Paeds · professional-practice-and-evidence
Recognition, reporting and analysis of adverse events
Also known as Paediatric incident reporting · Adverse event analysis children · Near miss reporting paediatrics · Trigger tool paediatric safety · Patient harm investigation children
Fellowship guide to recognising, reporting and analysing paediatric adverse events and near misses: systems thinking, trigger tools, disclosure principles, second-victim support, closed-loop learning and exam defence.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A toddler’s infusion is running at ten times the ordered rate. The nurse stops the pump. The child is pale. Your first job is clinical rescue. Your second job is recognition, reporting and analysis of an adverse event so the next child is safer. This leaf owns that pathway. Deep human-factors theory also lives on the patient-safety systems page; dosing mechanics live on medication safety. [1] [2]
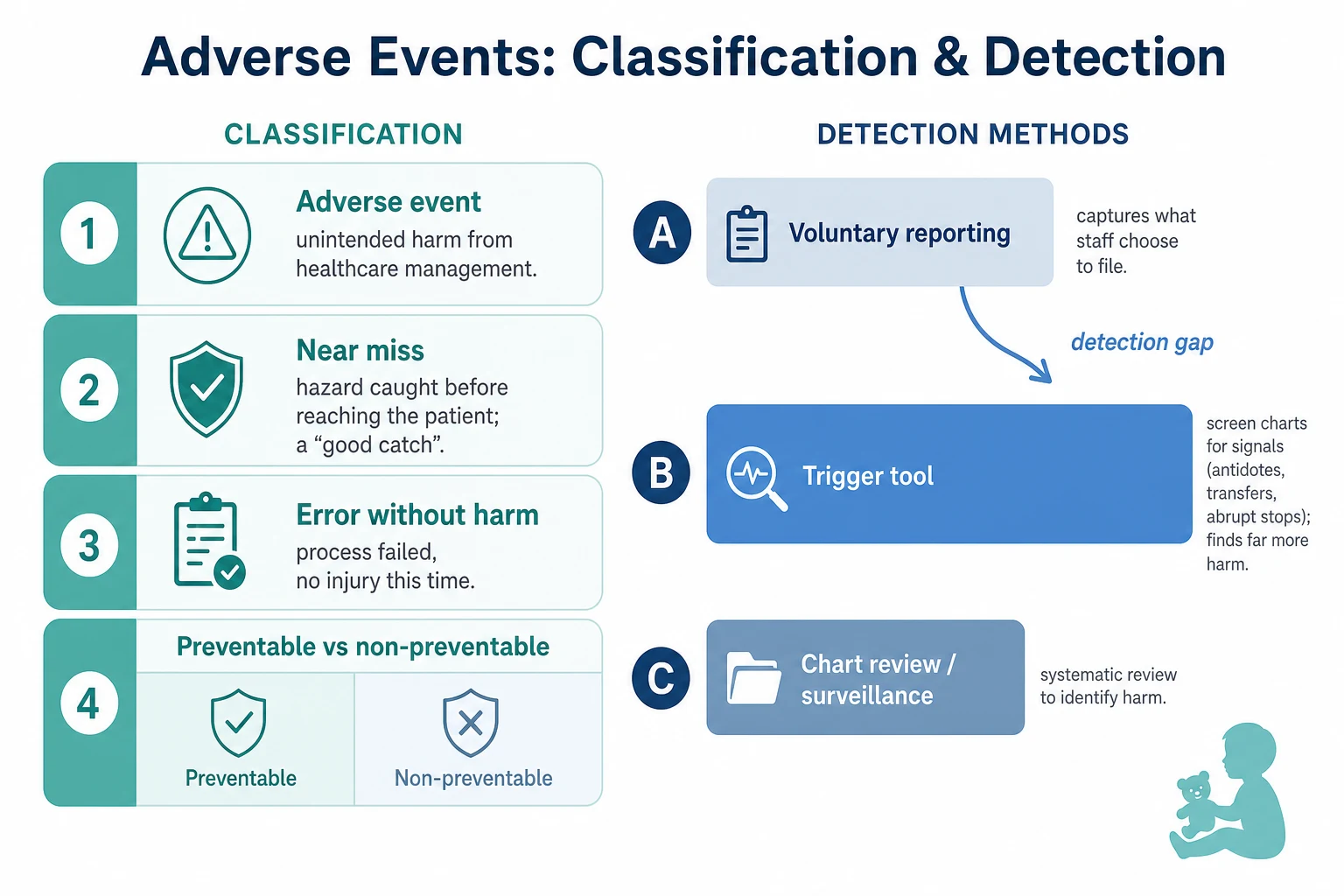
An adverse event (AE) is unintended injury or complication caused by health care management rather than the child’s disease alone. A preventable AE is one that could have been avoided with currently accepted practice. A near miss is an event that could have caused harm but did not, often because someone caught it. An error is a failure of a planned action; not every error causes harm, and not every AE is caused by a single person’s slip. [2] [3] [5]
Classification
Classify every event along three axes the viva expects: what happened, how much harm, and how preventable. Separate disease progression from care-related harm. Separate near miss from actual AE. Separate active failure at the sharp end from latent conditions in design, staffing, equipment and culture. Reason’s model remains the examinable language for that split. [1] [2]
