Paeds · professional-practice-and-evidence
Trauma-informed paediatric care
Also known as Trauma-informed care in paediatrics · TIC for children · Adverse childhood experiences and toxic stress · SAMHSA trauma-informed approach · Preventing medical traumatic stress
Fellowship guide to trauma-informed paediatric care: the SAMHSA four Rs and six principles; the ACE study and toxic-stress mechanism; recognising trauma across age groups; the trauma-informed encounter and procedural adaptations; screening safely; building resilience; preventing medical traumatic stress; and ANZ/UK/US/Canada system and cultural considerations.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
The 4 Rs of trauma-informed care
Overview & Definition
An eight-year-old freezes and becomes mute when you reach for the otoscope. A toddler in the ED screams through a cannula insertion while being held down by three adults. A teenager in foster care refuses to speak to any clinician. Each of these is a trauma response, and each is an invitation to do harm or to do better. [10] [11]
Trauma, in the SAMHSA definition, means an event or set of circumstances experienced as physically or emotionally harmful or life-threatening, with lasting adverse effects on functioning and wellbeing. It is the lived experience and its aftermath — not the event alone. [10]
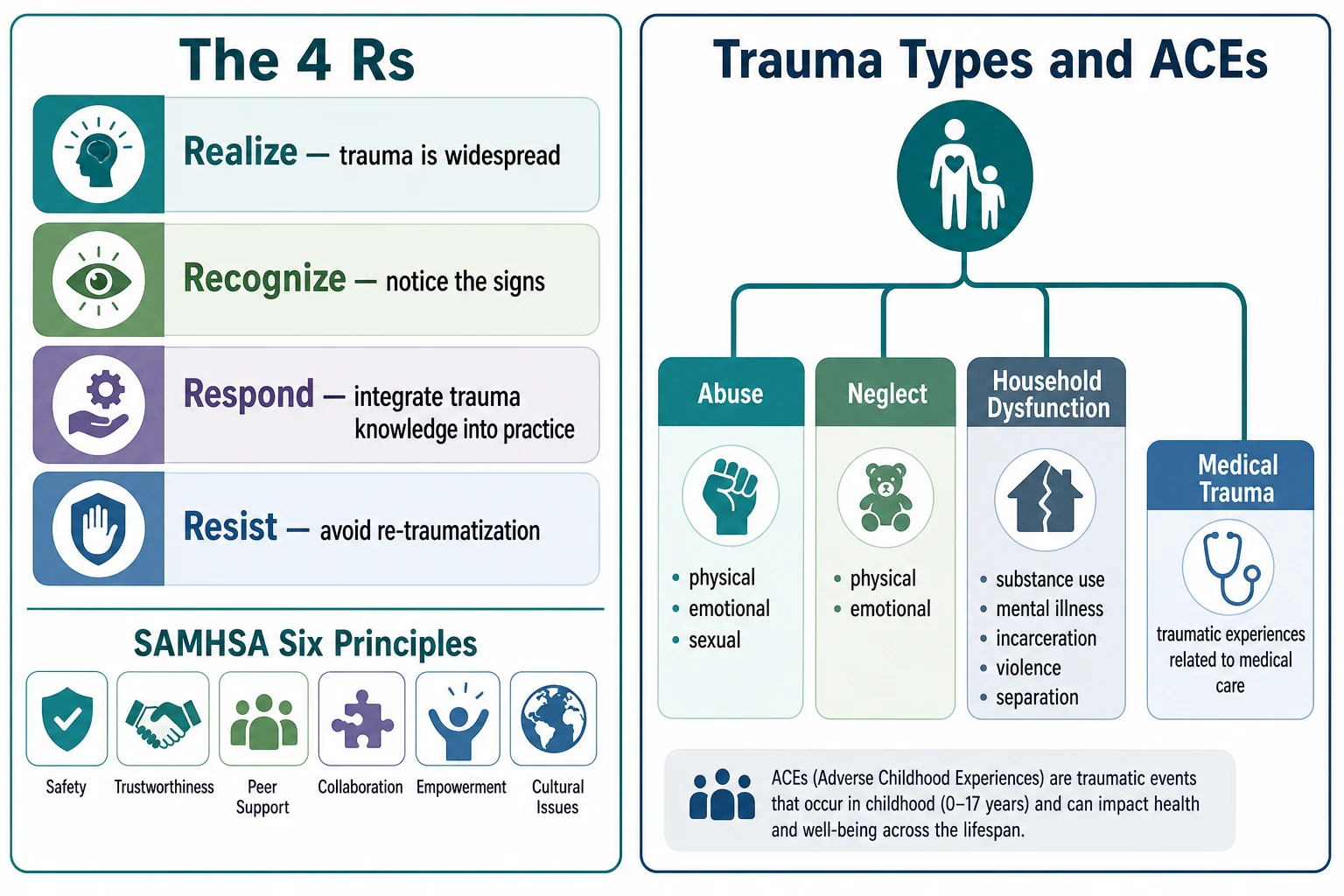
Trauma-informed care is the organisational and clinical approach that follows from that realisation. The SAMHSA framework asks every member of the workforce to realise the prevalence of trauma, recognise its signs, respond by integrating that knowledge into practice, and resist re-traumatising the people they serve. [9] [10]
This page owns the practice, framework and evidence of TIC. Cross-link dedicated leaves for child maltreatment and safeguarding, breaking bad news, shared decision-making, consent and mature-minor frameworks, and working with interpreters — do not rebuild their content here. [10]
Classification
Sort the work by the framework you are operating within and the type of trauma the child carries. [9] [10]
The four Rs are the operational heart of TIC: Realise that trauma is pervasive; Recognise its signs in patients, families and staff; Respond by changing policy and practice; Resist re-traumatising through restraint, powerlessness or unpredictability. [10]
The six SAMHSA principles tell you what good looks like: Safety in the physical and psychological setting; Trustworthiness and transparency in what you say and do; Peer support between families who share experience; Collaboration that shares power; Empowerment that offers voice and choice; and attention to Cultural, historical and gender issues. [9] [10]
Trauma types. Abuse — physical, emotional and sexual. Neglect — physical and emotional. Household dysfunction — parental substance use, mental illness, incarceration, domestic violence, and separation. Each carries its own pattern of injury and its own re-traumatisation triggers. [1] [6]
Epidemiology & Risk Factors
Childhood adversity is not rare — it is the rule, not the exception, in the populations paediatrics serves. [1] [6]
