Paeds · professional-practice-and-evidence
Implementation science and translating evidence into practice
Also known as Implementation science paediatrics · Translating evidence into child health practice · Knowledge translation in paediatrics · Research-to-practice gap child health · CFIR and RE-AIM in paediatric care
Fellowship guide to implementation science: the research-to-practice gap, why evidence takes about 17 years to reach children, the frameworks (CFIR, RE-AIM, Cabana, knowledge-to-action), Proctor implementation outcomes, the ERIC strategy compilation, designing and judging paediatric implementation projects, and defending evidence and equity at viva.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A paediatric emergency department has a sepsis guideline that works — proven by trials, endorsed by the college — yet only half of eligible children receive the first antibiotic within the recommended hour. A community mental health service offers a therapy shown to halve adolescent depression, yet most young people get something looser instead. These are not research failures and they are not single errors; they are implementation failures, the gap between what we know and what we actually do. This leaf teaches you how to close that gap for children. The deeper evidence appraisal lives on the EBM page and the PDSA change engine on the quality-improvement page; this leaf is about moving proven practice into routine use. [1] [9]
Implementation science is the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine care. Bauer and colleagues frame it for the non-specialist as a young, method-driven field that grew up precisely because publishing a guideline was never enough to change practice. [1]
The central fact that justifies the whole discipline is the time lag. Morris, Wooding and Grant estimated that it takes about seventeen years for original research to reach routine practice, and that even then only a minority of evidence is fully adopted. For a child born today, that is an entire generation of preventable under-treatment. This is the problem implementation science exists to solve. [2]
Classification
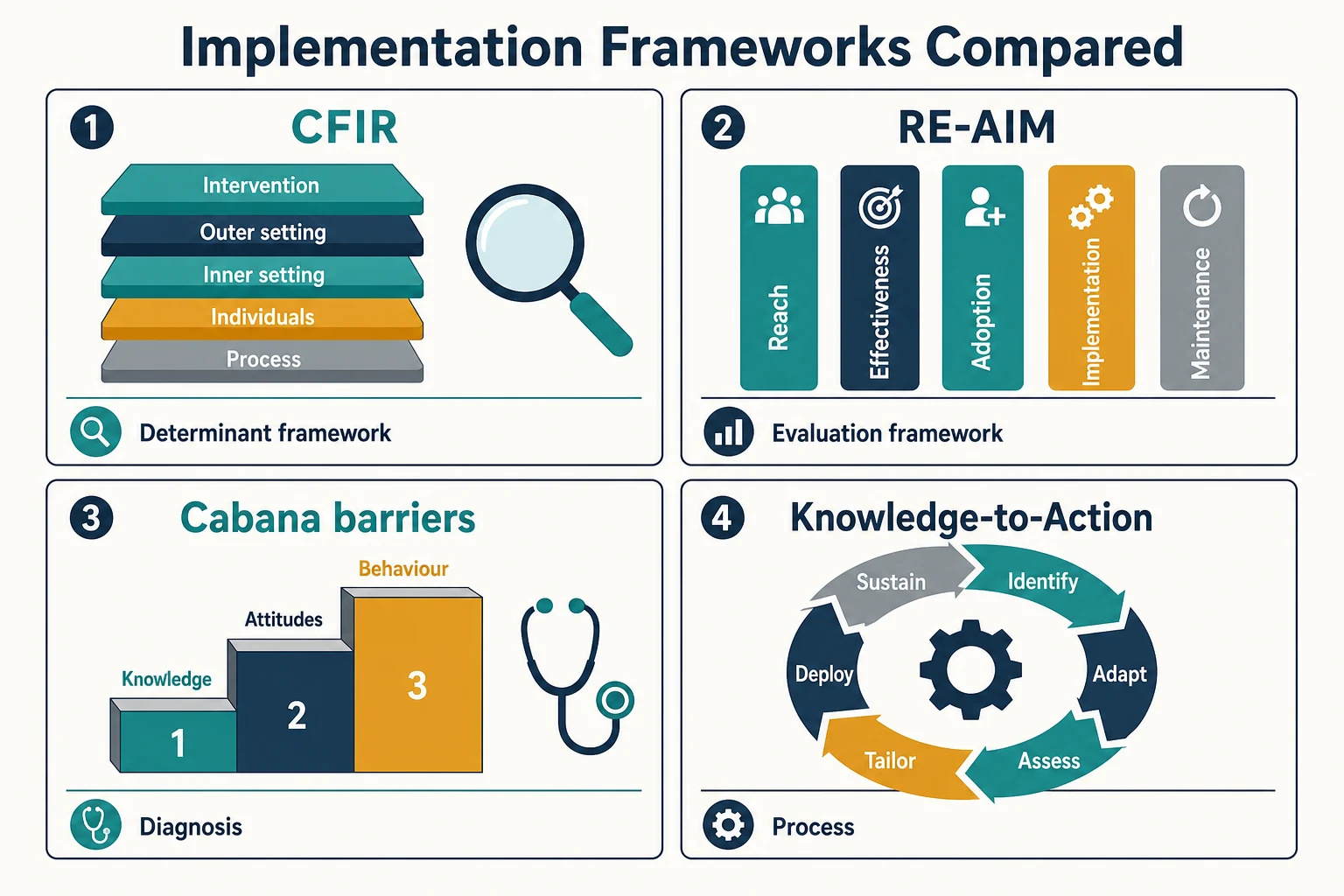
Implementation science has grown a crowded toolbox of frameworks, and a candidate who treats them as interchangeable will founder at viva. Classify them by the job they do, and the field becomes navigable. Tabak and colleagues catalogued over sixty models and grouped them by whether they are used to understand what determines success, to do the implementation, or to evaluate it afterward. [10]
A determinant framework (the best known is CFIR) does not tell you what to do; it tells you what to look at. It lists the factors — features of the intervention, the inner and outer setting, the people and the process — that determine whether an evidence-based practice will take hold. A process framework like the knowledge-to-action cycle gives you a sequence to follow: identify the gap, adapt the evidence to context, assess barriers, choose and tailor a strategy, deploy it, measure, sustain. An evaluation framework like RE-AIM tells you how to judge the result: did it reach the children who needed it, did it work, was it adopted, delivered with fidelity, and maintained? [4] [5] [10]
The other half of classification is the outcome. Proctor and colleagues drew a line that examiners love because it explains why projects fail silently. An intervention can have a perfectly good clinical outcome (children get better) and a failed implementation outcome (the staff never adopted it, or delivered it badly, or dropped it after the grant ended). Naming the implementation outcome separately is what lets you diagnose and fix. [7]
The four frameworks you must be able to place
- Determinant framework — tells you what to assess
- Five domains: intervention, outer setting, inner setting, individuals, process
- Use it before you choose a strategy
- Evaluation framework — tells you how to judge
- Reach, Effectiveness, Adoption, Implementation, Maintenance
- Best for estimating public health impact
- Diagnostic framework — tells you why staff are not following a guideline
- Three tiers: knowledge, attitudes, behaviour/external
- Maps each barrier to a strategy
- Process framework — tells you the sequence
- Identify, adapt, assess, tailor, deploy, sustain
- A cycle, not a checklist
Epidemiology & Risk Factors
