Paeds · professional-practice-and-evidence
Working with interpreters and culturally responsive communication
Also known as Interpreters in paediatric care · Limited English proficiency children · Cultural competence paediatrics · Language concordant care · Telephone and video interpreting · Cultural humility communication · Ad hoc interpreter errors
Fellowship-level approach to working with interpreters and culturally responsive communication in paediatrics: interpreter modes, structured interpreter-mediated consultation, error and outcome evidence, cultural competence and humility frameworks, and high-stakes acute, consent, bad-news and adolescent scenarios.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Life stages
Care settings
Clinical exam formats
Board mappings
Overview & Definition
A mother brings her feverish toddler to the emergency department. She speaks Dari and a few words of English, and the registrar, busy and well-meaning, asks the eight-year-old sibling to translate. That single shortcut shapes the whole encounter — what history you get, whether the mother understands the plan, whether consent means anything, and whether the family ever trusts the service again. Working with interpreters and communicating in a culturally responsive way is how you stop that shortcut from happening. [1]
Limited English proficiency (LEP) means a family who cannot speak, read, write or understand English well enough to interact effectively with clinical staff. It is common in paediatrics because the child is often the Australian-, UK- or US-born English speaker while the parents are not, which makes the temptation to use the child as interpreter ever-present. [4]
Culturally responsive communication goes further than language. It is care that acknowledges and integrates the family's beliefs, health practices and social context into clinical decisions. A professional interpreter fixes the language barrier; cultural responsiveness fixes the meaning. You need both, and a fellowship answer treats them as one combined skill. [10] [1]
Classification
Sort the interpreter modes first, then sort the frameworks. [4]
Five interpreter modes. A professional in-person interpreter sits with you and the family and is the gold standard for complex encounters. Telephonic interpreting is available within minutes and is the workhorse for urgent and after-hours care. Video remote interpreting (VRI) adds visual cues and is a strong middle ground. Ad-hoc interpreters are untrained bilingual staff pulled in opportunistically. Family members and children are the last resort and are unsafe for consent, history and bad news. [4] [8]
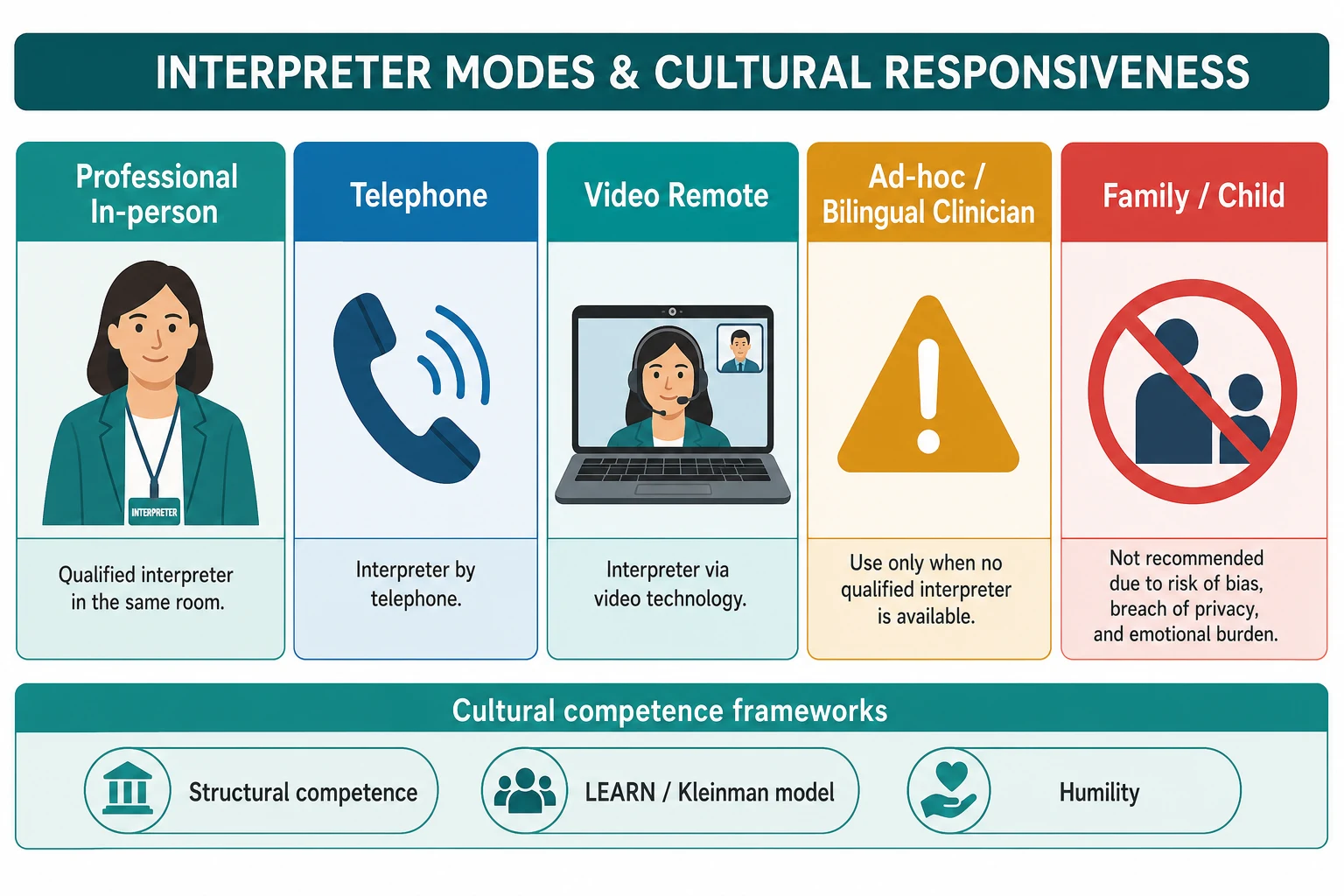
Two frameworks for the cultural dimension. Cultural competence is the knowledge and skills you build to work across cultures; cultural humility is the lifelong self-reflection that keeps you honest about the power gap between clinician and family. They are partners, not rivals. Betancourt frames competence at three levels — organisational, systemic and clinical — which is the structure an examiner wants when you talk about a service, not just a single encounter. [10] [11]
