Paeds · professional-practice-and-evidence
Health literacy and accessible paediatric information
Also known as Health literacy in paediatrics · Teach-back and plain language · Universal precautions health literacy · Accessible information for children and families · Parental health literacy · Plain language paediatric communication · Millilitre dosing and pictograms
Fellowship-level approach to health literacy and accessible paediatric information: universal precautions, teach-back, plain language, millilitre dosing with oral syringes and pictograms, reader-matched written materials, language and disability access, child health-literacy development, and AHRQ, NHS Accessible Information Standard and ANZ frameworks.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
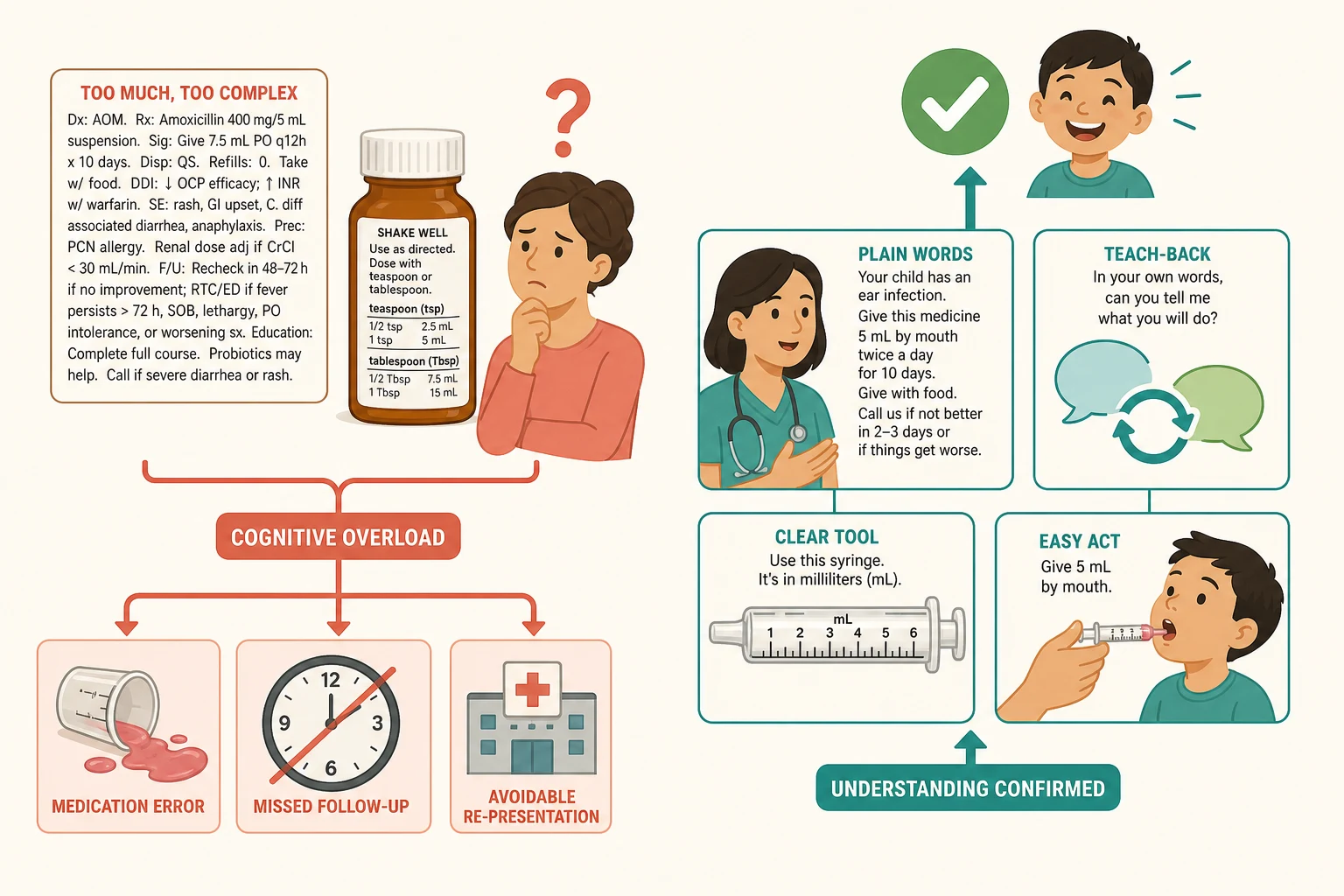
A mother is sent home from the emergency department with a febrile child, an antibiotic, and a leaflet. She nods, signs, and leaves. Two days later the child is back — under-dosed, the course unfinished, the safety-net misunderstood. Nothing here was rare, and nothing about the family was unusual. The failure was that information was given but never made usable. That gap is what health literacy is about. [1] [8]
Health literacy is the motivation, knowledge, confidence and skill a person needs to find, understand, appraise and use health information to make decisions for themselves and their child. It is not the same as being able to read. A highly educated parent can still be defeated by a jargon-heavy discharge summary, a confusing medicine label, or fear in a frightened moment. [1] [6]
Paediatrics adds a layer, because the information has to reach the parent and, over time, the child. You are building two sets of skills at once: the carer's capacity to act today, and the young person's capacity to manage their own health tomorrow. A service that ignores this produces avoidable errors, missed follow-up, and widening inequity. [1] [4]
The job is concrete. Make every instruction plain, confirm it with teach-back, dose liquid medicines safely, match written materials to the family, and meet language and accessibility needs every time. Do this for everyone, not just the families who look like they need it. [2] [7]
Classification
Think of health literacy as having two faces and two strategies. The two faces say whose skills are in play; the two strategies say how you respond. [1] [7]
Personal health literacy is the family's own capacity — what the parent or young person can find, understand and do. Organizational health literacy is the mirror image: how equitably your service makes information easy to reach, understand and act on. A parent with strong skills can still fail inside a system that defaults to jargon forms and teaspoon units, so you must work on both. [1] [7]
The two strategies are universal precautions versus targeted screening. Universal precautions means you assume every family may have difficulty and you apply plain language and teach-back to all, without singling anyone out. Routine adult-style literacy testing is not recommended in paediatric care, because it costs time, causes shame, and you cannot reliably tell who needs help by looking. [7] [1]

A useful third lens is Nutbeam's depth of skill. Functional literacy is reading a dose label. Interactive literacy is pulling the right answer out of a fast consultation. Critical literacy is judging whether the online advice a parent found is trustworthy. You build all three, but most of your daily work sits at the functional and interactive level — the dose, the plan, the warning signs. [1] [6]