Detection methods also classify your system’s eyesight. Voluntary reporting captures what staff choose to file. Trigger tools screen charts for signals (antidotes, transfers, abrupt stops) then confirm harm. Automated surveillance and infection metrics add other lenses. Classen showed hospital AE rates measured by global trigger methods can be an order of magnitude higher than rates inferred from voluntary reporting. [11] [10]
Event types at the bedside
- Unintended harm from care
- May or may not be preventable
- Needs rescue, report, disclose, analyse
- Hazard interrupted before harm
- High learning value
- Still report — free lesson
- Process failed
- No patient injury this time
- Still a system signal
Epidemiology & Risk Factors
Landmark adult hospital studies (Harvard Medical Practice Study; Vincent’s UK review) established that AEs are common and often preventable. Paediatrics is not a miniature adult service. Woods and colleagues quantified AEs and preventable AEs in children using large data. Matlow’s Canadian Paediatric Adverse Events Study measured hospital AE epidemiology in Canadian children. Stockwell reported AEs among hospitalised paediatric patients in a multicentre US context. NICU-focused trigger work (Sharek) shows high-risk environments generate frequent detectable events. [3] [4] [5] [6] [7] [8]
Risk rises with complexity, polypharmacy, devices, transfers and handoffs. Children with medical complexity concentrate exposure. Landrigan found little improvement in hospital harm rates over time in studied US settings — a sobering exam point against complacency. Under-reporting is worse where blame culture thrives. [12] [13] [17]
Pathophysiology
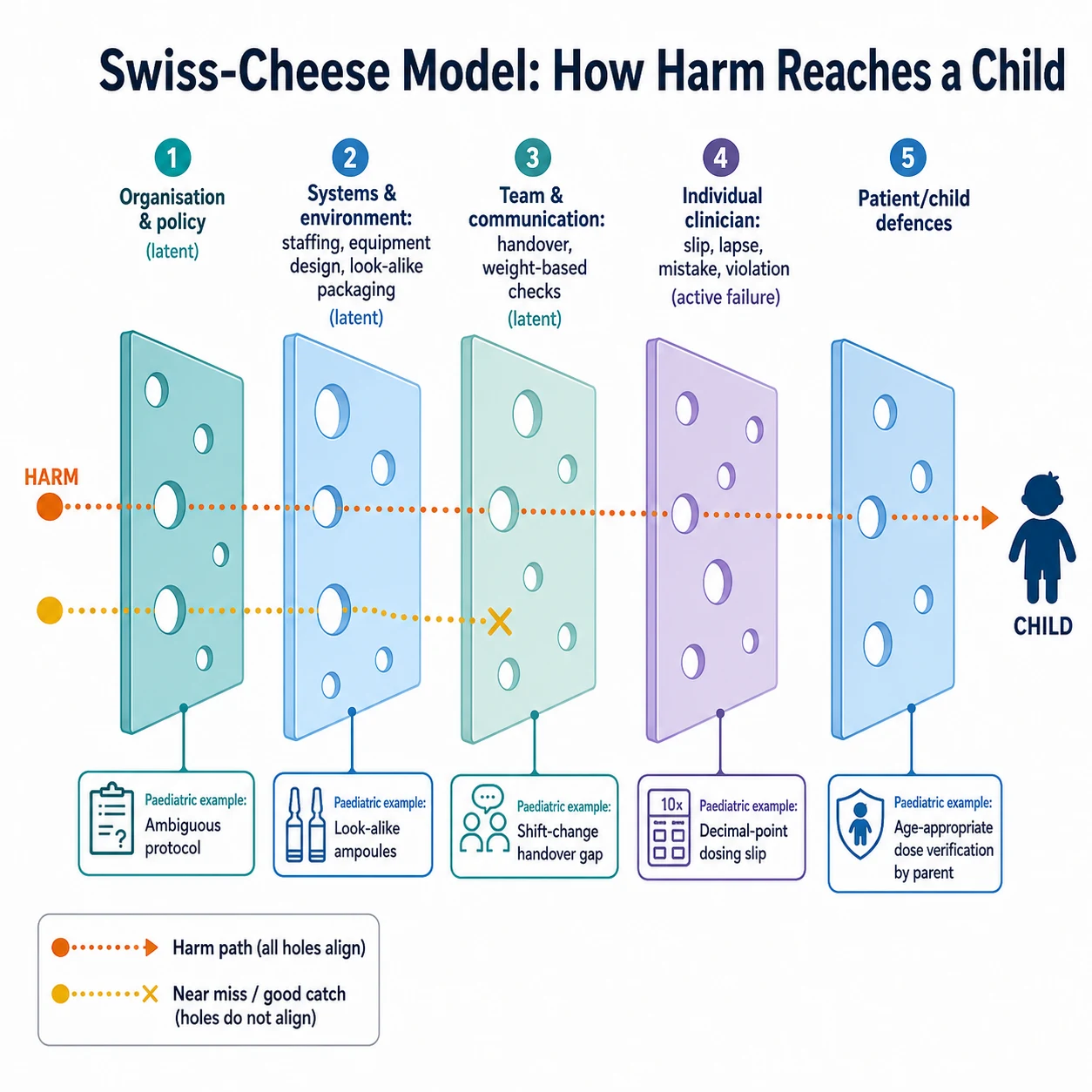
