Paeds · professional-practice-and-evidence
Leadership and interprofessional team management
Also known as Clinical leadership paediatrics · Interprofessional team management · Crew resource management in child health · TeamSTEPPS paediatrics · Team leadership resuscitation
Fellowship guide to leading and managing interprofessional teams in child health: leadership styles, building a high-performing team, shared mental models, closed-loop communication, psychological safety and speak-up, crew resource management, TeamSTEPPS and SBAR, structured handover, conflict and burnout, and the Cochrane evidence for interprofessional collaboration and education.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A two-year-old arrests on the ward at three in the morning. Within a minute the bed space is crowded: a registrar, two nurses, a resident, a pharmacist, a parent watching from the door. Whether that child survives in good neurological shape depends less on any single clinician's knowledge than on how well the team works together. This leaf teaches you how to lead, join and judge that team. Deep human-factors theory lives on the patient-safety page; the improvement methods on the quality-improvement page; the conflict-handling on the difficult-encounters page. [2] [4]
Clinical leadership is setting a direction, aligning people around it, and creating the conditions in which they can do good work. The systematic reviews distinguish leadership sharply from management (planning, organising, budgeting and control) and from mere clinical expertise. A brilliant clinician can be a poor leader, and a strong leader does not have to be the most senior person in the room. [14] [15]
An interprofessional team is a group from different professions who learn with, from and about each other and share decisions around a common goal — a paediatrician, a nurse, a pharmacist, an allied-health therapist, a social worker and the family working as one. That is stronger than a multidisciplinary team, where experts work in parallel, and more integrated than an interdisciplinary team, where information is shared but decisions are not always joint. The child with medical complexity is the clearest case for genuine interprofessional care. [5] [17]
Classification
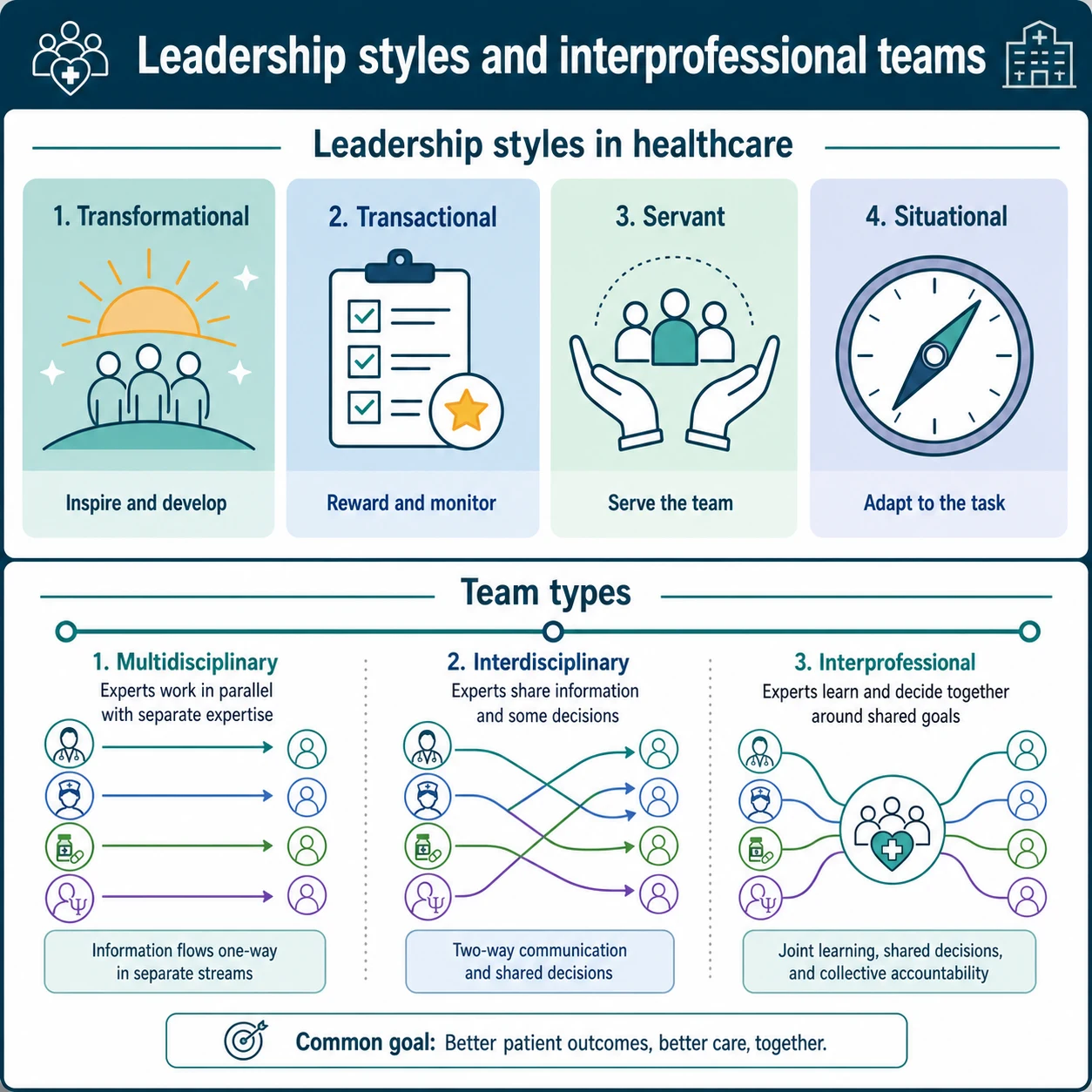
Classify leadership first by style, because examiners reward the candidate who can name a style and say when to use it. Transformational leadership inspires and develops people toward a shared vision; it builds the climate in which teams improve. Transactional leadership rewards and monitors against clear targets; it suits reliable, repeatable work. Servant leadership puts the team's needs first; it builds trust and psychological safety. Situational (contingency) leadership adapts the style to the task and the person. The evidence reviews show that leadership style is consistently associated with quality-of-care measures, though the literature is heterogeneous. [14] [16]
The second axis is the team itself. A multidisciplinary team has separate experts who work in parallel; an interdisciplinary team shares some decisions; an interprofessional team learns and decides together around shared goals. Moving a team up that spectrum — from parallel practice to genuinely shared decisions — is one of the most effective things a leader can do. [5] [17]
Leadership styles at a glance
- Inspires and develops people
- Builds an improving, learning climate
- Best for change and complex goals
- Rewards and monitors against targets
- Clear expectations and feedback
- Best for reliable, repeatable work
- Puts the team's needs first
- Builds trust and psychological safety