The size of the evidence-practice gap in child health is sobering. Children receive the recommended care only about half the time across common conditions, and the lag is measured in years rather than months. Morris and colleagues put the typical delay at around seventeen years from evidence generation to routine use, and noted that even at the end of that wait much of the evidence remains incompletely applied. The corollary is that a better guideline changes nothing on its own — only implementation moves the curve. [2]
The gaps cluster where the evidence is newest, the population is least studied, or the system is hardest to change. Child and adolescent mental health carries one of the largest reach gaps: a minority of young people who need an evidence-based therapy receive one, and those who do often get a diluted version. Sepsis bundle timing, asthma discharge planning, ADHD medication monitoring and antibiotic stewardship all show proven interventions applied inconsistently across units. [1] [9]
The risk that an intervention will fail to take hold is predictable from Greenhalgh's systematic review of how innovations spread through service organisations. It depends on properties of the innovation itself (is it a clear relative advantage, is it simple enough to trial, can it be adapted), the people who must adopt it, the team and its leadership, and the wider system. A therapy that is brilliant but hard to pilot, or a guideline that conflicts with ingrained workflow, will stall regardless of the evidence behind it. [6]
Children add their own risk factors. They are under-represented in the trials that generate the evidence to be implemented, so paediatric guidelines often extrapolate from adults and inherit implementation uncertainty. Weight-based dosing multiplies the points at which a protocol can be delivered wrongly. Rural and remote units face low volumes and thin staffing that slow adoption, and equity gaps widen when reach is not measured by subgroup — Indigenous, migrant and disadvantaged children are the ones most often left behind by an improving average. [1] [11]
Pathophysiology
How does a therapy proven in a trial fail to reach a real child? Through a cascade with several places to break. The evidence must first be synthesised into a guideline, the guideline must reach the clinician, the clinician must agree with it, the clinic must be set up to deliver it, the team must actually deliver it as designed, and the delivery must persist over time. A break at any link loses the child. Implementation science studies each link deliberately rather than hoping the chain holds. [1] [3]
Cabana's framework is the most useful way to diagnose why a specific guideline is not followed, and it works because it refuses to stop at "they don't care". Cabana and colleagues decomposed non-adherence into three tiers. The first is knowledge: the clinician may simply lack awareness of the guideline or familiarity with its content. The second is attitudes: the clinician may not agree with it, may lack self-efficacy, may doubt it will help, or may be caught in the inertia of previous practice. Only then comes behaviour and external barriers — the guideline is unwieldy, the patient refuses, the environment lacks the staff or the system to support it. Each tier calls for a different strategy, which is the whole point. [3]
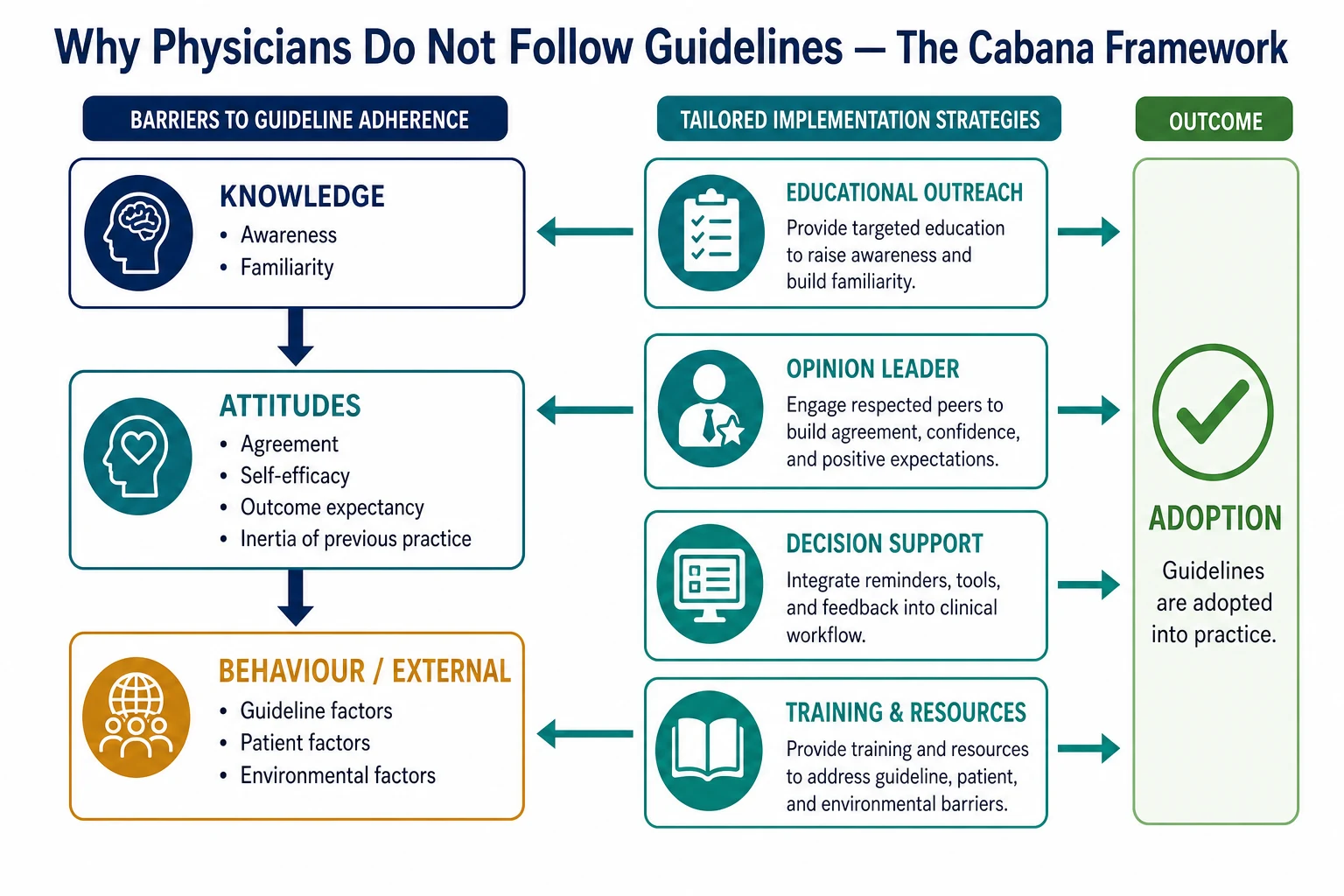
This is why an untargeted strategy so often fails. An educational lecture is the right answer to an awareness barrier and the wrong answer to an environmental one; if the real obstacle is that the clinic has no space for the therapy, more lectures change nothing. Grimshaw, Eccles and Lavis synthesised the evidence on knowledge-translation strategies and found that tailored, multifaceted approaches generally outperform single passive ones, but a strategy works only when it acts on the barrier that is actually blocking the link. [9]
Context is the second pathophysiology lesson, and CFIR exists to make it explicit. A complex intervention that thrived in one neonatal unit may fail next door because the inner setting differs — a different leadership, a different culture, less access to information, fewer engaged champions. CFIR's five domains (intervention characteristics, outer setting, inner setting, characteristics of individuals, and process) are precisely the levers that determine whether an evidence-based practice will adapt or die when it moves. Ignoring context is the most common reason a copied intervention disappoints. [4]
