated prognostic scoring is the closest thing to an objective test in surge triage. Paediatric-aware mortality prediction and organ-dysfunction scores reduce individual clinician bias, and a published protocol that incorporates them is more defensible than a registrar's gut sense. Use them, while acknowledging that any score is a crude proxy for a child. [6] [7]
Ethics committee consultation and a second senior clinician are the procedural "investigations" of a contested allocation. Bring them in before the decision is fixed, not after, because their value is in shaping the reasoning rather than rubber-stamping it. [2]
Health-technology-assessment appraisal — cost-effectiveness, budget impact, quality-adjusted life-years — informs cost-based allocation. Use it, but guard against its tendency to disadvantage disabled children whose life-years count equally, and read the result alongside equity, not instead of it. [9]
Audit and registry data check that an allocation system is not systematically disadvantaging a group of children. If the indigenous, disabled, rural or migrant children are consistently under-represented among recipients, the system has a problem the next cycle must correct. [8]
When the scarcity is disputed — is this a real shortage or a planning failure? — the right "investigation" is an honest review of flow, capacity and regional coordination, because fixing a process failure removes an artificial scarcity. [12]
Management — Resuscitation
In an acute surge, invoke the pre-agreed triage protocol immediately rather than improvising at the bedside. The separation of a triage officer from the treating clinician preserves trust: the treating team advocates for their patient, and the triage officer applies the population logic, so no single clinician carries both. [6] [7]
Maintain comfort care for every child regardless of the allocation outcome. No child loses symptom relief, family presence or dignity because a scarce bed or ventilator went elsewhere — allocation withdraws only the specific intervention, never care. [5] [8]
Distinguish a reversible intercurrent event from progression of the underlying condition. A child on a comfort plan may still develop a treatable, distressing problem, and you treat what relieves suffering and stabilise the child while the triage decision is made. [8]
Do not let the absence of a bed delay parallel actions. Escalate comfort, support the family, activate retrieval, and hand over the triage decision explicitly so the direction of care never depends on who is on shift. [12]
Reassure the family that a triage decision reflects scarcity, not a judgement that their child's life is worth less. This reframe matters: a family that hears "your child was not worth a bed" has been grievously misled, and a family that hears "we had to follow the protocol and your child still receives full comfort care" can grieve without betrayal. [4] [8]
Anticipate and treat the distress a triage decision creates in staff as well as families. A debrief, a clear record and visible ethics support carry the team through a decision no one wanted to make. [8]
Management — Definitive & Stepwise
Use a sequence you can defend out loud in a viva, anchored on the four principles and accountability for reasonableness. [1] [2]
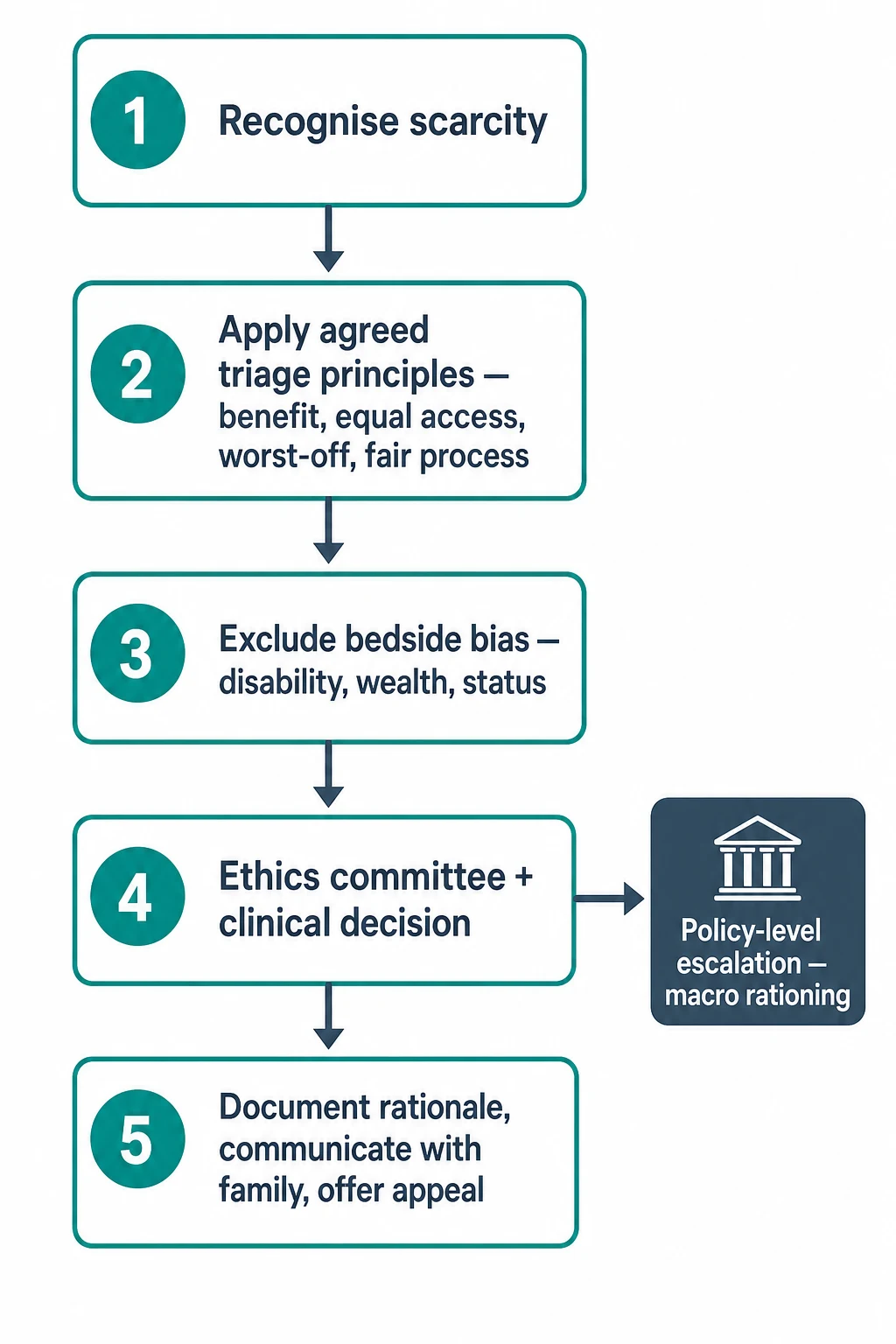
Paediatric resource-allocation algorithm
Recognise the scarcity — absolute, relative or cost-based — and invoke the correct pathway
Apply the agreed triage principles — maximise benefit, treat equally, prioritise worst-off, instrumental value
Exclude bedside bias — disability, weight, socioeconomic status, family influence, race, indigeneity, migrant status
Seek ethics and clinical consensus — second senior clinician, ethics committee, and the treating team
Operationalise accountability for reasonableness — publicity, relevance, appeals, enforcement
Document the scarcity, the criteria, the ethics input, the family communication and the appeal pathway
Maintain comfort care for every child regardless of outcome; allocation withdraws only the specific intervention