- Best for sustaining a healthy team
- Adapts style to task and follower
- Directive in crisis, facilitative in complexity
- The everyday default for a consultant
Epidemiology & Risk Factors
When serious adverse events are analysed, communication failure is the single most common contributing factor — not a knowledge gap. Reviews of paediatric and anaesthetic harm repeatedly find that information was available somewhere in the team but never reached the person who could act on it. That is why team management is patient safety. [2] [4]
Several risk factors predict that a team will fail. A steep authority gradient silences juniors. Unclear roles mean a critical task falls between people. Unstructured handover loses medications and plans between shifts. Fatigue, noise and distraction degrade communication at the exact moments it matters most. Children are especially exposed because resuscitation is weight-based, time-critical and rare, so the team is often working at the edge of its routine. [4] [10]
The structural pressures on paediatric teams are also examinable. Children with medical complexity need many teams at once, which multiplies the chance of fragmented care. Rural and remote services run with small numbers and long retrieval times. Shift work and high turnover mean the team that starts a child's care is rarely the team that finishes it — so handover quality is load-bearing. [7] [13]
Pathophysiology
Picture the resuscitation bed again. What keeps five people coordinated as the picture changes every minute is a shared mental model — an agreed, up-to-date picture of who the child is, what is wrong, what the plan is, who is doing what, and what will happen next. When the model is shared, the team anticipates. When it is not, people work from different assumptions and the same task is done twice or not at all. Reader showed that team situation awareness on intensive-care rounds predicts whether the team correctly anticipates patient progress. [4] [12]
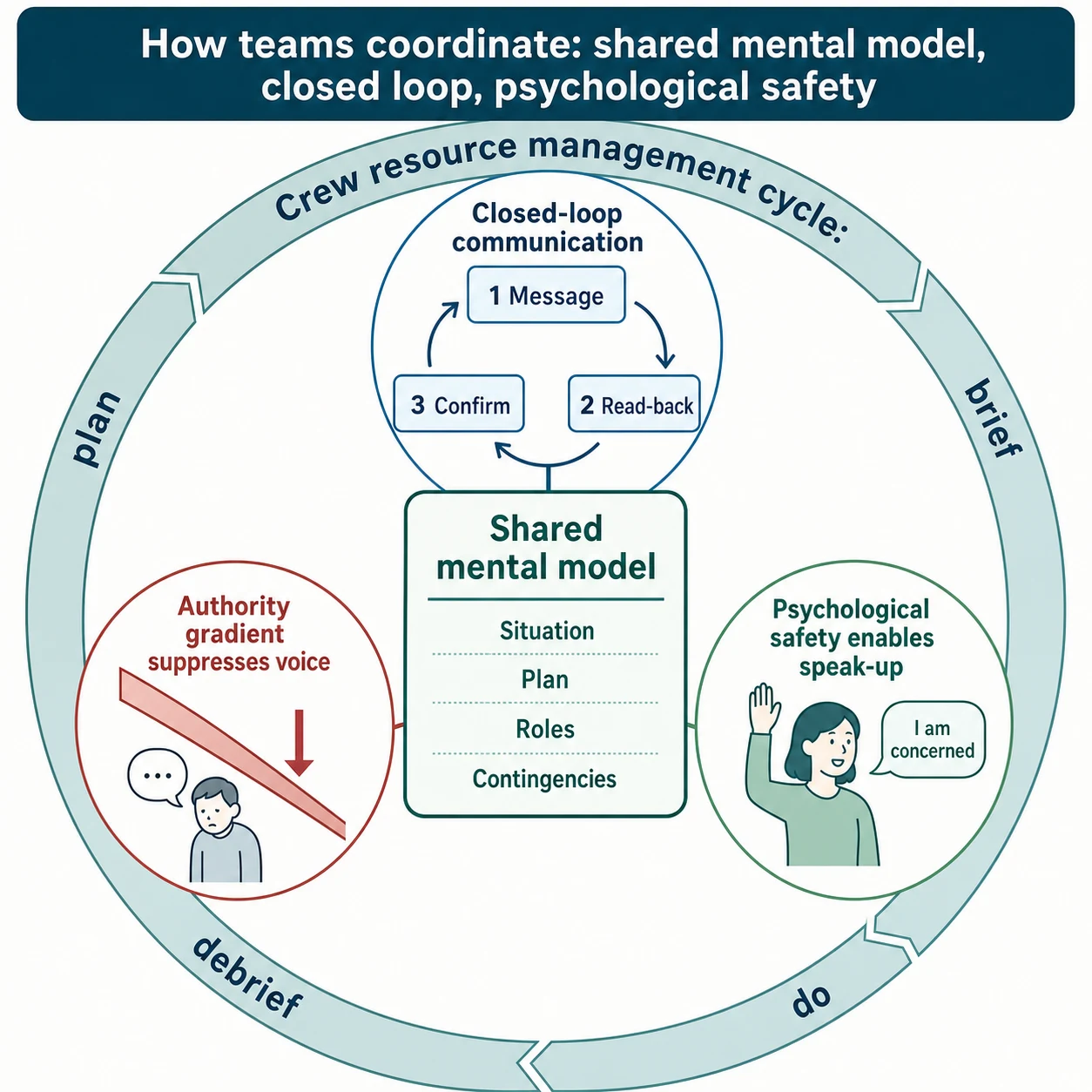
Closed-loop communication is the mechanical fix for information loss. The sender states the message; the receiver repeats it back (read-back); the sender confirms. It feels slow in a calm room and it is lifesaving in a crisis, because it guarantees the dose and the task were heard. Open-loop orders — "give some adrenaline" into the air — are how drugs are missed or doubled. [2] [11]
The deeper mechanism is psychological safety: a shared belief that the team is safe for interpersonal risk-taking, so a nurse or a junior can say "I think that dose is wrong" or "I am uncomfortable" without being punished. Psychological safety enables voice, and voice is what catches the error before it reaches the child. The enemy of voice is the authority gradient: the combined weight of seniority, personality and hierarchy that makes a junior hold back exactly the information that would have changed the outcome. Aviation learned this lesson the hard way, and medicine borrowed it through crew resource management. [1] [4]
Crew resource management (CRM) is the aviation-derived discipline of using all available resources — people, information and equipment — to operate safely. Manser's review of teamwork in dynamic domains shows the same mechanisms recur across anaesthesia, surgery, emergency care and the intensive-care unit: leadership, workload management, situation awareness, communication and teamwork behaviours. These are learnable, and they are what simulation-based CRM training practises. [4] [11]
Clinical Presentation