| Aspect | Personal health literacy | Organizational health literacy |
|---|---|---|
| Whose skills | The parent's and child's own | The service's systems and defaults |
| Example failure | Cannot parse a decimal dose | Leaflet written three grades too high |
| Lever | Teach-back, plain language, skill-building | Readable templates, mL-only prescribing, interpreters |
| Goal | Equip the family to act | Stop the system defeating them |
Epidemiology & Risk Factors
Low health literacy is common and it is hidden. Population studies put roughly half of adults below the level needed for everyday health tasks, so in any paediatric waiting room a large fraction of carers are quietly struggling. A systematic review of health literacy and child health outcomes linked lower literacy to poorer knowledge, weaker self-management and worse service use in families. [1] [6]
The families carrying the heaviest information load are often given the densest instructions. Parents of children with chronic, complex or technology-dependent illness manage polypharmacy, multiple specialists and intricate action plans — and they are the ones most harmed by inaccessible information. [8] [10]
Several factors magnify the risk rather than cause it on their own: limited English proficiency, lower formal education, socioeconomic disadvantage, recent migration or refugee experience, intellectual or learning disability, and vision or hearing impairment. None of these lets you predict an individual, which is exactly why universal precautions beats profiling. [11] [12]
Language discordance carries its own measurable harm. Parents who are less comfortable in English experience more adverse events when their child is hospitalised, and Hispanic parents with lower health literacy and English proficiency make more liquid-medication dosing errors. These are safety signals, not cultural curiosities. [12] [11]
Pathophysiology
There is no enzyme for misunderstanding a dose, but there is a mechanism. Information harm is a cognitive-load problem. When instructions are dense, jargon-heavy, numerically demanding, or delivered under time pressure, working memory is overwhelmed and key actions get dropped. The parent who nodded in clinic is genuinely unable to hold all the pieces at once. [1] [8]
The mismatch is structural. Most paediatric patient-education materials are written well above the recommended reading level, so the default handout silently excludes a large share of families before anyone opens their mouth. You are fighting the system's defaults, not just one conversation. [1] [9]
Numeracy is the choke point for medication safety. A label that mixes teaspoon and tablespoon, a dosing cup with confusing marks, or a decimal point can convert a capable parent into a measurably worse doser. When the unit is unclear, the error rate climbs. [3] [9]
Teach-back works by forcing the information back through the parent's own words. If they can restate the plan, the gap between giving and understanding is closed before the family leaves the room. Schillinger's closing-the-loop study linked this single technique to better diabetic control among low-literacy adults, and it remains the best-studied brief intervention we have. [5] [8]
The ceiling is set by the organization. If the system defaults to unreadable leaflets, teaspoon units and no interpreter, even excellent individual communication cannot fully protect the family. That is why health-literate care is a system responsibility, not a personal virtue. [7] [10]