| Mode | Best for | Key risk |
|---|---|---|
| Professional in-person | Consent, bad news, complex chronic care | Needs booking; cost |
| Telephone | Urgent and after-hours encounters | No visual cues |
| Video remote (VRI) | Middle ground, procedures, telehealth | Connectivity and framing |
| Ad-hoc bilingual staff | Only when nothing else is available | Untrained; error-prone |
| Family member or child | Not acceptable for history, consent or bad news | Confidentiality, coercion, error |
Epidemiology & Risk Factors
Families with limited English proficiency are a large and growing part of paediatric practice, concentrated among migrant, refugee, asylum-seeking and some Indigenous communities. Despite that, they receive interpreter services far less often than they need them, and ad-hoc or family interpreters remain common in surveys of ward and emergency care. [8] [1]
Language discordance is not a soft problem. It is linked to longer hospital stays, more investigations, lower understanding and satisfaction, lower follow-up and a measurably higher rate of patient-safety incidents. Migrant and refugee children are over-represented in admissions for ambulatory-care-sensitive and complex conditions, so the cost of poor communication falls on children who are already vulnerable. [2] [5]
Risk factors for a poor encounter cluster around three things. The clinician assumes language proficiency from a name or a few words of English; the system rewards throughput and does not make booking easy; and the family lacks the power to insist. Deaf and hard-of-hearing parents are often missed entirely and given written notes instead of a sign-language interpreter. [7] [4]
Pathophysiology
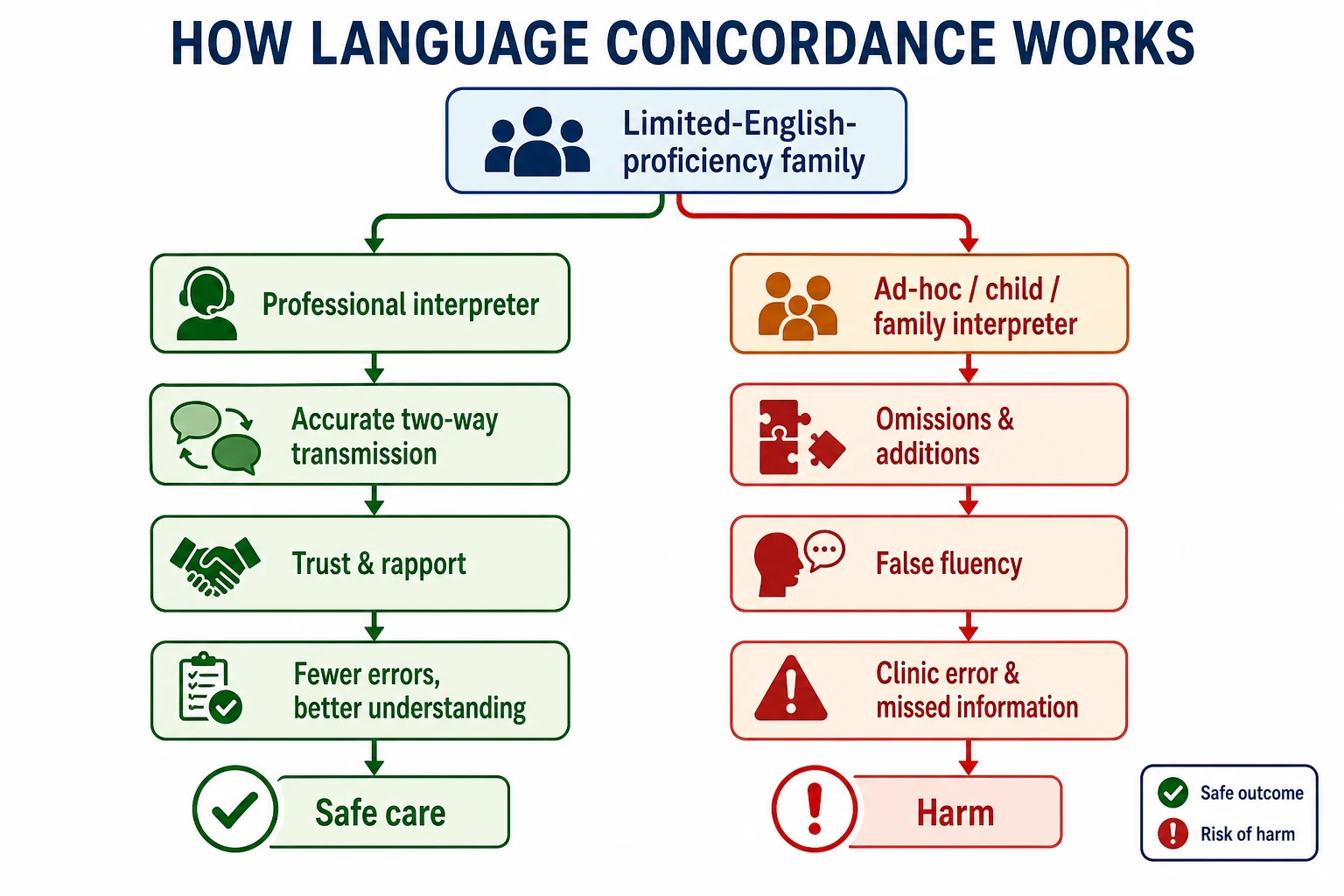
There is no enzyme for a good interpreted conversation, but there is a mechanism. The encounter works when meaning travels accurately in both directions, when the family trusts enough to disclose what matters, and when they can act on what they hear. Each of those steps can fail silently, which is what makes interpreter work a clinical skill rather than a translation utility. [4] [5]
A professional interpreter works by transmitting content faithfully, managing the triadic relationship, flagging cultural misunderstanding and protecting confidentiality. That fidelity is the difference between a plan the family understands and one they nod through. The interpreter also absorbs the emotional weight of the encounter so the clinician and family can speak to each other, not around each other. [4] [6]
Ad-hoc and family interpreters fail through mechanisms you cannot detect at the bedside: omission of content you said, addition of content you did not, substitution of one drug or dose for another, editorialising that softens or exaggerates, and false fluency where the family nods but has not understood. Using a child inverts the family hierarchy, exposes the child to distressing content, breaches confidentiality and hollows out consent. None of this appears on the chart; it just surfaces later as a safety event or a complaint. [5] [6]