A well-led team is visible at the bedside. There is a named leader standing back far enough to see the whole child. Roles are allocated out loud — airway, breathing, circulation, drugs, scribe. Every order is closed-loop. The team takes a structured pause to share the picture and the plan. The leader invites questions and names uncertainty out loud. The family is included rather than managed. After the event the team debriefs. [4] [11]
A dysfunctional team shows itself just as clearly. No one is named leader, so everyone tries to lead and no one does. Orders float into the air with no read-back. The plan lives in the consultant's head and nowhere else. A nurse who has noticed the wrong dose goes quiet. The registrar and the nurse disagree openly about the fluid rate and the child is caught between them. After the event the team disperses with no debrief, so the same trap is set for next time. [2] [4]
A failing handover presents as the morning discovery: a medication that was not given overnight, a task duplicated by two people, a family told three different plans. A failing culture presents as burnout — the team that has stopped speaking up, stopped eating, and started describing work in terms of moral distress. Recognising these presentations is half the viva; the other half is knowing what to do about them. [13] [14]
Differential Diagnosis
- Leadership versus management. Leadership sets direction and enables; management plans, organises and controls. Both are needed; they are not the same skill. [14] [15]
- Transformational versus transactional versus servant versus situational leadership. Inspire-and-develop versus reward-and-monitor versus serve-the-team versus adapt-to-the-moment. Choose by the situation. [16]
- Multidisciplinary versus interdisciplinary versus interprofessional teams. Parallel practice versus shared information versus shared learning and decisions. [5] [17]
- Interprofessional collaboration (IPC) versus interprofessional education (IPE). IPC is different professions working together for care; IPE is learning together to be able to. The Cochrane reviews cover each separately. [5] [17]
- Crew resource management versus TeamSTEPPS versus simulation-based CRM training. CRM is the resource-use discipline; TeamSTEPPS is the toolkit; simulation is how the skills are practised. [3] [11]
- SBAR versus I-PASS handover. SBAR escalates a moment; I-PASS structures a whole handover. [2] [13]
- Command (authoritative) leadership versus facilitative leadership. Directive clarity in crisis versus inclusive facilitation in complexity. [4]
- Task conflict versus relationship conflict. Disagreement about the work can help; interpersonal hostility harms. [15]
- Burnout versus moral injury versus compassion fatigue. Different aetiologies, overlapping presentation, different remedies. [14]
Clinical & Bedside Assessment
Before you lead a resuscitation, read the team in the first ten seconds. How many people are here? Who is most senior? Is anyone already doing compressions? Then declare yourself loudly: "I am taking the role of team leader." Stand where you can see the whole bed space and the monitors but far enough back to think. Allocate roles by name and by task — "Sarah, you are airway; David, you are doing compressions; Maria, you are drugs and draw up as I call them; Tom, you are scribe and time-keeper." A leader who is also doing compressions has stopped leading. [4] [11]
To escalate a deteriorating child to a senior, use SBAR — Situation, Background, Assessment, Recommendation. It takes 30 seconds, it forces you to synthesise, and it hands the receiver a recommendation to act on rather than a ramble to decode. SBAR is the communication tool Leonard and colleagues anchored to the human factor of safe care. [2]