The ACE Study (Felitti 1998) established a dose-response relationship between the number of adverse childhood experiences and the leading causes of adult death. As ACE count rises, so does the risk of ischaemic heart disease, cancer, chronic lung disease, liver disease, depression, suicide and substance use. [1]
Hughes's 2017 meta-analysis confirmed and extended this: across 37 million people in 20 countries, there is a strong, graded dose-response between cumulative ACE exposure and mental and physical health outcomes throughout life. [4] Bellis's 2019 follow-up quantified the annual economic cost — hundreds of billions across Europe and North America. [5]
The prevalence is sobering. Finkelhor's national survey found that a substantial proportion of children experience direct or witnessed violence, abuse or crime each year, and many experience multiple types. [6]
Medical events themselves are a source of trauma. Injury, acute critical illness, ICU admission and repeated painful procedures can produce medical traumatic stress — a point many clinicians overlook because they see themselves as helping, not harming. [12]
The burden falls unevenly. Children in out-of-home care, those in socioeconomic disadvantage, Indigenous children and refugee or asylum-seeking families carry higher cumulative adversity. [5] [10]
Despite this, most paediatricians do not routinely ask about ACEs. Kerker's 2016 study found that only a minority screen, even though the vast majority recognise the impact of adversity on health. [7] [8]
Pathophysiology
Think about the biological cascade that turns early adversity into lifelong disease — and where trauma-informed care interrupts it. [2] [3]
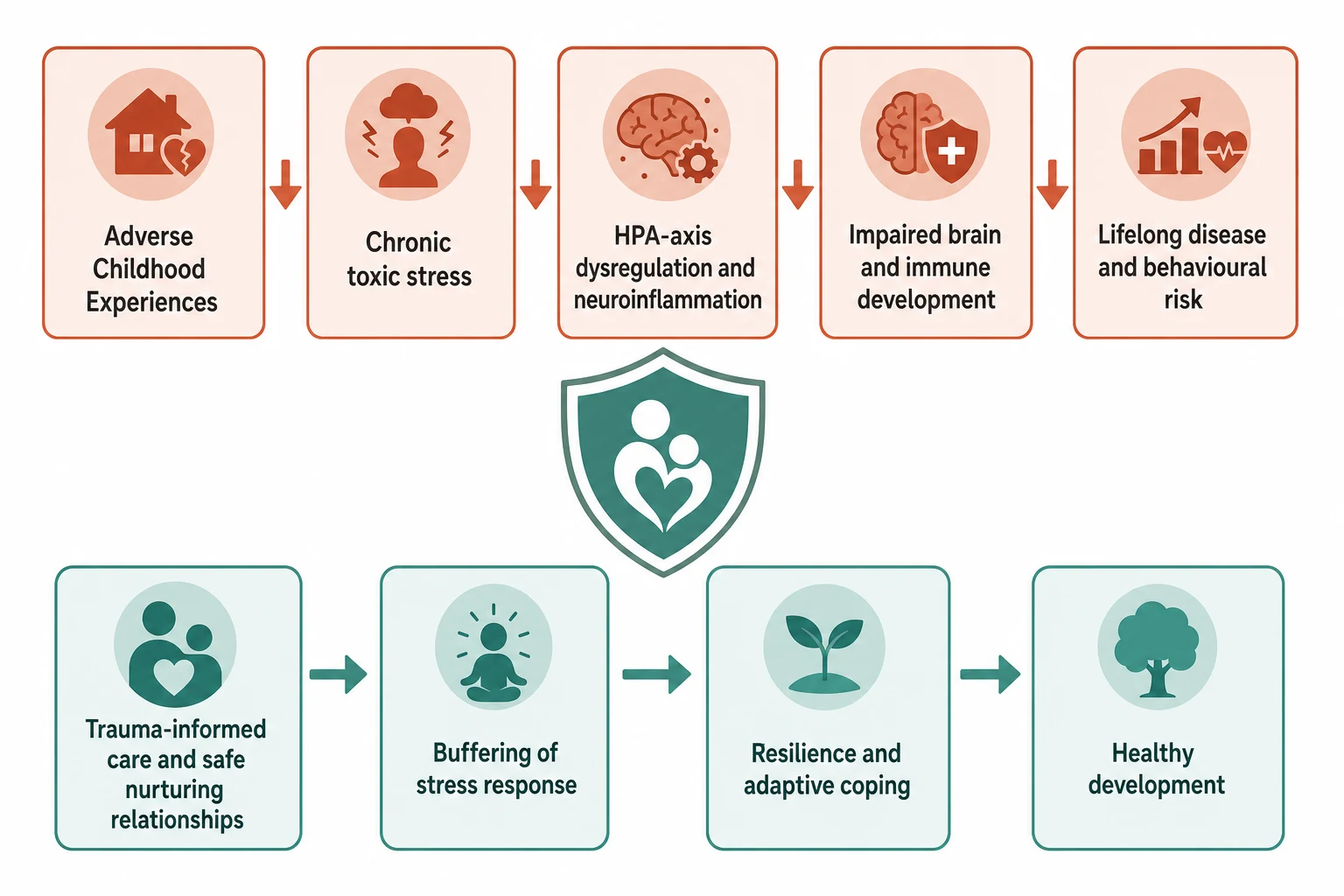
Toxic stress and the HPA axis. A single frightening event activates the fight-flight system and resolves. Chronic adversity without the buffering of a stable, caring adult keeps the hypothalamic-pituitary-adrenal axis and sympathetic nervous system activated for prolonged periods. This toxic stress floods the developing brain and body with cortisol and inflammatory mediators. [2]
Neurodevelopmental disruption. Shonkoff's work shows that toxic stress disrupts the architecture of the developing brain — pruning, myelination and synaptogenesis — and alters immune and metabolic regulation. The prefrontal cortex, hippocampus and amygdala are especially vulnerable. [2] [3]
Epigenetic and systemic change. Sustained stress produces lasting epigenetic modifications, telomere shortening and chronic neuroinflammation — the biological substrate that links ACEs to cardiovascular disease, mental illness, autoimmunity and early mortality decades later. [1] [4]
Resilience is ordinary magic. Masten's framework shows that resilience is not a rare trait but the product of ordinary, adaptive systems — most powerfully, the presence of a safe, stable, nurturing adult relationship that buffers the stress response. [13]
Medical traumatic stress. The healthcare encounter itself can drive the same cascade. Pain, separation from caregivers, fear, and loss of control during procedures and admissions activate the stress system and can produce lasting traumatic stress in children. [11] [12]
Clinical Presentation
Trauma does not always announce itself. It hides inside the presentations you see every day. [10] [11]