Audit outcomes by disadvantage and correct systematic inequity in the next cycle
Route cost-based decisions through the funding body rather than the bedside. A gene therapy, an enzyme replacement or an orphan drug is allocated by explicit macro-level criteria — cost-effectiveness, equity, budget impact — adjudicated by a health-technology-assessment body, and the clinician's role is to advocate for the child within that system, not to gatekeep silently. [9]
For organ allocation, follow the transparent scoring system that balances urgency, waiting time, waiting-list mortality and post-transplant prognosis. Document any exception and the reason for it, and remember that the clinician assesses and advocates but does not own the allocation. [11]
Build equity into every level. Monitor allocation outcomes by indigenous status, disability, rurality and socioeconomic status, and where a group is systematically disadvantaged, correct it in the next planning cycle. Equity is not a footnote to allocation; it is a condition of its legitimacy. [8]
Specific Subtypes & Scenarios
Pandemic surge triage. Apply a published paediatric-aware triage protocol that maximises lives and life-years, excludes blanket exclusion criteria, and protects disabled children. Separate the triage officer from the treating team, apply validated prognostic scoring, and document every decision against the protocol. [6] [7]
Organ transplant listing. A scarce donated organ is allocated by a transparent score balancing urgency, waiting time, waiting-list mortality and post-transplant prognosis. The clinician assesses suitability, advocates for the child, and documents any exception — but does not route around the system. [11]
Expensive gene and enzyme therapies. CAR-T for relapsed leukaemia, a gene therapy for spinal muscular atrophy, or an enzyme replacement for a lysosomal storage disorder are cost-based allocations decided at macro or meso level with explicit criteria. The bedside clinician does not individually gatekeep; they make the case and let the system decide transparently. [9]
ECMO allocation. When circuits are scarce, apply principles of benefit, worst-off and fair process. Whether past treatment decisions or refusals should affect a child's claim is itself a question for ethics and protocol, not bedside judgement. [11]
Chemotherapy drug shortages. Allocate scarce life-saving oncology drugs by clinical priority and equipoise, with institutional ethics input and transparent documentation. The consensus is explicit, prioritised allocation — never quiet clinician preference. [9] [10]
Rural and remote access. Address geographic inequity by retrieval planning, telehealth and outreach so that distance does not become covert rationing. A child in a remote community should not lose a claim on a resource because the resource is far away. [8]
Indigenous and disadvantaged children. Apply culturally safe, equity-corrected allocation so that system-level disadvantage is not compounded at the point of distribution. Involve kinship and community decision structures where the family seeks it, while verifying legal authority. [8]
Withdrawal to reallocate during scarcity. Truog, Mitchell and Daley argued that withdrawing a ventilator from one patient to save more lives is ethically permissible under transparent, consistent criteria — but it is never a unilateral bedside act, and the decision must be defensible, documented and accompanied by comfort care. [5]
Complications & Pitfalls
- Covert bedside rationing by an individual clinician with no transparent policy or appeal pathway. [12]
- Ranking children by disability, weight, socioeconomic status or family influence. [8]
- Treating a funding dispute as a clinical-scarcity triage and acting at the bedside. [9]
- Applying an adult triage protocol to children without paediatric prognostic adjustment. [6]
- Letting QALY logic systematically disadvantage disabled children whose life-years count equally. [8]
- Withholding comfort care from a child who did not receive the scarce resource. [5]
- Improvising triage during a surge instead of invoking the pre-agreed protocol. [7]