Think in layers. Latent conditions — ambiguous protocols, look-alike packaging, understaffing, poor interface design — sit in the system for months. Active failures — a slip, lapse, mistake or violation — punch through on a busy night. When holes in successive defences align, harm reaches the child. That is Reason’s Swiss-cheese teaching model. [1] [2]
Paediatric pathways add weight-based dosing, off-label use, developmental communication limits and caregiver-dependent observation. Diagnostic overshadowing in disability can hide new harm under “usual baseline.” Communication failures at shift change convert a contained risk into a ward-wide event. After serious events, second-victim distress can impair the next clinician’s performance if support is absent. Incomplete analysis that stops at “be more careful” leaves latent holes open. [15] [17]
Clinical Presentation
AEs present as clinical change, family concern, device alarms, laboratory extremes, unexpected transfers, antidote use or “this feels wrong.” Near misses present as good catches — the wrong drawer opened and closed, the pump reprogrammed in time. Delayed diagnosis AEs present as prolonged untreated illness after missed red flags. Handoff failures present as omitted overnight tasks, missed antibiotics or unknown allergies after shift change. Empty incident dashboards in a busy unit are themselves a presentation of under-reporting, not proof of safety. [8] [9] [13]
Differential Diagnosis
- Preventable AE versus unavoidable complication of severe disease. [5]
- Near miss versus hazardous condition without a discrete event. [1]
- System design failure versus isolated human slip — usually both. [1]
- Device failure versus use error versus both. [8]
- Natural history versus iatrogenic harm.