Behavioural signs. Hypervigilance, an exaggerated startle, aggression, withdrawal, dissociation, emotional dysregulation, regression in milestones or toileting, and sleep disturbance. A child who freezes when you reach for them is giving you information, not defiance. [10] [11]
Somatic presentations. Unexplained or recurrent pain, headaches, abdominal pain, enuresis, feeding difficulty and functional symptoms. These are real; the mechanism is the stress system, not malingering. [2] [10]
Developmental regression. Loss of language, milestones or toileting after a frightening event — an injury, a hospital admission, a frightening procedure, or a change in the family — is a hallmark of trauma in a young child. [10]
Medical-event trauma. A child who becomes distressed, avoidant or behaviourally changed after injury, hospitalisation, ICU admission or repeated procedures may be experiencing medical traumatic stress. Ask about it specifically. [11] [12]
Adolescent presentations. Risk-taking, self-harm, substance use, school disengagement, eating changes and distrust of adults may all be trauma-driven. The absence of a disclosed history does not exclude it. [4] [10]
Differential Diagnosis
Name the true problem before you reach for a label that misses it. [10] [2]
| You see | Consider also | Trap |
|---|---|---|
| Inattention, impulsivity, hyperactivity | Trauma-driven dysregulation vs ADHD | Treating only with stimulants while the adversity continues |
| Withdrawal, flat affect, regression | Trauma vs autism spectrum | Missing sensory or communication needs, or missing the trauma |
| Recurrent unexplained pain | Somatic stress response vs organic disease | Over-investigating or dismissing; both harm |
| Oppositional or conduct behaviour | Fight-or-flight survival response vs primary conduct disorder | Punishing survival behaviour rather than building safety |
The guiding principle. Trauma is not a diagnosis of exclusion — it is a lens you apply alongside your differential, not instead of it. A child can have both ADHD and trauma, both autism and adversity, both organic disease and somatic amplification. [10] [2]
Clinical & Bedside Assessment
Apply universal trauma precautions from the first contact. Assume every child may carry a trauma history. Greet warmly, explain what you are about to do before you do it, offer choice wherever possible, and never force a non-urgent examination on a distressed child. [9] [11]
Recognise trauma cues in real time. A child who freezes, dissociates, becomes aggressive or recoils when you approach is showing a stress response, not misbehaviour. Stop, slow down, and change your approach. [10] [11]
Ask about adversity when it is indicated and safe. Screening for ACEs has a role, but only when you have the capacity to respond. Use a validated tool, ask in a calm and private setting, and never open a door you cannot walk the family through. [7] [8]
Assess the buffering system. The single most protective factor in a child's life is a safe, stable, nurturing adult relationship. Identify who that is — a parent, grandparent, teacher, carer — and build your plan around strengthening it. [13] [3]
Offer choice and control at every step. Let the child decide which ear to examine first, whether a parent holds them, when to take a break. Small choices restore the agency that trauma strips away. [10] [11]
Investigations
The investigations here are structured assessments, not blood tests. [7] [10]