At a shift change, lead a structured handover with I-PASS — Illness severity, Patient summary, Action list, Situation awareness and contingency planning, and Synthesis by the receiver. The receiver reads back the plan (synthesis), which is the closed loop of handover. Starmer showed a standardised handoff programme reduced medical errors across nine paediatric training programmes. [13]
Around any high-risk procedure, run a brief before (the plan, the roles, the contingencies) and a debrief after (what went well, what we learned, what we will change next time). A 30-second debrief is enough; the point is to make learning routine. To flatten the authority gradient, name it out loud: "If anyone sees something wrong, please say it — that includes the student." Then respond well the first time someone does, or you will never be told again. [3] [11]
Investigations
In a teamwork leaf, "investigations" means the tools you use to assess how the team is performing. You can observe a team directly with validated instruments — the TEAM tool (Team Emergency Assessment Measure) scores leadership, teamwork and task management during a resuscitation, and NOTECHS and OTAS do similar work for non-technical skills and theatre teams. Use them to give specific, behaviour-focused feedback rather than a vague "good job". [4] [11]
You can measure the climate you are trying to build. Psychological safety is captured with Edmondson's team-learning scale, and speaking-up behaviour with companion instruments. The two are read together: a team can score well on safety but still not speak up if the authority gradient is steep, so behaviour is the truer measure. [4] [15]
Audit the processes that teamwork is meant to protect. Track handover completeness (did the action list transfer?), near-miss reports (are people willing to report?), and staff experience. When you evaluate team training itself, the meta-analytic evidence is that it improves team performance and, to a lesser degree, affective outcomes — so measure performance, not just satisfaction. [3] [13]
Management — Resuscitation
- Name the leader, out loud. Without a named leader the team has no one to follow and no one thinking ahead. [4]
- Allocate roles by name and task. Airway, breathing, circulation, drugs, scribe — each assigned so nothing falls between people. [11]
- Use closed-loop communication for every dose and critical task. Call the dose, hear the read-back, confirm. [2]
- Share the mental model in a structured pause. Every minute or two, summarise who the child is, the working diagnosis, the plan and the next contingency. [4] [12]
- Flatten the authority gradient. Invite speak-up by name and respond well to it. [1]
- Run the event and the family in parallel. One team member keeps the parent informed while the clinical work continues. [14]
Management — Definitive & Stepwise
The definitive work of team leadership is building a team that performs reliably even when you are not standing in it. Start with role clarity: every person should know their role, who they report to, and what decisions are theirs. Then build the shared mental model — make the plan explicit and repeatable, not something that lives only in your head. Then protect psychological safety so the plan can be corrected by anyone who sees it is wrong. [4] [15]
Match your leadership style to the moment. In a resuscitation be authoritative and clear — a crisis is not the time for a committee. In a complex longitudinal plan for a medically complex child be facilitative — draw the team and the family into shared decisions. The situational leader moves fluently between the two. The reviews show style is associated with quality measures, so treat leadership as a deliberate clinical skill, not a personality trait. [14] [16]