Clinical Presentation
You will recognise a family that needs an interpreter by listening for the gaps. A parent answers in short, generic phrases and nods to everything, but cannot restate the plan in their own words. A school-age child is gently pushed forward to "help mummy understand". A registrar switches into a few words of a shared second language and proceeds to consent. A family's real concerns surface only as non-attendance, or as a late and angry complaint. [1] [8]
The high-yield presentations are the high-stakes ones: consent for surgery, breaking serious news, a refugee family with trauma-related silence, an adolescent who needs a confidential conversation, and a Deaf parent booked into clinic with no sign-language interpreter. Each is a moment where using a child or winging it in a second language causes measurable harm. [2] [1]
Differential Diagnosis
When communication feels stuck, diagnose the obstacle before talking louder or slower. [10] [5]
| Surface story | Real obstacle | What to do |
|---|---|---|
| "They don't understand" | Language barrier | Book a professional interpreter |
| "They're non-compliant" | Cultural health belief or values gap | Elicit the explanatory model, negotiate |
| "They're poor historians" | Trauma, fear or mistrust | Trauma-informed, interpreter-mediated history |
| "They seem confused" | Low health literacy, even in shared language | Plain language, teach-back, pictures |
| "They're refusing" | Hearing impairment missed for LEP | Arrange a sign-language interpreter |
Safeguarding can hide behind language or cultural framing. Coerced interpretation, family violence, female genital mutilation and forced marriage may be masked as "cultural difference", and a child pressed into interpreting is itself a safeguarding concern. Your duty to protect overrides the cultural-respect frame — but respect is how you deliver protection, not an excuse to look away. [1] [2]
Clinical & Bedside Assessment
Assess language need before you assess the child. Identify the family's preferred spoken and written language at booking or triage and record it where the whole team can see it. Do not assume proficiency from a name, appearance or a few words of English — ask, and then confirm it. [8] [7]
Then assess the clinician's own role. If you share a second language with the family, judge honestly whether your skill covers consent, dosing and bad news, not just pleasantries. Self-rated clinician second-language skill is unreliable and tends to run ahead of tested competence, so when in doubt, book an interpreter. Screen for hearing impairment and arrange a sign-language interpreter for Deaf or hard-of-hearing families rather than substituting written notes. [7] [4]
Explore the family's explanatory model with open questions: what do you think is causing this, what worries you most, what treatment were you hoping for. Identify who in the family is the decision-maker and how decisions are usually made. Then check understanding by teach-back in the family's language, never with a closed "do you understand?". [10] [11]
