Paeds · professional-practice-and-evidence
Medication safety and error prevention in children
Also known as Paediatric medication errors · Adverse drug events in children · Tenfold dosing errors · Safe paediatric prescribing · Medication Without Harm children
Fellowship guide to medication safety and error prevention in children: the medication-use process, why children are vulnerable, error classification and harm severity, the Swiss-cheese mechanism, high-risk drugs, tenfold dosing errors, and the layered prevention and response system.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A registrar writes an opioid infusion for a six-month-old. The pump is set ten times too fast. The nurse notices the baby is dusky and stops it. Your first job is clinical rescue. Your second job is to understand medication safety and error prevention in children so the next infant is protected. This leaf owns that pathway; the broader human-factors and incident-reporting theory lives on the adverse-events page. [1] [13]
A medication error is any preventable event that may cause or lead to inappropriate medication use or patient harm while the drug is in the control of a clinician, patient or carer. An adverse drug event (ADE) is actual injury caused by a medication — not every error causes an ADE, and not every ADE starts with an error. An adverse drug reaction is an intrinsic, often non-preventable pharmacological response. A near miss is an error caught before it reaches the child. Holding these four ideas apart is half the viva. [1] [2]
Classification
Classify every event along three axes the examiner expects: where in the process, how much harm, and how preventable. The medication-use process runs prescribing → transcribing → dispensing → administration → monitoring. Prescribing is the most error-prone stage; administration is where harm is most often realised. Separating the stage tells you which defence to strengthen. [1] [6]
Harm severity is graded on an index that rises from no error, through no harm and temporary harm, to permanent harm and death. This is the NCC MERP-style ladder hospitals use, and it is the language of an incident review. Preventability sits alongside it — most errors cause no harm, but the preventable minority that reach a child can be devastating, especially in neonates and intensive care. [2] [5]

Four terms that trip up candidates
- Preventable process failure
- May or may not reach the child
- May or may not cause harm
- Actual harm from a drug
- Often but not always from an error
- Needs rescue and disclosure
- Intrinsic pharmacological response
- Often non-preventable
- Report but not always an error
- Error caught before reaching the child
- High learning value
- Still report — free lesson
Epidemiology & Risk Factors
Kaushal's landmark JAMA study showed medication errors and preventable ADEs are substantially more common per paediatric admission than in adults, with the youngest and sickest children at greatest risk. Miller's systematic review confirmed the highest error rates cluster in neonatal and paediatric intensive care, where dilution maths, infusions and off-label use converge. Ghaleb quantified the incidence and nature of prescribing and administration errors in paediatric inpatients. [1] [5] [6]