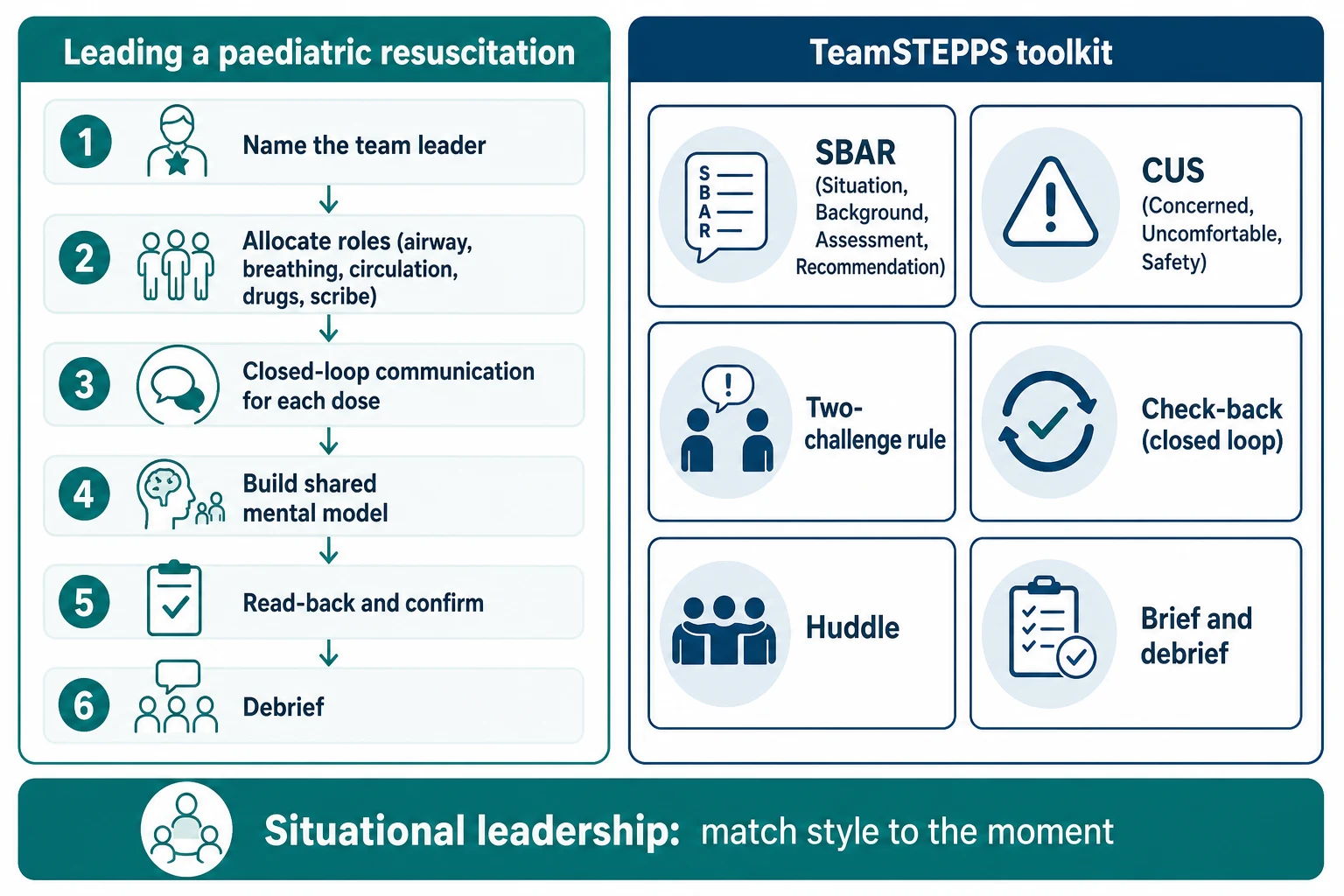
Embed the TeamSTEPPS toolkit into daily work. Use SBAR to escalate, call-outs to broadcast critical information to the whole team, check-backs (closed loops) to confirm critical orders, CUS ("I am Concerned; I am Uncomfortable; this is a Safety issue") to escalate concern up the hierarchy, the two-challenge rule to force a hearing when a concern is dismissed once, and huddles, briefs and debriefs around planned and unplanned events. These are not acronyms to memorise for an exam; they are the everyday vocabulary of a safe team. [2] [11]
Sustain it through simulation-based CRM training with structured debrief — the form of education that best transfers non-technical skills to the bedside. Cheng and colleagues set out the instructor framework for simulation-based CRM in paediatric critical care, and Eppich and colleagues made the case for team training across emergency and critical-care paediatrics. Without reinforcement the skills decay, so build it into routine unit life, not a one-off course. [10] [11]
Building a high-performing interprofessional team
Clarify roles: who does what, who reports to whom, whose decisions are whose
Make the plan explicit and repeatable so the team shares one mental model
Build psychological safety so the plan can be corrected by anyone
Embed TeamSTEPPS tools in daily work — SBAR, check-back, CUS, huddles and debriefs
Standardise handover with I-PASS and audit it
Reinforce with simulation-based CRM training and structured debrief
Specific Subtypes & Scenarios
Paediatric resuscitation team leadership (PICU/ED). In an arrest the leader's job is to run the team, not to do the tasks. Allocate roles, keep the shared mental model current, watch the monitors from a step back, and use closed-loop communication for every drug. Simulation-based CRM training is the evidence-based way to rehearse this, and it is now standard in paediatric critical-care education. [11] [12]
Neonatal and paediatric retrieval. Retrieval multiplies the team — the referring hospital, the retrieval team, the receiving unit — and the handovers between them are where harm hides. Distributed leadership matters here: the retrieval consultant leads the plan, but the referring nurse holds local knowledge the team needs, and a good leader pulls that knowledge out. [7] [13]
Structured handover (I-PASS). Starmer's handoff programme reduced medical errors across nine North American paediatric training programmes, and the lesson generalises: a standardised, receiver-synthesised handover is one of the highest-yield team interventions in child health. Implement it with training, an electronic template, and ongoing audit. [13]
Surgical safety checklist and team time-out. Haynes showed a simple surgical safety checklist reduced morbidity and mortality across a global population of surgical patients, and the mechanism is teamwork — the time-out forces a shared mental model, role clarity and explicit contingency planning before incision. Pronovost's central-line bundle works for the same reason: standardise the reliable process and make the team accountable to it. [6] [8]
Surgery-to-intensive-care handover. Catchpole adapted the Formula 1 pit-stop and aviation models to the paediatric handover from theatre to intensive care, showing that a structured, role-led handover reduces information loss at exactly the moment patients are most fragile. It is the clearest paediatric example of borrowing an aviation tool wholesale. [9]