Minimum communication assessment: [4] [8]
- Confirm preferred spoken and written language and interpreter need. [8]
- Decide interpreter mode for this encounter and book it. [4]
- Elicit the family's explanatory model and decision-maker. [10]
- Check understanding by teach-back, not a closed question. [5]
- Record the interpreter's name, ID, mode and language. [4]
Investigations
You do not order a blood test for a language barrier. The "investigations" here are structured tools that make communication visible and repeatable. [4] [12]
- Language need record: preferred language and interpreter need flagged in the chart and on the handover sheet so every clinician sees it. [8]
- Translated and plain-language materials: validated leaflets in the family's language, used alongside — not instead of — an interpreter. [11]
- Objective clinician language testing: where a clinician wants to work in a second language, test the skill against a standard rather than trusting self-report. [7]
- Service audit: track interpreter use and unmet need to surface the system gaps that a single clinician cannot fix. [12]
Management — Resuscitation
In the emergency or resuscitation setting, reach for a professional interpreter immediately by telephone or video. Do not wait for an in-person interpreter to arrive for a time-critical decision, and do not use an unaccompanied child if any alternative exists, because telephone interpreting is almost always available. [1] [4]
Stabilise the child first. Spoken information for consent is delivered in the family's preferred language once the child is safe. Keep explanations short, concrete and free of jargon, and check the essentials back rather than attempting a full history under time pressure. For high-stakes acute decisions — consent for surgery, a change in the resuscitation plan — escalate to a senior and switch to in-person or video interpreting. [1] [2]
Management — Definitive & Stepwise
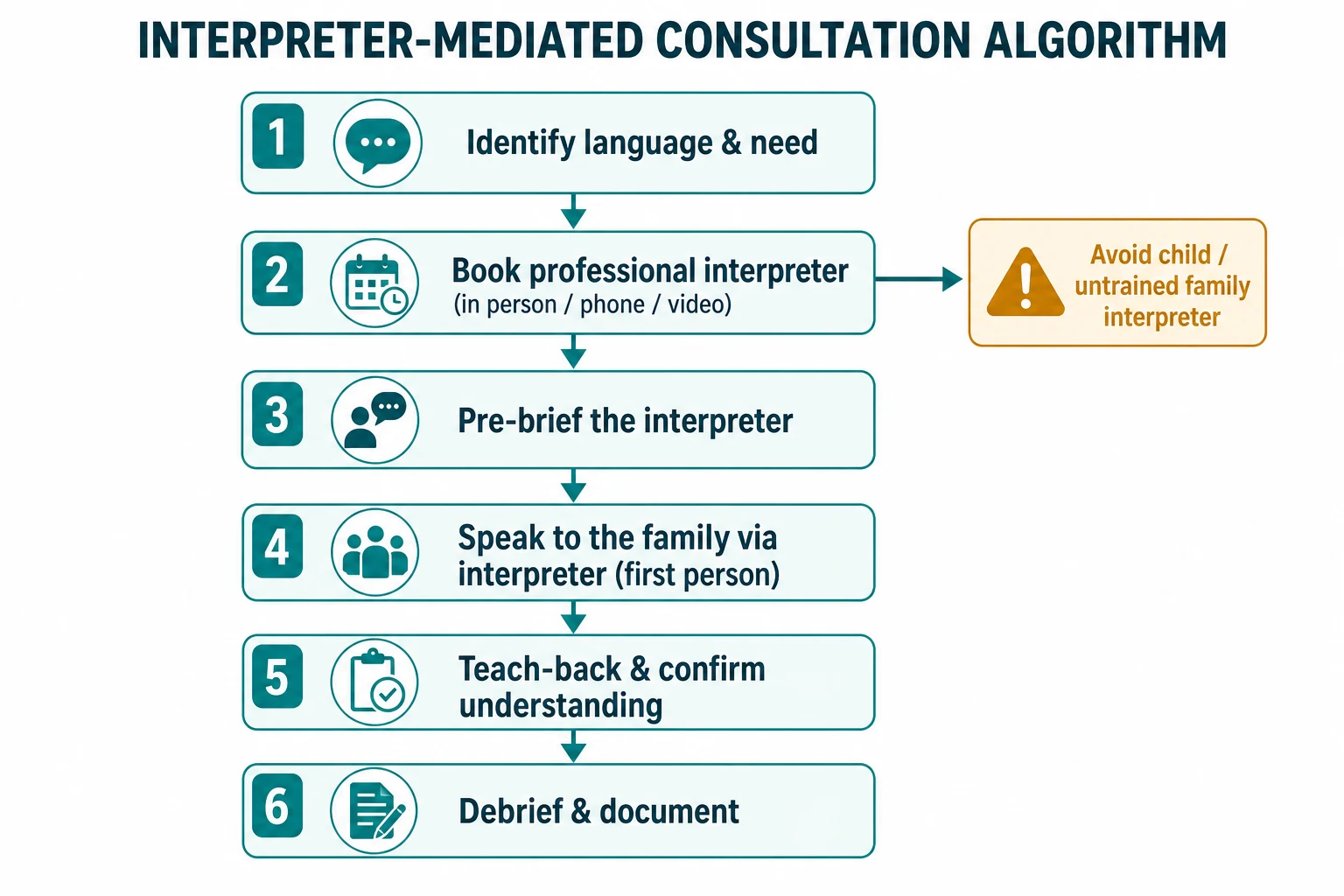
Use a structure you can recite under viva pressure. The cleanest scaffold is the seven-step interpreter-mediated consultation, with cultural responsiveness threaded through. [4] [10]
Interpreter-mediated consultation algorithm
Identify the family's preferred language and interpreter need, and record it
Book a professional interpreter: match language, dialect and, where relevant, gender and religion
Pre-brief the interpreter: state the goal, the likely content and any sensitive material
Speak to the family in the first person, in short chunks, pausing for complete interpretation
Check understanding by teach-back in the family's language; ask for their own words
Debrief the interpreter; thank them and flag anything culturally significant you missed
Document interpreter name, ID, mode and language, teach-back and translated materials given
Speak in the first person, not the third. Say "What worries you about your son?" to the parent, not "Ask her what worries her" to the interpreter. Speak in short chunks, avoid jargon and idioms, and pause for full interpretation. The interpreter is a conduit for meaning, not a spokesperson you address instead of the family. [4] [6]