Clinical Presentation
Low health literacy rarely announces itself. The clues are indirect, and they usually show up as a consequence of the gap rather than a disclosure of it. Incomplete forms, missed appointments, a dosing error found on review, or a parent who says they left their glasses at home — any of these can be the first signal. [1] [8]
A parent who cannot name their child's medicines or doses is not necessarily low-literacy; they are signalling that an earlier explanation did not land. The same is true for repeated presentations for an easily managed condition. Before labelling a family "non-compliant", ask whether the instructions were ever actually accessible. [8] [9]
The high-yield moments are the ones where information access is decisive. A new liquid-medication prescription, a hospital discharge, a fresh asthma action plan, a new diagnosis, vaccine hesitancy, and adolescent transition are each forks where plain language and teach-back earn their keep. [2] [8]
The adolescent who cannot explain their own condition or action plan at transition is showing an unmet health-literacy need that will resurface as poor self-management. And a parent overwhelmed by a patient portal, or distressed by conflicting online advice, is demonstrating a critical-literacy gap you can help with. [4] [6]
Differential Diagnosis
When a family seems not to have understood, name the obstacle before you repeat yourself louder. Each one has a different fix. [1] [12]
| Surface story | Real obstacle | What to do |
|---|---|---|
| "They didn't understand" | Language barrier, not literacy | Use a professional interpreter; translate materials |
| "They keep getting it wrong" | Numeracy or unit confusion | Switch to mL, oral syringe, pictogram |
| "They missed everything" | Vision or hearing impairment | Large print, audio, captions, communication support |
| "They can't follow the plan" | System complexity, polypharmacy | Simplify the plan; reduce the load |
| "They refused" | Values conflict, fully understood | Treat as a choice, not a literacy failure |
A language barrier is the most common mimic. The parent understands the medicine perfectly but receives it in a language they do not speak fluently — and the fix is an interpreter, not slower English. Anxiety, pain or acute distress can transiently impair anyone's comprehension, so revisit the information once the family is settled. And never confuse a genuine values-based choice with a comprehension failure; some families understood the plan and simply chose differently. [11] [12]
Clinical & Bedside Assessment
You assess understanding, never literacy. Do not test reading skill, and never ask a parent to read something aloud. The whole encounter should be framed so that any family can ask for help without shame. [7] [8]
Open with a shame-free frame that puts the burden on your explanation, not their ability. Say something like: "I give a lot of information and I want to check I explained it clearly — can you tell me back how you'll give the medicine?" That single phrasing turns a test of the parent into a check of your teaching. [5] [7]
Ask about language and format need routinely, not by guessing. "What language do you feel most comfortable speaking about your child's health?" is a better question than "Do you need an interpreter?" — and you record the answer so it follows the child. [12] [10]
Minimum health-literacy-sensitive assessment: [7] [8]
- Frame the teach-back as a check on your explanation. [5]