Clinical Presentation
An implementation problem rarely arrives labelled as one. What you actually see is a child who should have received a proven therapy and did not, an audit showing a guideline applied in only half of cases, a successful pilot that never left its original ward, or a service where a therapy is "offered" but delivered so variably that the children barely benefit. The presentation is a signal that the chain from evidence to child has broken somewhere, and the skill is to find the link. [1] [3]
A failing implementation project has a recognisable shape too. It selected a strategy before assessing the barriers. It measured whether children improved (a clinical outcome) but never whether the staff actually adopted the practice (an implementation outcome), so when nothing changed no one knew why. It has no fidelity check, so it cannot tell a therapy that does not fit from a therapy that is delivered badly. And it has no plan for what happens after the enthusiastic registrar rotates — so the gains decay. [7]
Inequitable reach is the presentation that is easiest to miss. The unit average looks fine, but when the data are disaggregated, the Indigenous children, the children with interpreters, the children from the poorest postcodes never received the intervention at all. An implementation that lifts the average while leaving a subgroup behind has widened a gap, and spotting that pattern is a viva merit point. [1]
Resistance deserves a careful read. A clinician who pushes back on a new pathway may be voicing a legitimate context barrier — the pathway genuinely does not fit their workflow — or may simply be in the inertia Cabana named. Distinguishing the two is clinical judgement: investigate the first, address the second. Dismissing all resistance as inertia loses the signal that the intervention is a poor fit. [3]
Differential Diagnosis
The viva most often asks you to separate implementation science from its close cousins, because the terms are used loosely and the right method depends on the right diagnosis. [1] [9]
- Implementation science versus quality improvement. QI tests small local changes to move practice toward a better state using PDSA cycles and run charts; implementation science studies the systematic methods that get proven practices adopted and sustained. QI asks "how do we make this better here, now?"; implementation science asks "how do we reliably get this known-effective practice into routine use?" They overlap and reinforce, but the centre of gravity differs. [1]
- Implementation science versus clinical research. Research generates generalisable new knowledge for a population; implementation science gets existing knowledge into the hands and habits of the clinicians who treat these children. [1]
- Dissemination versus implementation. Dissemination spreads information; implementation changes behaviour. A published guideline is dissemination; a re-engineered workflow that delivers it is implementation. The distinction is the single most tested idea on this leaf. [9]
- Determinant versus evaluation framework. CFIR helps you understand what determines success; RE-AIM helps you evaluate the result. Use CFIR before, RE-AIM after. [4] [5]
- Adoption versus fidelity versus sustainment. Adoption asks whether the unit took up the practice; fidelity asks whether they delivered it as intended; sustainment asks whether it lasted. A project can succeed on one and fail on another. [7]
- Implementation outcome versus clinical outcome. The child improving is a clinical outcome; the staff adopting, delivering with fidelity, and persisting are implementation outcomes. Proctor's taxonomy separates them so a silent failure can be named and fixed. [7]
Clinical & Bedside Assessment
Before you choose a single strategy, assess the problem as you would assess a child: take a structured history and examine the context. Start by naming the specific evidence-practice gap and its magnitude. "Our sepsis bundle is delivered late" is a complaint; "in the last quarter, only 52% of eligible children received the first antibiotic within one hour" is a gap you can act on. The size of the gap is the case for change. [3]