Build the family's explanatory model into the plan. Use the LEARN model — Listen to the family's perspective, Explain the clinical view, Acknowledge the differences, Recommend a plan, and Negotiate a shared way forward. That negotiation is where culturally responsive care stops being a slogan and becomes a plan the family can actually follow. [10] [11]
Specific Subtypes & Scenarios
Consent for procedures and surgery. Conduct consent in the family's preferred language with a professional interpreter, document the interpreter, and never rely on a child to interpret consent. The same applies to assent from an able older child. [1] [4]
Breaking serious or bad news. Book an in-person or video interpreter, pre-brief them on what is coming, pace the information in short chunks, and check the family's understanding and support. Silence is part of the message; let the interpreter hold it. [1] [2]
Adolescent confidential consultation. Book an interpreter who is not a family member or a community peer, so confidentiality holds. A shared community interpreter can undo in one encounter what an adolescent trusted you to keep private. [1]
Deaf and hard-of-hearing families. Arrange a qualified sign-language interpreter — Auslan, BSL or ASL — and do not substitute written notes, lip-reading or a relative. Hearing impairment in a parent is routinely missed because it looks like limited English proficiency. [4]
Refugee and asylum-seeking families. Take a trauma-informed, interpreter-mediated history; avoid re-traumatising; respect the family's pacing on disclosure; and screen for physical and mental-health sequelae as trust builds. [2]
Telehealth. Confirm interpreter connectivity before the visit and use video where possible so the non-verbal cues that carry so much meaning are not lost to a phone line. [12]
Complications & Pitfalls
- Using a child or family member as interpreter for history, consent or bad news. [1] [6]
- Relying on the clinician's untested second-language skill and missing errors through false fluency. [7] [5]
- Speaking to the interpreter in the third person instead of to the family in the first person. [4] [6]
- Assuming cultural competence from a single ethnicity label and missing within-group variation. [10] [11]
- Treating a translated leaflet or a translation app as a substitute for a professional interpreter. [4] [11]
- Breaching adolescent confidentiality by booking an interpreter connected to the family or community. [1]
- Missing safeguarding concerns hidden behind language or cultural framing. [2] [1]
Prognosis & Disposition
Professional interpreters improve communication, understanding, satisfaction, appropriate service use and patient safety in families with limited English proficiency. The honest framing for an examiner is that interpreter use and culturally responsive care raise the quality and safety of care; they are not a courtesy bolted onto a busy clinic. [4] [3]
