Paeds · professional-practice-and-evidence
Interpreting systematic reviews and clinical guidelines
Also known as Critical appraisal of systematic reviews and meta-analyses · Reading a forest plot and the PRISMA flow diagram · Appraising clinical practice guidelines with AGREE II · AMSTAR-2 and ROBIS for systematic reviews · GRADE Evidence-to-Decision and recommendation strength
Fellowship guide to interpreting systematic reviews, meta-analyses, network meta-analyses, and clinical practice guidelines in child health: reading the PRISMA 2020 flow and a forest plot, quantifying heterogeneity with I-squared, appraising a review with AMSTAR-2 and ROBIS, appraising a guideline with AGREE II, moving from GRADE certainty to recommendation with the Evidence-to-Decision framework, and judging applicability to the child — with ANZ, UK, US and Canada guidance.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Read a systematic review in the right order
Overview & Definition
A parent hands you a printout of a meta-analysis that claims a preventive therapy halves the risk of their child's chronic illness, and a leaflet from a guideline body that recommends the same drug. Before you answer the clinical question, you face an evidence question: can the synthesis and the guideline be trusted, how large is the effect in absolute terms, and do the children in the studies look anything like yours. [10]
A systematic review answers a focused clinical question by assembling, appraising, and — when the studies are similar enough — pooling all the relevant evidence, using methods that another team could reproduce. A meta-analysis is the statistical pooling that may sit inside a systematic review; not every systematic review pools, and not every pooled number is justified. A clinical practice guideline turns the body of evidence into recommendations for practice, through a transparent process that names the certainty of the evidence and the strength of each recommendation. [1] [11]
This page owns the interpretation of synthesised evidence and of guidelines. The five-step engine of evidence-based practice, the PICO question, and the appraisal of single studies with RoB 2, ROBINS-I, and QUADAS-2 belong to the dedicated evidence-based medicine leaf, and the underlying statistics belong to the biostatistics and clinical epidemiology leaves. Read this page as the layer above them: what to do when the evidence arrives already pooled or already turned into a recommendation. [10]
Classification
Sort the evidence you find by the kind of synthesis it is, then match each kind to the appraisal tool it demands. [1] [10]
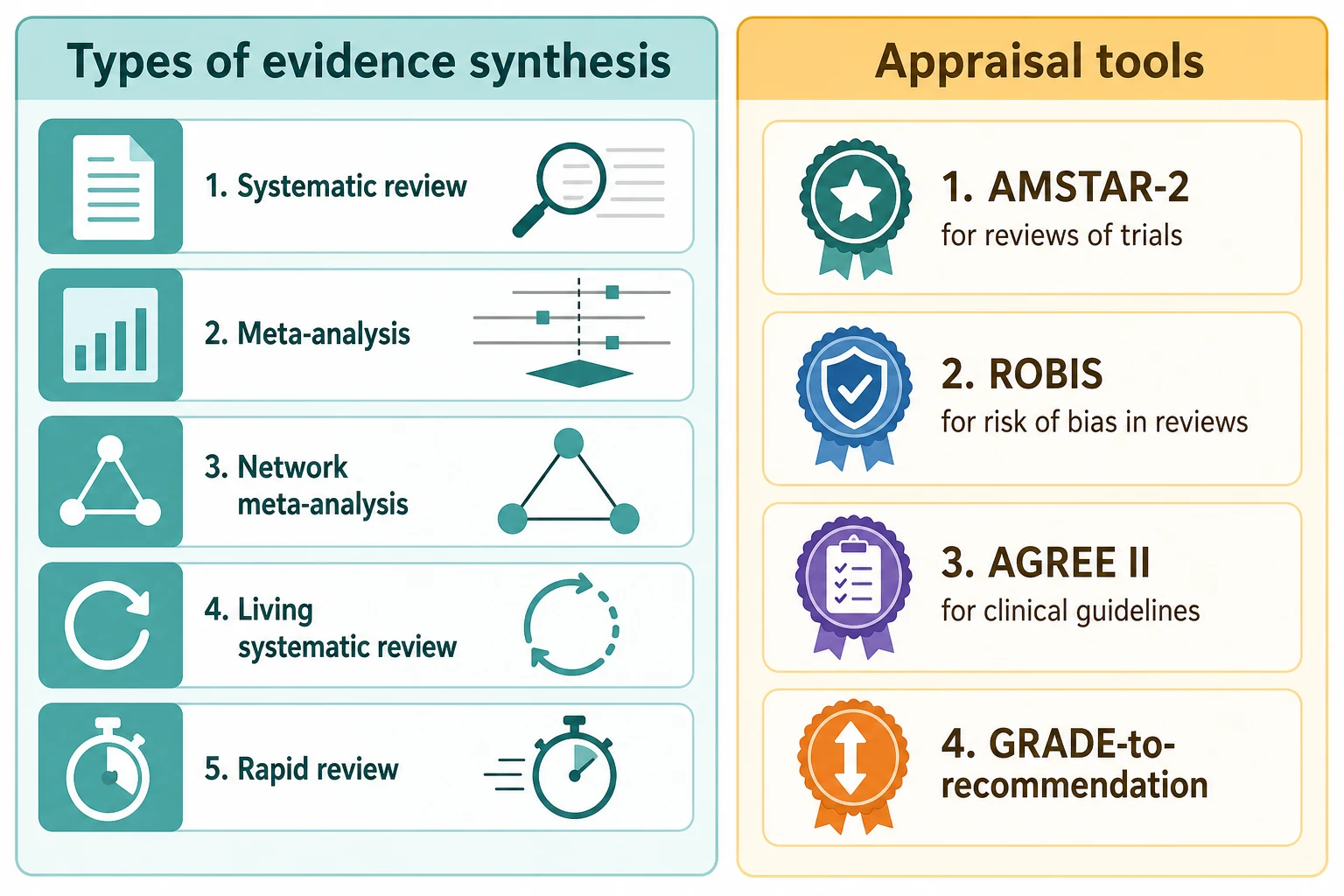
Types of evidence synthesis. A conventional systematic review asks a focused question and may pool its results. A meta-analysis is the statistical pooling step, valid only when the included studies are similar enough in population, intervention, comparator, and outcome. A network meta-analysis extends pooling to compare three or more treatments that may never have been tried head-to-head, by combining direct and indirect evidence across a network. A living systematic review is updated continually as new evidence appears, suited to fast-moving questions. A rapid review sacrifices breadth for speed, and is used when a decision cannot wait — as in a pandemic. [5] [13]