Examine the context with CFIR as your structure. Who leads the unit, and do they champion evidence-based practice? What is the culture around change and failure? Is there data infrastructure, protected time, engaged clinicians? Are there opinion leaders whose endorsement would carry weight? Aarons and colleagues showed that unit-level implementation leadership — a leader who is proactive, knowledgeable, supportive and perseverant — measurably predicts adoption, so assessing leadership is not soft; it is diagnostic. [4] [11]
Assess the barriers with the Cabana framework. Talk to the clinicians who would deliver the practice and ask where it breaks down: do they know it exists (knowledge), do they believe in it (attitudes), can the clinic actually support it (behaviour/external)? A short round of structured interviews or a survey will tell you whether the real obstacle is awareness, agreement or environment far more reliably than guessing. [3]
Engage families and children as partners in the assessment, not just as recipients. A family can tell you that the pathway fails at discharge handover, or that the therapy feels culturally unsafe, in a way no chart audit will reveal. An implementation designed around clinician assumptions but never tested with families will founder on exactly the barrier no one measured. [1]
Finally, observe whether the practice is currently delivered with fidelity before you try to spread it. Walk the ward and watch. A "successful" pilot that has already drifted from the original protocol cannot be scaled honestly until you know what was actually delivered. [7]
Investigations
In implementation, the "investigations" are the measurement plan, and Proctor's outcome taxonomy is the scaffold. Proctor and colleagues separated implementation outcomes — acceptability, adoption, appropriateness, feasibility, fidelity, implementation cost, penetration and sustainability — from the service outcomes (efficiency, safety) and clinical outcomes (symptom relief, survival) that depend on them. Measuring all three layers lets you explain a project that failed to help children: was the practice never adopted, delivered without fidelity, or genuinely ineffective here? [7]
ACCEPTS+
Fidelity is the single most neglected measure and the one examiners probe. Fidelity is the degree to which a practice is delivered as it was designed, and without it you cannot distinguish a therapy that does not work in this context from one that was simply delivered badly. Operationalise it: list the key components of the practice, define what "delivered as intended" looks like for each, sample it, and track drift over time. [7]
Use RE-AIM as your quantitative frame for impact. Reach is the proportion of eligible children who receive the intervention, broken down by subgroup so an equity gap is visible. Effectiveness is whether it works in the real world, not only the trial. Adoption is the proportion of settings and clinicians who take it up. Implementation captures fidelity, cost and adaptation at delivery. Maintenance asks whether the effect persists over time. Glasgow and colleagues built RE-AIM precisely so a programme could look good on one dimension and fail on another. [5]
Study design matters for implementation questions in a way the EBM page covers more deeply. The hybrid designs that Curran described are the headline: a Type I trial tests clinical effectiveness with implementation secondary; a Type II tests both together; a Type III tests the implementation strategy itself, with clinical effectiveness assumed. Stepped-wedge and cluster-randomised designs suit settings where you cannot randomise individual children. Choose the design that matches the question you actually have. [9] [10]
Management — Resuscitation
When a proven practice is failing at the bedside and children are being harmed now, the immediate job is to charter the response and protect the team. State the gap and the harm it is causing in plain terms so the case for change is unanswerable, then assemble a multidisciplinary team that includes the clinicians who will deliver the practice, a senior sponsor who will protect their time, and a family partner. Secure a reliable baseline showing the size of the gap before anything else, because without a baseline you cannot prove the change worked. [1] [9]