A structured, interpreter-mediated and culturally responsive encounter builds trust that pays off across future encounters and adherence, especially in chronic disease and transition. The family that was understood once will engage again. [9] [2]
Disposition is a documented encounter: the language and interpreter mode used, teach-back completed, the family's explanatory model and agreed plan in their words, and the follow-up arrangements. Escalate to social work, refugee health, cultural support or clinical ethics when complex cultural, trauma or safeguarding issues surface. [2] [12]
Special Populations
Migrant, refugee and asylum-seeking children. Provide interpreter-mediated, trauma-informed care and screen for physical and mental-health sequelae as trust builds. These families carry the double burden of language discordance and displacement. [2] [1]
Indigenous families. Deliver culturally safe care with Aboriginal health workers or cultural brokers, acknowledge intergenerational trauma, and respect holistic health models that sit alongside biomedical care. [11] [10]
Deaf and hard-of-hearing parents and children. Arrange qualified sign-language interpreters; never substitute written notes or a family member. [4]
Adolescents. Use an interpreter separate from the family for confidential content, and protect privacy and consent. [1]
Families with low health literacy or disability. Use plain language, teach-back and pictures regardless of language, and book longer interpreter-mediated encounters for complex chronic disease. [5] [11]
Rural and remote families. Use telephonic and video interpreting to overcome distance, and plan ahead for in-person interpreter need at key encounters. [12]
Evidence, Guidelines & Regional Differences
Practice anchors: the Karliner 2007 systematic review showing professional interpreters raise the quality of clinical care while ad-hoc interpreters increase errors; the Flores 2005 systematic review linking interpreter services to better communication, understanding, service use and satisfaction; the Nápoles 2015 finding that clinically significant interpretation errors are common without trained interpreters and predict misunderstanding; and the Boylen 2020 JBI review showing professional interpreters improve outcomes for hospitalised children from migrant and refugee families. [4] [3] [5] [2]
On the clinician side, Diamond showed that self-rated second-language skills usually exceed tested competence, with policy implications for testing and teaching, and that patient-physician language concordance is associated with better quality and outcomes. Schenker documented that ad-hoc and family interpreters remain common for hospitalised patients despite the guidance, and Taira reviewed the hospital-level interventions that actually move the needle at a system level. [7] [9] [8] [12]
Controversies to handle calmly: the cost and access limits of in-person interpreters; how far to trust remote simultaneous and machine translation; and whether language-concordant care widens or closes equity gaps depending on who receives it. [9] [12]