- Family dissatisfaction without harm versus true AE — both need listening; only one is an AE. [14]
- Second-victim distress versus unrelated mental health crisis — support either way. [15]
- Safeguarding issues that supersede standard incident workflows.
Clinical & Bedside Assessment
Stabilise ABCs and stop the hazard first. Then assess: what happened, who is at risk now, what records and devices must be preserved, who needs to know. Document a factual timeline without blame adjectives. Notify the consultant and local safety pathway. Check whether other children share the same drug batch, device or protocol. Screen the reporting clinician for acute distress. Rate severity using your hospital’s tool — do not invent a scale in the viva; name the local framework. [1] [18]
Investigations
Investigation means learning, not theatre. Immediate clinical tests serve the child. Safety investigation uses chart review, interviews, device inspection and sometimes trigger-tool methods. Paediatric medication trigger tools (Takata), NICU tools (Sharek) and paediatric Global Trigger Tool applications (Kirkendall) show how structured review finds harm voluntary systems miss. ICU trigger methods (Resar) illustrate the broader approach. Root-cause or systems analysis should map latent conditions, not only the last person touching the child. Look up local mandatory reporting thresholds rather than inventing them. [8] [9] [10] [11]
Management — Resuscitation
- Rescue the child — airway, breathing, circulation, antidotes, stop infusions, call for help. [2]
- Stop the hazard for this child and others. [1]
- Escalate to senior clinicians and unit leadership. [18]
- Preserve evidence — pumps, labels, bags, settings, notes. [1]
- Communicate early with the family that something unexpected happened and care is focused on safety. Full disclosure follows as facts clarify. [14]
Management — Definitive & Stepwise
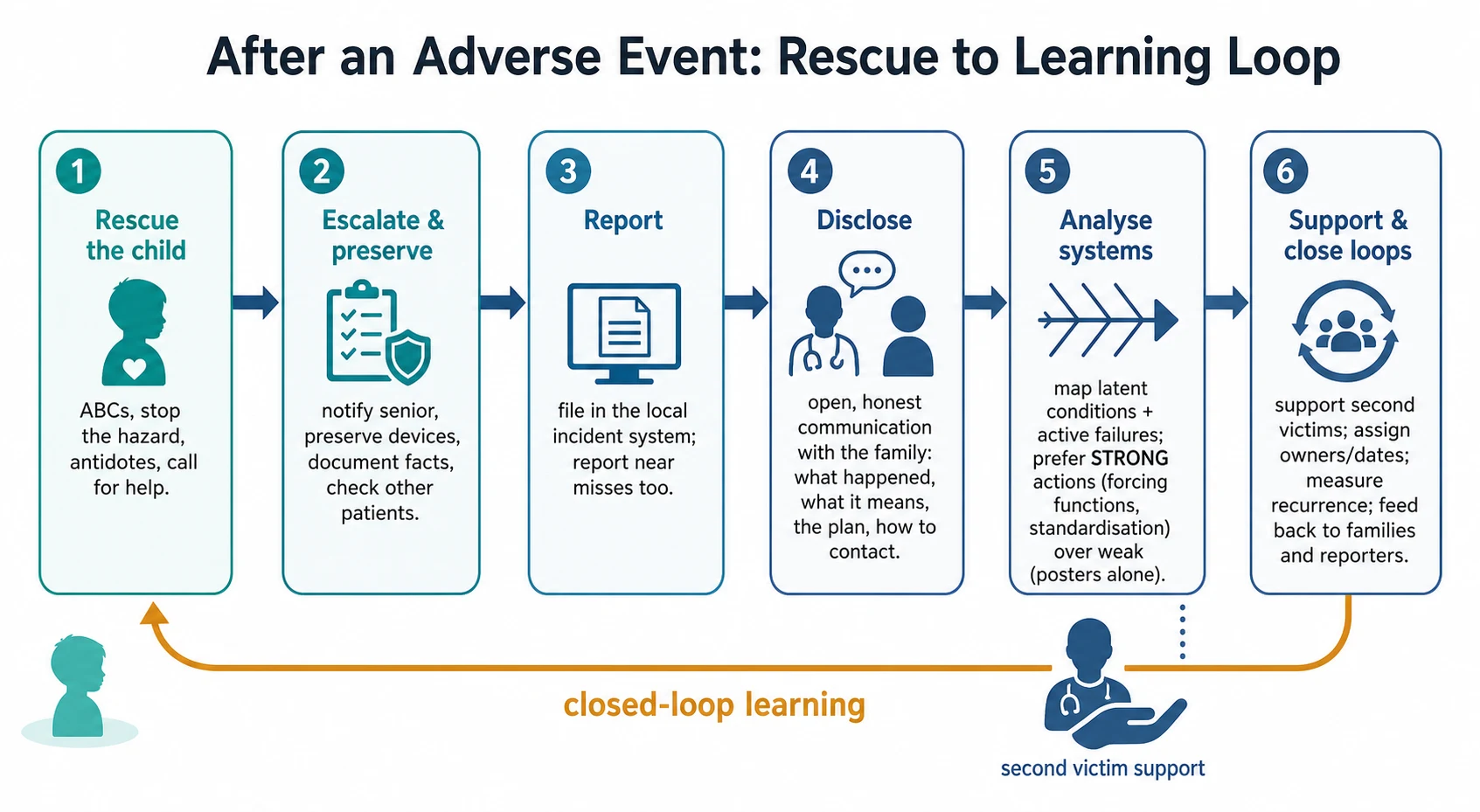