Rapid response team (MET/RRT). Sharek showed a hospital-wide rapid response team in a children's hospital was associated with reduced mortality and code rates outside the intensive-care unit. The RRT is a team intervention as much as a clinical one — it brings a structured team to the deteriorating child before they arrest. [7]
Rural and remote paediatric team leadership. Small teams, low volumes and long retrieval times change the job. The leader is often a generalist working by telehealth with a distant specialist, so distributed leadership, structured communication and a clear retrieval interface become survival skills. Build the relationships and the protocols before the emergency, not during it. [10] [13]
Complications & Pitfalls
- Assuming seniority equals leadership ability, and so never developing the team's leadership skills. [14] [15]
- Authoritarian leadership that silences a junior and lets a preventable error reach the child. [1] [4]
- Open-loop orders — a dose called into the air with no read-back — that are missed or doubled. [2]
- Handover with no structure, so medications, tasks and the plan are lost between shifts. [13]
- No debrief after a critical event, so the team does not learn and the same harm recurs. [11]
- Ignoring burnout and moral distress until a team member errs or leaves. [14]
- Lip-service team training with no reinforcement, so the skills decay within months. [3] [10]
- Confusing interprofessional collaboration with simply holding more meetings. [5] [17]
- Failing to address unprofessional behaviour under a just-culture framework, which erodes the safety of the whole team. [15]
- Forgetting the second victim — the clinician harmed by an adverse event needs structured support, not blame. [4]
Prognosis & Disposition
A team sustains high performance when four things hold: stable leadership, psychological safety, routine training with feedback, and a culture that rewards speaking up. When any one weakens, performance decays — often silently, visible only in a rising near-miss rate or a quieter team. The leadership reviews are consistent that leadership and team climate are associated with quality-of-care measures, even where the study designs are weak. [14] [16]
You know a team intervention has worked when the observable outcomes move: fewer handover omissions, fewer medication errors, more near-miss reports (a sign people feel safe to report), and better staff and family experience. The strongest intervention evidence is for team training — the Salas meta-analysis found team training improves team performance across healthcare and other domains — and for structured handover. [3] [13]
When leadership of a complex child must pass between consultants across a rotation, the handover of the plan matters as much as the handover of the patient. Write the shared mental model down — the goals of care, the agreed ceilings, the family's preferences — so the next team inherits the team's thinking, not just the chart. Safety-net with a named owner and a scheduled review so the gains do not quietly decay. [4] [13]
Special Populations
Neonates and infants concentrate the need for crisp team leadership because resuscitation is weight-based, time-critical and rare; a two-person check on every drug and a closed loop on every dose are non-negotiable. Children with medical complexity live across many teams at once, so a care coordinator and a single shared plan are what prevent fragmentation and polypharmacy harm. [8] [13]
Indigenous children need culturally safe interprofessional teams that include an Aboriginal health worker or cultural advisor as a core member, not an afterthought. Rural and remote teams work with small numbers and long retrieval times, so distributed leadership, telehealth-enabled multidisciplinary care and a rehearsed retrieval interface are central to the job. [7] [10]