Frame the problem as a system gap, never a blame question. A sepsis antibiotic that is late is almost never a lazy clinician; it is a workflow, staffing or decision-support failure. A blame framing drives the problem underground and destroys the psychological safety that implementation needs. Align the urgent effort with existing governance — the quality committee, the incident pathway, the sepsis lead — so it is supported rather than competing. [6]
Build in an equity check from the first day. Decide now that reach will be measured by subgroup, so that when the average improves you will know whether Indigenous, migrant and disadvantaged children improved with it. An implementation that lifts the average while leaving the most vulnerable behind is not a success, and the only way to know is to measure from the outset. [1]
Finally, agree how to fail fast. If an early strategy is not working, the disciplined move is to adapt or abandon it quickly, not to push through on principle. A safety-net — a named owner and a review date — ensures the work does not silently die when attention moves on. [8]
Management — Definitive & Stepwise
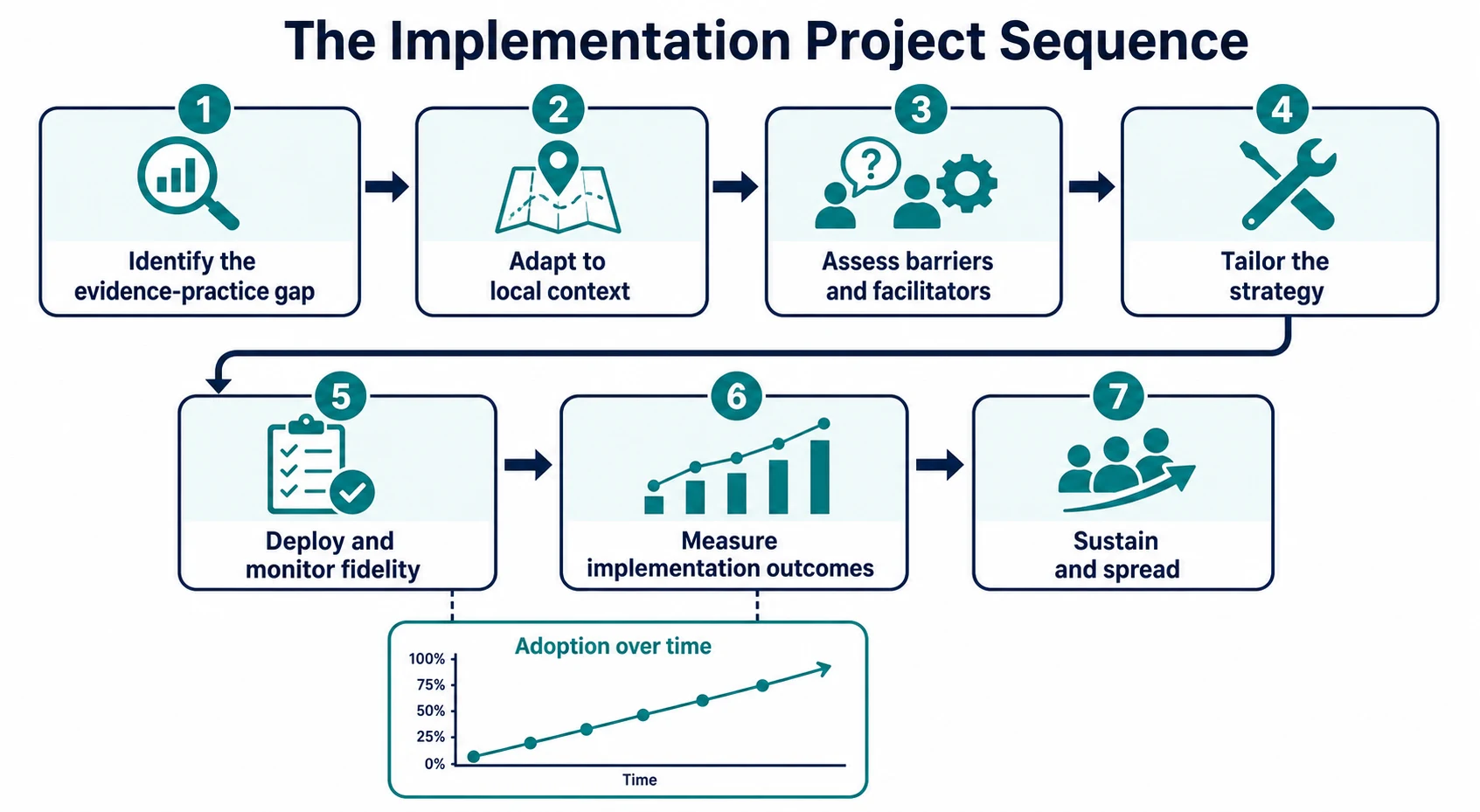
The definitive method is the knowledge-to-action cycle, and it is best read as a sequence that loops. First, identify the evidence-practice gap and the evidence that should close it. Second, adapt that evidence to the local context — a protocol copied verbatim rarely fits a real clinic, and adaptation is legitimate as long as it is deliberate and documented. Third, assess the barriers and facilitators using CFIR and Cabana so you know what you are working against. Fourth, tailor and select strategies from the ERIC compilation that act on those specific barriers. Fifth, deploy and monitor fidelity as the practice goes live. Sixth, measure the implementation outcomes (Proctor) and the impact (RE-AIM). Seventh, sustain and spread. The cycle then repeats at a higher level. [3] [8] [10]
Strategy selection is where candidates panic and need not. Powell and colleagues, through the Expert Recommendations for Implementing Change (ERIC) project, compiled seventy-three discrete implementation strategies and clustered them into families: planning, educating, financing, restructuring, managing quality, and policy. The skill is not to memorise all seventy-three but to map a diagnosed barrier to the right family. An awareness barrier calls for educational strategies and clinical opinion leaders; an attitude barrier calls for local champions and consensus; an environmental barrier calls for workflow redesign and decision support; a sustainability barrier calls for finance and policy levers. [8]
Build a strategy bundle that is multifaceted but parsimonious. The older dogma that more strategies are always better has not held up; Grimshaw's synthesis found that a few well-targeted strategies matched to assessed barriers usually beat a pile of untargeted ones, and an over-bundled strategy fatigues the team. Choose two or three strategies that each address a named barrier, deploy them together, and watch for alert fatigue and overload. [9]
Running an implementation project — practical sequence
Identify the evidence-practice gap and quantify its size
Adapt the proven practice to the local context deliberately
Assess barriers and facilitators with CFIR and Cabana
Map each barrier to an ERIC strategy; build a parsimonious bundle
Deploy with fidelity monitoring from day one
Measure implementation outcomes (Proctor) and impact (RE-AIM)
Plan sustainability with an owner, data and policy levers; then spread
Sustainability is planned from the outset, never hoped for at the end. Assign a named owner, keep the fidelity and outcome data flowing, build the practice into policy, order sets and orientation so it survives staff turnover, and engage finance and governance so the work has a home. Spread a local success to other units only after fidelity and impact are proven, and report it with the StaRI or SQUIRE standards so others can appraise, adapt and adopt. [6] [8]
Specific Subtypes & Scenarios
Paediatric sepsis bundle. Sepsis is the archetype implementation problem: the bundle is proven, yet time-to-antibiotic lags because triage, weighing, escalation and pharmacy each offer a place to break. A barrier assessment usually lands on environment and behaviour: no pre-mixed weight-based antibiotics, unclear escalation triggers, decision support buried in the record. Tailored strategies — a sepsis trolley, an opinion-led escalation pathway, a visible time-stamp — act on those barriers, and fidelity is measured as the proportion delivered as a complete bundle within the hour. [3] [9]