Use a validated adversity screen selectively. Tools such as the ACE questionnaire or a brief psychosocial screen help structure the conversation, but they are not screening tests in the newborn-bloodspot sense. Use them only when you can act on the answers. [7] [8]
Screen for behavioural and emotional sequelae. Instruments such as the Strengths and Difficulties Questionnaire (SDQ) or the Pediatric Symptom Checklist (PSC) help quantify the functional impact and track change over time. [10]
Investigate somatic presentations appropriately. Exclude organic disease — but do not over-investigate. Endless normal results do not reassure a family whose child's pain is driven by the stress system, and each test can itself reinforce illness behaviour. [2] [10]
Assess functional impact. How is the child functioning at school, at home, with peers? Functional impairment, not symptom count alone, determines the urgency and intensity of the response. [10]
Document with sensitivity. Record what is relevant to care, what the family has agreed can be shared, and the safety plan. Trauma-informed documentation protects the child and the clinician. [10]
Management — Resuscitation
Some moments in trauma-informed care are emergencies of a different kind. [10] [12]
Acute behavioural dysregulation. A child triggered by a clinical encounter may escalate to fight, flight or freeze. Prioritise physical safety, remove triggers, lower the sensory load, use grounding, and bring in a trusted adult. Do not add restraint to terror. [11]
Safeguarding surfaced. A trauma-informed approach can surface a disclosure of abuse or signs of maltreatment. Follow your mandatory-reporting pathway exactly as you would anywhere else — the child's safety comes before the therapeutic relationship. [10]
Medical deterioration in a frightened child. If physiology is unstable, stabilise first. Address pain and fear as part of the resuscitation, not after it. A child who is terrified cannot cooperate with care. [12]
Clinician acute distress. Working with traumatised children carries vicarious trauma. A registrar who is shaken, numbed or distressed after a difficult encounter needs immediate peer support, relief, and a debrief. [11] [10]
Management — Definitive & Stepwise
The SAMHSA four Rs translate into a six-step bedside algorithm. [9] [10]
- Universal precautions. Assume trauma may be present in every child. Create a calm, predictable, welcoming environment from the moment of arrival. [9]
- Recognise and screen. Observe for trauma cues, and when indicated and safe, ask about adversity using a validated tool with follow-up capacity. [7] [10]
- Respond. Integrate trauma knowledge into the plan. Explain before you act, offer choice, collaborate with the family, and empower the child's voice. [10] [11]
- Resist re-traumatisation. Minimise triggers. Prepare for procedures, control pain, avoid unnecessary restraint, and never strip a child of control or dignity. [11] [12]
- Connect and refer. Link the family to mental health, social work and community supports with a warm handover — not a phone number on a leaflet. [10]
- Build resilience and follow up. Strengthen the buffering relationship, schedule review, reinforce coping, and monitor progress over time. [13] [3]