Filtered versus unfiltered evidence. Pre-appraised and filtered resources — systematic reviews, evidence summaries, and guidelines — do the appraisal work for you and should be searched first, but they inherit every weakness of the studies and the pooling beneath them, so you must still judge their method. A well-conducted Cochrane review of well-conducted trials sits near the apex of the hierarchy; a predatory-journal meta-analysis sits lower than a single honest trial. [10]
Recommendation strength and direction. GRADE classifies each recommendation by direction — for or against an intervention — and by strength. A strong recommendation means the guideline panel is confident that most patients would want it and that it should be offered; a weak or conditional recommendation means the choice is preference-sensitive, and the family should share it. Strength is not the size of the effect; it is the panel's confidence that following the recommendation does more good than harm across most patients. [8] [11]
Epidemiology & Risk Factors
Children have historically been therapeutic orphans, and the synthesised evidence that reaches you reflects that history. Far more paediatric treatments are used off-label or extrapolated from adult trials than in any other age group, so the reviews and guidelines you read rest, on average, on smaller studies, fewer trials, and more indirect evidence than their adult counterparts. [10]
Publication and reporting bias warp the literature a review can see. Studies with positive findings reach print more often than negative ones, so any pooled estimate built only on published studies overstates the true effect. The guard against this distortion is a search that reaches trial registers and unpublished data, plus a funnel plot that checks for the asymmetry bias produces. [2] [12]
Features of the synthesis itself predict whether it can be trusted. An industry-funded meta-analysis, a guideline panel stacked with conflicts of interest, a review that never registered its protocol, and a synthesis published in a predatory journal each carry a structural tilt that survives even careful statistics. Naming these pressures is the first defence against them. [2] [10]
Pathophysiology
Three forces drag a pooled estimate away from the truth, and rigorous synthesis resists each. [4] [10]
Bias in the included studies propagates upward. If the trials that feed a meta-analysis are themselves biased — through poor randomisation, lack of blinding, or selective reporting — then the pooled estimate inherits and often amplifies that bias. A large meta-analysis of biased studies is a precisely wrong answer, which is why AMSTAR-2 and ROBIS make the risk of bias of the included studies their first concern. [2] [3]
Heterogeneity is the genuine disagreement between the studies being pooled, beyond what chance alone would produce. It arises when the studies differ in population, dose, comparator, outcome definition, or setting, so much that a single pooled number misrepresents them all. Higgins and colleagues quantify it with the I-squared statistic, the proportion of total variation due to heterogeneity rather than chance, with rough thresholds of 25 percent for low, 50 percent for moderate, and 75 percent for substantial heterogeneity. Where heterogeneity is high, the pooled estimate is fragile, and you should look for its explanation through subgroup analysis before you trust it. [4]