Child and adolescent mental health. Evidence-based therapies for depression, anxiety and trauma exist, yet reach only a minority of young people, and those who do access care often receive a diluted version. The reach gap is the headline implementation failure of the field. Closing it demands workforce training, supervision to protect fidelity, and measurement of whether the therapy is delivered as designed — not merely whether it is "offered". [1] [11]
ADHD in primary care. Guidelines for diagnosis, medication initiation and monitoring are well established, yet adherence is patchy. Cabana's framework was built on exactly this problem, and the recurring barriers are attitudes (familiarity, agreement, outcome expectancy) and behaviour (visit time, follow-up systems). Strategies of audit and feedback, clinical decision support and local opinion leaders move primary care toward the guideline. [3]
Developmental screening in primary care. Tools such as the Modified Checklist for Autism in Toddlers (M-CHAT) and the Ages and Stages Questionnaire (ASQ) are validated, yet adoption stalls when the workflow has no place for them. This is an inner-setting and process problem in CFIR terms, solved by embedding screening at the scheduled health-supervision visit and building a referral pathway so a positive screen does not dead-end. [4] [6]
Antibiotic stewardship in newborns and children. Criteria-based review of antibiotic duration is proven to reduce unnecessary exposure, yet sustaining it needs a stewardship strategy (audit and feedback, pharmacist-led review, criteria embedded in the record) and a balancing measure to detect under-treatment. The implementation outcome — adoption and fidelity of the review — is what sustains the clinical gain. [9]
Family-integrated care in neonatal units. Moving care toward parents changes the inner setting deeply, and its success depends on leadership and culture (CFIR inner setting and individuals). Implementation leadership, as Aarons showed, is a measurable predictor: a unit leader who is proactive and perseverant makes the difference between a practice that sustains and one that fades. [4] [11]
Telehealth-enabled implementation in rural and remote child health. Distance is an outer-setting barrier that no educational strategy alone can fix. Telehealth, hub-and-spoke mentoring and shared data across sites let a proven practice reach children it otherwise could not, and the reach dimension of RE-AIM becomes the primary metric. [5] [10]
Equity-focused implementation. An intervention that improves the average while leaving Indigenous, migrant or disadvantaged children behind has widened a gap. Equity-focused implementation makes reach-by-subgroup an explicit aim and chooses strategies — culturally safe design, community partnership, interpreter-integrated delivery — that close rather than open the gap. [1]
Complications & Pitfalls
- Choosing a strategy before assessing barriers. A one-size-fits-all educational push is the classic error; it works only when awareness is the actual barrier, which is often not the case. [3]
- Dissemination mistaken for implementation. Publishing a guideline and assuming behaviour will change changes almost nothing. [9]
- No implementation outcome measured. Measure the clinical outcome alone and a silent failure is invisible — you cannot explain why the project did not work. [7]
- No fidelity measure. Without fidelity you cannot tell a therapy that is a poor fit from one delivered badly; both look like "it didn't work". [7]
- No sustainability plan. Adoption decays the moment the champion rotates; gains vanish within months. [6]
- Equity blind spot. The average reaches its target while a disadvantaged subgroup is untouched, widening a gap under cover of success. [1]
- Pilot-itis. A stream of small, successful, well-funded pilots that never scale into routine care. [9]
- Over-bundling. Stacking every available strategy fatigues and overwhelms the team; a parsimonious bundle matched to barriers beats a strategy pile-up. [8]
- Ignoring context. Assuming an intervention that worked elsewhere will work identically here ignores CFIR and Greenhalgh's evidence that context governs transfer. [4] [6]
- Hawthorne effect. Attributing a change to the strategy when it is really novelty and attention; the effect fades when the project ends. [9]