Report promptly in the local incident system. Classify harm and preventability with a team. Disclose using open, plain language: what happened, what it means, what is being done, and how to contact you — families want honesty; Gallagher’s work shows patients value disclosure more than many clinicians fear. Analyse with systems methods. Choose strong actions (forcing functions, standardisation, equipment redesign, staffing, forcing double-checks that work) over weak actions (re-education posters alone). Implement, assign owners and dates, and measure recurrence. Support second victims. Close the loop with family and reporters. Handoff redesign such as I-PASS-type structured communication reduces medical errors and is a concrete prevention lever after communication AEs. Infection-prevention bundles (Pronovost’s central-line work) show system interventions can drive harm down. [13] [14] [15] [16]
After an adverse event — practical sequence
Stabilise the child and stop the hazard
Escalate and preserve facts and devices
Report in the incident system
Disclose to the family with humility and a plan
Systems analysis with strong actions and owners
Support second victims and close learning loops
Specific Subtypes & Scenarios
Medication AE. Use paediatric trigger thinking; check weight, dilution and pump libraries; involve pharmacy. [9]
Handoff AE. Reconstruct what was omitted; redesign with structured handoff rather than “try harder.” [13]
NICU device AE. High trigger density; preserve device data. [8]
Complex chronic child. Multi-team fragmentation is a latent condition — coordinate care. [17] [18]
Near miss good catch. Celebrate reporting; fix the latent hole that required heroics. [1]
Second victim. Name it, relieve from high-risk tasks if needed, offer peer support. [15]
Complications & Pitfalls
- Blame culture that kills reporting. [2]
- Reporting without analysis or action. [1]
- Weak actions for design problems. [1]
- Delayed or incomplete disclosure. [14]
- Ignoring near misses. [11]
- Failing to screen other exposed patients. [8]
- Neglecting second victims. [15]
- Inventing legal duties not in local policy.
- Vanity metrics without closed loops.