- Failing to document the scarcity, the criteria, the ethics input and the appeal pathway. [2]
- De-prioritising indigenous, migrant or rural children because their access or advocacy is weaker. [8]
- Conflating the fair-innings argument (justified) with blanket ageism against disabled children (not). [1]
Prognosis & Disposition
A transparent, principle-based allocation process pays off in legitimacy. Families and the public can accept a painful outcome when they can see how the decision was made, and a service that allocates fairly earns the trust that lets it function in the next crisis. [2] [4]
Covert or biased allocation erodes that trust. It invites complaint and litigation, deepens staff moral distress, and produces outcomes that are hard to defend because no one can explain how they were reached. [12]
Children who do not receive a scarce resource must still receive active comfort care and family support. Allocation never withdraws care — only the specific scarce intervention — and a disposition that omits comfort is incomplete and examinable. [5]
An appeal pathway and ethics review belong to the disposition of any contested allocation. A family who can appeal, and a team who can debrief, carry the decision better than one left to absorb it alone. [2]
Audit and follow-up of allocation outcomes identify and correct systematic inequity over time. A system that monitors who receives scarce resources — by indigenous status, disability, rurality and socioeconomic status — and corrects the gaps is one that stays legitimate. [8]
The long-term legitimacy of a paediatric service depends on being able to show that its allocation was fair, not merely that it was clinical. Process, documentation and equity are the disposition, not an afterthought. [1] [2]
Special Populations
Disabled children and children with neurodisability. Guard against QALY and quality-of-life bias. Their life-years count equally in any allocation, and a triage protocol that discounts them is discriminatory. [8]
Indigenous children. Apply culturally safe, equity-corrected allocation, and involve kinship and community decision structures where the family seeks it, while verifying legal authority. [8]
Migrant, refugee and asylum-seeking children. Allocate on clinical need alone, never on citizenship, visa status or ability to pay. A child is a child for the purposes of scarce-resource allocation. [8]
Rural and remote children. Correct for geography and retrieval time so distance is not covert rationing. Retrieval planning, telehealth and outreach are part of equitable allocation. [8]
Socioeconomically disadvantaged children. Counter the advocacy gap so that quieter families are not disadvantaged. Explicit criteria protect families who cannot push as hard. [8]
Neonates and infants. The fair-innings argument applies, balanced against prognosis and best interests. A whole uncompleted life gives weight, but it does not override a defensible prognosis. [1]
Technology-dependent children. Recurrent admissions do not by themselves reduce a child's claim on scarce resources. Their place in a triage depends on the same criteria as anyone else's. [8]
Adolescents. Involve the young person's voice and assent within the allocation decision where developmentally appropriate, even when they are not the legal decision-maker. [8]
Evidence, Guidelines & Regional Differences
Persad, Wertheimer and Emanuel (Lancet 2009) set out the canonical principles for allocating scarce medical interventions — maximise benefit, treat people equally, prioritise the worst off, and promote instrumental value — and they remain the spine of every modern triage protocol. [1]
Daniels and Sabin (1997) articulated accountability for reasonableness as the procedural standard for fair allocation: the criteria are public, relevant, appealable and enforced. Their work frames why a fair process can be legitimate even when the outcome is painful. [2]
Emanuel and colleagues (NEJM 2020) and White and Lo (JAMA 2020) adapted these principles for COVID-19 ventilator and critical-care-bed rationing, emphasising maximising benefit, treating equally, prioritising the worst off, and recognising instrumental value. [3] [4]