Prognosis & Disposition
An evidence-based practice sustains when leadership owns it, the data keep flowing, it fits the context, and a named owner carries it past the project phase. When any one of these weakens, adoption decays — often within months of the champion's departure. Aarons made implementation leadership measurable precisely because it predicts which units sustain and which do not, so leadership is a prognostic factor you can assess in advance. [6] [11]
A project is "done" when adoption, fidelity and sustainment targets are met equitably across subgroups — not when the team presents at a conference. Define those targets at the outset so the finish line is honest. When a project does not improve adoption, the disciplined response is to diagnose rather than to hide: was the barrier assessment wrong, was the strategy mismatched, was the context not ready, or is the practice itself a poor fit here? Re-assess, re-tailor, or abandon honestly. [3] [8]
Spread follows proven local success. Scale the practice only after fidelity and impact are established, and report with StaRI or SQUIRE so other teams can appraise and adapt it. The long-term value of this work is not any single project but the implementation capacity it builds into the workforce — clinicians who know how to move evidence into practice become a compounding asset. [9]
Special Populations
Neonates carry the sharpest stakes: weight-based sepsis and stewardship bundles multiply the points at which a protocol can be delivered wrongly, and family-integrated care changes the inner setting so deeply that leadership is decisive. Children with medical complexity concentrate implementation risk through polypharmacy, devices and fragmented teams, so an evidence-based practice must reach every clinician in the chain, not just the primary one. [4] [11]
Indigenous children need equity-focused, culturally safe implementation — an intervention designed without community partnership may reach the population on paper while being refused or adapted away in practice. Rural and remote children face the outer-setting barrier of distance, addressed by telehealth, hub-and-spoke mentoring and shared data. Migrant and refugee families need interpreter-integrated delivery so the practice reaches the child rather than stopping at the language barrier. [1] [5]
Children and adolescents with mental health needs face the largest reach gap of any child-health domain; closing it is a workforce, supervision and fidelity problem more than a knowledge problem. Children with disability and neurodiversity need accessible evidence-based practices and family-reported outcomes that capture what matters to them. Out-of-home care and socioeconomically disadvantaged children need context-aware implementation that closes rather than widens gaps, because an improving average is the most common way equity silently fails. [1] [7]
Evidence, Guidelines & Regional Differences
The evidence base for implementation science is genuine, though it carries caveats the viva expects. Morris established the seventeen-year time-lag that justifies the whole field. Cabana built the barriers framework that remains the most useful bedside diagnosis of non-adherence. Greenhalgh's systematic review of how innovations diffuse through service organisations grounded the field in real health-service complexity, and showed that adoption depends on the innovation, the people, the team and the system together. [2] [3] [6]
The frameworks themselves are evidence products. Damschroder consolidated the determinants into CFIR; Glasgow built RE-AIM to estimate public health impact; Proctor drew the implementation-outcome line that lets silent failures be named; Powell compiled the ERIC strategy catalogue that turns a diagnosed barrier into an actionable choice; and Tabak catalogued over sixty models so the field could be navigated. Grimshaw, Eccles and Lavis synthesised the evidence on knowledge-translation strategies and tempered the "more is always better" dogma: tailored strategies matched to barriers usually beat untargeted bundles. [4] [5] [7] [8] [9] [10]