Prognosis & Disposition
Successful outcomes are clinical recovery plus system learning: recurrence falls, families trust the process, staff still report. Disposition of the child follows clinical need. Governance “closure” requires completed actions, not a filed form. Disclosure quality influences trust and sometimes legal trajectory; honesty remains the ethical default. Safety-net families with clear contacts if symptoms evolve after an event. [14] [16]
Special Populations
Neonates and NICU need device- and medication-focused surveillance. Non-verbal children may show harm only as behaviour or vital-sign change. Adolescents may want direct disclosure involvement. Indigenous and language-discordant families need interpreters and culturally safe processes. Rural retrieval multiplies handoff risk. Out-of-home care needs careful record continuity. Staff of all seniority can be second victims. [8] [13] [15] [17]
Evidence, Guidelines & Regional Differences
Reason and Leape frame systems error thinking. Brennan/Harvard and Vincent quantify hospital AEs. Woods, Matlow and Stockwell anchor paediatric epidemiology. Sharek, Takata and Kirkendall operationalise paediatric trigger detection. Classen exposes voluntary-report blindness. Landrigan challenges assumptions of automatic improvement. Starmer proves structured handoff reduces errors. Gallagher and Wu cover disclosure and second victims. Pronovost shows system bundles can cut harm. [1] [5] [6] [11] [13] [14] [15] [16]
Use local incident systems and the Australian Open Disclosure Framework principles: open, timely, supportive communication after harm. Look up state mandatory notification rules rather than inventing them. [14]
Controversies: how much reporting should be mandatory; legal privilege of quality reviews; where just culture draws the line between system support and individual accountability. Answer with principles and local policy, not slogans. [1] [2]
Exam Pearls
- Rescue first, then report and analyse. [2]
- Near misses are gold — file them. [11]
- Voluntary reports undercount; triggers find more. [11] [10]
- Swiss cheese: latent + active. [1]
- Strong system actions beat posters. [16]
- Families want honest disclosure. [14]
- Second victims need care. [15]
- Structured handoff reduces medical errors. [13]
- Paediatric risk includes weight-based meds and devices. [8] [9]
- Close loops with families and reporters. [18]
References
- [1]Reason J Human error: models and management. The Western journal of medicine, 2000.PMID 10854390
- [2]Leape LL Error in medicine. JAMA, 1994.PMID 7503827
- [3]Brennan TA Incidence of adverse events and negligence in hospitalized patients. Results of the Harvard Medical Practice Study I. The New England journal of medicine, 1991.PMID 1987460
- [4]Vincent C Adverse events in British hospitals: preliminary retrospective record review. BMJ (Clinical research ed.), 2001.PMID 11230064
- [5]Woods D Adverse events and preventable adverse events in children. Pediatrics, 2005.PMID 15629994
- [6]Matlow AG Adverse events among children in Canadian hospitals: the Canadian Paediatric Adverse Events Study. CMAJ : Canadian Medical Association journal = journal de l'Association medicale canadienne, 2012.PMID 22847964
- [7]Stockwell DC Adverse Events in Hospitalized Pediatric Patients. Pediatrics, 2018.PMID 30006445
- [8]Sharek PJ Adverse events in the neonatal intensive care unit: development, testing, and findings of an NICU-focused trigger tool. Pediatrics, 2006.PMID 17015521
- [9]Takata GS Development, testing, and findings of a pediatric-focused trigger tool to identify medication-related harm in US children's hospitals. Pediatrics, 2008.PMID 18381521
- [10]Kirkendall ES Measuring adverse events and levels of harm in pediatric inpatients with the Global Trigger Tool. Pediatrics, 2012.PMID 23045558
- [11]Classen DC 'Global trigger tool' shows that adverse events in hospitals may be ten times greater than previously measured. Health affairs (Project Hope), 2011.PMID 21471476
- [12]Landrigan CP Temporal trends in rates of patient harm resulting from medical care. The New England journal of medicine, 2010.PMID 21105794
- [13]Starmer AJ Changes in medical errors after implementation of a handoff program. The New England journal of medicine, 2014.PMID 25372088
- [14]Gallagher TH Patients' and physicians' attitudes regarding the disclosure of medical errors. JAMA, 2003.PMID 12597752
- [15]Wu AW Medical error: the second victim. The Western journal of medicine, 2000.PMID 10854367
- [16]Pronovost P An intervention to decrease catheter-related bloodstream infections in the ICU. The New England journal of medicine, 2006.PMID 17192537
- [17]Kuo DZ Recognition and Management of Medical Complexity. Pediatrics, 2016.PMID 27940731
- [18]Turchi RM Patient- and family-centered care coordination: a framework for integrating care for children and youth across multiple systems. Pediatrics, 2014.PMID 24777209