- Ask the preferred language and record it. [12]
- Ask the parent to demonstrate drawing up and giving a liquid dose with the real tool. [2]
- Quantify plan complexity — how many medicines, how many instructions, how many teams. [8]
- Confirm the safety-net and the return trigger in the family's own words. [1]
Observe the medication moment. Asking a parent to draw up the dose with the actual syringe they will use at home exposes errors you would never catch on paper, and it turns assessment into teaching. [2] [3]
Investigations
There are no blood tests for health literacy. The investigations here are the checks that make information quality visible and repeatable — on your materials, your labels and your system. [7] [1]
- Readability assessment of written materials you hand out, aiming for a grade 5 to 6 reading level. Most default leaflets sit well above this and silently exclude families. [1] [9]
- Label and tool audit at the point of prescribing — confirm the unit is mL, the tool is an oral syringe, and a pictogram is present. [2] [3]
- Communication-need record, mirroring the NHS Accessible Information Standard: identify need, record it, flag it, share it, meet it. [10]
- Plan-complexity review for children with medical complexity, so the burden of information is measured, not assumed. [8]
Formal adult literacy tools exist — the Rapid Estimate of Adult Literacy in Medicine, the Test of Functional Health Literacy in Adults, and the Newest Vital Sign. They are not recommended for routine paediatric screening because of shame, time and the universal-precautions principle. The Newest Vital Sign can be used selectively or in research, but it supplements universal precautions; it never replaces them. [7] [6]
Management — Resuscitation
When a dosing error or a missed critical instruction turns up acutely, secure the child first. Assess and treat the poisoning or the untreated condition before you turn to the communication failure that caused it. [2] [9]
Replace the confusing tool at the bedside immediately. Discard household teaspoons, dispense an oral syringe, relabel the medicine in millilitres, and demonstrate the correct dose with the family watching before they leave the room. A correct tool is treatment. [2] [3]
For any acute discussion with a language-discordant family, use a professional interpreter — in person, by phone or by video. Never rely on a child or a relative to interpret critical safety information; the risk of unsafe miscommunication is real and the breach of confidentiality is avoidable. [12] [11]
Give the safety-net verbally and in an accessible format, then teach-back the warning signs and the return trigger. Do not delay life-saving treatment to run a communication assessment — deliver the essentials in compressed, plain-language form and revisit them fully once the child is stable. [1] [10]
Management — Definitive & Stepwise
Use a structure you can recite under viva pressure. The universal-precautions sequence is the cleanest scaffold, and every step is evidence-informed. [7] [1]
Accessible paediatric information algorithm
Assume difficulty (universal precautions) — apply plain language and teach-back to every family
Use plain language: short sentences, common words, one idea per sentence, define every term
Run teach-back: ask the family to explain or demonstrate the plan in their own words, then re-explain gaps without blame
Dose liquid medicines in millilitres only, dispense an oral syringe, and add a pictogram