What the evidence supports. Marsac's 2016 framework for implementing TIC in paediatric networks shows that organisational-level change — training, policy, environment and leadership — is what shifts outcomes, not individual clinician goodwill alone. [9]
What screening achieves. Universal ACE screening remains debated, but targeted screening with integrated follow-up improves identification and connection to services. The evidence favours building the response capacity before expanding the ask. [7] [8]

Specific Subtypes & Scenarios
ED presentation after injury or acute illness. This is the highest-yield moment to prevent medical traumatic stress. Use adequate pain control, keep the family present, explain each step, and debrief afterwards. What you do in the first hour shapes the memory. [11] [12]
Procedural setting. Prepare the child, use distraction and comfort positioning (a parent's lap, not a board), minimise restraint, use topical or local anaesthesia, and debrief. A procedure done badly can traumatise for years. [11] [10]
Ward admission of a child with known or suspected trauma. Adapt the environment: consistent staff, predictable routines, clear explanations, and a plan for what happens if the child becomes distressed. Share the plan across the team. [9] [11]
NICU stay. Protect the parent-infant bond as both the buffer and the site of risk. Support kangaroo care and breastfeeding, reduce painful procedures and cluster them, use sucrose, and recognise that parents in the NICU may themselves be traumatised. [11] [3]
Child in out-of-home care. These children carry high ACE burdens. Coordinate with carers and child protection, ensure a comprehensive health assessment, and plan care that accounts for attachment disruption and developmental trauma. [10]
Adolescent with complex trauma. Build trust slowly, respect autonomy, address risk-taking and self-harm directly, and offer confidential time. Do not expect a single encounter to overcome years of broken trust. [4] [10]
Complications & Pitfalls
- Re-traumatising a child through restraint, unexplained procedures, or power-based interactions. [11]
- Asking about ACEs without any follow-up capacity, causing distress with no support pathway. [7] [8]
- Labelling trauma-driven behaviour as primary oppositional or conduct disorder, and missing the underlying adversity. [10] [2]
- Failing to recognise vicarious trauma and burnout in clinicians who work with traumatised children. [11]
- Treating TIC as a checklist rather than a whole-organisation culture change. [9]
- Ignoring cultural, historical and intergenerational trauma, especially in Indigenous and refugee families. [10]
Prognosis & Disposition
The prognosis of childhood adversity is not fixed. The buffer changes everything. [13] [2]
Resilience is ordinary and buildable. Masten's work shows that resilience is not a rare gift but the product of ordinary, adaptive systems — most powerfully, a safe, stable, nurturing adult relationship. When you strengthen that relationship, you change the trajectory. [13]
Early identification matters. The earlier adversity is identified and buffered, the better the long-term developmental, behavioural and health outcomes. Paediatric primary care is ideally placed to do this. [3] [2]