Chance and model choice. A single small trial can swing a pooled estimate when the pooling weights it heavily, and the choice between a fixed-effect model — which assumes all studies share one true effect — and a random-effects model, which allows the true effect to vary, changes the result when heterogeneity is present. A funnel plot whose small studies cluster to one side of the larger ones suggests publication bias, and a review that ignores that asymmetry hands you an inflated estimate. [4] [13]
Clinical Presentation
You will meet synthesised evidence in several recognisable shapes. [10] [1]
The new-meta-analysis question. A family arrives with a meta-analysis claiming a therapy halves a complication and asks whether to start it. Your job is to judge the method before the result, then report the absolute effect and check it applies to the child before counselling. [10]
The guideline-versus-patient mismatch. A guideline recommends an intervention, but the child differs from the trial population in age, severity, or comorbidity. You must weigh directness, decide whether the recommendation still holds, and depart from it with reasons where it does not. [8] [9]
The journal-club or viva task. A supervisor hands you a forest plot and a PRISMA flow diagram and asks you to interpret and appraise them. Move in the fixed order — question, search, bias, heterogeneity, certainty, applicability — and defend each judgement. [1] [2]
The conflicting-syntheses problem. Two meta-analyses report opposite pooled effects, and you must weigh their method, their included studies, and their handling of heterogeneity to decide which to trust, and how the totality of the evidence falls. [10] [5]
Differential Diagnosis
Name the true problem before you act on a pooled number or a recommendation. [10] [4]
| You see | Prefer this framing | Trap |
|---|---|---|
| Large pooled benefit | Is it real and precise, or inflated by bias and publication bias? | Trusting the diamond before the method |
| Moderate I-squared | Is the heterogeneity explained by a clinically sensible subgroup? | Pooling across genuinely unlike studies |
| Strong guideline recommendation | Is the underlying certainty high and the child inside the evidence? | Obeying a recommendation built on low certainty |
| Top-ranked treatment in a network meta-analysis | Are the indirect comparisons valid and the network consistent? | Reading a ranking as head-to-head proof |
Real effect versus artefact. A large pooled effect may be genuine, but in synthesised paediatric data it is more often the fingerprint of bias, publication bias, or a single dominant trial, so confirm it with the risk-of-bias appraisal and the funnel plot before you believe it. [2] [4]
Strong recommendation versus high certainty. A strong recommendation can rest on low-certainty evidence, and a high-certainty body of evidence can yield a weak recommendation when the balance of benefits and harms is finely poised. Read the strength and the certainty separately, and never assume one from the other. [8] [9]
Clinical & Bedside Assessment
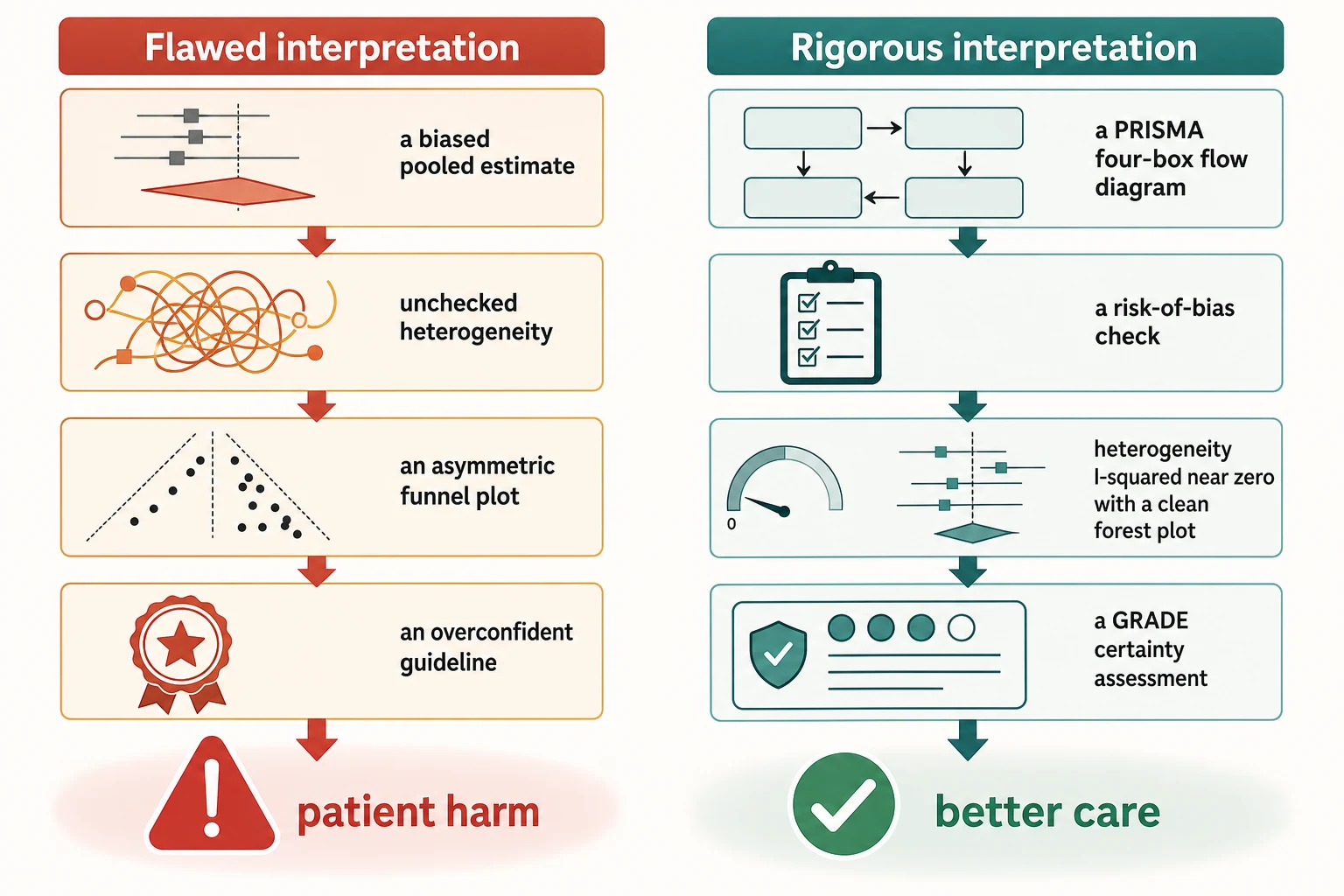
Read the PRISMA flow first. The 2020 PRISMA flow diagram traces every record from identification through screening, eligibility, and inclusion, and it shows you at a glance whether the search was broad, how many records were excluded and why, and how many studies and participants finally fed the synthesis. A flow that is missing, shallow, or unexplained is a warning that the search may not be reproducible. [1] [12]