Match written materials to a low reading level and offer them in the family's language and format
Build health-literacy-friendly defaults into the system — mL-only templates, standing interpreter orders, readable leaflets
Confirm understanding and a concrete safety-net, and revisit at milestones and transition
Millilitre dosing is the single highest-yield intervention in paediatric health literacy. In a randomised study, pictograms plus millilitre dosing tools reduced parent medication errors, and a label-unit experiment showed parents choose safer tools when the unit is mL. Prescribe in mL, give an oral syringe, and show the dose. That trilogy is examiner gold. [2] [3]
Plain language and teach-back are the daily work. Plain language means short sentences, common words, active voice and one idea at a time; define every medical term at first use or replace it. Teach-back means the family restates the plan in their own words, you fill the gaps, and only then do they leave. A health-literacy-informed rounds and discharge approach improves comprehension and can narrow language-related safety disparities in hospital. [5] [10]
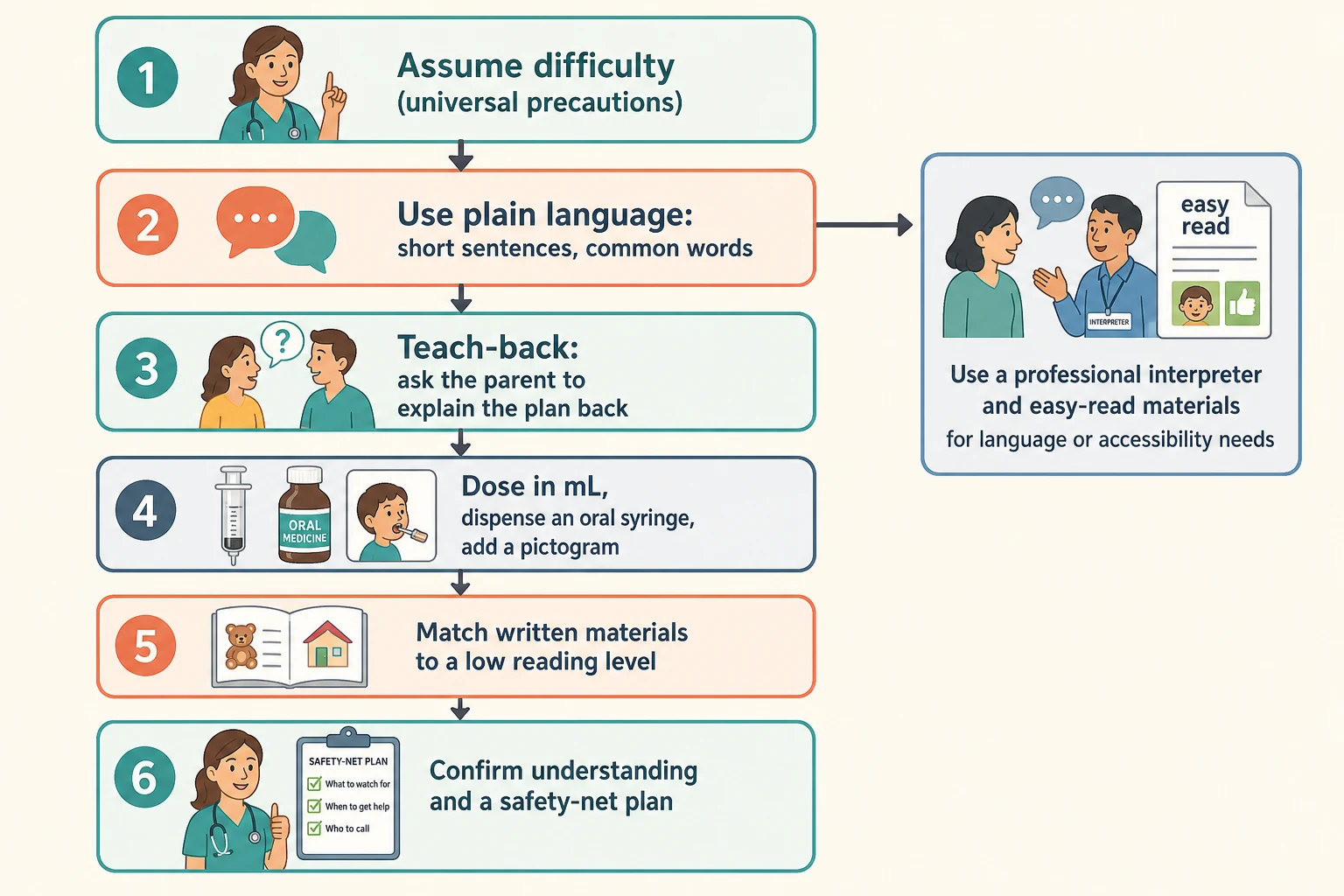
Match the format to the family. Offer materials in the preferred language and in the right format — easy-read for intellectual or learning disability, large print or audio for low vision, captions and interpreter for deaf or hard-of-hearing families. And co-design information with families so the materials you build actually work for the people who use them. [7] [10]
Specific Subtypes & Scenarios
Liquid-medication dosing. Prescribe in mL, dispense a marked oral syringe, and drop teaspoon and tablespoon language entirely — the household teaspoon varies and causes overdose and underdose. Add a pictogram. This one change is the most evidence-supported, highest-yield health-literacy intervention in paediatrics. [2] [3]
Hospital discharge. Most comprehension and adherence errors cluster here. Use plain-language instructions, teach-back the warning signs and the follow-up plan, and confirm the written summary is at the right reading level. Parents commonly overestimate how well they understood discharge instructions, especially when the plan is complex. [8] [10]
Chronic disease. Asthma, diabetes, epilepsy and sickle cell disease are taught to goal over repeat visits. Co-design a simple action plan and check the family can use the device or plan, not merely own it. A health-literacy-informed early-childhood intervention improved obesity-prevention outcomes in a cluster-randomised trial. [4] [1]
Children with medical complexity. These families carry the heaviest information load — polypharmacy, technology dependence, many teams. Standardise, simplify and confirm understanding at every handover, because fragmentation is where the gaps open. [8] [12]
Vaccine communication. Use plain language, acknowledge concerns, share balanced information in an accessible format, and avoid overwhelming the parent. A strong recommendation delivered in plain words builds confidence better than a statistics dump. [1] [6]
Adolescent transition. Teach the young person to explain their own condition, medication and action plan, and appraise online health information critically. Confirmed understanding at transition is the bridge to safe adult care. [4] [6]
Complications & Pitfalls
- Asking "do you understand?" — the universal wrong question; nearly everyone says yes. [5] [8]
- Prescribing liquid medicines in teaspoon or tablespoon units, or without a dosing tool. [2] [3]