TIC is universal. It is applied to every patient, not reserved for those with a known trauma history. The universal-precautions model means you do not need to identify trauma to practice trauma-informed care. [9] [10]
Disposition includes follow-up. Connect to supports, schedule review, and monitor resilience and coping over time. One encounter is never the whole story. [10] [12]
Special Populations
Indigenous children. Historical and intergenerational trauma compound present adversity. Use culturally safe, family- and community-centred pathways, follow locally endorsed services and trusted workers, and do not impose a generic model. [10]
Refugee and asylum-seeking children. These children carry cumulative pre-, peri- and post-migration trauma. Always use a trained interpreter, never a child or family member, and link to trauma-focused mental health services. [10] [4]
Children in out-of-home care. High ACE burden, attachment disruption, and often multiple placements. Ensure a comprehensive health assessment, coordinate with child protection, and plan care that accounts for developmental trauma. [10]
Children with disabilities or neurodiversity. Heightened vulnerability to trauma, atypical presentations, and communication barriers. Adapt your assessment to function and relationship, and assume the child understands more than they can express. [10] [2]
Adolescents. Respect autonomy, build trust slowly, address risk-taking and self-harm, and offer confidential time. The adolescent who trusts you will tell you what no screening tool will. [4] [10]
Evidence, Guidelines & Regional Differences
Core anchors are the Felitti 1998 ACE Study, the Shonkoff and Garner 2012 AAP policy statements on toxic stress, the Hughes 2017 and Bellis 2019 meta-analyses, the Finkelhor 2009 national survey, the Marsac 2016 implementation framework, the Forkey 2021 AAP clinical report on TIC, the Goddard 2022 nursing perspective, the Ridings 2023 trauma-centre screening data, and the Masten 2001 resilience framework. [1] [2] [3] [4] [5] [9] [10] [11] [13]
RACP and RCPCH-aligned curricula frame trauma-informed practice as core professional skill. The trauma-informed approach is embedded in child protection, mental health, and Aboriginal and Torres Strait Islander and Māori health pathways. Follow locally endorsed frameworks and trusted community-controlled services; do not invent local statutory wording. [9] [10]
NICE guidance on PTSD (NG116) and RCPCH Progress+ safeguarding and mental-health themes frame practice. Local safeguarding partnerships and child and adolescent mental health services (CAMHS) provide referral pathways. TIC principles are increasingly embedded in national policy. [10]
The AAP clinical report on trauma-informed care (Forkey 2021) and the AAP Healthy Foster Care America trauma toolbox shape practice. The SAMHSA framework — four Rs and six principles — originated in US federal policy and is the global reference standard. ACE screening is expanding in several states, with debate about universal versus targeted approaches. [9] [10]
CanMEDS roles (Communicator, Collaborator, Health Advocate) map directly onto trauma-informed practice. Provincial child welfare and mental health frameworks vary; use local documents, trained interpreters, and culturally safe pathways for First Nations, Inuit and Métis children, where intergenerational trauma from residential schools is a central consideration. [10] [4]