Read the forest plot for the story it tells. Each row is one study, shown as a point estimate bounded by its confidence interval, sized by its weight in the pooling. The vertical line is the line of no effect; a row crossing it is compatible with both benefit and harm. The diamond at the foot is the pooled estimate, and its width is the pooled confidence interval — a diamond that crosses the line of no effect is not a positive result. [10] [4]
Score the review's risk of bias with the matched tool. AMSTAR-2 appraises systematic reviews of randomised or non-randomised studies across sixteen items, seven of them critical — a single critical flaw can drop the whole review to critically low confidence. ROBIS assesses risk of bias in systematic reviews across three phases: study eligibility, identification and selection of studies, and risk of bias and synthesis of the included studies. Either way, you are asking whether the review itself is trustworthy, not just whether its studies were. [2] [3]
Investigations
The investigations here are searches and appraisals, not blood tests. [10] [1]
Confirm the search was reproducible and exhaustive. Check that the review registered its protocol, searched multiple databases, hunted trial registers and unpublished data, screened in duplicate, and reported a PRISMA flow. A review that found only what its authors happened upon is biased from the start. [1] [12]
Quantify and explain heterogeneity. Read the I-squared and, where reported, tau-squared for the magnitude of between-study variation. Where heterogeneity is moderate or greater, look for a subgroup or meta-regression that explains it — by age, dose, severity, or setting — and treat the pooled estimate as fragile until it is explained. [4]
Hunt for publication bias. Check whether the review examined funnel-plot asymmetry and searched for unpublished studies. A pooled estimate built only on published positive studies is an overestimate, and the more asymmetric the funnel, the larger the overstatement. [2] [12]
Read the subgroup and sensitivity analyses. A subgroup analysis tests whether the effect differs across a plausible patient feature; a sensitivity analysis tests whether the pooled estimate survives when the review's assumptions change — for example, when high-risk studies are removed. A robust estimate survives both; a fragile one swings. [4] [10]
Document the appraisal. Record the question, the synthesis you found, its method rating, the pooled effect with its interval, the certainty, and the plan to reassess. Documentation turns a private judgement into a defensible, teachable act. [10]
Management — Resuscitation
Some moments are emergencies of a different kind, where a flawed synthesis or an inapplicable guideline is about to drive harm. [10] [2]
Imminent treatment on a flawed review. A child is about to receive a therapy on the strength of a biased, industry-funded, or predatory-journal meta-analysis. Correct the appraisal before the decision, state the certainty honestly, and do not let momentum carry a harmful choice. [2] [10]