Risk concentrates wherever weight-based calculation meets acuity. Tenfold dosing errors are a recurring high-severity pattern, and Kozer showed that the reported incidence depends heavily on how hard you look. Ameer's review of hospital administration errors confirmed administration as a persistent failure point, while Bonafide linked nurse interruptions directly to administration errors in a PICU. Children with medical complexity, polypharmacy and repeated handoffs carry the heaviest exposure. [8] [12] [10]
Pathophysiology
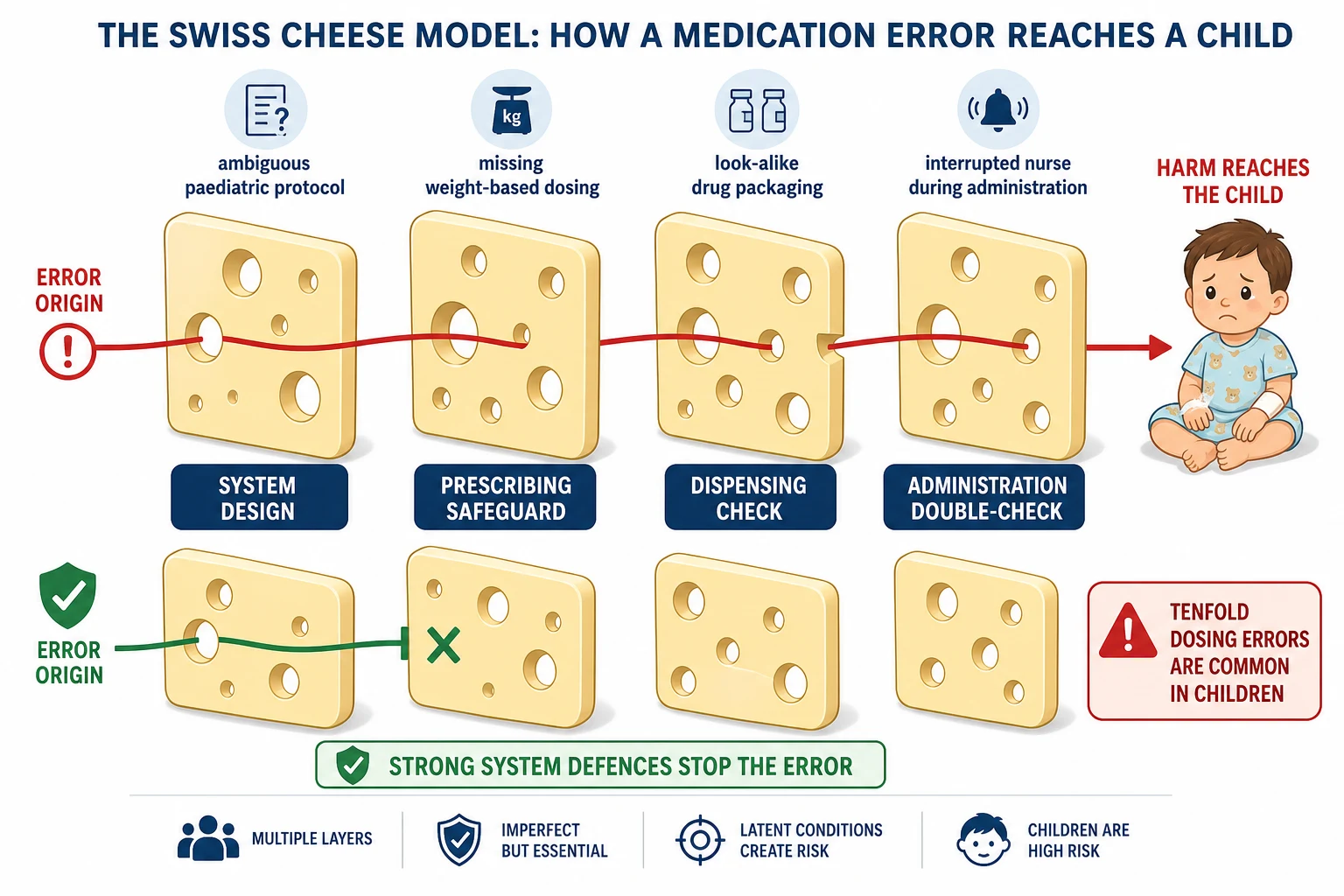
Think in layers. Latent conditions sit in the system for weeks — ambiguous paediatric protocols, look-alike packaging, understaffing, missing weight-based references, an interruption-prone drug-round. Active failures are the sharp-end slips, lapses and mistakes on a busy shift. When holes in successive defences align, the error passes through every check and reaches the child. That is Reason's Swiss-cheese model, applied to the medication-use process. [13] [2]
Paediatric pharmacology adds weight. Neonates and infants have immature hepatic metabolism and renal clearance, so the therapeutic window is narrow and a modest overdose can be lethal. Weight-based dosing in mg per kg turns one adult dose into a continuum of paediatric values, and a misplaced decimal — writing 10.0 instead of 1, or .5 instead of 0.5 — produces a tenfold error. Unit confusion between mg, mcg and units on insulin or digoxin does the same. Off-label and unlicensed prescribing removes the safety net of an established reference dose. [1] [8]
Clinical Presentation
A medication error presents as unexpected clinical change — a baby who becomes apnoeic after an infusion, a child with hypoglycaemia after insulin, an arrhythmia after an electrolyte push, or simply "this child looks wrong." Prescribing errors surface as wrong drug, wrong dose, wrong route, wrong frequency, or an allergy that was not checked. Administration errors present as a wrong-rate infusion, an omitted or duplicated dose, or a smart-pump alarm that was silenced rather than read. [1] [6]
Near misses present as good catches. The wrong drawer is opened and closed, a tenfold dose is spotted at the double-check, a pump is reprogrammed before it runs. An empty incident dashboard on a busy ward is itself a presentation of under-reporting, not proof of safety. Antidote use — naloxone, flumazenil, glucose — is a trigger that should make you ask what went upstream. [12] [10]
Differential Diagnosis
- Adverse drug event versus disease progression in a deteriorating child — investigate both, treat the child either way. [2]
- Medication error versus adverse drug reaction, which is a non-preventable pharmacological effect. [1]
- Tenfold dosing error versus an intended dose change — read the original order and units. [8]
- Look-alike sound-alike confusion versus two genuinely similar indications. [4]
- Calculation error versus a weight or unit recording error — was the weight in kilograms?