Migrant and refugee families need interpreter-inclusive teamwork — the interpreter is a team member, briefed and debriefed with everyone else. Adolescents need confidentiality-aware teams and a coordinated transition to adult care. Children with disability and neurodiversity need therapy-led interprofessional teams built around family-reported goals. Technology-dependent children need home-ventilation teams, nurse-led coordination and a clear escalation and retrieval plan. [5] [13]
Evidence, Guidelines & Regional Differences
The evidence base is real but carries caveats the viva expects. Sexton's cross-sectional surveys put medicine next to aviation and showed that the same teamwork failures — poor communication, flattened voice, high hierarchy — predict error in both. Leonard anchored safe care to teamwork and communication and gave medicine SBAR. Manser's review distilled the mechanisms that recur across dynamic domains: leadership, workload management, situation awareness, communication and teamwork behaviours. [1] [2] [4]
The intervention evidence is strongest for team training. The Salas meta-analysis found team training improves team performance and, to a lesser degree, affective outcomes; simulation-based CRM is the form that best transfers to the bedside. The Cochrane reviews are more cautious: Zwarenstein and colleagues found interprofessional collaboration interventions can improve practice and outcomes, and Reeves and colleagues found interprofessional education can too, but both flagged heterogeneous studies and weak designs. Treat the direction as reliable and the effect size as context-dependent. [3] [5] [17]
The leadership literature is observational but consistent. Al-Sawai framed leadership as a distinct clinical competency; Berghout and colleagues systematically reviewed medical leadership in hospitals and found it is associated with organisational performance; and Sfantou and colleagues found leadership style is associated with quality-of-care measures. All three flag that leadership is hard to study in randomised designs, so the evidence is associational rather than causal. [14] [15] [16]
Apply the Royal Australasian College of Physicians professional qualities framework and the Australian Commission on Safety and Quality in Health Care's teamwork and communication standards. Reference local clinical-handover and rapid-response policies rather than inventing mandated ratios. [2] [7]
Controversies: how much leadership is personality versus trainable skill; whether team-training gains decay without reinforcement (they do); and whether the observational leadership evidence warrants the strong claims sometimes made for transformational leadership. Answer with the direction of effect and the honest caveat about study design. [3] [16]
Exam Pearls
- Leadership sets direction and enables the team; management plans, organises and controls; followership is skilled support of good leadership. [14] [15]
- Transformational inspires and develops; transactional rewards and monitors; servant serves the team; situational adapts to the task and the follower. [16]
- CRM = crew resource management, from aviation: use all available resources — people, information, equipment — to operate safely. [1] [4]
- Closed-loop communication = message, read-back, confirm. [2]
- SBAR = Situation, Background, Assessment, Recommendation. [2]
- I-PASS = Illness severity, Patient summary, Action list, Situation awareness and contingency planning, Synthesis by receiver. [13]