Guideline that outruns its evidence. When a strong recommendation rests on low-certainty evidence or clashes with the child's circumstances, weigh the certainty and the applicability, depart from the recommendation with explicit reasons, and document the reasoning. A guideline is a starting point, not a substitute for the child in front of you. [8] [9]
Demand for an unproven intervention. A family, swayed by an online ranking from a network meta-analysis, insists on a top-ranked treatment. Acknowledge the hope, explain that an indirect ranking is not head-to-head proof, present the best direct evidence in plain absolute terms, and offer a shared, evidence-based alternative. [5] [6]
Management — Definitive & Stepwise
Work through the review in the right order, then turn to the guideline. [1] [10]
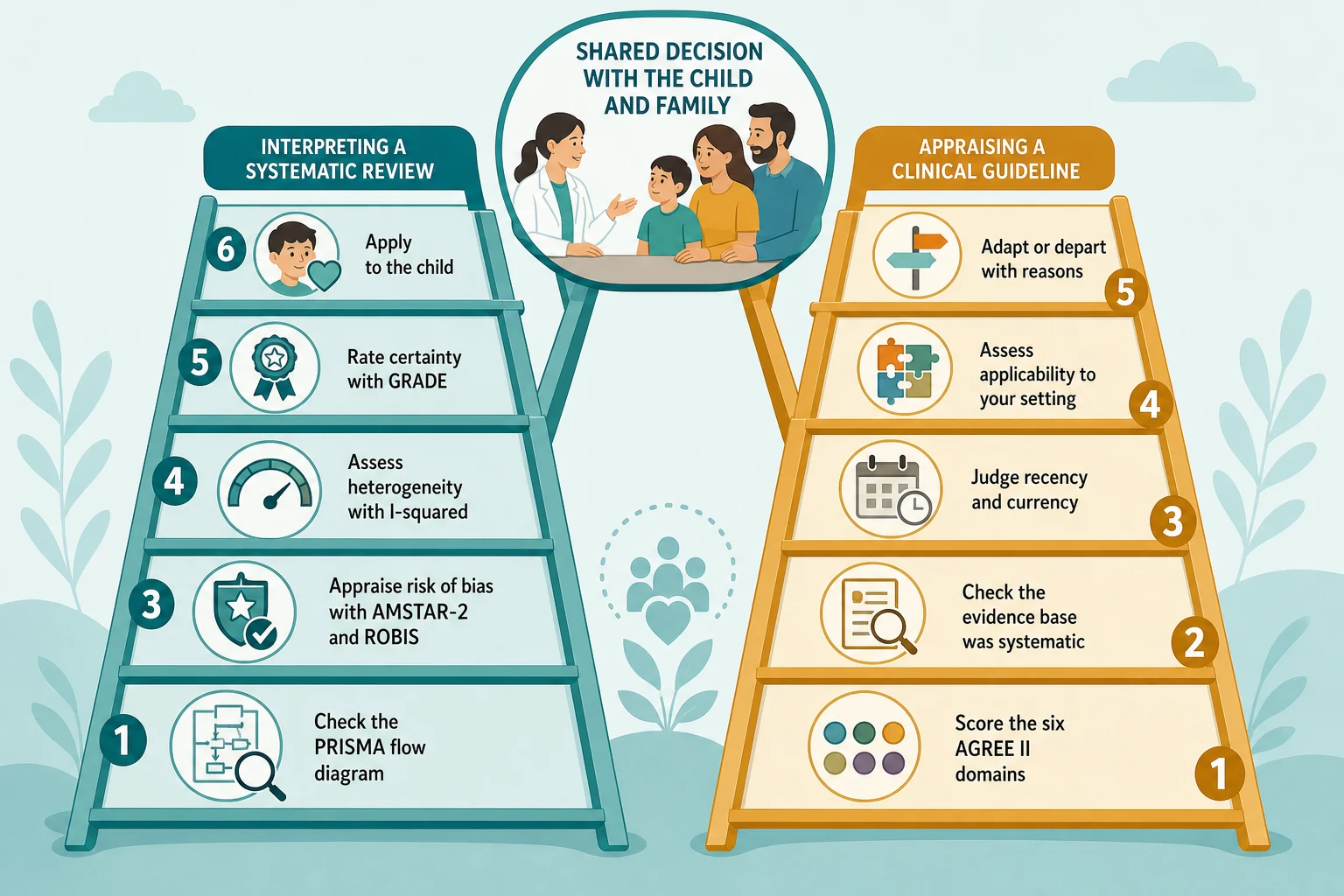
Interpreting a systematic review. First ask whether the question was focused and preregistered. Then confirm the search was reproducible and exhaustive, with a PRISMA flow you can read. Score the risk of bias of the review and its included studies with AMSTAR-2 or ROBIS, and only then read the pooled effect with its confidence interval. Quantify heterogeneity with I-squared and look for its explanation, check the funnel plot for publication bias, rate the certainty of the whole body of evidence with GRADE, and finally weigh applicability to the child. [1] [2] [3]
Appraising a clinical practice guideline. Score the guideline against the six AGREE II domains: scope and purpose, stakeholder involvement, rigour of development, clarity of presentation, applicability, and editorial independence. Check that it rests on a systematic review of the evidence, that it is current, and that it rated its own certainty with GRADE. Then judge whether the child sits inside the evidence, and decide whether to follow, adapt, or depart from each recommendation. [7] [8]
Moving from evidence to recommendation. GRADE's Evidence-to-Decision framework makes the move explicit by weighing the certainty of the evidence alongside the balance of desirable and undesirable effects, the values and preferences of those affected, the resources required, equity, acceptability, and feasibility. The panel's strength — strong or weak — reflects its confidence that following the recommendation does more good than harm across most patients, not the size of the effect. [7] [9] [11]
Specific Subtypes & Scenarios
A Cochrane review of an intervention in children. Cochrane reviews are produced to a strict method and are a strong default when one exists. Still check the recency, the risk of bias of the included trials, the heterogeneity, and the certainty, because a well-conducted review of weak trials yields a low-certainty answer. [10] [12]
A network meta-analysis ranking competing therapies. A network meta-analysis compares treatments that may never have been tried head-to-head by combining direct and indirect evidence across a network. Before you trust its ranking, check the assumptions it rests on — transitivity, that the studies are similar enough across comparisons; consistency, that direct and indirect evidence agree; and homogeneity within each comparison. A ranking built on violated assumptions is a league table, not evidence. [5] [6]
A living systematic review on a fast-moving question. A living review updates continually as new evidence appears, which is valuable when the question changes fast but demanding to appraise, because the pooled estimate and its certainty shift over time. Read the most recent update, note what changed, and check that the statistical methods for updating were sound. [13]