- Singling families out for literacy screening by appearance, accent or education — stigmatising and inaccurate. [7]
- Using routine formal literacy tests in clinic, which cause shame and are not recommended in paediatric practice. [6] [7]
- Handing out dense, high-readability leaflets and assuming information given equals information understood. [1] [9]
- Using a child or relative as interpreter for clinical or safety discussions. [12] [11]
- Digital exclusion — assuming every family can use a portal, app or video consultation without checking access. [10]
- Confusing a values-based choice with a comprehension failure and "correcting" a family who simply chose differently. [1]
Prognosis & Disposition
Accessible information measurably improves safety. Pictogram-plus-mL dosing reduces measured dosing errors in randomised study; teach-back and plain language improve comprehension, adherence and appropriate service use. The strongest effects are practical and proximal — the dose, the plan, the warning signs. [2] [5]
The honest framing for an examiner is that accessible communication improves understanding, safety and appropriate service use, and it builds trust that compounds across chronic-disease care and transition. It is not a single-dose cure for disparities driven by upstream determinants, but it is one of the few levers you control at the bedside today. [1] [4]
Disposition is a confirmed-understanding plan: a plain-language summary, a demonstrated dose, a recorded communication need, a concrete safety-net with named warning signs, and a review date. If the family cannot teach the plan back, you have not finished — re-explain, simplify, or arrange an interpreter, and document what you did. [8] [10]
Special Populations
Families with limited English proficiency. Use a trained professional interpreter every time, record the language and dialect, and provide translated materials. Never use a child as interpreter. Language discordance carries measurable inpatient harm, so this is a safety standard. [12] [11]
Families with low health literacy or lower formal education. Universal precautions apply; lead with plain language and teach-back and never assume. Over-the-counter cough-and-cold labels are misinterpreted by a sizeable minority of parents, so confirm even "obvious" instructions. [9] [1]
Children and families with intellectual, learning or developmental disability. Use easy-read formats, teach-to-goal across repeat sessions, and involve support people. [7] [1]
Deaf, hard-of-hearing, blind or low-vision families. Meet the sensory need with interpreters, captions, large print, braille or audio, per your accessible-information duty. [10]
Migrant, refugee and asylum-seeking families. Confirm language and literacy, use interpreters, and check materials are culturally and linguistically appropriate. [11] [12]
Adolescents. Build personal health literacy directly, offer confidential time, and appraise online information together as part of transition. [4] [6]
Families facing socioeconomic disadvantage and digital exclusion. Avoid portal-only pathways, offer non-digital routes, and check the real cost and access of any plan before it becomes a barrier. [10] [1]
Evidence, Guidelines & Regional Differences
Practice anchors: the DeWalt systematic review of health literacy and child health outcomes; the Berkman updated systematic review of low health literacy and health outcomes; the Yin randomised study of pictograms, units and dosing tools; the Yin label-unit experiment; Schillinger's closing-the-loop study of teach-back; the Glick work on discharge-instruction comprehension; and the Khan and Harris studies on language-related safety disparities. [1] [6] [2] [5] [12]