Controversies: universal versus targeted ACE screening; the risk of causing distress without follow-up capacity; the strength of evidence for organisational-level TIC outcomes; and how to adapt the SAMHSA framework across cultures and health systems without diluting it. Exam answers show structured knowledge, biological mechanism, and local humility. [7] [9] [10]
Exam Pearls
- The four Rs: Realise, Recognise, Respond, Resist re-traumatisation. [10]
- The six principles: Safety, Trustworthiness, Peer Support, Collaboration, Empowerment, Cultural issues. [9] [10]
- TIC is a universal approach for every patient, not a referral pathway. [9]
- Universal trauma precautions: assume every child may have a trauma history. [10]
- The safe, stable, nurturing adult relationship is the single most powerful resilience factor. [13] [3]
- Never ask about ACEs without a plan for follow-up and support. [7] [8]
- Medical events themselves can traumatise through pain, separation, fear and loss of control. [11] [12]
- Vicarious trauma in clinicians is an occupational hazard: recognise and address it early. [11]
Trauma-informed care at the bedside
Universal precautions: assume trauma, create a calm environment
Recognise trauma cues; screen when safe and indicated
Respond: explain, offer choice, collaborate, empower
Resist re-traumatisation: prepare, control pain, avoid restraint
Connect: warm handover to mental health and supports
Build resilience: strengthen the buffering relationship; follow up
References
- [1]Felitti VJ Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study. American journal of preventive medicine, 1998.PMID 9635069
- [2]Shonkoff JP The lifelong effects of early childhood adversity and toxic stress. Pediatrics, 2012.PMID 22201156
- [3]Garner AS Early childhood adversity, toxic stress, and the role of the pediatrician: translating developmental science into lifelong health. Pediatrics, 2012.PMID 22201148
- [4]Hughes K The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. The Lancet Public Health, 2017.PMID 29253477
- [5]Bellis MA Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America: a systematic review and meta-analysis. The Lancet Public Health, 2019.PMID 31492648
- [6]Finkelhor D Violence, abuse, and crime exposure in a national sample of children and youth. Pediatrics, 2009.PMID 19805459
- [7]Kerker BD Do Pediatricians Ask About Adverse Childhood Experiences in Pediatric Primary Care? Academic pediatrics, 2016.PMID 26530850
- [8]Szilagyi M Factors Associated With Whether Pediatricians Inquire About Parents' Adverse Childhood Experiences. Academic pediatrics, 2016.PMID 27157045
- [9]Marsac ML Implementing a Trauma-Informed Approach in Pediatric Health Care Networks. JAMA pediatrics, 2016.PMID 26571032
- [10]Forkey H Trauma-Informed Care. Pediatrics, 2021.PMID 34312292
- [11]Goddard A Trauma-informed care for the pediatric nurse. Journal of pediatric nursing, 2022.PMID 34798581
- [12]Ridings LE Behavioral Health Screening and Follow-Up Services in Pediatric Trauma Centers Across the United States. Journal of pediatric psychology, 2023.PMID 37794767
- [13]Masten AS Ordinary magic. Resilience processes in development. American psychologist, 2001.PMID 11315249