A national or international guideline. Whether from NICE, the AAP, WHO, or an Australian and New Zealand body, appraise each guideline with AGREE II, confirm it is current, and weigh its applicability to your setting and your child. Two guidelines on the same topic can differ because their populations, values, or evidence cutoffs differ, and the difference is often the teaching point. [7] [8]
A rapid review produced under time pressure. A rapid review trades breadth and duplication for speed, so its greatest weakness is a narrower search and less risk-of-bias work. Treat its conclusions as provisional, and revisit them when a full systematic review appears. [10]
Complications & Pitfalls
- Accepting a pooled estimate without checking heterogeneity, publication bias, or the risk of bias of the included studies. [2] [4]
- Equating a network meta-analysis treatment ranking with head-to-head trial evidence. [5] [6]
- Treating a weak or conditional GRADE recommendation as mandatory. [8]
- Following an outdated guideline after new evidence has appeared, or a guideline whose panel carried undisclosed conflicts. [7]
- Extrapolating adult-derived recommendations to a neonate or infant without weighing indirectness and dose. [10]
- Quoting the relative pooled effect without the absolute baseline and the number needed to treat. [10]
- Trusting an industry-funded or predatory-journal meta-analysis over an independent Cochrane review. [2]
Prognosis & Disposition
A good interpretation is measured by the decision it supports, not by how elegantly it ran. [10] [1]
Markers of an enduring answer. The conclusion rests on a well-conducted review of well-conducted trials, the pooled estimate is precise, the heterogeneity is explained, the funnel plot is symmetric, and the certainty is high. Where these hold, the answer is likely to endure; where they do not, expect revision. [2] [4]
When to defer. Where the certainty is low and a higher-quality review or a living update is imminent, or the decision is reversible, defer acting until better evidence arrives, or choose the reversible option and reassess. [13]
When to escalate. Sparse evidence combined with high stakes warrants a second opinion, specialist input, or an ethics consultation, especially where a guideline and the child's circumstances conflict or the child is vulnerable. [7] [9]
Disposition includes documentation. Record the synthesis or guideline you used, its method and certainty rating, the decision, and the plan to reassess, so the reasoning survives the moment and teaches the next clinician. [10]
Special Populations
Neonates and infants. Much of the synthesised evidence is extrapolated from older children or adults, so downgrade for indirectness under GRADE, appraise age-specific dose and safety with particular care, and watch for harm that age-specific pharmacology can produce. [10]
Children with rare disease. Evidence may be limited to case series and expert consensus, so rate the certainty low and lean on shared decision-making, patient registries, and networks that pool the few cases that exist. [10]