Truog, Mitchell and Daley (NEJM 2020) argued that even in extreme scarcity, withdrawing a ventilator from one patient to save more lives must rest on transparent, consistent criteria, accompanied by comfort care — never on bedside unilateralism. [5]
Christian and colleagues (CMAJ 2006) developed the seminal critical-care triage protocol for an influenza pandemic. Christian, Toltzis and Kanter (PCCM 2011) and Antommaria and colleagues (PCCM 2011) adapted treatment and triage for paediatric mass critical care, and set out the ethical safeguards for children. [6] [7] [8]
Unguru and colleagues (JNCI 2016) and DeCamp, Joffe and Fernandez (Pediatrics 2014) set out the ethical framework and consensus for allocating scarce chemotherapy in childhood cancer. Kukora and Laventhal (Acta Paediatr 2016) examined whether past medical decisions should affect ECMO allocation, and Sinuff and colleagues (CCM 2004) systematically reviewed how often rationing of critical-care beds is covert. [9] [10] [11] [12]
Australia and Aotearoa New Zealand approach resource allocation through publicly funded systems with explicit health-technology-assessment. Australia's Pharmaceutical Benefits Advisory Committee and New Zealand's Pharmac make cost-based allocation transparently, and state-based critical-care networks coordinate relative scarcity. State the principle — fair allocation rests on the four principles and accountability for reasonableness, with macro-level cost decisions made by the funding body — and direct examiners to local policy, hospital triage protocols and legal advice for operational thresholds. Never invent a budget figure or a named statutory section. [2] [9]
Exam Pearls
ALLOCATE
References
- [1]Persad G, Wertheimer A, Emanuel EJ Principles for allocation of scarce medical interventions. Lancet, 2009.PMID 19186274
- [2]Daniels N, Sabin J Limits to health care: fair procedures, democratic deliberation, and the legitimacy problem for insurers. Philos Public Aff, 1997.PMID 11660435
- [3]Emanuel EJ, Persad G, Upshur R, Thome B, Parker M, Glickman A, Zhang C, Boyle C, Smith M, Phillips JP Fair Allocation of Scarce Medical Resources in the Time of Covid-19. N Engl J Med, 2020.PMID 32202722
- [4]White DB, Lo B A Framework for Rationing Ventilators and Critical Care Beds During the COVID-19 Pandemic. JAMA, 2020.PMID 32219367
- [5]Truog RD, Mitchell C, Daley GQ The Toughest Triage - Allocating Ventilators in a Pandemic. N Engl J Med, 2020.PMID 32202721
- [6]Christian MD, Hawryluck L, Wax RS, Cook TJ, Lazar NM, Herridge MS, Muller MP, Gowans DR, Fortther T, Burkle FM Development of a triage protocol for critical care in an influenza pandemic. CMAJ, 2006.PMID 17116904
- [7]Christian MD, Toltzis P, Kanter RK, Burkle FM, Vernon DD, Ni ET, Trees AL; Task Force for Mass Critical Care Treatment and triage recommendations for pediatric emergency mass critical care. Pediatr Crit Care Med, 2011.PMID 22067919
- [8]Antommaria AH, Powell T, Miller JE, Christian MD, Randolph A, Remy L, Silveira MJ; Task Force for Mass Critical Care Ethical issues in pediatric emergency mass critical care. Pediatr Crit Care Med, 2011.PMID 22067926
- [9]Unguru Y, Fernandez CV, Bernhardt B, Brock DW, Kodish E, Abbott L, Donenfeld A, Godder K, Pentz R, Berg SL, Adamson PC, Wood A, Hlubocky F, Daugherty CK An Ethical Framework for Allocating Scarce Life-Saving Chemotherapy and Supportive Care Drugs for Childhood Cancer. J Natl Cancer Inst, 2016.PMID 26825103
- [10]DeCamp M, Joffe S, Fernandez CV, Fossella N, Hooke MC, LaFond N, McCarten K, Pearson M, Stork L, Wagner L, Adamson PC, Hlavorson A, Liu D, Unguru Y; Children's Oncology Group Chemotherapy drug shortages in pediatric oncology: a consensus statement. Pediatrics, 2014.PMID 24488741
- [11]Kukora S, Laventhal N Choosing wisely: should past medical decisions impact the allocation of scarce ECMO resources? Acta Paediatr, 2016.PMID 27146166
- [12]Sinuff T, Kahnamoui K, Cook DJ, Luce JM, Levy MM Rationing critical care beds: a systematic review. Crit Care Med, 2004.PMID 15241106