Controversies to handle calmly: whether to screen or to assume universally; how far digital tools widen or close equity; how to resource teach-back under genuine time pressure; and how to measure child and adolescent health literacy robustly. On each, the defensible fellowship position is that universal precautions is the standard, with selective use of tools where they add value. [7] [10]
In Australia, the Australian Commission on Safety and Quality in Health Care embeds health literacy in the National Safety and Quality Health Service Standards, making health-literate communication an organisational requirement rather than a personal nicety. Aotearoa New Zealand frames health literacy as part of equitable, whānau-centred care. Practice plain language, teach-back and interpreter use as standards, and use the Ophelia approach to co-design services with communities. [1]
Exam Pearls
PLAINRx
References
- [1]DeWalt DA, Hink A Health literacy and child health outcomes: a systematic review of the literature. Pediatrics, 2009.PMID 19861480
- [2]Yin HS, Parker RM, Sanders LM, Mendelsohn AL, Dreyer B, Bailey SC, ... Wolf MS Pictograms, Units and Dosing Tools, and Parent Medication Errors: A Randomized Study. Pediatrics, 2017.PMID 28759396
- [3]Yin HS, Parker RM, Sanders LM, Dreyer BP, Mendelsohn AL, ... Wolf MS Effect of Medication Label Units of Measure on Parent Choice of Dosing Tool: A Randomized Experiment. Academic pediatrics, 2016.PMID 27155289
- [4]Sanders LM, Perrin EM, Yin HS, Bronaugh A, Beatson B, ... Cox JE A Health-Literacy Intervention for Early Childhood Obesity Prevention: A Cluster-Randomized Controlled Trial. Pediatrics, 2021.PMID 33911032
- [5]Schillinger D, Piette J, Grumbach K, Wang F, Wilson C, Daher C, Leong-Grotz K, Castro C, Bindman AB Closing the loop: physician communication with diabetic patients who have low health literacy. Archives of internal medicine, 2003.PMID 12523921
- [6]Berkman ND, Sheridan SL, Donahue KE, Halpern DJ, Crotty K Low health literacy and health outcomes: an updated systematic review. Annals of internal medicine, 2011.PMID 21768583
- [7]DeWalt DA, Broucksou KA, Hawk V, Berkman ND, Schillinger D, ... Huezo-Medina TB Developing and testing the health literacy universal precautions toolkit. Nursing outlook, 2011.PMID 21402204
- [8]Glick AF, Farkas JS, Rosenberg RE, Mendoza-Fernandez A, Kumar S, ... Yin HS Accuracy of Parent Perception of Comprehension of Discharge Instructions: Role of Plan Complexity and Health Literacy. Academic pediatrics, 2020.PMID 31954854
- [9]Lokker N, Sanders L, Perrin EM, Kumar D, Hea V, Cyna-Amerlian K, ... Rothman N Parental misinterpretations of over-the-counter pediatric cough and cold medication labels. Pediatrics, 2009.PMID 19482755
- [10]Rajbhandari P, VanGeest J, Grossoehme DH, Zhang M, ... Glick AF Hospitalists' Practices and Barriers to Health-Literate Communication in Pediatric Inpatient Care. Hospital pediatrics, 2026.PMID 41921989
- [11]Harris LM, Dreyer BP, Mendelsohn AL, Bailey SC, Sanders LM, ... Yin HS Liquid Medication Dosing Errors by Hispanic Parents: Role of Health Literacy and English Proficiency. Academic pediatrics, 2017.PMID 28477800
- [12]Khan A, Yin HS, Brach C, Cerra ME, Lerner C, ... for the HOMERUN Network Association Between Parent Comfort With English and Adverse Events Among Hospitalized Children. JAMA pediatrics, 2020.PMID 33074313