Aboriginal and Torres Strait Islander, Maori, and other Indigenous children. Appraise whether the guideline was developed with the community and is culturally and epidemiologically applicable, and privilege locally endorsed guidance and Indigenous data sovereignty. A guideline written for a different population can mislead even when its method is sound. [7]
Adolescents. Ensure the synthesised evidence actually includes adolescents, and apply it with the young person through shared decision-making that respects their emerging autonomy. [8]
Children with medical complexity. Weigh applicability to a heterogeneous group that trials and guidelines often exclude, and prioritise patient-centred outcomes such as quality of life and family burden alongside survival. [10]
Evidence, Guidelines & Regional Differences
Core anchors are the Page PRISMA 2020 statement for reporting reviews, the Shea AMSTAR-2 tool and the Whiting ROBIS tool for appraising them, the Higgins I-squared paper for quantifying heterogeneity, the Cipriani and Al Khalifah papers on network meta-analysis, the Alonso-Coello GRADE Evidence-to-Decision framework, the Andrews GRADE guidelines for moving from evidence to recommendations, the Guyatt GRADE consensus paper, the Murad Users' Guide for reading a systematic review, and the Simmonds paper on living systematic reviews. [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13]
The RACP curriculum names the interpretation of evidence synthesis and guidelines as a core professional skill, and the Cochrane Australasia centre and national guideline organisations publish appraised syntheses. Use locally endorsed guidelines and registries, and where evidence is sparse for Aboriginal and Torres Strait Islander and Maori children, seek community-generated data and culturally safe pathways. [10] [1]
The RCPCH Progress+ curriculum frames evidence-based practice and research methodology as a core professional skill, and the National Institute for Health and Care Excellence publishes transparently graded guidelines built on systematic evidence reviews. Use NICE and Cochrane syntheses, and follow PRISMA 2020, AGREE II, and GRADE in any appraisal you perform. [1] [8]
The American Academy of Pediatrics issues clinical practice guidelines built on graded evidence, and the United States Preventive Services Task Force grades recommendations on a transparent certainty-and-benefit scale. Use these alongside Cochrane reviews, and apply the GRADE Evidence-to-Decision framework when moving from evidence to a recommendation. [7] [8]
The CanMEDS Scholar role maps directly onto locating, appraising, and applying synthesised evidence, and Canadian guideline bodies publish AGREE-II-appraised, GRADE-based recommendations. Use locally endorsed guidance and appraised syntheses, and document the certainty of the evidence behind each decision. [7] [10]
Controversies: how much weight to give a network meta-analysis ranking against direct head-to-head evidence; whether living systematic reviews improve outcomes or simply multiply work; how to handle conflicts of interest on guideline panels; and whether rigid adherence to guidelines helps or harms the children the guidelines never studied. Exam answers show a structured appraisal, an honest certainty rating, and local humility. [5] [9] [13]
Exam Pearls
- Read the PRISMA flow and score AMSTAR-2 or ROBIS before you read the pooled diamond. [1] [2]