- Omitted dose versus a dose held for a clinical reason — check the chart notes.
- Intentional overdose in an adolescent — this is safeguarding and mental health, not only a medication error.
Clinical & Bedside Assessment
Stabilise the airway, breathing and circulation first; give the reversal agent if one exists; stop the infusion. Only then assess the error. Confirm the actual dose, units, weight in kilograms, route and time against the original order and the drug that was given. Rate severity on your hospital's harm index — do not invent a scale in the viva. Identify which stage of the medication-use process failed. Screen for other children exposed to the same batch, protocol or pump setting, and preserve the syringe, bag, pump settings and order trail before the bedside is cleared. [1] [4]
The five rights of administration
Investigations
Clinical investigation serves the child: a drug level where relevant, a glucose, electrolytes, and an ECG for any pro-arrhythmic overdose. Systems investigation is how the next child stays safe. Use chart review, the order-entry audit trail, pump logs, staff interviews and a structured analysis that maps latent conditions rather than stopping at the last person who touched the syringe. Trigger-tool methods — antidote use, abrupt stops, transfers to higher care — find medication harm that voluntary reports miss. Pharmacy should review the prescribing against a paediatric reference and the administration against the medication record. Document a factual timeline without blame adjectives. [2] [13]
Management — Resuscitation
- Rescue the child — airway, breathing, circulation; give the reversal agent if one exists and call for senior help. [1]
- Stop the hazard — stop the infusion, remove the wrong drug, isolate look-alike stock for this child and others. [4]
- Escalate to the consultant, pharmacy and unit leadership. [3]
- Preserve evidence — pump, syringe, bag, settings, order trail. [13]
- Communicate early with the family that something unexpected happened and care is focused on safety; full disclosure follows as facts clarify. [1]
Management — Definitive & Stepwise
Prevention is a layered system, not a memory test. Standardise prescribing with computerised prescriber order entry carrying paediatric weight-based decision support and dose-range checking. Weigh every child in kilograms and reconcile medicines at every transition. Require an independent double-check by two clinicians for high-risk drugs, infusions and patient-controlled analgesia. Administer with smart pumps running paediatric drug libraries and minimise interruptions during preparation and administration. Monitor for early adverse events, empower nurses and families to question a dose, and keep reversal agents accessible. Potts and Jani each showed computerised order entry cuts prescribing errors; Bonafide showed interruptions drive administration errors; Konwinski tested the human factors of the double-check itself. [7] [11] [10] [14]
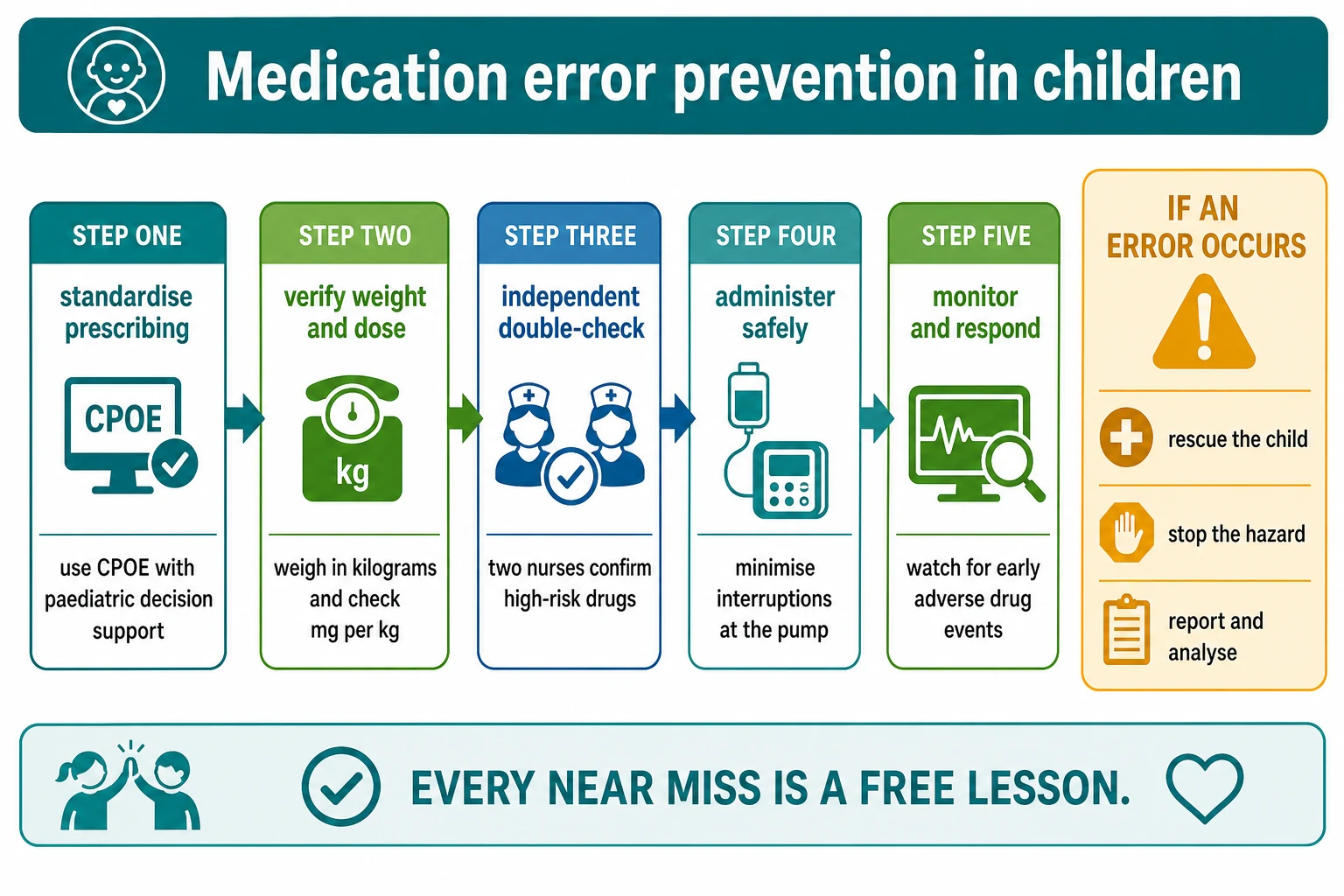
Preventing a paediatric medication error — layered sequence
Standardise prescribing with CPOE and paediatric decision support
Weigh in kilograms and confirm the mg per kg dose and maximum
Independent double-check for high-risk drugs and infusions
Administer with a smart pump and minimise interruptions
Monitor for early adverse drug events
Report every near miss and analyse the system
Specific Subtypes & Scenarios
High-risk drugs. Insulin, opioids, sedatives, anticoagulants, chemotherapy, concentrated electrolytes and inotropes have a narrow therapeutic index or look-alike packaging. They earn an independent double-check and a standard concentration every time. [4] [14]