- CUS = "I am Concerned, I am Uncomfortable, this is a Safety issue"; the two-challenge rule forces a hearing when a concern is dismissed once. [11]
- Psychological safety (Edmondson) = a shared belief the team is safe for interpersonal risk-taking; it enables voice and learning. [4] [15]
- Salas meta-analysis: team training improves team performance. Cochrane (Reeves/Zwarenstein): interprofessional collaboration and education can improve practice and outcomes, with heterogeneous evidence. [3] [5] [17]
- Authority gradient: flatten it so juniors speak up; in a crisis a clear, authoritative leader is still needed. The second victim needs structured support, not blame. [4] [14]
References
- [1]Sexton JB, Thomas EJ, Helmreich RL Error, stress, and teamwork in medicine and aviation: cross sectional surveys. BMJ, 2000.PMID 10720356
- [2]Leonard M, Graham S, Bonacum D The human factor: the critical importance of effective teamwork and communication in providing safe care. Quality & safety in health care, 2004.PMID 15465961
- [3]Salas E, DiazGranados D, Klein C, Burke CS Does team training improve team performance? A meta-analysis. Human factors, 2008.PMID 19292013
- [4]Manser T Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta anaesthesiologica Scandinavica, 2009.PMID 19032571
- [5]Zwarenstein M, Goldman J, Reeves S Interprofessional collaboration: effects of practice-based interventions on professional practice and healthcare outcomes. The Cochrane database of systematic reviews, 2009.PMID 19588316
- [6]Haynes AB, Weiser TG, Berry WR, Lipsitz SR A surgical safety checklist to reduce morbidity and mortality in a global population. The New England journal of medicine, 2009.PMID 19144931
- [7]Sharek PJ, Parast LM, Leong K, Coombs J Effect of a rapid response team on hospital-wide mortality and code rates outside the ICU in a Children's Hospital. JAMA, 2007.PMID 18029830
- [8]Pronovost P, Needham D, Berenholtz S, Sinopoli D An intervention to decrease catheter-related bloodstream infections in the ICU. The New England journal of medicine, 2006.PMID 17192537
- [9]Catchpole KR, de Leval MR, McEwan A, Pigott N Patient handover from surgery to intensive care: using Formula 1 pit-stop and aviation models to improve safety and quality. Paediatric anaesthesia, 2007.PMID 17474955
- [10]Eppich WJ, Brannen M, Hunt EA Team training: implications for emergency and critical care pediatrics. Current opinion in pediatrics, 2008.PMID 18475092
- [11]Cheng A, Donoghue A, Gilfoyle E, Eppich W Simulation-based crisis resource management training for pediatric critical care medicine: a review for instructors. Pediatric critical care medicine, 2012.PMID 21499181
- [12]Reader TW, Flin R, Mearns K, Cuthbertson BH Team situation awareness and the anticipation of patient progress during ICU rounds. BMJ quality & safety, 2011.PMID 21700727
- [13]Starmer AJ, Spector ND, Srivastava R, West DC Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [14]Al-Sawai A Leadership of healthcare professionals: where do we stand? Oman medical journal, 2013.PMID 23904925
- [15]Berghout MA, Fabbricotti IN, Buljac-Samardzic M, Hilders CG Medical leaders or masters? A systematic review of medical leadership in hospital settings. PloS one, 2017.PMID 28910335
- [16]Sfantou DF, Laliotis A, Patelarou AE, Sifaki-Pistolla D Importance of Leadership Style towards Quality of Care Measures in Healthcare Settings: A Systematic Review. Healthcare (Basel), 2017.PMID 29036901
- [17]Reeves S, Perrier L, Goldman J, Freeth D, Zwarenstein M Interprofessional education: effects on professional practice and healthcare outcomes. The Cochrane database of systematic reviews, 2013.PMID 23543515