The honest caveat is that the field's predictive power is still maturing. Frameworks organise thinking but do not yet reliably guarantee success; multifaceted strategies are not always superior to a single well-targeted one; before-after evaluation is weak and the Hawthorne effect confounds it; and context frequently defeats an intervention copied from elsewhere. A candidate who states these caveats calmly is far stronger than one who oversells the method. [9]
The Australian Commission on Safety and Quality in Health Care and the Health Quality & Safety Commission promote evidence-based care and clinical-practice-guideline implementation. Cite the principle of locally adapted, equity-aware, sustained implementation rather than inventing mandated adoption quotas. [1]
Controversies that earn viva credit: how much implementation work needs formal research oversight; whether frameworks predict outcomes or merely describe them; how to publish negative implementation so others learn; and how to evaluate a complex intervention that the team has legitimately adapted. Answer with principles and honest caveats, not slogans. [6] [9]
Exam Pearls
- Implementation science = the scientific study of methods to promote the systematic uptake of research findings into routine practice. [1]
- It takes about seventeen years for research to reach practice, and even then a minority is fully adopted. [2]
- Dissemination spreads information; implementation changes behaviour — the most-tested distinction. [9]
- Cabana barriers: knowledge (awareness, familiarity), attitudes (agreement, self-efficacy, outcome expectancy, inertia of previous practice), behaviour/external (guideline, patient, environment). [3]
- CFIR five domains: intervention characteristics, outer setting, inner setting, characteristics of individuals, process. [4]
- RE-AIM: Reach, Effectiveness, Adoption, Implementation, Maintenance. [5]
- Proctor implementation outcomes: acceptability, adoption, appropriateness, feasibility, fidelity, cost, penetration, sustainability. [7]
- ERIC = Expert Recommendations for Implementing Change; seventy-three compiled strategies in Powell 2015. [8]
- Hybrid designs: Type I tests effectiveness, Type II tests both, Type III tests implementation. [10]
- Fidelity separates a therapy that does not fit from a therapy delivered badly — measure it or you cannot tell. [7]
References
- [1]Bauer MS, Damschroder L, Hagedorn H, Smith J, Kilbourne AM An introduction to implementation science for the non-specialist. BMC Psychology, 2015.PMID 26376626
- [2]Morris ZS, Wooding S, Grant J The answer is 17 years, what is the question: understanding time lags in translational research. Journal of the Royal Society of Medicine, 2011.PMID 22179294
- [3]Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud PA, Rubin HR Why don't physicians follow clinical practice guidelines? A framework for improvement. JAMA, 1999.PMID 10535437
- [4]Damschroder LJ, Aron DC, Keith RE, Kirsh SR, Alexander JA, Lowery JC Fostering implementation of health services research findings into practice: a consolidated framework for advancing implementation science. Implementation Science, 2009.PMID 19664226
- [5]Glasgow RE, Vogt TM, Boles SM Evaluating the public health impact of health promotion interventions: the RE-AIM framework. American Journal of Public Health, 1999.PMID 10474547
- [6]Greenhalgh T, Robert G, Macfarlane F, Bate P, Kyriakidou O Diffusion of innovations in service organizations: systematic review and recommendations. Milbank Quarterly, 2004.PMID 15595944
- [7]Proctor E, Silmere H, Raghavan R, Hovmand P, Aarons G, Bunger A, Griffey R, Hensley M Outcomes for implementation research: conceptual distinctions, measurement challenges, and research agenda. Administration and Policy in Mental Health, 2011.PMID 20957426
- [8]Powell BJ, Waltz TJ, Chinman MJ, Damschroder LJ, Smith JL, Matthieu MM, Proctor EK, Kirchner JE A refined compilation of implementation strategies: results from the Expert Recommendations for Implementing Change (ERIC) project. Implementation Science, 2015.PMID 25889199
- [9]Grimshaw JM, Eccles MP, Lavis JN, Hill SJ, Squires JE Knowledge translation of research findings. Implementation Science, 2012.PMID 22651257
- [10]Tabak RG, Khoong EC, Chambers DA, Brownson RC Bridging research and practice: models for dissemination and implementation research. American Journal of Preventive Medicine, 2012.PMID 22898128
- [11]Aarons GA, Ehrhart MG, Farahnak LR The Implementation Leadership Scale (ILS): development of a brief measure of unit level implementation leadership. Implementation Science, 2014.PMID 24731295