Tenfold dosing error. Read decimal points and units carefully. Never write a trailing zero, always write a leading zero before a decimal, and confirm the weight. A weight-based check and an independent double-check are the strongest defences. [8]
Neonatal and paediatric intensive care. Dilution and infusion-rate calculations, standard concentrations and smart-pump libraries concentrate the risk. This is where the highest error rates live. [5] [7]
Emergency department and procedural sedation. Time pressure and verbal orders raise prescribing error; standardised protocols and written orders lower it. A short tutorial on paediatric prescribing can cut errors in the ED. [9]
Out-of-hospital and caregiver dosing. Dosing-device confusion and spoon-in-millilitre errors are common. Counsel with an oral syringe marked in millilitres and a written plan, using a trained interpreter when needed. [12]
Decision-support alerts. Over-sensitive alerts breed override fatigue — clinicians dismiss warnings they judge irrelevant, so the real warning is lost. Tune the system, then trust it. [15]
Complications & Pitfalls
- Writing a trailing zero (10.0 read as 100) or omitting a leading zero (.5 read as 5) — decimal errors are the engine of tenfold overdose. [8]
- Confusing mg, mcg and units on insulin or digoxin. [4]
- Relying on voluntary incident reports alone, which under-detect harm. [13]
- Choosing weak actions — posters and re-education — for a design problem that needs a forcing function. [2]
- A blame-focused response that suppresses further reporting and hides latent conditions. [13]
- Failing to reconcile medicines at admission, transfer and discharge, producing duplicated or omitted therapy. [5]
Prognosis & Disposition
Most medication errors cause no or temporary harm when they are caught. The preventable minority that reach the child can be severe, especially tenfold errors in neonates and intensive care. A successful outcome is clinical recovery plus durable system change: recurrence falls, families trust the process, and staff still report. Disposition follows clinical need; governance closure requires completed strong actions with owners and dates, not a filed form. Honest disclosure and a clear plan shape family trust and the longer-term safety culture. [1] [2]
Special Populations
Neonates and infants are the highest-risk group because of immature organ function, grams-versus-kilograms weight ambiguity and frequent off-label use. Children with medical complexity and technology dependence concentrate risk through polypharmacy, multiple prescribers and home infusions, so medicine reconciliation is essential at every transition. Children with disability or neurodiversity may communicate an adverse drug event only as behaviour or vital-sign change. Migrant and language-discordant families need trained interpreters and translated written dosing plans. Out-of-home care and rural-remote retrieval multiply fragmented-record and handoff risk. [5] [12]
Evidence, Guidelines & Regional Differences
Kaushal's JAMA study and Leape's systems analysis anchor paediatric and adult medication-error epidemiology. Fortescue ranked paediatric prevention strategies by effectiveness, and Stucky's AAP policy set the inpatient prevention standard. Miller's and Ameer's systematic reviews synthesise prescribing and administration error epidemiology. Potts and Jani proved computerised order entry reduces paediatric prescribing errors; Jani later warned of decision-support alert fatigue. Kozer quantified tenfold errors and the effect of detection method, Bonafide linked interruptions to administration errors, and Konwinski examined the human factors of the double-check. Reason's Swiss-cheese model remains the theoretical backbone. [1] [3] [8] [10] [13] [14]