In Australia and Aotearoa New Zealand, free professional interpreting is available to general practices and hospitals through TIS National (Doctors Priority Line) and equivalent services; the national standards for healthcare interpreters set competence, confidentiality and ethics expectations. Recognise the cultural safety obligations to Māori, Aboriginal and Torres Strait Islander families and use cultural brokers and Aboriginal health workers alongside interpreters. [1] [11]
Exam Pearls
BRIDGES
References
- [1]Flores G, Rabke-Verani J, Pine W, Sabharwal A The importance of cultural and linguistic issues in the emergency care of children. Pediatric emergency care, 2002.PMID 12187133
- [2]Boylen S, Cherian S, Gill FJ, Leslie GD, Wilson S Impact of professional interpreters on outcomes for hospitalized children from migrant and refugee families with limited English proficiency: a systematic review. JBI evidence synthesis, 2020.PMID 32813387
- [3]Flores G The impact of medical interpreter services on the quality of health care: a systematic review. Medical care research and review : MCRR, 2005.PMID 15894705
- [4]Karliner LS, Jacobs EA, Chen AH, Mutha S Do professional interpreters improve clinical care for patients with limited English proficiency? A systematic review of the literature. Health services research, 2007.PMID 17362215
- [5]Nápoles AM, Santoyo-Olsson J, Karliner LS, Gregorich SE, Pérez-Stable EJ Inaccurate Language Interpretation and Its Clinical Significance in the Medical Encounters of Spanish-speaking Latinos. Medical care, 2015.PMID 26465121
- [6]Elderkin-Thompson V, Silver RC, Waitzkin H When nurses double as interpreters: a study of Spanish-speaking patients in a US primary care setting. Social science & medicine (1982), 2001.PMID 11286360
- [7]Diamond LC, Tuot DS, Karliner LS The use of Spanish language skills by physicians and nurses: policy implications for teaching and testing. Journal of general internal medicine, 2012.PMID 21773850
- [8]Schenker Y, Pérez-Stable EJ, Nickleach D, Karliner LS Patterns of interpreter use for hospitalized patients with limited English proficiency. Journal of general internal medicine, 2011.PMID 21336672
- [9]Diamond L, Izquierdo K, Canfield D, Matsoukas K, Gany F A Systematic Review of the Impact of Patient-Physician Non-English Language Concordance on Quality of Care and Outcomes. Journal of general internal medicine, 2019.PMID 31147980
- [10]Betancourt JR, Green AR, Carrillo JE, Ananeh-Firempong O 2nd Defining cultural competence: a practical framework for addressing racial/ethnic disparities in health and health care. Public health reports (Washington, D.C. : 1974), 2003.PMID 12815076
- [11]Anderson LM, Scrimshaw SC, Fullilove MT, Fielding JE, Normand J, Task Force on Community Preventive Services Culturally competent healthcare systems. A systematic review. American journal of preventive medicine, 2003.PMID 12668199
- [12]Taira BR, Kim K, Mody N Hospital and Health System-Level Interventions to Improve Care for Limited English Proficiency Patients: A Systematic Review. Joint Commission journal on quality and patient safety, 2019.PMID 30910471