- I-squared rough thresholds: 25 percent low, 50 percent moderate, 75 percent substantial heterogeneity. [4]
- A diamond that crosses the line of no effect is not a positive result. [10]
- AMSTAR-2 has seven critical domains; a single critical flaw can drop the whole review to critically low confidence. [2]
- A GRADE strong recommendation means most patients would want it; a weak one means the choice is preference-sensitive. [8]
- AGREE II has six domains and a 23-item checklist: scope and purpose, stakeholder involvement, rigour of development, clarity, applicability, and editorial independence. [7]
- A network meta-analysis assumes transitivity, consistency, and homogeneity — check these before trusting the ranking. [5] [6]
- Always report the absolute effect and the number needed to treat, never the relative pooled figure alone. [10]
Interpret a systematic review and apply it to a child
Ask whether the question was focused and preregistered
Confirm a reproducible search and read the PRISMA flow
Score risk of bias with AMSTAR-2 or ROBIS
Read the pooled effect, its confidence interval, and the I-squared
Check the funnel plot and the subgroup and sensitivity analyses
Rate the certainty with GRADE and weigh applicability to the child
Apply through shared decision-making and document the plan to reassess
References
- [1]Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ, 2021.PMID 33782057
- [2]Shea BJ, Reeves BC, Wells G, et al. AMSTAR 2: a critical appraisal tool for systematic reviews that include randomised or non-randomised studies of healthcare interventions, or both. BMJ, 2017.PMID 28935701
- [3]Whiting P, Savovic J, Higgins JP, et al. ROBIS: A new tool to assess risk of bias in systematic reviews was developed. Journal of clinical epidemiology, 2016.PMID 26092286
- [4]Higgins JP, Thompson SG, Deeks JJ, Altman DG Measuring inconsistency in meta-analyses. BMJ, 2003.PMID 12958120
- [5]Cipriani A, Higgins JP, Geddes JR, Salanti G Conceptual and technical challenges in network meta-analysis. Annals of internal medicine, 2013.PMID 23856683
- [6]Al Khalifah R, Florez ID, Guyatt G, Thabane L Network meta-analysis: users' guide for pediatricians. BMC pediatrics, 2018.PMID 29843665
- [7]Alonso-Coello P, Oxman AD, Moberg J, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction. BMJ, 2016.PMID 27365494
- [8]Andrews J, Guyatt G, Oxman AD, et al. GRADE guidelines: 14. Going from evidence to recommendations: the significance and presentation of recommendations. Journal of clinical epidemiology, 2013.PMID 23312392
- [9]Andrews JC, Schunemann HJ, Oxman AD, et al. GRADE guidelines: 15. Going from evidence to recommendation-determinants of a recommendation's direction and strength. Journal of clinical epidemiology, 2013.PMID 23570745
- [10]Murad MH, Montori VM, Ioannidis JP, et al. How to read a systematic review and meta-analysis and apply the results to patient care: users' guides to the medical literature. JAMA, 2014.PMID 25005654
- [11]Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating quality of evidence and strength of recommendations. BMJ, 2008.PMID 18436948
- [12]Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Journal of clinical epidemiology, 2009.PMID 19631508
- [13]Simmonds M, Salanti G, McKenzie J, Elliott J Living systematic reviews: 3. Statistical methods for updating meta-analyses. Journal of clinical epidemiology, 2017.PMID 28912004