Apply the Australian Commission on Safety and Quality in Health Care medication-safety guidance and the National Medicines Policy. Use local high-alert-medicine lists and independent-double-check policy. State formulary cut-offs by name rather than from memory. [3]
Controversies: how reliable voluntary reporting is, whether double-checks add value or theatre, alert fatigue from over-sensitive decision support, and how to reach the WHO Medication Without Harm goal of halving severe avoidable medication harm. Answer with principles and local policy, not slogans. [13] [15]
Exam Pearls
- Children are vulnerable because dosing is weight-based in mg per kg. [1]
- Five rights: right patient, drug, dose, route, time. [4]
- Tenfold errors come from decimals and units — never write a trailing zero. [8]
- Prescribing fails most; administration harms most. [5] [6]
- Strong actions beat posters: forcing functions, standardisation, CPOE with decision support. [2] [7]
- Every near miss is a free lesson — report it. [13]
- NICU and PICU carry the highest risk. [5]
- Independent double-checks target high-risk drugs, infusions and PCA. [14]
- Minimise interruptions during medication preparation and administration. [10]
- WHO Medication Without Harm aims to halve severe avoidable medication harm.
References
- [1]Kaushal R Medication errors and adverse drug events in pediatric inpatients. JAMA, 2001.PMID 11311101
- [2]Leape LL Systems analysis of adverse drug events. ADE Prevention Study Group. JAMA, 1995.PMID 7791256
- [3]Fortescue EB Prioritizing strategies for preventing medication errors and adverse drug events in pediatric inpatients. Pediatrics, 2003.PMID 12671103
- [4]Stucky ER Prevention of medication errors in the pediatric inpatient setting. Pediatrics, 2003.PMID 12897304
- [5]Miller MR Medication errors in paediatric care: a systematic review of epidemiology and an evaluation of evidence supporting reduction strategy recommendations. Quality and safety in health care, 2007.PMID 17403758
- [6]Ghaleb MA The incidence and nature of prescribing and medication administration errors in paediatric inpatients. Archives of disease in childhood, 2010.PMID 20133327
- [7]Potts AL Computerized physician order entry and medication errors in a pediatric critical care unit. Pediatrics, 2004.PMID 14702449
- [8]Kozer E The effect of detection approaches on the reported incidence of tenfold errors. Drug safety, 2006.PMID 16454544
- [9]Kozer E The effect of a short tutorial on the incidence of prescribing errors in pediatric emergency care. Canadian journal of clinical pharmacology, 2006.PMID 17085777
- [10]Bonafide CP Association Between Mobile Telephone Interruptions and Medication Administration Errors in a Pediatric Intensive Care Unit. JAMA pediatrics, 2020.PMID 31860017
- [11]Jani YH Electronic prescribing reduced prescribing errors in a pediatric renal outpatient clinic. The Journal of pediatrics, 2008.PMID 18206691
- [12]Ameer A Systematic literature review of hospital medication administration errors in children. Integrated pharmacy research & practice, 2015.PMID 29354530
- [13]Reason J Human error: models and management. The Western journal of medicine, 2000.PMID 10854390
- [14]Konwinski L Evaluating Independent Double Checks in the Pediatric Intensive Care Unit: A Human Factors Engineering Approach. Journal of patient safety, 2024.PMID 38231892
- [15]Jani YH Characteristics of clinical decision support alert overrides in an electronic prescribing system at a tertiary care paediatric hospital. International journal of pharmacy practice, 2011.PMID 21899617